
Abstract
Background
Palliative care is an integral aspect of stroke unit care. In 2016, the American Stroke Association published a policy statement on palliative care and stroke. Since then there has been an expansion in the literature on palliative care and stroke.
Aim
Our aim was to narratively review research on palliative care and stroke, published since 2015.
Results
The literature fell into three broad categories: (a) scope and scale of palliative care needs, (b) organization of palliative care for stroke, and (c) shared decision making. Most literature was observational. There was a lack of evidence about interventions that address specific palliative symptoms or improve shared decision making. Racial disparities exist in access to palliative care after stroke. There was a dearth of literature from low- and middle-income countries.
Conclusion
We recommend further research, especially in low- and middle-income countries, including research to explore why racial disparities in access to palliative care exist. Randomized trials are needed to address specific palliative care needs after stroke and to understand how best to facilitate shared decision making.
Introduction
Stroke is a leading cause of death and disability, with 5.5 million attributable deaths and 80 million stroke survivors worldwide in 2016. 1 Stroke incidence and standardized death rates are falling but population growth and ageing are likely to increase the burden of stroke. 1
The World Health Organization (WHO) defines palliative care as An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.
2
The key aspects of the WHO definition of palliative care, and how this type of care is already provided, to some extent, by stroke units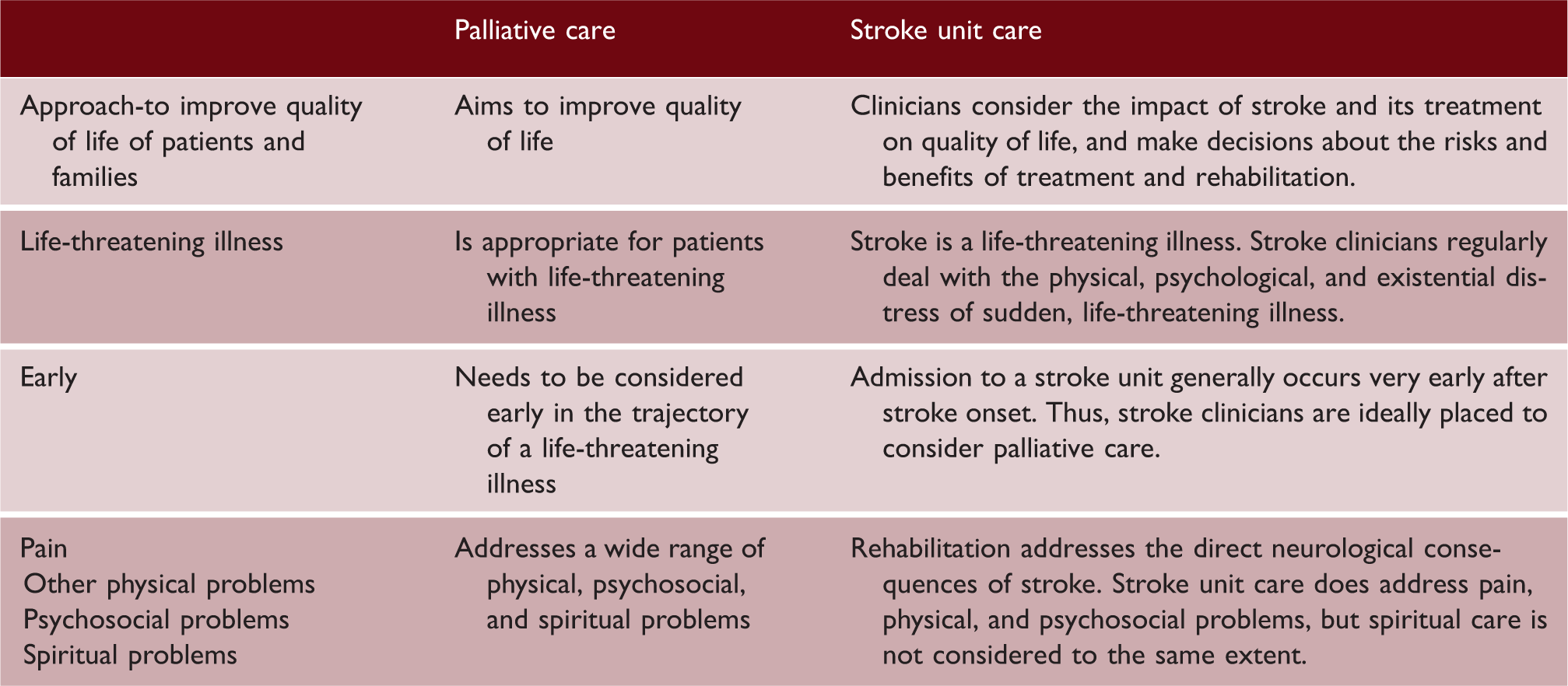
Shared decision making (SDM) is an integral aspect of palliative care. SDM involves combining the best available evidence and patients’ values and preferences into decisions about care, 5 including decisions about interventions that improve survival but with severe disability, and about transitions between care settings.4,6 Stroke has a profound psychological effect on family as well as patient. A truthful, compassionate, appraisal of likely prognosis is essential7–9 (see Supplementary Table 1 for a bereaved carer’s perspective).
Since publication of the American Heart Association’s policy statement on palliative care and stroke in 2016, 3 new literature has been published in this field. Our aim was to identify and critically appraise this new literature; and make recommendations for future research based on gaps identified in the literature.
Search strategy and criteria
We included systematic reviews, observational studies, and trials that focused on palliative care and stroke.
Search methods
On 1 June 2020, we searched multiple databases (Cochrane Stroke Group’s trials register, the Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library, MEDLINE Ovid, Embase Ovid, CINAHL EBSCO and Clinicaltrials.gov) using the terms “palliative care” AND “stroke” (Supplementary Table 2), from 2015 onwards, to identify new literature published since the AHA policy statement on palliative care and stroke published in 2016.
3
Two authors screened titles, obtained full texts of potentially relevant articles, and both read the full texts. We found that this literature fell into three broad categories: (a) scope and scale of palliative care needs, (b) organization of palliative care for stroke and (c) SDM. To identify randomized trials addressing the specific palliative care needs identified in the initial database searches, one author (GEM) then searched the Cochrane Library and Database of research in stroke (DORIS). All authors provided other key papers, not identified in the initial searches.
Figure 1 shows the search results. Further details are in Supplementary Information.
PRISMA flow diagram.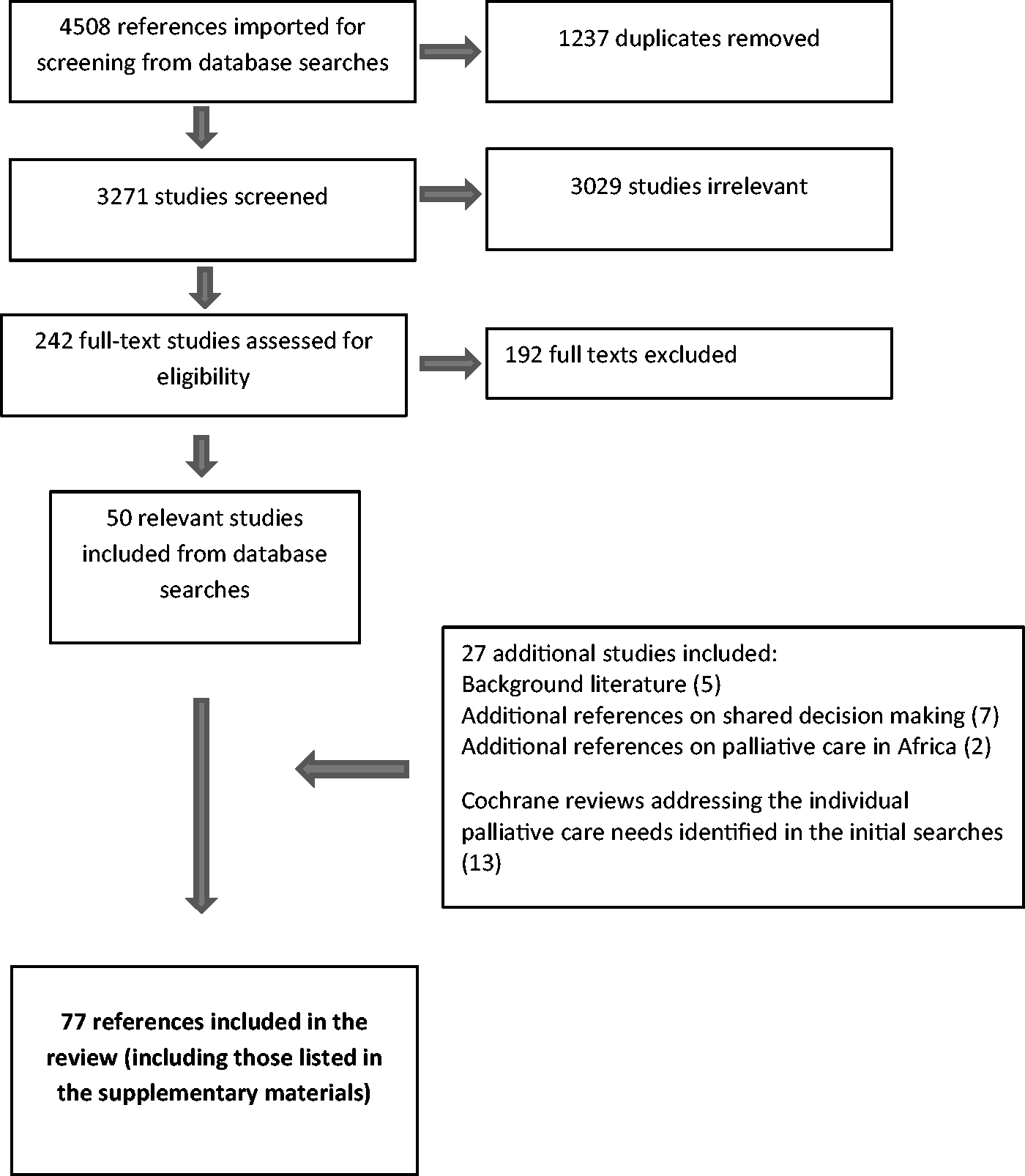
Scope and scale of palliative care needs
Overview of the literature
Observational studies were mostly limited to end-of-life care.4,10–17 These included retrospective cohorts,10,11 a retrospective registry study, 12 a national clinical audit, 13 retrospective case note studies,14,15 a qualitative study with healthcare professionals, 16 cross-sectional face-to-face survey, 17 and one mixed methods longitudinal study. 4 Four studies4,10,11,17 collected data on stroke survivors/decedents in their own homes, six were hospital based,4,12–16 and two were from nursing homes. The studies were from US,10,11 Europe (UK, Ireland),4,14 Sweden, 12 Portugal, 15 Australia, 13 and India.16,17 Three10–13 report large cohorts of stroke patients which were subsets of larger palliative care cohorts.
Frequency of individual palliative care needs
The most frequently recorded needs were dysphagia (96.8%), 15 death rattles (31.5–60.7%), dyspnea (16.3–48.4%), and pain (30.3–42.7%).12,14,15 Two studies14,15 reported anxiety (12.9–18.9% ) and confusion or delirium (7.9–19.4%), while one 14 reported agitation (25.9%). Other symptoms included constipation, dry mouth, and seizures. 15 After hospital discharge, pain affected 50%, numbness or tingling 48%, sleep disturbance 43%, and nausea/vomiting and bladder/bowel incontinence affected 15%. 17 In a large US cohort10,11 receiving home hospice care, stroke was a common cause of fecal 10 or urinary incontinence. 11 Existential needs are also reported; in the UK, 4 hopelessness or loss of meaning was partly related to having to move home or to a care home. In India, 17 over 40% of survivors reported hopelessness and 8% thought about death.
Identification of palliative care needs after stroke
Palliative care symptoms were recognized in about two-thirds of patients who died on an acute stroke unit, 14 although the true frequency is likely to be higher. Swedish healthcare professionals were less likely to know if end-of-life symptoms were present in stroke patients than in cancer patients, or to know if stroke patients’ preferences regarding place of care had been met. 12 Cognitive impairment, aphasia, and dysarthria were barriers to pain assessment 15,16 and accessing services. 4 The largest studies of palliative care needs after stroke were from specialist palliative care settings10,11,13 or unspecified hospital or care home settings, 12 and so cannot easily be generalized to a broader stroke population.
Organization of services, referrals to specialist palliative care services, and place of death
We identified 21 observational studies (mostly reporting referrals to specialist palliative care services) and one prospective study 18 of a palliative care checklist used in a neurointensive care unit.
Very few patients referred to specialist palliative care had had a stroke (0.4%,19,20 4.1%,10,11 6%, 21 8.9% 13 ), and stroke patients tended to be referred only in the terminal phase of their illness.22,23 Six papers from the USA addressed factors predicting referrals to specialist palliative care.24–29 Only 25% of variance was explained by hospital site, 26 and racial minorities were less likely to receive palliative care referral27,28,30 and more likely to receive life-sustaining interventions. 25
Five studies addressed place of death after stroke.4,31–34 Most people dying from stroke do not die at home, 34 only half of stroke patients died in their preferred place (i.e. home); 33 and a quarter of those dying in hospital die alone. Honest discussions with patients and families are needed to explore preferred place of death, to discuss the practicalities of a home death and if this is not possible, how to ensure a “good” hospital death.
Stroke patients, including those with mental capacity, are less likely than cancer patients to receive information about their transition to end-of-life care 12 and their families less likely to receive bereavement support. Healthcare professionals tend to focus instead on physical recovery rather than the psychosocial and spiritual needs. 4 Potentially futile interventions are often ongoing when specialist palliative care referrals are made, 15 or on day of death. 12 Inadequate prescribing of palliative medications is also described15,16 and few physicians saw spiritual care as a significant issue. 16
Management of individual palliative care problems after stroke
Patients with major stroke were often excluded from the Cochrane reviews of interventions 35 and the trials did not include “palliative care” endpoints. 36 One ongoing trial is seeking to improve care in the longer term. 37 Two trials which explored transitions of care did not include people with incapacity or severe stroke.38,39 The table in the supplementary materials summarizes additional relevant reviews for each symptom.
Low- and middle-income countries
Our searches identified two studies from India, and six studies from Africa. Western African low- and middle-income countries (LMICs) have little established palliative care activity, because of resource limitations and lack of political, organizational, or interprofessional collaboration. 40 Pain control was identified in one study 41 as the main unmet palliative care need, and in South Africa, physical, emotional, and social dysfunctions were major concerns for stroke survivors. 42 In Nigeria, informal stroke caregivers reported dissatisfaction with infrastructure, waiting times, and information quality; 43 and stroke survivors’ preferences for rehabilitation settings were influenced by age and finances. 44
In sub-Saharan Africa, some still believe that stroke arises from witchcraft or demons. 45 These beliefs affect treatment preferences for acute stroke care and rehabilitation, but any potential influence on choices about end-of-life care has not been researched. Palliative care research, education of health workers, improved palliative service provision, and policy development in this area are needed. 40 In Nigeria this is beginning to happen, as stroke is now included in the national non communicable diseases multi-sectoral action plan.
Shared decision making
All the literature we identified was observational research or reviews, except for two relevant trials; one is ongoing (“Team-based Versus Primary Care Clinician-led Advance Care Planning in Practice-based Research Networks”) 46 which includes stroke patients; and a feasibility trial of a “Decision Aid for Families of Critically Ill Stroke Patients” that has not yet started. 47
SDM, autonomy, and anticipatory care plans
The ethical principle of autonomy underpins SDM and affirms the right of patients to select their medical therapy from a number of appropriate options. Advanced care plans (ACPs) are rarely in place 48 pre-stroke; for example, of all stroke deaths in an Australian study, only 4% had a pre-stroke ACP in place. 23 After stroke, an ACP for ongoing care can enable preferences, values, beliefs, and goals to be articulated by patients (if they are able to do so) or by their surrogates and enable clinicians to tailor treatment in line with their patient and family wishes.
Patients expect clinicians to take responsibility for initiating SDM, and for identifying a patient’s requirement for information. Clinicians need to plan care consistent with patients’ values and goals. 49 ACPs need regular review and update of a patient’s care preferences in the context of ongoing communication between clinicians, patients, and carers, 50 and the development of a trusting relationship, particularly as prognosis is often uncertain early after stroke and sometimes patients “rally” unexpectedly.
Practical ways to promote SDM in stroke care
The ideal processes of SDM may be impossible to achieve after stroke (because of lack of capacity, need for quick decisions, or uncertain prognosis), but the basic principles of SDM still need to be applied. 51 The key decision makers should be identified and brought together; there needs to be trustworthy and honest exchange of information about treatment options; information must be tailored towards individuals’ needs, and prognostic information must be as accurate as possible and given consistently by different members of the health care team. SDM also requires the best available knowledge of the patients’ personal preferences.
For patients who cannot communicate, the clinician should make sure that the people closest to patient are able to express their views. Discussions should always be recorded. Clinicians should ascertain the extent to which the patient and/or carers wish to have a say in the final decision. 52 Since these decisions may involve heavy responsibility, e.g. for an indefinite life of long-term care versus probable death, they must be made in a way that allows for trust-building and reflection. For irrevocable decisions, the burden of post-decisional regret must be minimized. 52
Strategies for health care professionals during shared decision making after severe stroke
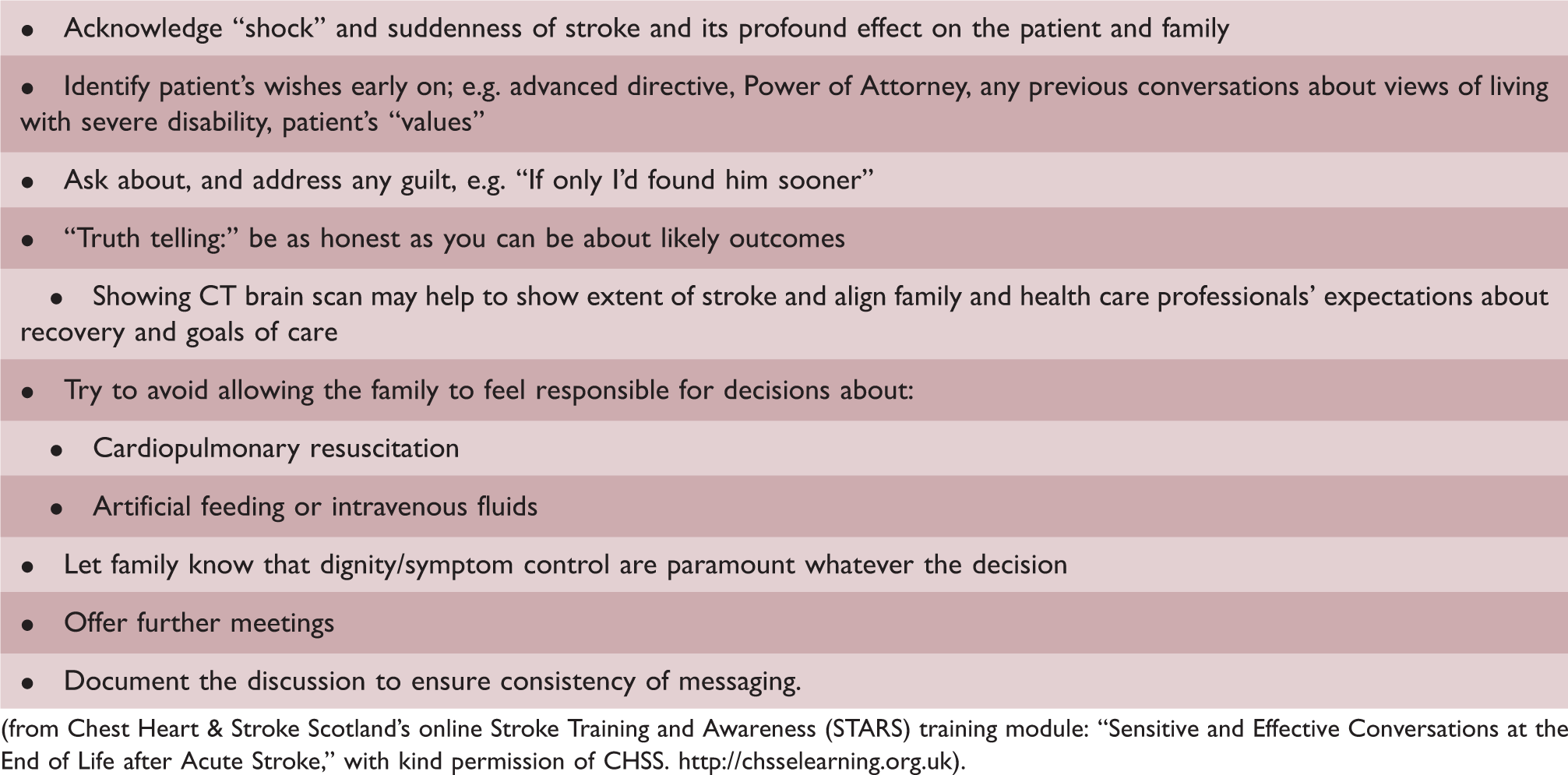
(from Chest Heart & Stroke Scotland’s online Stroke Training and Awareness (STARS) training module: “Sensitive and Effective Conversations at the End of Life after Acute Stroke,” with kind permission of CHSS. http://chsselearning.org.uk).
There is no Cochrane review of SDM specifically in stroke.55–57 Stroke teams nevertheless should offer realistic planning with patients and carers, raising the possibility of death or survival with disability.4,58 Realistic information should be given, avoiding the impression that all treatments result in a functional recovery. 9 Physicians should avoid conveying information from a neutral position or wholly delegate decisions to patients or families.59,60
Healthcare professionals should consider different cultural preference of decision makers, and be aware of the significant burden of family in making decisions.61,62 Substantial grief and stress reactions were identified in 30% of decision makers for severely ill neuro-ICU patients. 63 Therefore, psychological support for carers and patients together with personalized, tailored care, and realistic information should be offered. 8 SDM tools that include predictions from prognostic models appear helpful 64 and information should be framed positively (e.g. independence rather than dependence) yet honestly.65,66
Conclusion and future directions
Almost all of the existing literature is observational, most was from high-income countries, and most focused on end-of-life care and SDM in this context. Stroke patients experience multiple palliative care symptoms (physical, psychological, and existential), few stroke patients are referred to specialist palliative care services, referrals are made close to death, few deaths occur at home, and there are racial differences in palliative care referrals. Uncertainty of prognosis and the need to balance hope with reality is challenging.
Recommendations for clinical care
How can we ensure that people with severe stroke receive holistic care in keeping with their preferences and values? Based on our review of the literature, we suggest three actions:
Clinicians should consider systematically seeking “palliative care problems” in the same way that medical and rehabilitation issues are identified and addressed through history taking, examination, and checklists. SDM needs careful consideration of patient’s values and beliefs, clinicians need to be honest, yet compassionate, about likely outcomes, and patients and families need considerable support to be involved in decision making. Palliative care specialists have extensive experience of similar palliative care problems in other patient groups, and stroke unit care already includes multiple aspects of palliative care. Closer working between stroke clinicians and palliative care clinicians might facilitate better sharing of ideas and knowledge, and help ensure that stroke survivors’ palliative care needs are met.
Recommendations for future research
Observational research is needed to identify the frequency of specific palliative care needs, to explore attitudes and beliefs about stroke and death, and to better understand why there appears to be racial disparities in referral for palliative care. Research is needed particularly in low- and middle-income countries.
Randomized controlled trials are needed to identify management strategies for palliative care problems including pain, delirium, psychological distress, and existential distress, perhaps by adapting interventions that have been tested in palliative care settings in other patient populations.
Developing and testing standardized ways to make shared decisions after severe stroke, including decision aids and information tailored towards patient’s individual needs, might help ensure that patient outcomes are more in line with their beliefs and values.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930211016603 - Supplemental material for Palliative care after stroke: A review
Supplemental material, sj-pdf-1-wso-10.1177_17474930211016603 for Palliative care after stroke: A review by Eileen Cowey, Markus Schichtel, Joshua D Cheyne, Lorna Tweedie, Richard Lehman, Rita Melifonwu and Gillian E Mead in International Journal of Stroke
Footnotes
Authors’ contributions
GEM devised the review. JC designed and ran initial searches and exporting of results. LT reviewed search terms. GEM, JC, and EC ran follow-up searches. EC and GEM screened and selected papers for inclusion and checked reference lists. GEM wrote the outline manuscript draft. RL and MS drafted the section on shared decision making. RM drafted the section on palliative care in Africa. EC then wrote the paper. All authors approved the final draft of the paper.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GEM reports grants from Chief Scientist Office, during the conduct of the study. EC reports contributing authorship to Chest Heart & Stroke Scotland Stroke Training and Awareness (STARS) online training. MS, JDC, LT, RL, RM declare no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Rita Melifonwu https://orcid.org/0000-0002-5192-3871 Gillian Mead ![]()
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.