
Abstract
Background and purpose
“Take Charge” is a novel, community-based self-directed rehabilitation intervention which helps a person with stroke take charge of their own recovery. In a previous randomized controlled trial, a single Take Charge session improved independence and health-related quality of life 12 months following stroke in Māori and Pacific New Zealanders. We tested the same intervention in three doses (zero, one, or two sessions) in a larger study and in a broader non-Māori and non-Pacific population with stroke. We aimed to confirm whether the Take Charge intervention improved quality of life at 12 months after stroke in a different population and whether two sessions were more effective than one.
Methods
We randomized 400 people within 16 weeks of acute stroke who had been discharged to institution-free community living at seven centers in New Zealand to a single Take Charge session (TC1, n = 132), two Take Charge sessions six weeks apart (TC2, n = 138), or a control intervention (n = 130). Take Charge is a “talking therapy” that encourages a sense of purpose, autonomy, mastery, and connectedness with others. The primary outcome was the Physical Component Summary score of the Short Form 36 at 12 months following stroke comparing any Take Charge intervention to control.
Results
Of the 400 people randomized (mean age 72.2 years, 58.5% male), 10 died and two withdrew from the study. The remaining 388 (97%) people were followed up at 12 months after stroke. Twelve months following stroke, participants in either of the TC groups (i.e. TC1 + TC2) scored 2.9 (95% confidence intervals (CI) 0.95 to 4.9, p = 0.004) points higher (better) than control on the Short Form 36 Physical Component Summary. This difference remained significant when adjusted for pre-specified baseline variables. There was a dose effect with Short Form 36 Physical Component Summary scores increasing by 1.9 points (95% CI 0.8 to 3.1, p < 0.001) for each extra Take Charge session received. Exposure to the Take Charge intervention was associated with reduced odds of being dependent (modified Rankin Scale 3 to 5) at 12 months (TC1 + TC2 12% versus control 19.5%, odds ratio 0.55, 95% CI 0.31 to 0.99, p = 0.045).
Conclusions
Confirming the previous randomized controlled trial outcome, Take Charge—a low-cost, person-centered, self-directed rehabilitation intervention after stroke—improved health-related quality of life and independence.
Clinical trial registration-URL
http://www.anzctr.org.au. Unique identifier: ACTRN12615001163594
Introduction
Stroke is the third leading cause of global disability and rates of stroke-related disability have increased in the last 20 years. 1 Activity limitation, participation restriction, and reduced quality of life remain very common for survivors of all types of stroke.2,3 The main components of community stroke rehabilitation practice in Western countries remain task-specific therapy in the context of goals agreed between the patient and the therapy team. 4 Unfortunately, adequately powered randomized studies have failed to demonstrate that these interventions improve independence, participation, or quality of life.5–8 Effective interventions are needed to improve outcomes for people in the community phase of stroke.
The novel “Take Charge” intervention is a community-based session that facilitates self-management of stroke recovery. 9 The intervention was developed from our qualitative research findings where people with stroke felt that the ability to take charge of their health condition was important to them, 10 and was refined by Self Determination Theory, which proposes that people with enhanced autonomy, competence, and relatedness have better outcomes—research largely published in the psychological literature.11,12
We previously tested an intervention based on this principle in a New Zealand study with Māori and Pacific people following stroke—the Māori and Pacific Stroke Study (MaPSS). 13 In that randomized controlled trial (RCT) with 172 Māori and Pacific people with stroke, a single Take Charge session 6–12 weeks after stroke resulted in both statistically and clinically significant improvements in quality of life, carer strain, and independence at 12 months.
The Taking Charge after Stroke (TaCAS) study reported here was a larger study using the same intervention in a broader stroke population similar to those in other major Western countries. We incorporated an evaluation of dose in the study design with participants in the active arms receiving either one or two Take Charge sessions six weeks apart. Our hypotheses were that Take Charge would improve health-related quality of life 12 months after stroke and that a second session would be more effective than one.
Method
Study design
This was a prospective, randomized, open trial of two active and one control interventions with blinded endpoint assessment. The study protocol was approved by the Health and Disability Ethics Committee. Written informed consent was obtained from all participants. The trial is registered with the Australia New Zealand Clinical Trials Registry ACTRN12615001163594. The trial protocol was published before unblinding. 14
Participants
Participants were adults diagnosed with stroke and not of Māori or Pacific ethnicity by self-report. At randomization, participants had to be living in the community in non-institutional care, no more than 16 weeks following their stroke. Exclusions were full recovery from stroke (modified Rankin Scale (mRS) <1), 15 a communication or cognitive deficit precluding personal written informed consent, or a premorbid condition making 12-month survival unlikely. All participants received evidence-based acute stroke care along with inpatient and community stroke rehabilitation as indicated, that was unaffected by study allocation.
Setting
The trial was conducted in seven centers in New Zealand, four tertiary and three non-tertiary centers, serving a catchment population of around 2.4 million people, roughly half the population of New Zealand. 16
Interventions
Following baseline assessments in the person’s home, participants were randomized to either a control intervention, a single Take Charge session, or two Take Charge sessions six weeks apart. Participants randomized to control were given written educational material about stroke produced by the Stroke Foundation of New Zealand, covering common issues following stroke and risk factor management. 17 Participants randomized to the Take Charge interventions received a one-to-one, non-directive exploration of their views on what and who was important to them in their lives, and what they wanted to prioritize for the next 12 months, from a research clinician trained to facilitate this process (see Table A and description in the online appendix). Family members or friends could be present at the person’s request. An illustrated workbook was used to structure the process, to help the person consider the future, and to generate ideas (under headings such as mobility and activities of daily living, communication, information needs, financial issues, emotional needs, supports, and stroke prevention) and the booklet remained with them after the session was completed. 18 The facilitator encouraged the person with stroke to describe their desired outcomes and possible ways to achieve them.
Research clinicians who delivered the intervention worked independently from the community stroke rehabilitation service, and were either nurses or physiotherapists, of whom fewer than half had rehabilitation or stroke experience. They received a half-day training session plus one follow-up session after two months, supplemented by a training manual 18 with email and phone backup from a central trainer and fellow research clinicians. The training emphasized the Take Charge session aims (Table A, online appendix). The intervention was not time-limited and usually took between 30 and 60 minutes to complete. The second Take Charge session included all components of the first, including a repeat baseline assessment.
Randomization and blinding
Participants were randomized into the three intervention arms in a 1:1:1 ratio. The allocations were concealed in sequentially numbered, opaque, sealed envelopes, and once opened either the control or active intervention proceeded at the same visit. Envelopes were prepared for each center in blocks of 18 by the study statistician using computer-generated random numbers.
A schedule of assessments and brief description is in Table B in the online appendix. Measures included Barthel Index (BI), 19 Frenchay Activities Index (FAI), 20 mRS, 15 Short Form 12 Physical Component Summary (SF-12 PCS) score, 21 Short Form 36 (SF-36) PCS, 22 Caregiver Strain Index, 23 and Euroqol EQ-5D-5L. 24 All baseline and 12-month assessments were collected face-to-face apart from five (1.3%) 12-month assessments made by telephone. Six-month and 12-month assessments were collected blind to treatment allocation. Six-month assessments were made by postal or electronic questionnaire with a small number of assessments (6%) by telephone. All 12-month assessments were completed in person by the same outcome assessor. At six and 12 months following stroke, information about hospital admissions, new episodes of stroke, and any rehabilitation contact were collected directly from participants. Hospital admission details were checked by case-note review.
Outcomes and statistical methods
The primary outcome was the PCS score of the SF-36, 12 months after stroke, comparing any Take Charge intervention (either one session (TC1) or two sessions (TC2)) with control. This is a psychometrically robust instrument measuring health-related quality of life, well validated in people with stroke. 22 A short summary of how the PCS is derived, along with normal values is in the online appendix.
The primary analysis was analysis of variance (ANOVA). Secondary analyses included analysis of covariance (ANCOVA) with adjustments for pre-specified important baseline variables and treating the amount of Take Charge sessions (zero, one, or two sessions) as a dose variable. Pre-specified sub-groups were analyzed using general linear models.
Pre-specified secondary outcome variables assessed at six and 12 months following stroke are listed in Table B (online appendix). These were analyzed by either a general linear model (ANOVA) or logistic regression. Analysis results are shown for both the main effect of randomization (i.e. whether there was evidence that the means for TC1, TC2, or control were different from each other) and also for the specific comparison between any Take Charge intervention compared to control. A pre-specified individual patient meta-analysis combining the results of the current study with the previous MaPSS study was undertaken, comparing Take Charge intervention against control for SF-36 PCS and mRS. SAS 9.4 (SAS Institute) was used.
In our previous study, the difference in the mean PCS was six points. 13 There is no published evidence to define the minimal clinically important difference (MCID) of the SF-36 PCS in stroke. Our study was powered to detect a difference of five points on the PCS based on our previous study and the “universal law” propounded by Norman et al. 25 that the MCID for health-related quality of life measures such as the SF-36 for chronic diseases is half a standard deviation (about five points) no matter which health condition, and of any severity. Agreement with Norman’s law is not universal, 26 and in non-stroke conditions, MCIDs of 2–3 points for the SF-36 PCS have been suggested.27,28 For this study, 120 participants would be needed in each of three arms to detect a five-point difference in the PCS with 90% power and alpha of 0.05. We allowed for a 10% drop out rate and aimed to recruit 400 participants.
Results
Between October 2015 and August 2017, 400 participants were randomized to one Take Charge session (TC1, n = 132), two Take Charge sessions (TC2, n = 138), or control intervention (n = 130). Two participants withdrew consent for follow-up (one from TC1 who withdrew after randomization but before delivery of the intervention, and one from TC1 after completing the intervention but before six-month follow-up). Ten participants (two control, four TC1, four TC2) died during the follow-up period. Deaths were attributed to cancer (n = 4), sepsis following a fall (n = 1), complications related to severe stroke (n = 1), and “died at home from natural causes” (n = 4). All remaining participants (n = 388, 97%) were followed up 12 months following stroke. Two episodes of inadvertent unmasking of the outcomes assessor occurred at the 12-month visits.
The flow of participants is shown in Figure 1. Reasons and numbers of participants excluded prior to randomization are in Table C, online appendix. Of 2686 patients screened in hospital but excluded by the randomization visit, 2255 (84%) did not meet inclusion criteria and 373 (14%) declined to participate or lived too far away to be visited.
CONSORT diagram.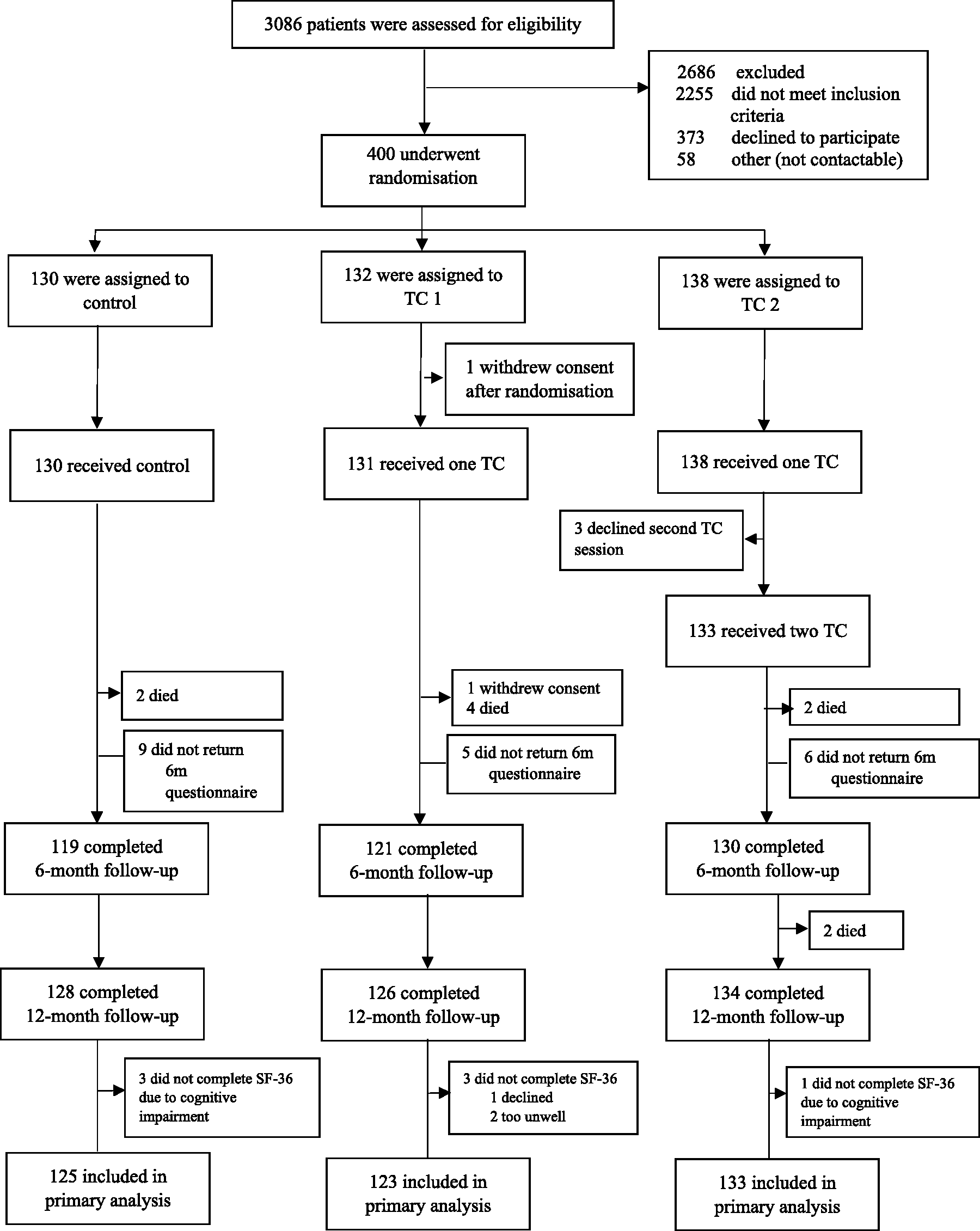
Description of participants at baseline assessment
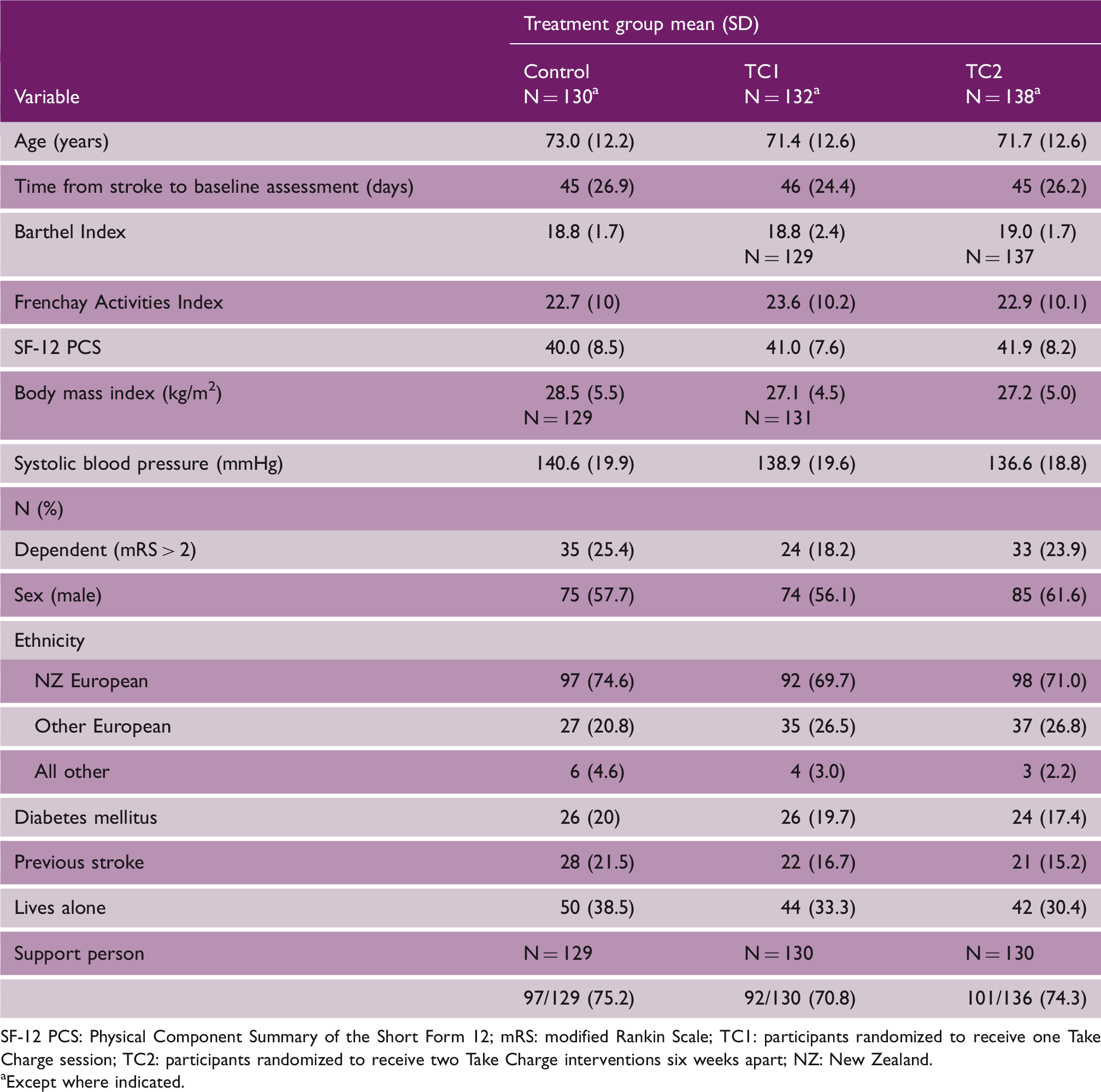
SF-12 PCS: Physical Component Summary of the Short Form 12; mRS: modified Rankin Scale; TC1: participants randomized to receive one Take Charge session; TC2: participants randomized to receive two Take Charge interventions six weeks apart; NZ: New Zealand.
Except where indicated.
Primary outcome
Results
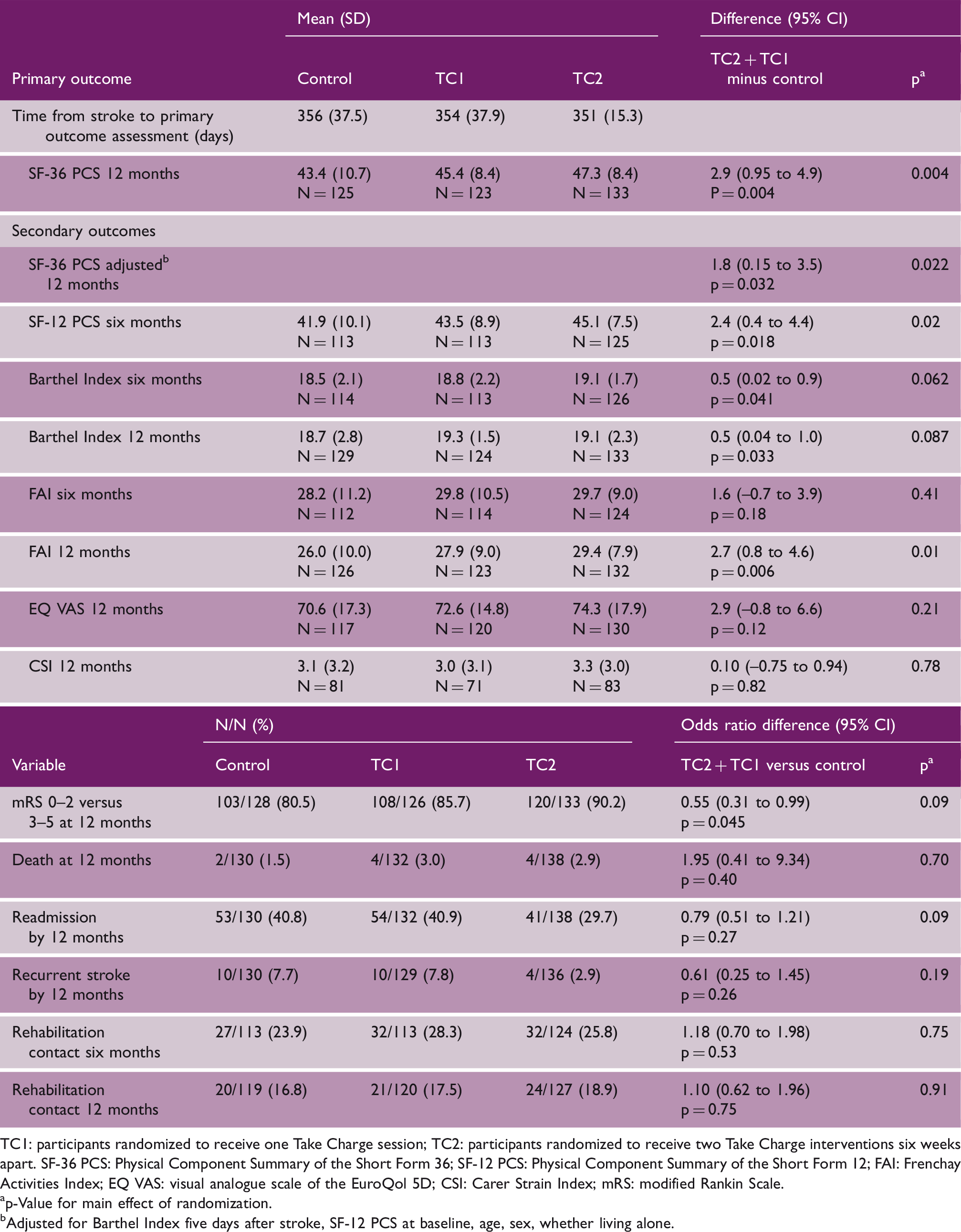
TC1: participants randomized to receive one Take Charge session; TC2: participants randomized to receive two Take Charge interventions six weeks apart. SF-36 PCS: Physical Component Summary of the Short Form 36; SF-12 PCS: Physical Component Summary of the Short Form 12; FAI: Frenchay Activities Index; EQ VAS: visual analogue scale of the EuroQol 5D; CSI: Carer Strain Index; mRS: modified Rankin Scale.
p-Value for main effect of randomization.
Adjusted for Barthel Index five days after stroke, SF-12 PCS at baseline, age, sex, whether living alone.
The PCS difference amongst pre-specified subgroups is shown in Table D (online appendix) and Figure 2 with apparently greater difference for TC1 + TC2 compared to control for female participants, those living alone, and those with a support person. There was no significant interaction with age or stroke severity.
Interaction plot: Differences in SF-36 PCS at 12 months; any Take Charge intervention minus control by subgroups. SF-36 PCS: Physical Component Summary of the Short Form 36.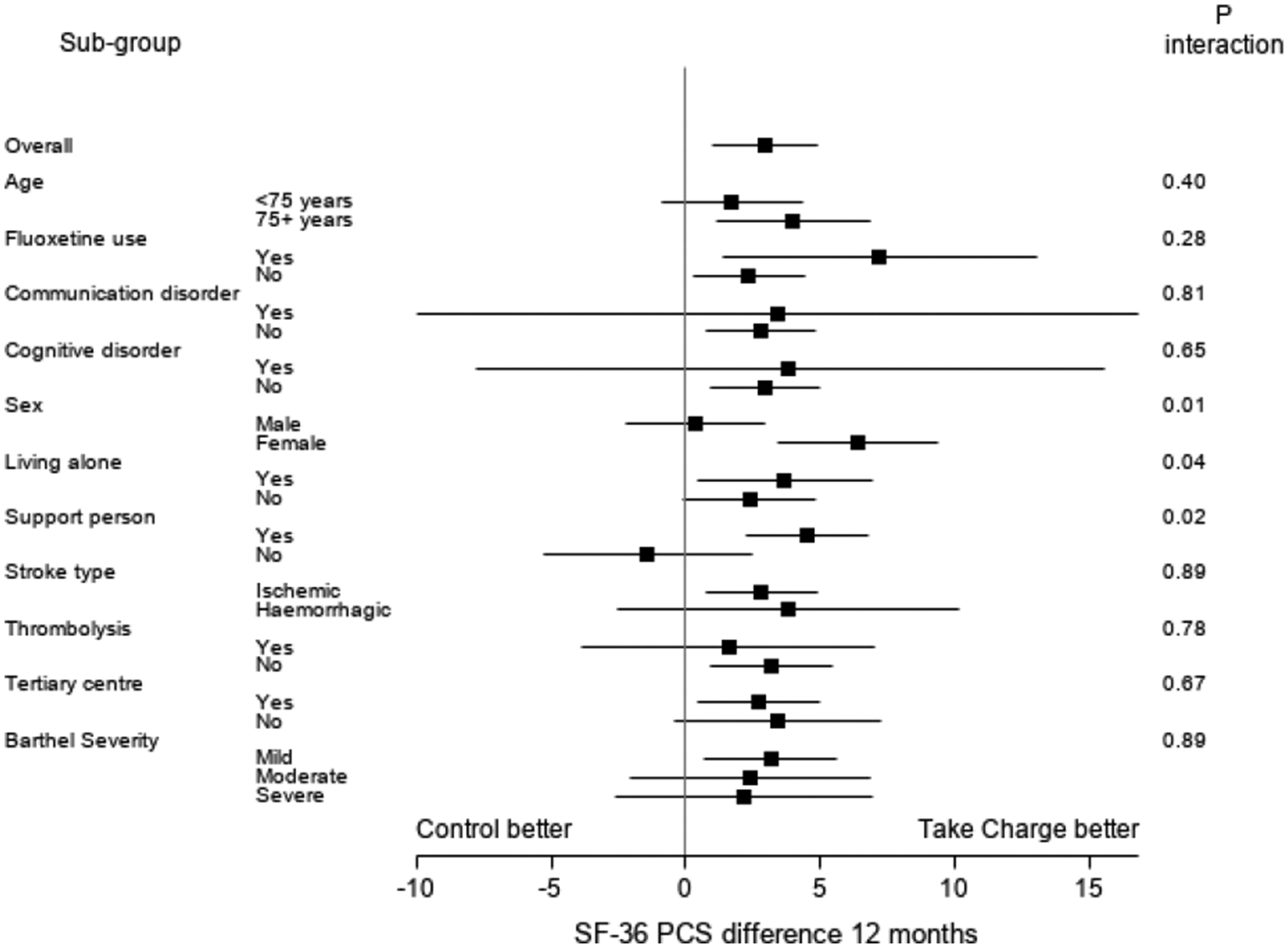
Secondary outcomes
Compared to control, participants in TC1 + TC2 scored 2.4 units (95% CI 0.4 to 4.4, p = 0.018) higher on the SF-12 PCS after six months, 2.7 units (95% CI 0.8 to 4.6, p = 0.006) higher on the FAI after 12 months, 0.5 units higher (95% CI 0.02 to 0.9, p = 0.04) on the BI after six months, and 0.5 units higher (95% CI 0.04 to 1.0, p = 0.033) on the BI after 12 months (Table 2). There were no statistically significant differences at 12 months after stroke for any of the dimensions of the EuroQol EQ-5D-5L, CSI or mRS using ordinal regression (Table E, online appendix). Participants receiving either one or two Take Charge sessions were less likely to be dependent (mRS 3 to 5) at 12 months compared to control, (TC1 + TC2 12% versus control 19.5%, odds ratio (OR) 0.55, 95% CI 0.31 to 0.99, p = 0.045). There were no adverse events attributed to the intervention. Readmission within 12 months (TC1 + TC2 35.2% compared to control 40.8%, p = 0.09) and recurrent stroke within 12 months (TC1 + TC2 5.3% compared to control 7.7%, p = 0.19) were not significantly different. Rehabilitation contact at six and 12 months was not different between groups (Table 2).
Results in context: Individual patient data meta-analysis
Pre-specified individual patient meta-analysis combining the results of the MaPSS and TaCAS studies (N = 572 participants) showed a pooled estimate of the improvement in SF-36 PCS at 12 months after stroke for participants who received the Take Charge intervention compared to control of 3.7 units (95% CI 2.0 to 5.5, p < 0.001) (Figure 3). Dependence (mRS 3 to 5) at 12 months after stroke for the Take Charge intervention was reduced: 47/329 (14.3%) compared to control, 53/197 (26.9%), OR 0.51 (95% CI 0.32 to 0.80, p = 0.003). For the combined studies, the number needed to treat (NNT) with the Take Charge intervention for one fewer person to be dependent at 12 months post-stroke was 7.9 (95% CI 5.0 to 18.5).
Individual participant meta-analysis across two Take Charge studies in people with stroke: SF36 PCS and mRS, 12 months following stroke. MaPSS: Maori and Pacific Stroke Study; TaCAS: Taking Charge after Stroke study; SF-36 PCS: Physical Component Summary of the Short Form 36; mRS: modified Rankin Scale. Box size is proportional to the study variance. This individual participant meta-analysis incorporates study as a main effect but also treats both Take Charge intervention arms in the TaCAS study as one type of intervention rather than two different interventions to be consistent with the MaPSS which only had one Take Charge intervention. The estimates in the model incorporating study as a main effect have led to slightly different point estimates and confidence intervals when the studies are treated together in the meta-analysis compared to when the studies are treated separately.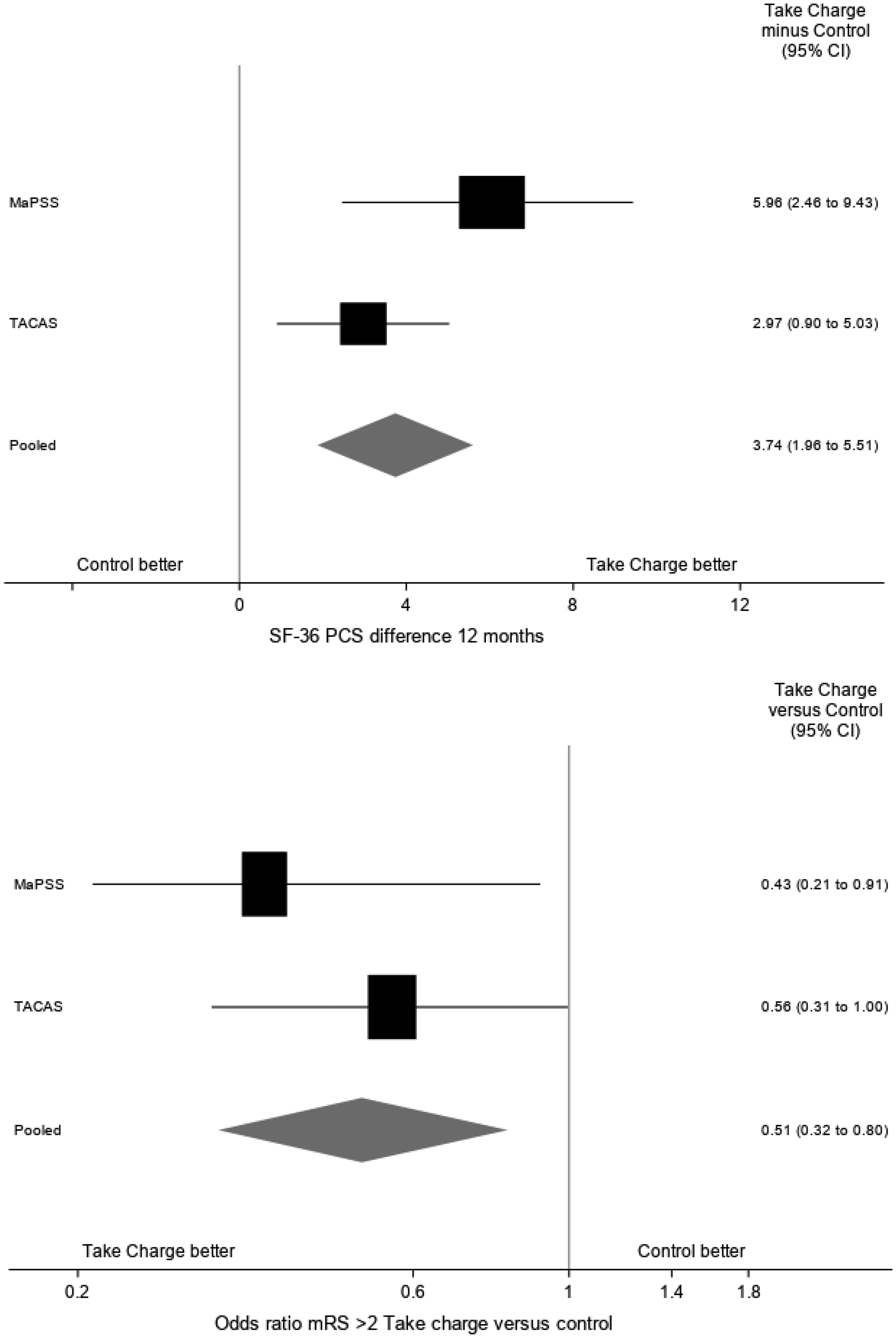
Discussion
The Take Charge session is a simple, low-cost intervention that, when applied in the early community phase of stroke recovery, leads to an improvement in health-related quality of life six months following stroke which is sustained at 12 months. Two sessions, six weeks apart, were better than a single session. Improvements were also seen in basic and advanced activities of daily living and independence.
The strengths of this study include adequate size, masked outcome assessment, outcomes measured 12 months after stroke to ensure sustained response, and excellent follow-up rate. Positive results at the level of activity limitation, participation, independence, and quality of life support the validity of the results and suggest they will be meaningful to people with stroke. Replication of the positive results from a previous study, 13 but in a different population, supports the generalisability of the results to similar populations. The results of the individual patient meta-analysis of the MaPSS and TaCAS studies suggest a clinically significant improvement in PCS and independence with an NNT for avoiding dependence at 12 months after stroke of about eight, equivalent to the effect size for intravenous thrombolysis within three hours of acute stroke. 29 A cost-effectiveness analysis of the TaCAS study has been completed and will be submitted for publication in due course.
It may surprise some that this low-intensity intervention delivered several weeks after acute stroke could be effective with a sustained response 12 months after stroke. Support for our approach comes from several sources: qualitative research that “taking charge” matters to people with stroke,10,30 a large body of theoretical and experimental research based on Self-Determination Theory published in the psychology literature11,12 showing evidence for better outcomes for people with enhanced autonomy, competence, and relatedness—all components of the Take Charge intervention, and evidence from a recent systematic review suggesting that self-management strategies can improve quality of life after stroke. 31 We suggest that the Take Charge intervention likely works by stimulating a person’s intrinsic motivation with a clearer sense of purpose, hope, and enhanced autonomy. For this study, we did not collect detailed information about the actual steps individuals took in response to the Take Charge intervention. However, a linked qualitative study exploring these responses, collected 12 months following stroke, has been completed and will shed some light on this aspect of the intervention.
Further, we think that the delivery of the Take Charge intervention as a fully person-centered approach to life following stroke is one key to its effectiveness. Rehabilitation clinicians may feel that they already include “person-centered goal-setting” in their normal clinical practice, but evidence, including a systematic review, suggests otherwise.32,33 A recent re-evaluation of the negative results of the moderate to large RCTs of stroke rehabilitation in the last decade 8 suggests that a failure “to incorporate patient values, goals, perspectives, and capacity into the trial design and outcomes” was an important factor in their failure to show benefit. Our positive results, with a study design fully incorporating values, goals, and perspectives of the person with stroke, support this premise. Dominant rehabilitation orthodoxy supports the notion of “SMART” goals (Specific, Measurable, Achievable, Realistic/relevant, and Timed). 34 The Take Charge approach rejects all of these elements apart from the “R” for “relevant to the person with stroke.” The SMART approach may promote precise measurement and efficiency, but in rehabilitation of people with stroke, it risks weakening autonomy and sense of purpose. There was no evidence for increased rehabilitation contact in the Take Charge groups as a possible alternative mechanism for improved outcomes.
Both MaPSS and TaCAS were carried out in New Zealand, which has a publicly funded health service where acute hospital care, early supported discharge, and community rehabilitation is free to the patient. People with rehabilitation needs generally receive several weeks of therapy-based rehabilitation in outpatient or domiciliary settings. 35 We believe the results from this study can be applied to similar stroke populations in developed countries but may be of particular relevance in developing countries given the simplicity of the intervention, low cost, and absence of harm.
There is no published MCID for the PCS for people with stroke. We arbitrarily chose a difference of five points which was not achieved in this study. We will report an analysis of the MCID for the PCS for people with stroke separately. The statistically significant reduction in dependence, measured by the mRS, supports the notion that the Take Charge intervention produces clinically significant change.
Four weaknesses of the study should be highlighted. First, using opaque sealed envelopes for randomization is not as robust as centralized electronic assignment, but the groups were generally well matched at baseline limiting concerns about systematic bias. Second, there was a (non-significant) imbalance in SF-12 PCS scores at baseline, favoring the intervention groups. However, a sensitivity analysis incorporating these scores, along with other pre-specified variables (Table 2), showed that the conclusions were robust to this imbalance. Third, the study population was skewed towards people with milder stroke, reflecting inclusion criteria that required participants to be discharged to non-institutional community living within 16 weeks: 84% had either mild or moderate stroke severity. There was no difference in the direction or size of the treatment effect in the subgroup analysis for people with mild, moderate, or severe stroke, but the CIs for moderate and severe categories are wide. Finally, regarding potential assessment bias, measures to maintain masking of the outcomes assessor were rigorous and only two instances of inadvertent unmasking at the 12-month visit occurred. Also arguing against significant assessment bias at 12 months, the difference in PCS scores at six months (collected in 94% of participants by post or electronically) was of similar size and direction to that at 12 months, collected face-to-face.
The Take Charge approach may be effective in other health conditions. One such study, after acute exacerbation of chronic obstructive pulmonary disease, is underway. 36
In conclusion, Take Charge improves quality of life and reduces dependence after stroke. It is simple, low cost, safe, and we believe appropriate for most people following stroke.
The TaCAS study group
Wellington/Lower Hutt: Harry McNaughton, Vivian Fu, William Taylor, Tom Thomson, Mark Weatherall, Judith Riley, Kathryn Fernando, Anna Hunt, Gayle Williams, Claire Houghton, James Berry, Tony Mallon, Tanya Baker, Joanna Read, Allie Eathorne, Nick Shortt.
Palmerston North: Annemarei Ranta, Rebekah Higgs.
Christchurch: Carl Hanger, Deborah Allen, Haley Evans.
Counties-Manukau: Geoff Green, Amanda Retter.
Hawke’s Bay: John Gommans, Eryn Kyle-Foulds.
Auckland: Anna McRae, Nicole Nancarrow, Lauren Lucas.
Supplemental Material
WSO915144 Supplemental Material - Supplemental material for Taking Charge after Stroke: A randomized controlled trial of a person-centered, self-directed rehabilitation intervention
Supplemental material, WSO915144 Supplemental Material for Taking Charge after Stroke: A randomized controlled trial of a person-centered, self-directed rehabilitation intervention by Vivian Fu, Mark Weatherall, Kathryn McPherson, William Taylor, Anna McRae, Tom Thomson, John Gommans, Geoff Green, Matire Harwood, Annemarei Ranta, Carl Hanger, Judith Riley and Harry McNaughton in International Journal of Stroke
Footnotes
Acknowledgements
The authors wish to thank Professors Peter Sandercock and Richard Lindley for their helpful comments on an earlier version of the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor McPherson was Chief Executive of the Health Research Council of New Zealand, the funding body, at the time the study was undertaken. She had no role in the decision to fund the study. Otherwise, the authors report no financial relationships with any organizations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a grant from the Health Research Council of New Zealand (15/297).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.