
Abstract

Dear Editor,
Primary central nervous system vasculitis (PCNSV), also known as primary angiitis of the central nervous system (CNS), is a rare condition affecting the arteries of the CNS. 1 The diagnosis is challenging and based on extensive investigations including MRI, cerebrospinal fluid (CSF) examination, angiography and biopsy, all of which have a limited sensitivity or specificity.1–3 MRI with vessel wall imaging (VWI) showing gadolinium enhancement of the vessel wall may be an important tool for the diagnosis of PCNSV, 4 the value of which will have to be established.
Patient 1
A 50-year-old male, with a medical history of recurrent sinusitis and a lumbar spine operation, presented with headaches followed two months later by acute diplopia and veering towards the right. Neurological examination showed upward deviation of the left eye, an upbeat nystagmus, and unstable gait with a tendency to fall toward the right. No diagnosis was made and no treatment was started. The deficits recovered gradually. For three months, episodes of diplopia and transitory weakness recurred, without any neurological deficits. Five months after the initial onset of the headaches, a motor aphasia developed. The MRI showed new T2-hyperintense lesions and diffusion abnormalities in the left thalamus. A diagnosis of ischemic stroke was made and high dose low-molecular weight heparin (LMWH) was started. The patient was transferred to our hospital.
A 7 Tesla-MRI with VWI was added to the regular diagnostic work-up to investigate its potential diagnostic contribution. This protocol included a T1-MPIR-TSE sequence before and after gadolinium administration, including transverse imaging of the basal intracranial vessels.
Laboratory investigations were normal for blood cell counts, ESR, electrolytes, creatinine, liver enzymes, glucose, C-reactive protein, ACE, antiphospholipid antibodies, p-ANCA, and c-ANCA. ANA showed weak positivity at 1:100. Serological tests for Borrelia, syphilis, HIV, hepatitis C, HSV, VZV, and CMV were all negative.
A chest-CT scan and an FDG-PET scan showed no abnormalities.
CSF examination showed 18 × 106/L leukocytes, a total protein concentration of 0.88 g/L, an IgG-index of 1.23, and positive oligoclonal banding. Cytological examinations were normal on two occasions. Microbiological and serological studies were also normal.
Gadolinium-enhanced T1-MRI showed two small areas of parenchymal enhancement adjacent to the pre-existing ischemic lesions. MR-angiography (MRA) followed by conventional angiography in the third week after onset of aphasia showed multifocal narrowing of the distal carotid, and the anterior, middle, and posterior cerebral arteries on both sides. Subsequently, vessel wall images of 7T-MRI showed extensive multifocal vessel wall enhancement and thickening of the wall of the arteries of the circle of Willis at segments of arterial narrowing visible on conventional angiography. The enhancement was mostly circular but also irregular and eccentric (Figure 1). The images were highly suggestive of cerebral vasculitis.
7T-MRI with a T1-weighted magnetization preparation inversion recovery turbo spin echo (MPIR-TSE) after gadolinium administration showing diffuse circular and irregular enhancement. Note the eccentric enhancement of the left anterior cerebral artery (ACA). (a) Transverse image of left ACA. (b) Transverse image of distal internal carotid arteries (ACI), proximal medial cerebral arteries (MCA), and posterior cerebral arteries (PCA), and (c) Transverse image of vertebral, basilar, and posterior cerebral arteries.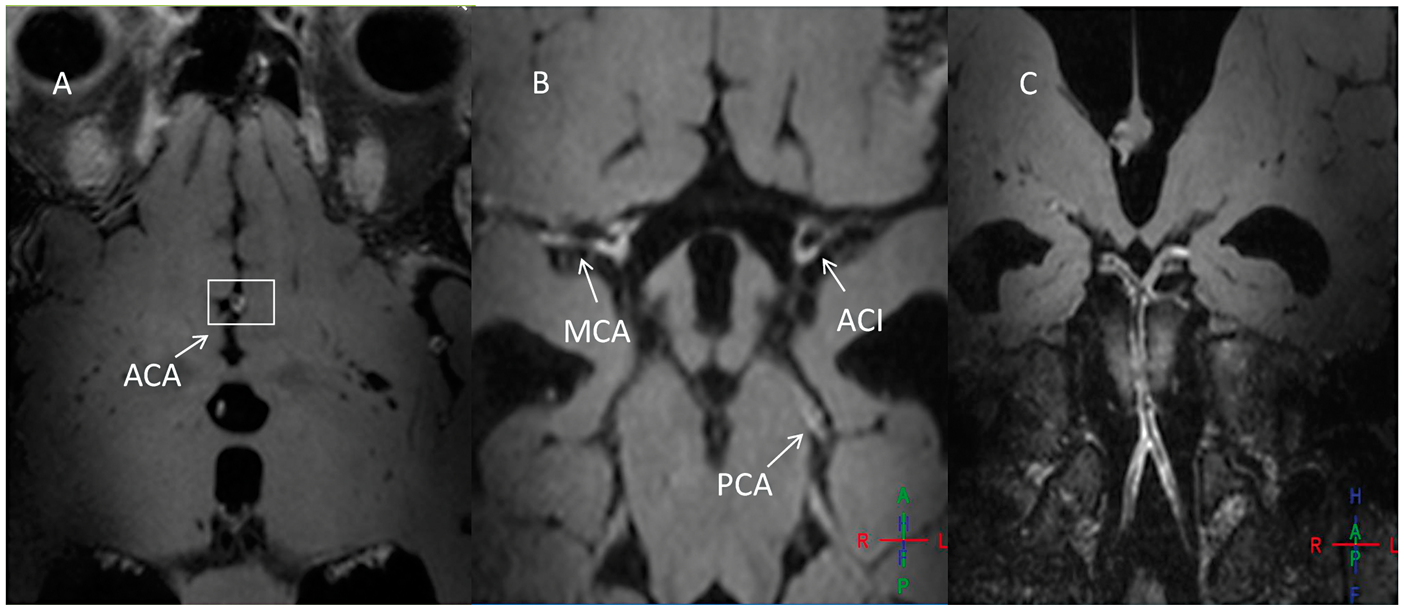
To confirm the diagnosis of PCNSV, a brain biopsy was performed. On the second postoperative day, after LMWH was restarted, an acute subdural hematoma occurred at the area of the biopsy. Despite immediate surgical evacuation of the hematoma, the patient remained in a deep coma and died three days later.
Pathological examination of the brain biopsy specimen was inconclusive. Postmortem examination showed widespread multifocal inflammation throughout arterial walls of middle and large intracranial arteries that was compatible with a diagnosis of PCNSV and concurred with the MRI findings. There were ischemic changes of the parenchyma in several cortical and subcortical areas of both cerebral hemispheres. The inflammatory changes occurred at the same arterial segments that showed narrowing on MR-angiography and intense wall enhancement on the gadolinium enhanced T1-weighted MPIR-TSE images (Figure 2).
Pathological specimen from the slice of the anterior cerebral artery shown in Figure 1(a). (a) Hematoxylin and eosin (H&E) stain of the anterior cerebral artery shows thickening of the tunica intima (marked by double-headed arrow) and infiltration of inflammatory cells in the tunica media (box, enlarged in figure c). (b) EvG staining emphasizes the elastic lamina between tunica intima and tunica media with some disturbance in elastine fibers in the elastic lamina (marked by single arrow), and (c) Enlarged image of the mixed infiltration of inflammatory cells in the tunica media (box in a), composed of lymphocytes, macrophages, and monocytes.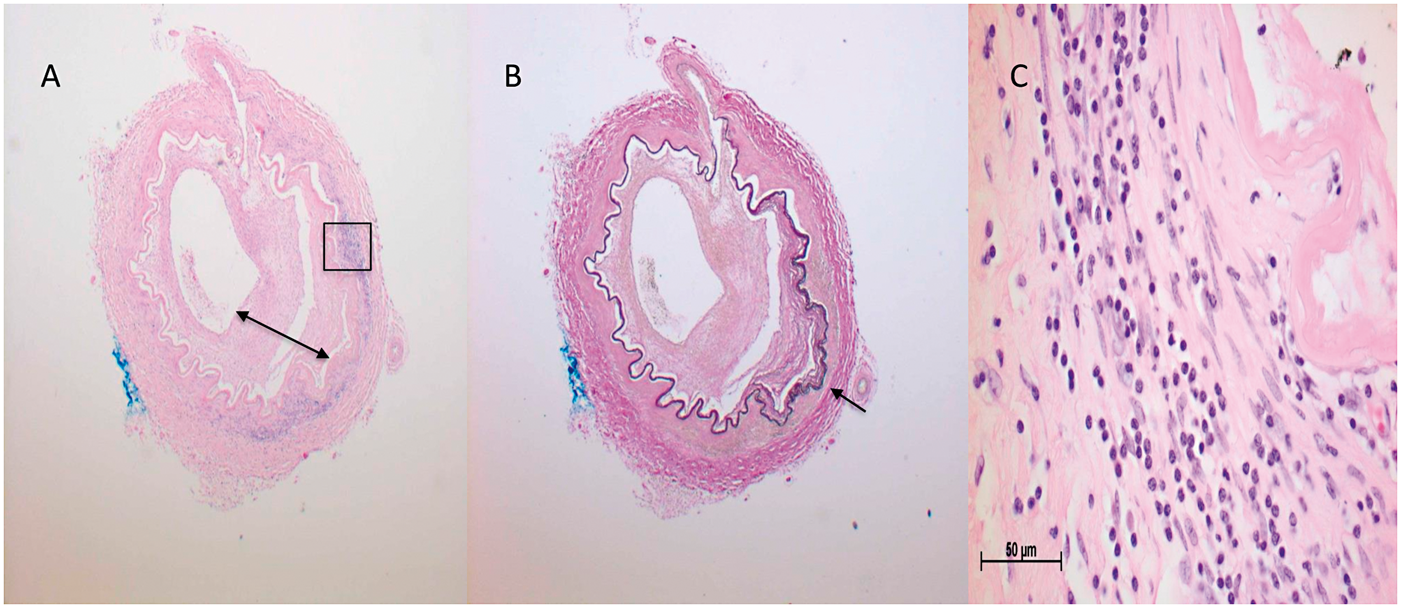
Patient 2
A 47-year-old male, with no medical history, suffered headaches and neck pain, followed several weeks later by fever (>38.5℃) and pain in his right eye. Four days after onset of fever, he suddenly developed a hemiparesis of the left side. In another hospital, he was treated with intravenous thrombolysis, followed by antiplatelet treatment. The symptoms gradually improved.
Two weeks later, he was readmitted because of severe headaches, drooping left corner of the mouth, an unstable gait and diplopia. MRI showed no new regions of infarction.
Despite treatment, cognitive impairment occurred during the following weeks. Antiplatelet treatment was replaced by a vitamin K antagonist after the MRI showed new lacunar infarctions.
When he presented to our hospital, neurological examination showed cognitive impairment and a slight drooping of the left corner of the mouth without any other neurological deficits.
The diagnostic work-up of this patient included a 3T MRI protocol containing standard anatomical and diffusion-weighted sequences and TOF-MRA, and an additional T1-weighted volumetric isotropically reconstructed turbo spin-echo acquisition (VIRTA) after contrast administration for assessment of vessel wall enhancement.4,5
Laboratory analysis showed blood cell counts, liver function, kidney function, infectious parameters, and several autoantibodies within normal ranges with the exception for rheumatoid factor which was slightly elevated (50 IU/ml). Serological tests for Borrelia, syphilis, HIV, Hepatitis C, HSV, VZV, EBV, and CMV were negative.
An MRA of the carotid arteries, PET-CT scan, electrocardiography and transesophageal echocardiography showed no abnormalities.
CSF examination showed 50 × 106/L leukocytes, a total protein concentration of 1.11 g/L, an IgG-index of 0.55, and negative oligoclonal banding. Cytological examinations were normal. Microbiological and serological studies were also normal.
MRA of the intracranial arteries showed multifocal narrowing of the distal carotid and the anterior, middle, and posterior cerebral arteries on both sides.
Subsequent MRI scans of the brain showed an increasing number of small deep bilateral infarcts in the basal ganglia area and in the right cerebellar hemisphere, and also one ischemic lesion in the right occipital cortex. Intra-arterial angiography showed multifocal segmental narrowing of the large and small vessels, suggestive of vasculitis.
Also, there was enhancement of the vessel walls of the affected arteries on both sides on a gadolinium-enhanced T1-weighted 3 Tesla MRI. The images were highly suggestive of cerebral vasculitis (Figure 3).
3T-MRI with vessel wall imaging using a T1 sequence after gadolinium administration showing enhancement of the intracranial arteries. (a) Coronal image showing enhancement of the right distal internal carotid artery (ACI) and the right proximal medial cerebral artery (MCA). (b) Transverse image showing diffuse enhancement of the right MCA and the left proximal anterior cerebral artery (ACA), proximal MCA, and distal ACI. (c) Transverse image showing enhancement of the left posterior cerebral artery (PCA).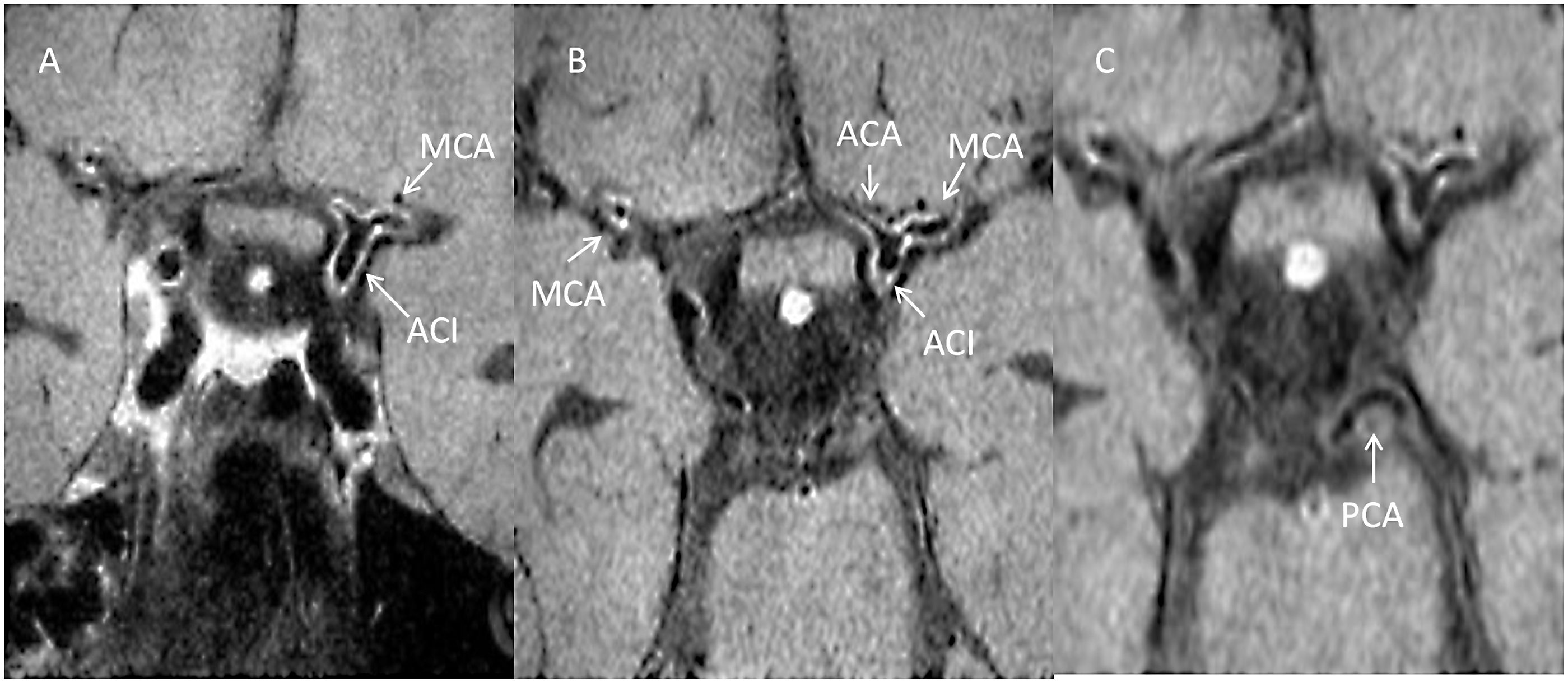
A brain biopsy was performed. Pathological examination showed no signs of vasculitis or other conditions.
The diagnosis of probable PCNSV was made, and the patient was treated with methylprednisolone and azathioprine. For three months, there were no new deficits, but the cognitive impairment remained unchanged. Subsequently, after an episode of short-lasting dysarthria, MRI showed a new lesion in the right caudate nucleus. Azathioprine was changed to monthly intravenous pulse treatment with cyclophosphamide for six months. No new clinical symptoms or radiological abnormalities have occurred since.
Conclusions
PCNSV is a rare condition with a significant mortality rate 2 and is often considered in the differential diagnosis of unexplained diseases of the CNS. In the diagnosis of PCNSV, brain biopsy is regarded as the gold standard, but it is an invasive procedure and it has a limited sensitivity due to sampling errors. 1 In both cases presented here, brain biopsies were inconclusive.
In PCNSV, a conventional MRI usually shows multiple infarctions and intracranial hemorrhages, whereas an MRI with gadolinium contrast may show small enhancing lesions in the parenchyma and leptomeninges in non-ischemic areas in 20% of cases. 2 A normal MRI of the brain can almost exclude PCNSV.2,3 With cerebral angiography, a multifocal pattern of narrowing and dilatation of the affected arteries may be seen, 3 but this pattern is not pathognomonic as it is also present in cases of intracranial atherosclerosis or reversible cerebral vasoconstriction syndrome (RCVS). 6 In biopsy-proven PCNSV, cerebral angiography was abnormal in 33–87%.2,3
Traditionally, PCNSV is subdivided into pathological categories or in biopsy-proven versus angiographically diagnosed PCNSV. 2 However, for clinical purposes, a distinction in suspected PCNSV predominantly affecting large vessels or predominantly affecting small vessels may be more suitable to guide ancillary investigations. In PCNSV involving the large arteries of the brain, MRI with VWI may be of great advantage in establishing the diagnosis, especially since biopsy sample errors in these patients may occur more frequently than in those with more superficially located involvement of small distal and meningeal arteries. 2
This study demonstrates that vessel wall enhancement on MRI that is suggestive of vasculitis of the large basal arteries of the brain is confirmed by postmortem pathology in the first patient, indicating the potential of this technique in diagnosing PCNSV. The second case showed similar vessel wall enhancement on MRI, which in addition to the comprehensive clinical data importantly contributed to the clinical diagnosis of PCNSV. Of note, in both cases, the results of a superficial brain biopsy were negative.
In the current literature, vessel wall enhancement is described in cases of PCNSV.6–9 However, to our knowledge, no cases report a pathological confirmation of the involved arterial segments showing enhancement on MRI with VWI. Importantly, RCVS, the most important mimic of PCNSV, does not show gadolinium enhancement on MRI with VWI. 6
For PCNSV with involvement of smaller distal arteries, the resolution of MRI with VWI is insufficient and brain biopsy will remain the most important diagnostic tool. However, if the large intracranial arteries are involved, MRI with VWI in patients suspected of PCNSV may substantially contribute to the clinical diagnosis.
Footnotes
Acknowledgment
We thank R. de Waal and R. Duijff for the referral of the patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
All authors contributed to this manuscript. JLM van Rooij contributed in literature search, designing figures, study design, data collection, data analysis, data interpretation and writing. DR Rutgers and WGM Spliet contributed in designing figures, data collection, data analysis, data interpretation and writing. CJM Frijns contributed in study design, literature search designing figures, data collection, data analysis, data interpretation and writing.