
Abstract
Post-stroke dysphagia (a difficulty in swallowing after a stroke) is a common and expensive complication of acute stroke and is associated with increased mortality, morbidity, and institutionalization due in part to aspiration, pneumonia, and malnutrition. Although most patients recover swallowing spontaneously, a significant minority still have dysphagia at six months. Although multiple advances have been made in the hyperacute treatment of stroke and secondary prevention, the management of dysphagia post-stroke remains a neglected area of research, and its optimal management, including diagnosis, investigation and treatment, have still to be defined.
Background
Stroke is recognized as a leading cause of death and disability worldwide and is associated with multiple medical complications leading to prolonged hospital admissions and significant health care costs. 1 Post-stroke dysphagia (PSD), defined here as difficulty in swallowing after a stroke, is a common complication affecting many patients in the first few hours and days after ictus. PSD is associated with increased mortality and morbidity due in part to aspiration, pneumonia, and malnutrition. Although many stroke patients recover swallowing spontaneously, 11–50% still have dysphagia at six months.2,3 Persistent dysphagia independently predicts poor outcome and institutionalization. 4 Dysphagia leading to aspiration of ingested foods, liquids, or oral secretions, is thought to be the primary risk factor for pneumonia after stroke. 5 Dysphagic patients are three times, and those with confirmed aspiration eleven times, more likely to develop pneumonia.1,6 A recent large retrospective US study of stroke patients quantified the individual cost of pneumonia and associated mortality as $21,338. The relative risk of hospital death in stroke patients with pneumonia is 5.7 (95% CI, 5.4–6.0). 5
Although multiple advances have been made in the hyper acute treatment of stroke (e.g. with thrombolysis, mechanical thrombectomy, and hemicraniectomy), and secondary prevention (antithrombotics, blood pressure lowering, lipid lowering), the management of PSD remains a neglected area of research. As such, the optimal management of PSD, including diagnosis, investigation and treatment, remains to be defined.
Epidemiology of PSD
Globally, 15 million people suffer a stroke annually 7 and up to 65% have swallowing problems of whom half will be symptomatic. 8 Some early studies included people with diagnosed dysphagia who were referred for further assessment and this increased artificially the rate of aspiration.9,10 The true prevalence of dysphagia can only be established by studying an unselected stroke population3,11 and there have been no such recent studies.
In acute stroke, the prevalence of dysphagia has been reported as between 28 and 65%,3,11–13 a variation that reflects differences in the assessment of dysphagia, setting, and timing of the test used. Dysphagia improves significantly during the early days and after two weeks 90% of patients swallow safely.3,8 although a small proportion will have problems for longer. 2 Further, some patients who appear to have a safe swallow at three months are found to have difficulties again at six.3,11 In general, if the swallow does not show any signs of recovery in the first 10 days after stroke, the return of a safe swallow may take up two or three months to show signs of recovery. 14
Aspiration in dysphagic patients is often not associated with a cough response or outward signs of difficulty in swallowing. This absence of any outward sign or distress is known as silent aspiration and has been reported as occurring in over 40% of patients. 15 Since there is an association between aspiration and abnormal pharyngeal sensation, with 8% of patients silently aspirating, 16 silent aspiration is considered to be related to sensory loss or gradual desensitization if aspiration is chronic. 17 Since 100% of dysphagic patients showed either unilateral or bilateral sensory loss in one study, and a sensory deficit exists in the pharynx and larynx in stroke patients with dysphagia, it has been concluded that the severity of laryngeal sensory deficits determines a predisposition to aspiration. 18
Mechanisms of PSD
PSD is thought to be due to damage to the cortex and subcortical structures. Cortical re-organization then leads to swallowing recovery. Studies using transcranial magnetic stimulation (TMS) have shown that pharyngeal musculature is represented bilaterally, but asymmetrically, in the cerebral cortex of healthy volunteers. 19 A stroke lesion affecting the “dominant swallowing hemisphere” may therefore be responsible for dysphagia following unilateral hemispheric stroke. 15
In an attempt to understand the mechanism for recovery of swallowing after stroke, swallowing was studied by videofluoroscopy (VFS) and TMS mapping over time in 28 hemispheric stroke patients. Subjects who were non-dysphagic after hemispheric stroke had greater pharyngeal cortical representation in the contralesional hemisphere as compared to dysphagic subjects. TMS follow-up data at one and three months indicated that subjects who recovered swallowing function had significantly greater pharyngeal representation in the unaffected hemisphere as compared to baseline. These findings suggest that re-organization in the contralesional hemisphere is key in swallowing recovery,
20
as illustrated in Figure 1.
Expansion of pharyngeal motor cortex on unlesioned hemisphere during swallowing recovery after stroke. Magnetic resonance image with co-registered topographic data from transcranial magnetic stimulation at baseline, one month, and three months after enrolment.
20
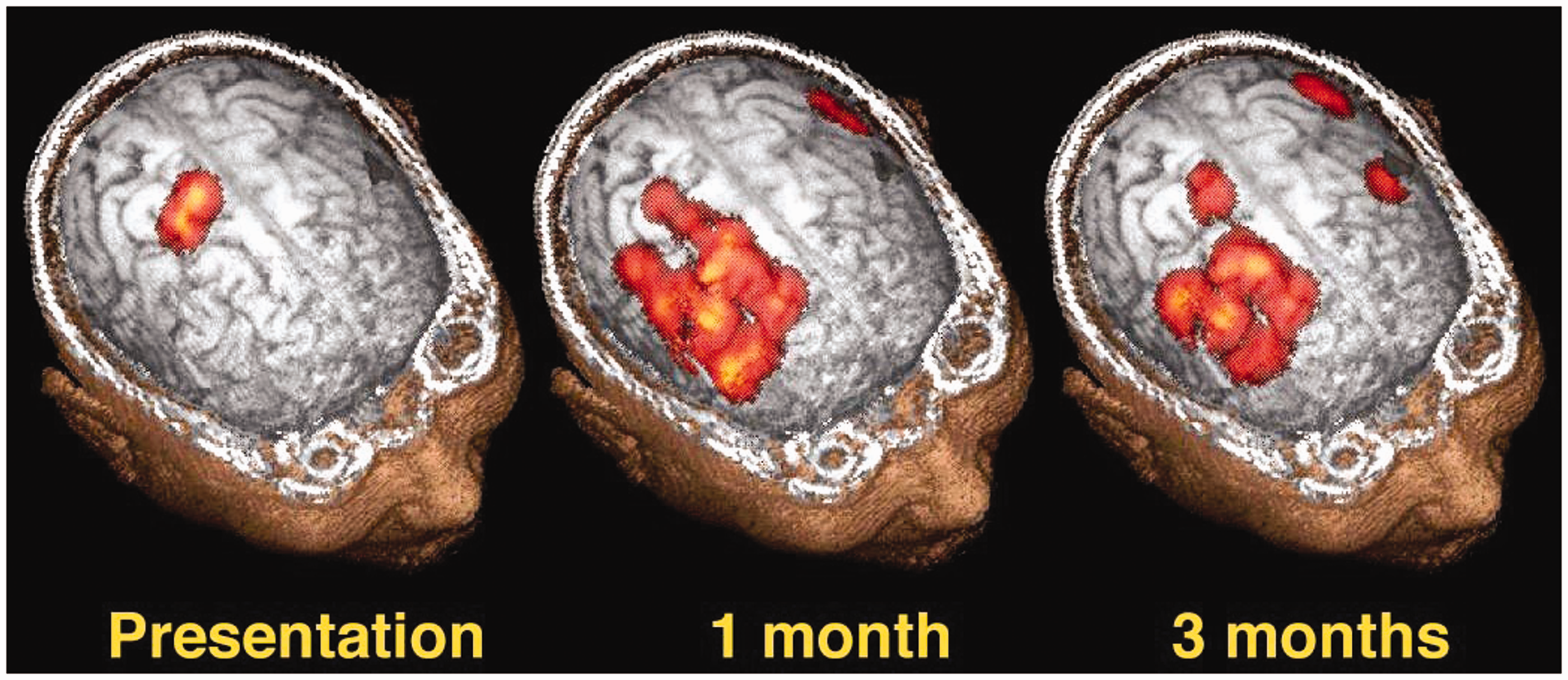
A recent functional magnetic resonance imaging study comparing cortical activations during swallowing between dysphagic hemispheric stroke patients and healthy subjects confirmed compensatory recruitment and activation of regions of the cerebral cortex in the intact hemisphere, supporting the theory that changes in the unaffected hemisphere are crucial in swallowing recovery. 21 Moreover, a magnetoencephalography (MEG) study imaged swallowing activations in subacute stroke patients with and without dysphagia compared with healthy controls described similar evidence for increased contralesional activity being predictive of no dysphagia. 22 Thus, neuroplasticity is likely to play a significant role in the recovery of swallowing function. 23
In addition to the neuropathophysiological changes described above, dysphagia will also occur when level of consciousness is reduced, either acutely due to a large stroke lesion with associated edema, or later due to delirium in which case the size and location of stroke will be less important.
Complications of PSD
Complications of dysphagia include the consequences of aspiration: pneumonia, recurrent cough, and choking, and those of modifications to dietary and fluid intake: compromised nutrition and hydration, reduced quality of life, and social isolation.
Pneumonia is a frequent complication of stroke, occurring in around 10% of hospitalized patients. 24 In those at greatest risk because of advanced age, severe stroke, and PSD, the incidence of pneumonia may be as high as 40%. 25 Confirmed aspiration is strongly associated with pneumonia (relative risk 11.56; 95% CI 3.36 to 39.77). 8 Current thinking recognizes the potential interplay between poor oral health, aspiration, and immune suppression in determining susceptibility to pneumonia. 26 Pneumonia most often presents in the first week after a stroke, probably because of the high prevalence of dysphagia and the extent of immune suppression during the acute phase. Nevertheless, the diagnosis of pneumonia complicating stroke remains challenging as its presentation may be non-specific and investigations such as chest radiography and microbiological specimens are of limited value. 27 This has significant implications for clinical care and research that considers pneumonia as a trial endpoint and recent consensus diagnostic criteria have been proposed to address this. 28
Patients developing pneumonia are more likely to die or survive dependent on others,24,29,30 and have a longer stay in hospital. As compared to alternative settings, care on a stroke unit compared to alternative settings reduces the frequency of pneumonia (odds ratio 0.60; 95% CI 0.42 to 0.87). 31 Little is known about the impact of particular care processes such as positioning, early swallow screening, and oral care practices. The time trend in pneumonia prevalence in stroke units is unclear, for example, one registry study suggested no significant change in pneumonia prevalence between 1998 and 2007. 32 Pneumonia remains an important and modifiable complication of stroke, and strategies to prevent it such as reducing aspiration could significantly improve outcomes.
Compromised nutrition, hydration, and poor quality of life caused by PSD have attracted less clinical and research attention than pneumonia. In a systematic review from 2009, the chance of malnutrition increased in patients with dysphagia particularly in the post-acute phase. 33 The conclusions were limited by widely varying definitions and prevalence of both dysphagia and malnutrition. The validity and utility of the available methods for assessing nutritional status in patients with stroke such as the Demiquet Index, anthropometry, and those for hydration status, are unclear and need further evaluation. Dysphagia-related quality of life tools such as SWAL-QUAL and SWAL-CARE are available 34 but these were not derived in patients with stroke and require evaluation in this setting.
Diagnosis: Clinical and instrumental
Dysphagia can be diagnosed by clinical bedside assessment (CBA), or instrumentally by VFS, or by fiberoptic endoscopic evaluation of swallowing (FEES). CBA consists of a detailed oral examination and an assessment with food and liquid to ascertain oral and pharyngeal competency. Several methodological variations have been reported. 35 CBA predicts pharyngeal dysphagia poorly and has been criticized for its inaccuracy in identifying aspiration,36,37 missing up to 40% of people who aspirate. 36
In hyperacute stroke studies, swallowing has been assessed using a water swallow test, a screening test rather than full assessment. 38 Many subsequent swallow screens have been based on this with or without a scoring mechanism.39–42 Some tests require specialist training or are copyrighted (e.g. TOR-BSST). 39 Assessment later after the stroke is more comprehensive but will detect fewer cases as swallowing improves or recovers.11,43 It is difficult to estimate how many patients simply have difficulty swallowing and how many are also aspirating as few studies have performed routine VFS in the first few days.
It is important to decide which aspect of swallowing, for example, clinical dysphagia or radiological aspiration, is the focus of study. This will determine the type of assessment required and the relevance to clinical practice. For example, it remains unclear whether a finding of asymptomatic aspiration on FEES is relevant or whether a minor tongue movement abnormality on clinical examination is important if it does not cause symptoms.
VFS is an instrumental assessment of swallowing and involves swallowing a radiological contrast agent such as barium. It is expensive as it needs a radiology suite and often a number of different staff. Many patients are too ill to travel to radiology and sit up for long enough to be assessed. It involves radiation exposure (although this is of less relevance to stroke patients) and is not readily repeatable. Hence, it is impractical to perform VFS in every case.
In FEES a laryngoscope is passed transnasally to the hypopharynx to view the larynx and pharynx. Food and drinks are dyed to aid visualization of the bolus. FEES allows an assessment of the anatomy, secretions and of food and drink management. Information is obtained on the ability to protect the airway, timing of the bolus through the hypopharynx and ability to clear the bolus during the swallow. It also allows the clinician to see pooling and residue in the hypopharynx and detect aspiration.44,45 The equipment is portable, sitting is not essential, and the procedure can be performed at the bedside. It is a repeatable, and safe allowing more swallows to be tested. Patients can be assessed while eating a full meal rather than with the limited number of spoonful’s of contrast given during VFS. However, FEES is not routinely available in many hospitals worldwide which, like VFS, limits the number of centers which could participate in research using it as an assessment.
VFS and FEES are considered interchangeable in clinical practice, especially when examining aspiration or penetration,45–50 and they are the only two assessments that can diagnose aspiration reliably. 51 VFS has been considered the gold standard for the diagnosis of dysphagia, but FEES is increasingly seen as a cost-effective, portable, and reliable alternative. 51 Validation of FEES against VFS showed high sensitivity and specificity.45,52,53 In one study FEES was shown to detect aspiration more reliably than VFS. 50 Other assessments, such as cervical auscultation or pulse oximetry are other potential approaches.
In conclusion, instrumental assessment is considered the gold standard in the diagnosis of dysphagia, but requires specialist staff and equipment and therefore cannot readily be conducted within a few hours of stroke onset, as would be needed in a study of early intervention. CBA is the only option in this situation but is not as reliable.
Dysphagia management
The primary aim of dysphagia management has been to reduce aspiration and to manage swallowing difficulties rather than rehabilitate the swallow. This is partly due to the heterogeneity of swallowing difficulties and developing knowledge of the normal and disordered swallow. Management includes modifying food and fluid, altering posture and changing swallowing strategies with some rehabilitative techniques. These may be used independently but are mostly used together. Management depends on whether the focus is on risk of aspiration or level of swallow breakdown and can be individualized.
Compensatory techniques support management of food and drink within a person’s current situation and reduce aspiration risk. They are short-term adjustments and may not improve the physiology of the swallow or promote neural network swallow recovery. Postural techniques (e.g. chin tuck) redirect the bolus and change pharyngeal dimensions. Compensatory swallow techniques such as the effortful swallow aim to increase the efficacy and safety of swallowing. There is some evidence of a reduction in aspiration with these techniques.54,55
Thickening liquids slow the bolus and increase bolus cohesion leading to a reduction in penetration and aspiration. 56 The quality and extent of modification of food and fluids are inconsistent and subjective as thickness of fluids depends on the base fluid, temperature, the individual making the drink, and the type of thickener, resulting in variability within and between patients. 57
Rehabilitation techniques such as oral and lingual exercises tend to focus on strength and endurance. 58 They result in an increase in isometric pressure, but are aimed at specific parts of the swallow so it is not clear how they generalize to the dynamic swallow. Other approaches report a more explicit focus on motor learning principles and the functional swallowing process. One of these with some evidence of effectiveness is the McNeill Dysphagia Therapy program. 59 More recently, neurostimulation techniques for rehabilitation have been employed, such as TMS, pharyngeal electrical stimulation (PES), and neuromuscular electrical stimulation; there is some evidence that these may reduce aspiration, pharyngeal residue, length of stay in hospital, and improved swallowing performance. 60 Recent reviews of dysphagia management report limited consistency of evidence for interventions, but with some evidence of effectiveness for behavioral interventions and PES on aspects of swallow and functional outcomes.55,61
Although there is little evidence for postural and compensatory techniques, these are widely but variably used leading to difficulties in establishing what “usual care” is in a research context. This could be addressed by cluster rather than patient level randomization. Issues around subjectivity of fluid modification can be addressed by using pre-thickened bolus which has been shown to be more consistent. 58
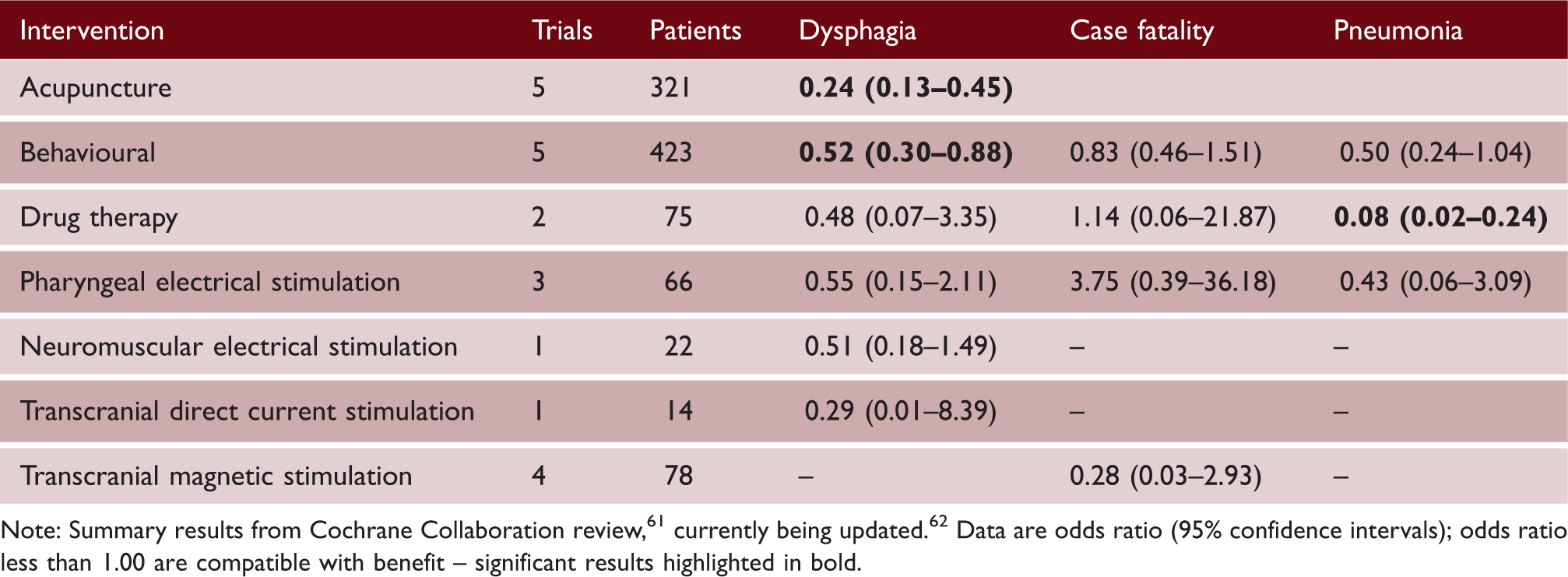
Medical treatment of dysphagia
Potential treatments for post-stroke dysphagia and their effects on important outcomes
Prevention of post-stroke pneumonia
Post-stroke pneumonia is due to a combination of dysphagia, aspiration, 8 and stroke-induced immunosuppression. 63 It can be caused by bacteria aspirated form the oropharynx or by the chemical effects of the gastric acid on the bronchial mucosa. 64 Prevention of pneumonia therefore includes early identification of dysphagia, interventions to reduce the volume and frequency of aspiration and the pathogenicity of the aspirate, enhancement of laryngeal sensation and protective mechanisms such as cough, and promotion of cortical plasticity to enhance recovery of the swallow.
Stroke unit care is associated with significant reductions in the incidence of pneumonia. 31 This is likely to be due to timely screening for dysphagia, modification of the consistency of diet and fluids and/or provision of enteral feeding65,66, and early mobilization.67,68 Pharmacologic approaches could further decrease the risk of pneumonia. Selective oral decontamination lowers oropharyngeal colonization with pathogenic Gram negative bacteria and was associated with a significant reduction in pneumonia in a study of 203 patients with acute stroke. 69 Prevention of vomiting and regurgitation is another promising approach, as stroke does not only cause dysphagia, but is also associated with lower esophageal sphincter dysfunction, gastro-paresis, increased gastric residual volume and gastro-esophageal reflux. 70 A recent randomized controlled study of the antiemetic agent metoclopramide in 60 patients with acute stroke fed via nasogastric tubes showed a 69% reduction in pneumonia with regular treatment. 71
Pneumonia after stroke could potentially be prevented by the use of prophylactic antibiotics. A Cochrane review of five studies including 506 patients demonstrated that prophylactic antibiotics significantly reduced post-stroke infection but had no effect on mortality. 72 Most of the included trials used broad-spectrum antibiotics, started within 24 h of stroke onset and continued for three to five days.73,74 While antibiotic prophylaxis prevented infections overall, there was no reduction in pneumonia. This was recently confirmed by two large randomized controlled trials. The Preventive Antibiotics in Stroke Study (PASS) randomized 2250 unselected patients with acute stroke patients to prophylactic ceftriaxone and reported an overall reduction in infections but no effect on pneumonia. 75 Similarly, the Stroke-Inf study, a cluster-randomized study including 1217 patients with acute ischemic stroke found no effect on pneumonia of prophylaxis based on co-amoxiclav and clarithromycin although urinary tract infection was reduced. 76 While antibiotic prophylaxis is clearly effective in the prevention of extra-pulmonary infections, there is now strong evidence form trials using a range of different antibiotics that such prophylaxis does not prevent pneumonia.
Cough is a well-known side effect of angiotensin converting enzyme inhibitors (ACEIs) and could potentially reduce pneumonia. This has only been tested in patients with chronic stroke, and effects appeared to be more pronounced in Asian than Caucasians, 77 a population that are more sensitive to ACE-I induced cough. Cilostazol, an antiplatelet agent with vasodilator effects has also been shown to reduce pneumonia in the chronic phase of stroke; the mechanism for this is unknown, but might involve bradykinin and substance P, as for ACEIs. 78 Excessive tracheobronchial sections (bronchorrhoea) have been described in posterior circulation strokes, and anticholinergic agents could reduce secretions and pneumonia in this group. 79
Pneumonia is an early complication of stroke, and usually associated with aspiration soon after the acute event. 80 The risk of aspiration declines within the first two weeks after stroke. 16 Therefore, prevention should be started early and continue over the first two weeks, the period when patients are most at risk of aspiration and pneumonia. As there is no agreed definition of post-stroke pneumonia, 28 comparison of the effectiveness of interventions aimed at prevention of pneumonia is difficult. Future studies should use agreed definitions. 27
Oral care
Poor oral care and dental hygiene increase risk of pneumonia, cause discomfort, and reduce quality of life after stroke. There are guidelines for best practice. 81 The majority of data, on which the recommendations are based, are from ventilated patients on intensive care units.82,83 Nursing home residents, people with dementia, or with learning difficulties are high-risk groups for poor mouth care. Poor dental hygiene is recognized as being associated with vascular disease and is more common in older people. It is likely that poor oral care is a cause for pneumonia in this group, particularly if there is also dysphagia and in individuals who are enterally fed (Beavan, Meagher & Robertson, unpublished).
Patients with neurodisability have difficulty undertaking their own oral and dental care due to physical, perceptual, and cognitive difficulties and therefore rely on help. They may be reluctant to ask for help, as oral care is not seen as a priority. 84 Lack of help is associated with poor oral and dental care.
The best way to deliver oral care is uncertain and practice varies widely. 81 Nurses worry about causing aspiration and therefore, although recommended, few use toothbrushes or toothpaste. Electric and suction toothbrushes are a potential option, but they are expensive and it is uncertain if they are of benefit after acute stroke. 85 The flora of the oral cavity is altered by the stroke itself, 69 by concurrent use of antibiotics, the development of candida infections, and by the build-up of oropharyngeal residues and dental plaque. The solutions used for oral care vary between units. The best agent to use in stroke patients is unclear but using some form of diluted chlorhexidine as part of an oral care regime, as in intensive care, may be beneficial. 82 The effectiveness and risks of pineapple juice (which contains sugar), artificial saliva and glycerin sticks are unclear. Glycerin sticks are discouraged as they may dry the mouth. The production and consistency of saliva may change post stroke and drying of the oral cavity may be affected by poor oral closure and positioning.
Patient and carer perspectives
When admitted to hospital following an acute stroke, patients and their relatives are often unaware that stroke can cause swallowing problems. They are frequently surprised, and distressed, when a “nil by mouth” order is placed until the swallow has been checked although this practice is evidence-based and supported by stroke guidelines. 86 This surprise is perhaps understandable as dysphagia is not a symptom a lay person would associate with stroke and does not feature in the act FAST campaign, even though dribbling saliva is common.
A swallow screen should be performed as early as possible in the person's assessment. If the swallow is considered unsafe, and the person is put “nil by mouth,” the patients’ and carers’ distress are frequently exacerbated. Further problems can ensue if no one who can do a more detailed assessment is available to say whether the patient must remain nil by mouth, or if they could manage a modified diet or fluids safely. Even a modified diet may cause further distress as it can be aspirated, causing coughing, or if the patient is unable to swallow it, collect in a cheek causing “pouching.” 87 Attention to oral care is particularly important in these patients for safety and because retained food debris can cause halitosis, causing further indignity and carer distress.
All staff working with stroke patients should have the knowledge and skills appropriate to their role in the pathway 88 including those for the detection and management of dysphagia and its complications. Inter-professional competences have been developed to inform the training and organization of teams in all aspects of dysphagia. 89 Implementation has the potential to reduce waiting times for swallowing assessments, improve patient’s safety at mealtimes, and optimizing dysphagia management, improving both patients and carers experience.
Training of carers in addition to training of staff is recommended because difficulties with swallowing may arise not only in hospital but also after discharge, and those in close contact with the patient have the unique opportunity to notice the signs: delayed cough after seemingly drinking competently. Patients are frequently distressed by the constant stream of saliva. Even if they are able to eat, patients may not eat in the presence of others because of failing to meeting other people's expectations of well-mannered behavior. This not only affects the patient but also their carers and friends. 90 Swallowing problems may persist long-term, and low mood and clinical depression may result. 91
Trial design considerations
Design considerations for future randomised controlled trials in the management of post-stroke dysphagia

DSRS: Dysphagia severity rating scale; EQ-5D: Euro-Qol 5 dimensions (from which health utility status can be calculated); FEES: fiberoptic endoscopic evaluation of swallowing; mRS: modified Rankin Scale; PEG: Percutaneous Endoscopic Gastrostomy; RIG: Radiologically Inserted Gastrostomy; VFS: videofluoroscopy.
Dysphagia-specific trial design considerations cover the type of intervention and outcomes. The primary outcome will depend on whether the trial is assessing primarily mechanisms (phase II) or efficacy (phase III or IV). Mechanistic studies need to focus on tolerability of the intervention and whether prognostic measures of aspiration (with assessment using FEES or VFS 96 ) and dysphagia (using a clinical scale such as the DSRS 60 ) are reduced. In contrast, phase III trials will need to assess real-world outcomes that may be dysphagia-related (such as pneumonia or need for PEG feeding) or functional (such as the modified Rankin Scale). Once the primary outcome is decided, an optimal method of analysis should be used to minimize sample size for a given power (with power typically set at 0.90); efficient statistical analyses can reduce sample size in stroke trials by 20–30%. 97
One caveat when considering the choice of primary outcome and its analysis is that treatment effects may move in opposite directions. For example, the large FOOD-2 trial of timing of tube feeding post stroke observed a non-significant reduction in death and non-significant increase in poor functional outcome (modified Rankin Scale 4 or 5). 98 (A similar divergence was seen in the CLOTS-3 trial of intermittent pneumatic compression stockings with less death but more severe dependency.99,100) The underlying issue is that effective treatment of stroke complications, such as dysphagia (or pulmonary embolism as in CLOTS-3), may reduce death but thereby create a surviving population of patients with severe stroke who have significant impairment and disability.
Ongoing studies as identified by electronic searches of WHO International Clinical Trials Registry, ISRCTN and Clinicaltrials.com databases.
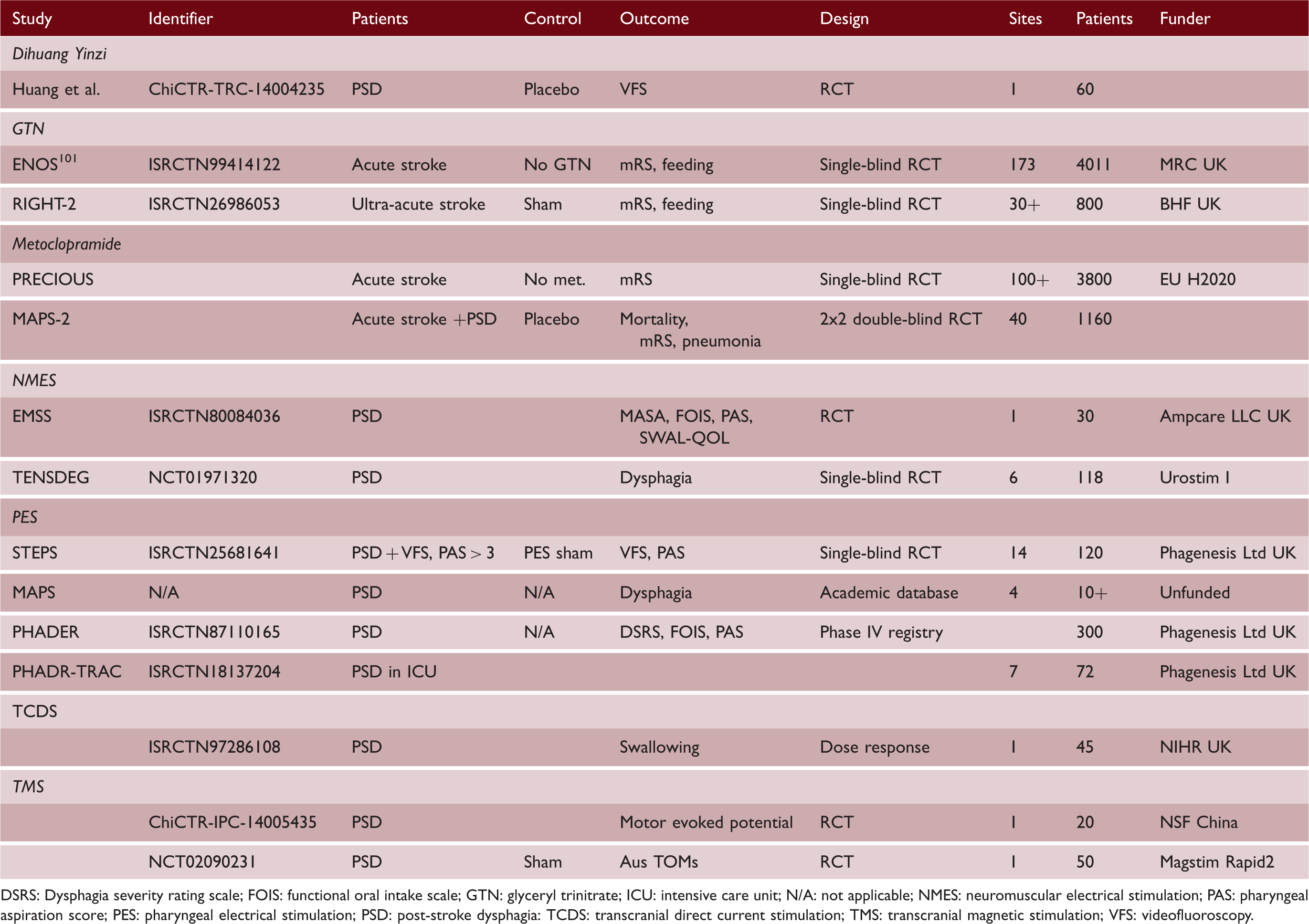
DSRS: Dysphagia severity rating scale; FOIS: functional oral intake scale; GTN: glyceryl trinitrate; ICU: intensive care unit; N/A: not applicable; NMES: neuromuscular electrical stimulation; PAS: pharyngeal aspiration score; PES: pharyngeal electrical stimulation; PSD: post-stroke dysphagia: TCDS: transcranial direct current stimulation; TMS: transcranial magnetic stimulation; VFS: videofluoroscopy.
Summary
The optimal diagnosis and treatment of PSD remain unclear and reported trials do not define optimal management. Ongoing studies may identify new strategies although their number is few. Nevertheless, their results, whether positive, neutral or negative, will help identify strategies that need testing or rejecting; if any trial is positive then a further one will probably be needed to validate the findings.
Footnotes
Acknowledgements
The UK NIHR Clinical Research Network, Stroke (formally Stroke Research Network, SRN) supports portfolio development workshops that bring together clinicians and researchers from multiple disciplines with the aim to develop high-quality clinical trials. The first of a two-part SRN funded workshop on PSD was held on 20 June 2014 in Nottingham UK. The meeting was attended by doctors, nurses, speech & language therapists (SLTs), clinical researchers and statisticians. The meeting aimed to summarize current knowledge on PSD and to establish how this might underpin development of future studies. The present report summarizes discussions at the meeting and is co-authored by meeting participants. It covers key PSD aspects including epidemiology, mechanisms, complications, diagnosis, patient and carer perspectives, therapy and medical treatment. A second workshop focused on design issues and outlined a potential academic protocol for a future trial in PSD. The SRN support covered travel and organization costs.We thank the UK Stroke Research Network, through Mrs Lucie Robinson, for supporting the workshop, Mrs Lauren Dunn for helping to organize the meeting, and Mr Wim Clarke for administering finances. PMB is Stroke Association Professor of Stroke Medicine.
Authors’ contributions
Each author individually wrote parts of the review. CR collated these and did initial editing with DC. PMB did final editing and submission.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PMB organized the NIHR SRN workshop; is senior author of a Cochrane review on PSD (see literature62,63); is Chief Investigator of the STEPS trial of PES (with funding by Phagenesis Ltd); has received honoraria and travel expenses from Phagenesis Ltd for his work on STEPS and PHADER; and coordinates the academic MAPS database of real-world use of PES. SH is inventor of PES, and owns stock in Phagenesis Ltd. PMB, CR, DLC, AW were Principal Investigators in the STEPS trial. PMB, CMcL have submitted clinical data to the MAPS database. PMB, SH, CMcL DS spoke at a Phagenesis Ltd-sponsored symposium and received travel expenses to attend. DLC has received travel expenses from Phagenesis Ltd.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.