
Abstract
The original version of this consensus statement on mechanical thrombectomy was approved at the European Stroke Organisation (ESO)-Karolinska Stroke Update conference in Stockholm, 16–18 November 2014. The statement has later, during 2015, been updated with new clinical trials data in accordance with a decision made at the conference. Revisions have been made at a face-to-face meeting during the ESO Winter School in Berne in February, through email exchanges and the final version has then been approved by each society. The recommendations are identical to the original version with evidence level upgraded by 20 February 2015 and confirmed by 15 May 2015. The purpose of the ESO-Karolinska Stroke Update meetings is to provide updates on recent stroke therapy research and to discuss how the results may be implemented into clinical routine. Selected topics are discussed at consensus sessions, for which a consensus statement is prepared and discussed by the participants at the meeting. The statements are advisory to the ESO guidelines committee. This consensus statement includes recommendations on mechanical thrombectomy after acute stroke. The statement is supported by ESO, European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), and European Academy of Neurology (EAN).
Methods
The Karolinska Stroke Update (KSU) consensus conferences take place every second year since 1996. From 2014, this is an official European Stroke Organisation meeting (ESO-KSU). The ESO-KSU program committee approves the final program. The core of the program is formed by consensus sessions, each dedicated to a topic within clinical stroke research with recent study results.
The participants in the consensus session prepare a draft consensus statement, coordinated by the session chairpersons and secretary. For the thrombectomy consensus session 2014, the secretary performed a Pubmed search for “mechanical thrombectomy and stroke”, “endovascular treatment of stroke”, “neurointervention” and others, as a basis for the draft statement. The draft circulated between the participants providing additional information on literature reviews and new publications. The draft was finally confirmed at a face-to-face session the afternoon before the start of the meeting and then discussed and modified at the meeting.
Since the participants at the Karolinska Stroke Update conference 2014 were aware of that several randomized studies on mechanical thrombectomy were about to be published within the next few months, it was decided that the session participants and the conference secretariat should revise the statement when relevant, based on the new reports. Since representatives of several professional organizations participated at the conference, the statement was also reviewed and agreed upon by these organizations.
New evidence since Karolinska stroke update 2012
Since the previous Karolinska stroke update consensus statement on mechanical thrombectomy 2012 results from randomized clinical trials and other retrospective cohort studies were made available as follows:
Large meta-analysis from randomized clinical trials of intravenous thrombolysis (IVT)
A recently published meta-analysis of individual patient data from 6756 patients in nine randomized trials comparing intravenous thrombolysis (IVT) with alteplase versus placebo or open control showed that alteplase significantly improves functional outcomes when delivered within 4–5 h of stroke onset, with earlier treatment associated with bigger proportional benefits (OR 1·75, 95% CI 1·35–2·27), thus emphasizing the need for preventing delays in acute stroke treatment. 1
Clinical trials on mechanical thrombectomy
Older generation devices and first use of stent retrievers
Three trials evaluating endovascular therapy, published in 2013, IMS III, MR RESCUE and SYNTHESIS, reported neutral results on clinical outcome. Possible explanations for failure to demonstrate superiority of endovascular therapy were long delay between symptom onset and treatment, inadequate patient selection, less than desired recanalization rates and use of older generation devices. IMS III showed no difference in safety and clinical outcomes compared to IVT but used six different procedural techniques with only four patients being treated with the new generation stent retrievers. 2 A subgroup analysis of IMS III showed that 48.2% of the patients were functionally independent at follow-up, corresponding to a modified Rankin score (mRS) 0–2 when recanalization to modified thrombolysis in cerebral infarction (mTICI) score 2b/3 was achieved (for internal carotid artery (ICA) occlusions 37–42% and proximal middle cerebral artery (MCA) (M1) occlusions 44%), 3 emphasizing the importance of recanalization of proximal occlusion. Importantly, IMS III demonstrated that a delay in time to reperfusion was associated with lower likelihood of good clinical outcome. 4 MR RESCUE allowed procedures up to 8 h based on penumbral imaging but used previous generation MERCI or Penumbra devices achieving mTICI 2b/3 recanalization rates of 67%. 5 The SYNTHESIS EXPANSION trial also used very few stent retrievers. 6 However, regarding safety, these trials showed similar rates of symptomatic intracranial hemorrhage (SICH) compared to IVT and even equivalence/superiority of IVT for minor stroke and stroke without large vessel occlusion on imaging. 7
In the meantime, evidence for the efficacy and safety of stent retrievers in mechanical thrombectomy continued to grow from non-randomized studies. The solitaire flow restoration thrombectomy for acute revascularization (STAR) study was an international, multicentre, prospective, single-arm study of the Solitaire™ device in 202 patients with large vessel occlusion of the anterior circulation within 8 h of onset. It reported a 79% rate of successful revascularization, 57.9% of mRS 0-2, 1.5% SICH and 6.9% mortality. Support for stent retrievers was further gathered in a 2013 pooled analysis of 19 studies using the Trevo™ (n = 221) or Solitaire™ (n = 355) devices, showing mTICI 2b-3 scores in 83 and 82%, hemorrhage in 8 and 6%, device complications in 5 and 6%, good functional outcomes in 51 and 47% of the patients with similar times to recanalization and with a mortality of 31 and 14%, respectively. 8
Stent retrievers in recent randomized controlled trials
Two smaller phase IIb randomized controlled studies compared stent retrievers with the original MERCI™ device (see also thrombectomy consensus statement from the 2012 KSU meeting):
The
The
Recent randomized controlled trials of endovascular therapy vs. standard treatment (trials published 2015)
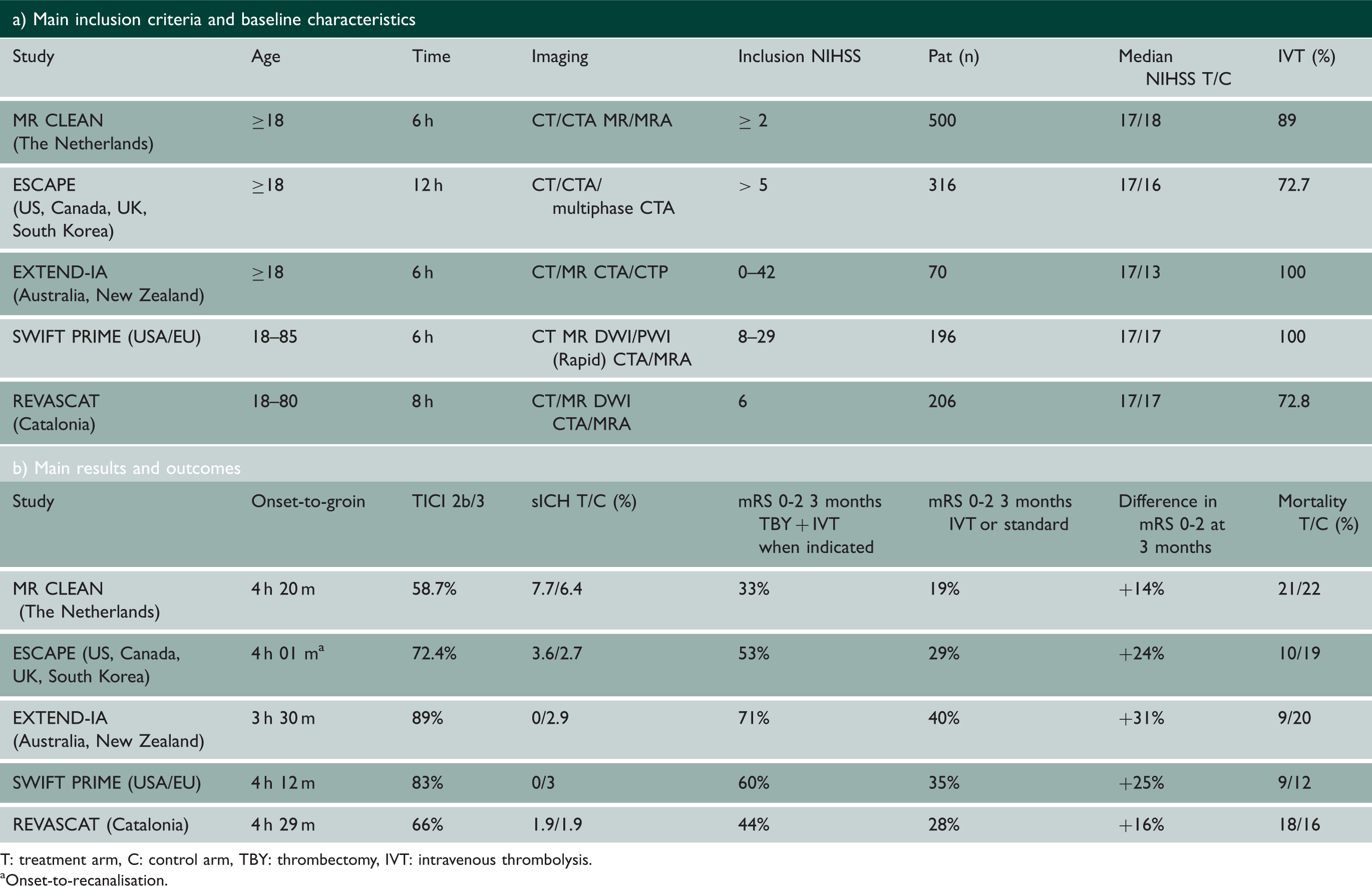
T: treatment arm, C: control arm, TBY: thrombectomy, IVT: intravenous thrombolysis.
Onset-to-recanalisation.
The
Secondary outcome parameters (National Institutes of Health Stroke Scale (NIHSS) score at 24 h and 1 week, recanalization at 24 h and final infarct at 1 week) were all indicating statistically significant favoring of the intervention group. Treatment effect was consistent in all pre-defined subgroups.
The
The
The
The
Two further randomized controlled trials compared endovascular therapy with usual therapy only; results to be published
In the THRACE trial (Trial and Cost Effectiveness Evaluation of Intra-arterial Thrombectomy in Acute Ischemic Stroke), patients receiving intravenous thrombolysis within 4 h were randomized to mechanical thrombectomy within 6 h with any approved device in France vs. no further treatment. The trial was halted after the second intermediate analysis of 395 patients. The results presented recently showed a reduction of disability in 12.1% with an independent functional outcome (mRS 0-2) in 42.1% after IV thrombolysis alone and 54.2% after IV thrombolysis and mechanical thrombectomy and lend further strong support for adding mechanical thrombectomy in selected patients. 16
The THERAPY-trial (THE Randomized, concurrent controlled trial to Assess the Penumbra sYstem’s safety and effectiveness in the treatment of acute stroke) compared IV thrombolysis alone with added thrombus aspiration with the Penumbra™ system within 6 h. Because of the positive mechanical thrombectomy trials, THERAPY was halted after 108 randomized patients. Preliminary results were presented recently and the intention to treat analysis showed a strong trend for benefit with this intervention. 17
In summary, there is very good evidence for early thrombectomy with stent retrievers. There is good evidence to favor stent retrievers over the MERCI™ device. At this moment, only limited data on other types of recanalization devices such as the Penumbra™ system are available. 18 Given the variable success rates and clinical outcomes with different recanalization devices in randomized trials, generalizability of all transvascular approaches cannot be assumed.
Meta-analysis of thrombectomy vs. standard treatment
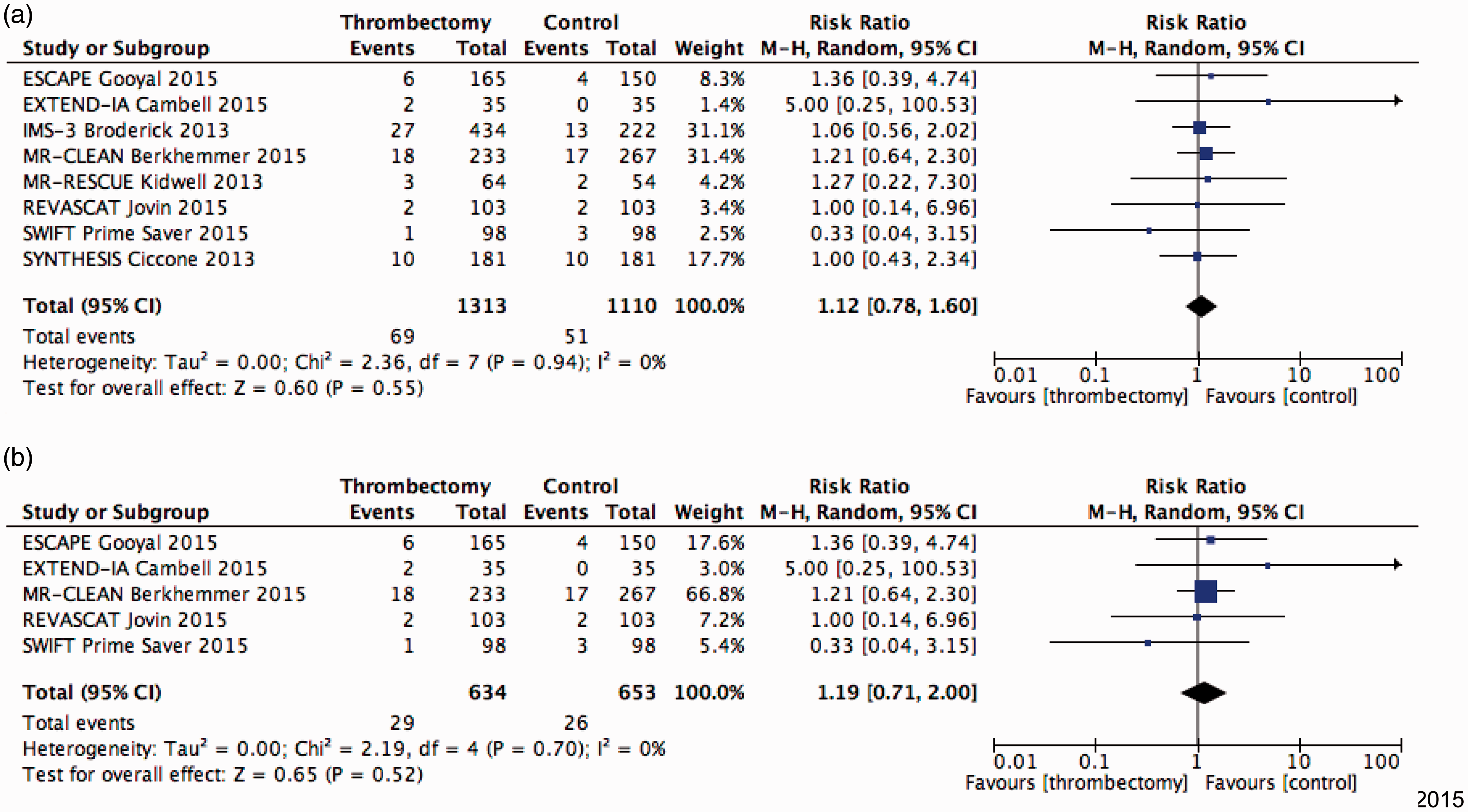
A meta-analysis of recent large trials comparing acute thrombectomy with no further treatment in patients with acute ischemic stroke and (suspected or documented) large intracranial artery occlusions was also performed by one of the authors (TS). Large randomized controlled trials with results published in peer-reviewed journals over the last three years were included. In a first analysis, all trials where included, and in a second, only the recent ones (published in 2015) were used where stent retrievers were the predominant thrombectomy method. Analysed outcomes were favourable outcome defined as an mRS 0-2 at 90 days, mortality at 90 days and symptomatic hemorrhage as defined by each study group. ORs and 95% CIs of the intention-to-treat analyses were calculated for each outcome using the Mantel-Haenszel method with random effects. Heterogeneity between trials was assessed by several methods. All analyses were performed with Review Manager (Version 5.2.6). Results are shown in Figures 1 to 3. Adding thrombectomy did not change the examined outcomes, except that favorable three months outcome was significantly better (OR 2.29, CI 1.82–3.18) in recent thrombectomy trials.
Endovascular vs. standard treatment or/and IVT outcome: mortality (day 90) (a) Only 2015 trials; (b) all trials. Endovascular vs. standard treatment or/and IVT outcome: symptomatic ICH; (a) Only 2015 trials; (b) all trials.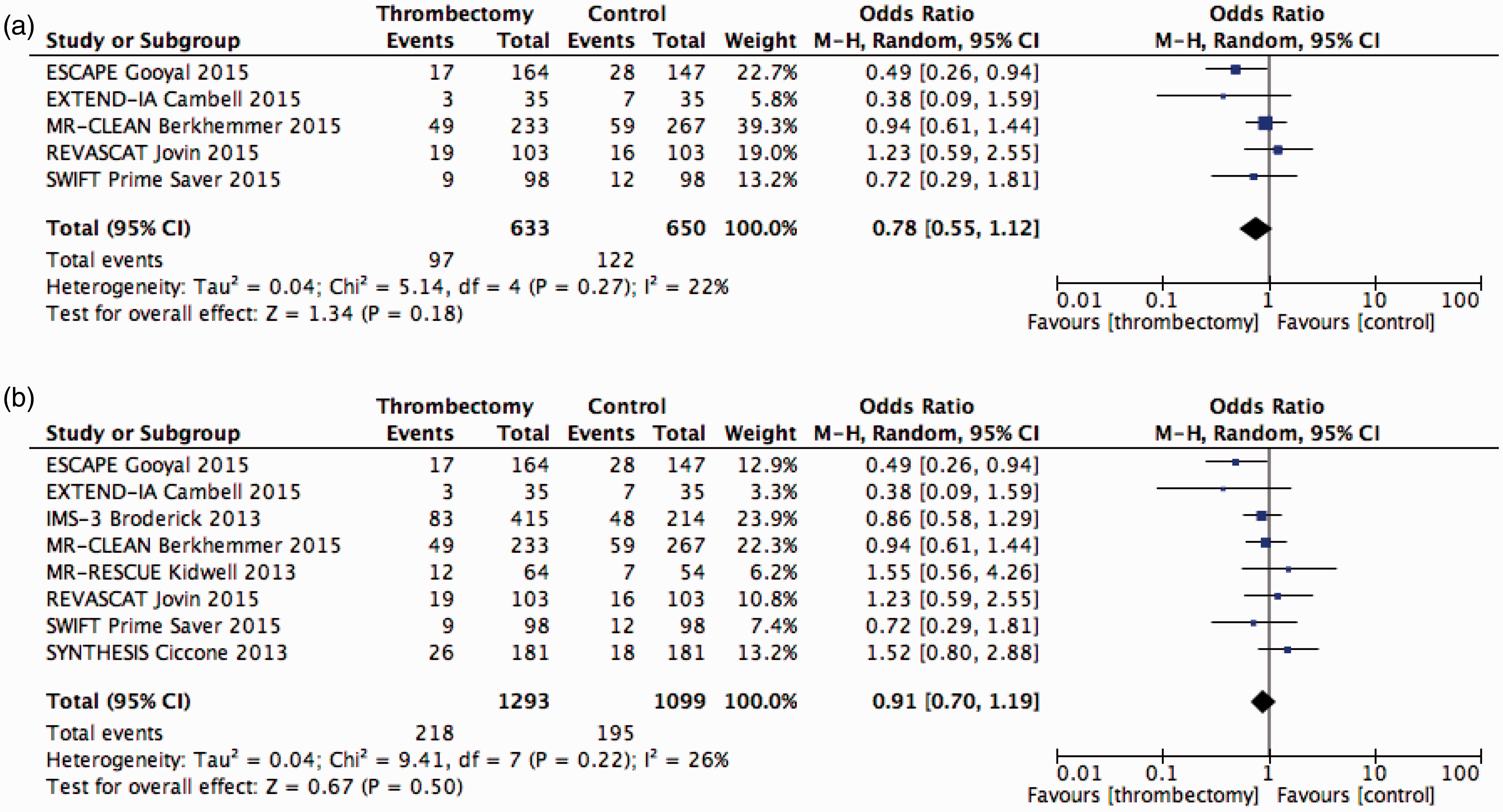
Aspects to be considered in mechanical thrombectomy
Mechanical thrombectomy in single centre cohorts: Outcomes and risk factors
A recently published single-centre series of 240 patients treated from 2005 to 2011 with mechanical thrombectomy alone or in addition to IVT (40%) (initially using MERCI™ and later on stent retrievers) achieved 50% mRS 0-2 at three months and reported 4.6% of SICH. 19
In a retrospective single-centre cohort of 176 consecutive patients focusing on complications of mechanical thrombectomy, it was shown that prolonged endovascular procedure beyond 1 h was associated with higher complication rates (such as SICH, embolism to new territories, dissection, vasospasm, stent dislocation/occlusion, cumulative 11% rate), but that the overall rate of SICH (5%) was comparable to IVT. 20 Post interventional subarachnoid hyperdensities were not shown to influence outcomes. 21
Mechanical thrombectomy in elderly patients
In MR CLEAN, 16% of the patients were 80 years or older; there was a positive treatment effect in this subgroup. This effect was significant and its size not different from the main effect size (OR 3.24, 95% CI 1.21–8.62). 10 Similarly, both randomized trials ESCAPE and SWIFT PRIME (in the latter with upper age limit of 80 years old) showed benefit for all subgroups including the elderly, who should thus be considered for thrombectomy.11,12 Previously, mortality in patients undergoing thrombectomy over 80 years of age was reported to be double that for younger patients in a large multicentre retrospective analysis in the US (9300 patients, of which 18% were above 80). However, the analysis period was restricted to 2008–2010, the type of device used was not mentioned and treatment effect could not be assessed. 22 Almekhlafi et al. 23 used the SPAN-100 index (i.e. positive index if age + NIHSS score = 100 or more) and found lower proportions of favorable outcome in the patients with positive (61%) compared to negative SPAN index (27%, OR 0.3; 95% CI 0.1-0.9), with 60% of positive SPAN index being 80 years of age and older. For the vertebrobasilar circulation, a retrospective analysis from a US nationwide database from 2006 to 2010 showed that age had an impact on in-hospital mortality of patients undergoing mechanical thrombectomy (n = 631) but not IVT (n = 1554), in particular those 65 years of age or older (43 vs. 23%). However, the types of devices used during that period were not reported. 24
Time to treatment and reperfusion
The positive effect in the MR CLEAN trial was time dependent, with acOR decreasing from 3.0 (95% CI: 1.6–5.6) at 3.5 h onset to reperfusion time, to 1.5 (95% CI: 1.1–2.2) at 6 h. 25 Treatment effect was not statistically significant anymore when reperfusion was achieved after 6 h 19 m. The benefit of thrombectomy was also shown to be time dependent in IMS III, where increased time to reperfusion was associated with a decreased probability of good functional outcome (adjusted relative risk for every 30-min delay 0·88, 95% CI 0·80–0·98). 4 Based on IMS III results and literature review, a cutoff of 347 min (5 h 47 m) for superiority of endovascular procedure over IVT alone was recently suggested, 26 and a first statistical review of published randomized controlled trials suggested a lower rate of good functional outcome (mRS 0-2) if stroke onset to reperfusion time exceeds 5–6 h. 27 These findings underline the necessity to treat as early as possible, and justify the time window of treatment within 6 h from symptom onset.
In the ESCAPE trial, however, 49 (15.5%) patients were included beyond 6 h, and treatment effect was not different but more advanced imaging (multiphase CTA) for inclusion in the trial was used. Also REVASCAT allowed inclusion up to 8 h. 14 This leaves room to investigate the possibilities of expanding the treatment time window for a selected group based on advanced imaging.
Tandem pathology
In the MR CLEAN trial, 146 (29%) patients had an additional extracranial ICA occlusion (tandem pathology), with treatment effect in favor of thrombectomy (OR 1.43, 95% CI 0.78–2.64). 10
In a systematic review of 32 studies including 1107 patients with intra and/or extracranial ICA occlusions, intra-arterial thrombolysis was compared with any kind of mechanical treatment and/or stent placement. Only studies with clinical outcomes reported beyond 30 days were included, ICA occlusions caused by dissection were excluded. Acute stenting of occlusions of the extracranial ICA resulted in a higher recanalization rate (87% vs. 48%, p = 0.001) and favorable outcomes (68% vs. 15%, p < 0.001) as well as lower mortality (18% vs. 41%, p = 0.048) when compared to intra-arterial thrombolysis. 28
Recently published cohort studies indicate that tandem stenosis/occlusions of the ICA/MCA can be treated with acute stenting of the extracranial internal carotid and stent retriever mechanical thrombectomy in the MCA with a reasonable risk profile.29–33 However, further evaluation of this treatment strategy is warranted.
Basilar artery occlusion
Despite high mortality and morbidity rates associated with basilar artery occlusion, 34 evidence from RCT’s on the effect of endovascular treatment is lacking. A recent meta-analysis of 45 observational studies (n = 2056) of reperfusion vs. no reperfusion of acute basilar occlusion showed NNT of 3 and 2.5 to decrease death or dependency and death alone, respectively. 35
Single-centre studies with samples less than 100 patients have shown good functional outcomes following thrombectomy of the basilar artery, ranging from 30%36,37 to 48%.38–40 Experience at the Karolinska Hospital showed a 57% rate of good functional outcome (95% CI 37% to 75%), and of 73% (95% CI 50% to 89%) when there were no signs of acute infarction prior to treatment, with about 21% mortality. 41
Recanalization rates over 75% were reported with new generation devices37,42 as well as with older generation devices in the MERCI and multi-MERCI trials but with lower benefit. 43
A previous prospective registry, the Basilar Artery International Cooperation Study (BASICS) could not demonstrate superiority of endovascular therapy against IVT; however, it employed mostly older-generation devices. 44 The same investigators are now undertaking the BASICS treatment randomized trial, comparing thrombectomy <6 h in addition to IVT with IVT alone.
Anesthesia in mechanical thrombectomy
Conscious sedation has gained support from a retrospective analysis of patients receiving either general anesthesia or conscious sedation (n = 507 in both groups, 1:1 matching). Patients receiving general anesthesia had significantly more in-hospital mortality (25%) and pneumonia (17%) compared to patients receiving conscious sedation (12% and 9.3%, OR 2.37 and 2.0, respectively) but similar rates of SICH. 45 A recent mini review from Takahashi et al. 46 also supports conscious sedation. Previous single-centre cohort studies47,48 and a review of five such studies 49 have reported similar findings. The post-hoc analysis of the thrombectomy patients in MR CLEAN showed better functional three months outcome in the absence of general anesthesia, but patients were not randomized to the type of anesthesia. 50 The issue of general anesthesia vs. sedation is currently studied in four randomized trials (ANSTROKE, COMET, GOLIATH and SIESTA).51–54
An expert consensus statement of the Society of Neurointerventional Surgery and the Neurocritical Care Society recommends the use of general anesthesia for patients with severe agitation, low level of consciousness (GCS < 8), loss of airway protective reflexes, respiratory compromise and in selected posterior circulation stroke presenting with these features. 55
Prehospital patient selection for immediate transfer to centers with multimodal imaging and availability of thrombectomy
A recently published SITS registry study found NIHSS scores of 11 and 12 points as predictors of baseline vessel occlusion and functional independence at three months in a cohort of 11,632 patients treated with intravenous thrombolysis with available baseline imaging data and three month functional outcome. 56 Moreover, if imaging was performed 3 h after stroke onset, NIHSS scores thresholds decreased to 9 and 10 points in predicting baseline vessel occlusion and functional independency at three months, respectively. Higher NIHSS scores predicted large vessel occlusion and functional dependence after three months if treated with intravenous thrombolysis. These results are in line with an initial single-centre retrospective study of 162 patients showing that an NIHSS score of 10 or more points up to 6 h after stroke onset increased by 16.9-fold the odds of unfavorable outcome or death (p = 0.013), and by 7.13-fold the odds of proximal vessel occlusion (p = 0.013 and p < 0.038, respectively; sensitivity, 83%; specificity, 78%). 57
Imaging-guided patient selection
Discussion regarding ongoing and future studies on mechanical thrombectomy
The recent results from several randomized controlled studies could potentially influence patient recruitment in ongoing RCT’s such as PISTE 64 or BASICS. 65 Until steering committees of the respective trials have halted the trial, randomization should be continued to help answer uncertainties of benefit and risk from thrombectomy in acute ischemic stroke.
Studies comparing active centres (IVT + possibility for thrombectomy) with control centres that do not yet have access to thrombectomy (IVT treatment alone), e.g. SITS-OPEN, 66 should continue its recruitment to strengthen the level of evidence. There are many reasons to recommend this approach such as the need for confirmatory studies, the desirability of narrowing the confidence interval to get a tighter estimate of the effect size for health economic reasons and the necessity for a wide range of data allowing subgroup analysis with adequate power. This type of design will also test thrombectomy in standard clinical practice in experienced centres.
In addition, it is desirable that all patients undergoing some form of acute revascularization therapy (IVT, mechanical thrombectomy, etc.) are prospectively included in registries (e.g. SITS-ISTR 67 or SITS-TBY 68 ) to ensure further evidence from routine clinical practice data.
Consensus statements of the ESO-Karolinska Stroke Update 2014/2015, Supported by ESO, ESMINT, ESNR and EAN
Prepared in November 2014, updated and released on 20 February 2015, after the International Stroke Conference, reconfirmed 15 May 2015
(Sources: Karolinska Stroke Update level of evidence for treatment recommendation: Appendix 1; Oxford Evidence-based level of evidence: Appendix 2)
Treatment recommendations
Mechanical thrombectomy, in addition to intravenous thrombolysis within 4.5 h when eligible, is recommended to treat acute stroke patients with large artery occlusions in the anterior circulation up to 6 h after symptom onset (Grade A, Level 1a, KSU Grade A). – new Mechanical thrombectomy should not prevent the initiation of intravenous thrombolysis where this is indicated, and intravenous thrombolysis should not delay mechanical thrombectomy (Grade A, Level 1a, KSU Grade A). – changed Mechanical thrombectomy should be performed as soon as possible after its indication (Grade A, Level 1a, KSU Grade A). For mechanical thrombectomy, stent retrievers approved by local health authorities should primarily be considered (Grade A, Level 1a, KSU Grade A). – new Other thrombectomy or aspiration devices approved by local health authorities may be used upon the neurointerventionists discretion if rapid, complete and safe revascularisation of the target vessel can be achieved (Grade C, Level 2a, KSU Grade C) – new If intravenous thrombolysis is contraindicated (e.g. Warfarin-treated with therapeutic INR) mechanical thrombectomy is recommended as first-line treatment in large vessel occlusions (Grade A, Level 1a, KSU Grade A) – changed and updated level of evidence. Patients with acute basilar artery occlusion should be evaluated in centres with multimodal imaging and treated with mechanical thrombectomy in addition to intravenous thrombolysis when indicated (Grade C, Level 4, KSU Grade C); alternatively they may be treated within a randomized controlled trial for thrombectomy approved by the local ethical committee – new The decision to undertake mechanical thrombectomy should be made jointly by a multidisciplinary team comprising at least a stroke physician and a neurointerventionist and performed in experienced centres providing comprehensive stroke care and expertise in neuroanaesthesiology (Grade C, Level 5, GCP, KSU Grade C). Mechanical thrombectomy should be performed by a trained and experienced neurointerventionist who meets national and/or international requirements (Grade B, Level 2b, KSU Grade B) – changed in level of evidence. The choice of anaesthesia depends on the individual situation; independently of the method chosen, all efforts should be made to avoid thrombectomy delays (Grade C, Level 2b, KSU Grade C) – changed.
Patient selection
Intracranial vessel occlusion must be diagnosed with non-invasive imaging whenever possible before considering treatment with mechanical thrombectomy (Grade A, Level 1a, KSU Grade A) – new. If vessel imaging is not available at baseline, a NIHSS score of ≥ 9 within three, and ≥ 7 points within 6 h may indicate the presence of large vessel occlusion (Grade B, Level 2a, KSU Grade B) – new. Patients with radiological signs of large infarcts (for ex. using the ASPECTS score) may be unsuitable for thrombectomy (Grade B, Level 2a, KSU Grade B) – new Imaging techniques for determining infarct and penumbra sizes can be used for patient selection and correlate with functional outcome after mechanical thrombectomy (Grade B, Level 1b, KSU Grade B) – new. High age alone is not a reason to withhold mechanical thrombectomy as an adjunctive treatment (Grade A, Level 1a, KSU Grade A) – new.
Recommendation for implementation, registries and further trials
Health authorities are strongly encouraged to implement access to thrombectomy within a reasonable time range in a network including stroke centres. Access to thrombectomy should be organised in a way that time between symptoms onset and to thrombectomy is minimised and that adequate competence within neurointervention, neurology, neuroradiology, neurosurgery and neuroanaesthesiology is provided. – new. It is encouraged to perform and include patients in RCT addressing unresolved thrombectomy questions such as thrombectomy for basilar artery occlusion, treatment in a late und unknown time windows, treating patients with imaging findings not sufficiently covered in recent trials, comparing new devices with widely-used stent retrievers, thrombectomy with or without intravenous thrombolysis, and different types of anaesthesia. – new. Non-randomized trials comparing centres not yet having access to mechanical thrombectomy with others should continue (such as SITS OPEN) – new. Ischemic stroke patients undergoing any type of acute revascularization treatment should be included systematically in national or international registries (such as SITS or SITS-TBY) – new.
Organisations represented by the authors
Nils Wahlgren, Tiago Moreira, Patrik Michel, Thorsten Steiner, Olav Jansen, Christophe Cognard, Heinrich P Mattle, Wim van Zwam, Staffan Holmin, Turgut Tatlisumak, Jesper Petersson, Valeria Caso, Werner Hacke: European Stroke Organisation-Karolinska Stroke Update (ESO-KSU) consensus conference Nils Wahlgren, Tiago Moreira, Patrik Michel, Thorsten Steiner, Christophe Cognard, Heinrich P Mattle, Turgut Tatlisumak, Valeria Caso, Werner Hacke, Mikael Mazighi, Marcel Arnold, Urs Fischer, Jens Fiehler, Jan Gralla, Kennedy R Lees: European Stroke Organisation (ESO) Christophe Cognard, Istvan Szikora, Laurent Pierot, Jens Fiehler, Jan Gralla, Olav Jansen: European Society of Minimally Invasive Neurological Therapy (ESMINT) Jens Fiehler, Jan Gralla, Olav Jansen: European Society of Neuroradiology (ESNR) Franz Fazekas: European Academy of Neurology (EAN)
Endovascular vs. standard treatment or/and IVT outcome: mRS 0-2 (day 90) (a) Only 2015 trials; (b) all trials.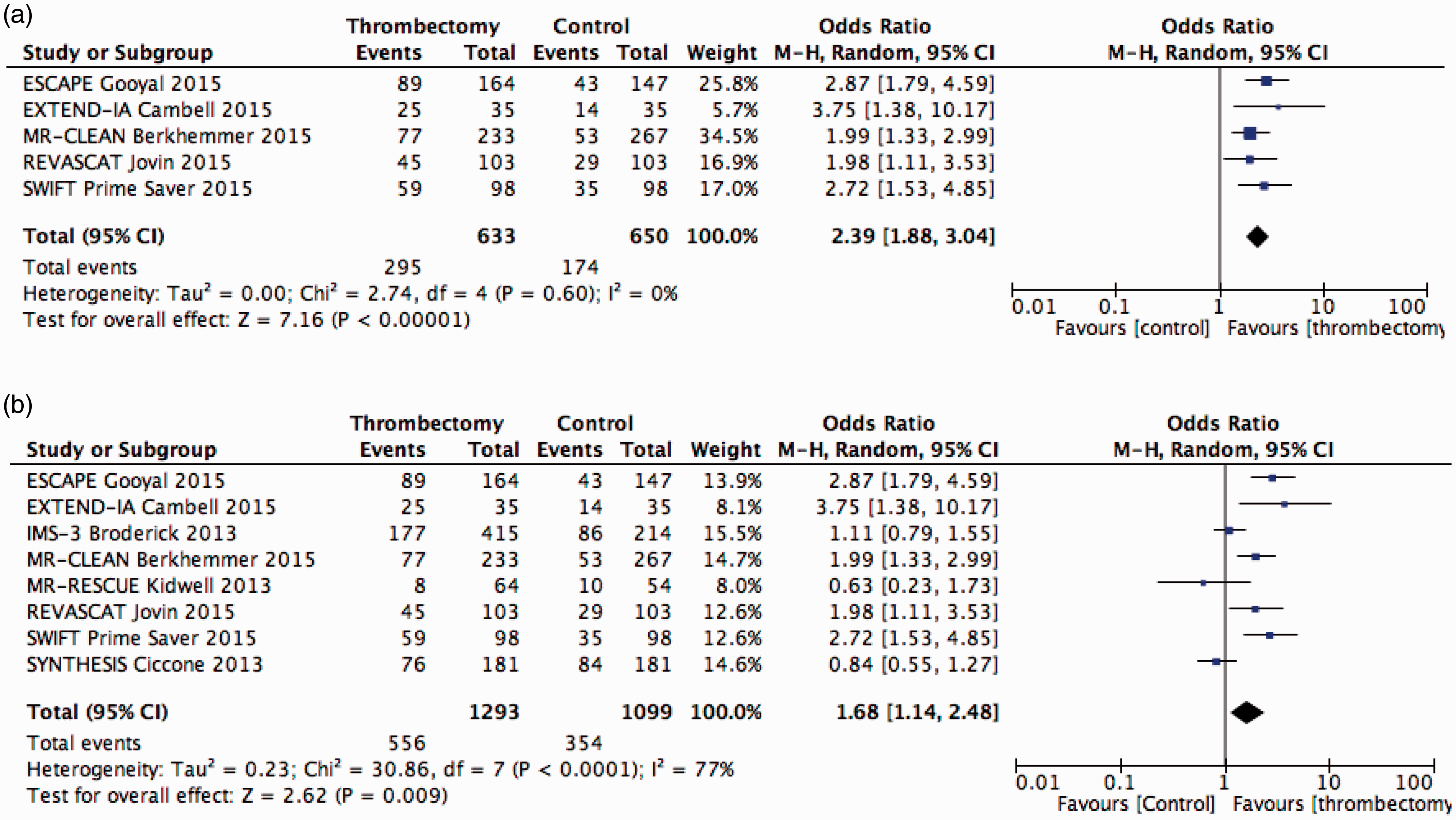
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Individual Funding
Jens Fiehler has received funding from the German Research Foundation (DFG) and the German Ministry of Education and Research (BMBF).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marcel Arnold had speaker engagements and advisory boards for Covidien, and Boehringer-Ingelheim, BMS, Pfizer and Bayer and declared co-authorship for some literature.49,50 Christoph Cognard was a co-author of SWIFT Prime. Valeria Caso declares speaker’s bureau for Boehringer Ingelheim and Pfizer and advisory board for Boehringer-Ingelheim. Franz Fazekas has no conflicts of interest. Jens Fiehler has received fees as consultant or lecturer from Acandis, Bayer, Boehringer-Ingelheim, Codman, Covidien, MicroVention, Penumbra, Philips, Sequent, Siemens and Stryker. Related: Consultant for Codman, MicroVention. Lectures for Boehringer-Ingelheim, Covidien, and Penumbra. Funding to institution: MicroVention. Unrelated: Consultant for Acandis, Sequent, Stryker. Lectures for Bayer, Philips, Siemens. Funding to Institution: DFG, BMBF, BMWi. Olav Jansen was a co-author of SWIFT-Prime, and is a steering committee member of SITS Open. Urs Fischer has speaker’s honorarium with Covidien. Jan Gralla is global PI of the STAR study, consultant for Covidien. Werner Hacke declares membership in the SWIFT Prime Steering Committee, and modest reimbursement for time spent. Staffan Holmin co-authored some literature19,41 and is a steering committee member of SITS Open and the SITS thrombectomy registry. Kennedy Lees was co-author of Emberson et al. 1 Heinrich Mattle was an advisor in the design of MR CLEAN, co-author of SWIFT Prime, and was involved in planning, conduction and writing the studies quoted in some literature.44,57,58 Mikael Mazighi has co-authored the IMS 3 trial Patrik Michel is co-investigator in SWIFT Prime, BASICS registry and BASICS trials Tiago Moreira is co-investigator in SITS Open. Jesper Peterson’s centre is participating in SITS Open. Laurent Pierot has no conflicts of interest. Thorsten Steiner had consulting from Covidien. Istvan Szikora has consulting agreements with Covidien, Stryker and Codman. Turgut Tatlisumak has no conflicts of interest. Wim van Zwam was one of the principal investigators of MR CLEAN. Nils Wahlgren is coordinator of SITS Open and chairman of SITS International. Co-authored some literature.1,19,41,56