
Abstract
There are notable data gaps for safety, dosing and effectiveness of many health products for pregnant and lactating individuals. There have been growing calls to timeously include this population in clinical trials to generate evidence-informed interventions for them and their foetus/nursing infants. This echoes calls for a better evidence base to address the HIV prevention needs of this population. Research Ethics Committees (RECs) or Institutional Review Boards (IRBs) are centrally positioned to review if enrolment of pregnant/breastfeeding individuals is ethically acceptable, according to leading ethics guidance. To perform this task, REC/IRBs may benefit from a better understanding of current recommendations from these international ethics guidelines. We aimed to identify pregnancy-related recommendations from key international ethics guidance documents, to identify areas of conflict and to support RECs/IRBs to efficiently and systematically identify whether ethics recommendations are met. We found a rich abundance of relevant ethics recommendations. We also found that most guideline recommendations are synergistic, with the most notable divergence arising in the terminology used for when it is acceptable to transition from preclinical (animal) studies to exposing pregnant/lactating humans to the study product. We developed a brief resource setting out guidance-informed queries that REC/IRB reviewers could use to focus their review. REC/IRBs are well-placed to judge the ethical acceptability of enrolling pregnant and lactating individuals in clinical trials of HIV prevention, leveraging rich, largely synergistic ethics recommendations from leading documents.
Keywords
Introduction
There are notable evidence gaps for the safety, dosing, and effectiveness of health products for pregnant and lactating individuals (Dey et al., 2025; Zur, 2023). Historically, this stems from excluding pregnant individuals from clinical trials, and requiring those of reproductive potential either to commit to contraceptive use or ensuring product discontinuation if they become pregnant while on study product (American College of Obstetrics and Gynaecology, 2015; PHASES, 2020; WHO, 2021). These measures generally arise from concerns regarding the safety of study products for foetuses and nursing infants (CIOMS, 2016). There has been growing momentum for the timely inclusion of pregnant and lactating individuals in clinical trials (American College of Obstetrics and Gynaecology, 2015; Baylis and Halperin, 2012; Bowen, 2006; Dey et al., 2025; Drapkin Lyerly et al., 2009; Little et al., 2021; Roes et al., 2018; Sewell et al., 2022; Singh et al., 2022; US Eunice Kennedy Shriver National Institute of Child Health and Human Development, n.d; van der Graaf et al., 2019; van der Zande et al., 2017). An increased evidence-base from clinical trials will prevent risk-shifting to patients and healthcare providers in the clinical context (Abrams and Penazzato, 2022; Waitt et al., 2022).
HIV is among the most serious health conditions affecting pregnant and lactating individuals (Little et al., 2016). During pregnancy and lactation, they are at increased risk of acquiring HIV and co-infections such as TB and malaria (HPTN, 2021; PHASES, 2020; UNAIDS, 2021). Pregnancy increases the risk of HIV infection by 2–3 times, while the postpartum period further amplifies the risk, increasing it fourfold (Mugo et al., 2011; Thompson et al., 2018, cited in Lorenzetti et al., 2024). This is likely attributable to hormonal, immunological and behavioural changes in this period (Graybill et al., 2020). Data gaps persist with regards to their HIV prevention needs (despite some progress) and consequently, their access to prevention products is often delayed relative to the general population (HPTN, 2021; UNAIDS, 2021). The field has seen numerous recommendations to include pregnant and lactating individuals in clinical trials of HIV prevention in a timely fashion, to increase the likelihood of providing safe, effective and evidence-informed interventions in the clinical setting (Joseph Davey et al., 2022; PHASES, 2020; WHO, 2021).
Increased action across the trial eco-system has been recommended to support the responsible enrolment of pregnant and lactating individuals in clinical trials. This includes the key role that Research Ethics Committees (RECs) or Institutional Review Boards (IRBs) play (Payne, 2019; van der Graaf et al., 2019; van der Zande et al., 2017) along with a range of other actors. In the context of HIV prevention clinical trials, it has been noted that RECs/IRBs are well-positioned to ensure that the participation of pregnant and lactating individuals is ethical, as part of larger collaborative efforts (PHASES, 2020; Sullivan et al., 2023). It has been argued that RECs/IRBs play a role in ensuring that “any proposed research meets appropriate criteria for their responsible inclusion” (PHASES, 2020: 17). Furthermore, it has been emphasised that RECs/IRBs may have a role to play in broadening attention beyond foetal risk - to the risks of “not pursuing the intervention” as well as to potential maternal benefit (PHASES, 2020: 19).
To determine if the enrolment of pregnant or lactating individuals in specific trials is ethically acceptable, RECs/IRBs may benefit from a good understanding of current recommendations from leading international guidelines, as well as areas of potential divergence. An overview of these recommendations might assist REC/IRB reviewers to more easily identify “permissible conditions” for the enrolment of these individuals (PHASES, 2020: 33), potentially enhancing the efficiency of ethics review. Additionally, such an overview may promote more consistent application of normative recommendations and inform the query-response interaction in the ethics review process.
Accordingly, we aimed to (firstly) identify pregnancy-related recommendations from leading international ethics guidance documents, (secondly) identify areas of conflict (Slack et al., 2021) and (thirdly) make recommendations for how RECs/IRBs could be supported to review trials of HIV prevention for the enrolment of pregnant and lactating individuals (Sullivan et al., 2023). While our primary audience is RECs/IRBs, it would be remiss to neglect the critical role of researchers in drafting ethical protocols for review. Therefore, we also make recommendations for this stakeholder.
Our focus was specifically on clinical trials of HIV prevention; therefore, we selected high-profile recently updated ethics guidance used broadly in the HIV field, namely the Ethical Considerations in HIV Prevention Trials published by the Joint United Nations Programme on HIV/AIDS (UNAIDS, 2021), and Ethics Guidance for Research published by the HIV Prevention Trials Network (HPTN, 2021). After discussion we agreed that two recent influential guidance documents were also relevant; namely the Ending the Evidence Gap for Pregnant Women around HIV & Co-Infections: A Call to Action published by the PHASES project (Pregnancy and HIV: Seeking Equitable Study) in 2020 and focussed on HIV, TB, and malaria research, as well as the Research for Informed Choices: Accelerating the Study of New Drugs for HIV in Pregnant and Breastfeeding Women published by the World Health Organization and focussed on HIV research (WHO, 2021). Despite our HIV prevention focus, we recognised that RECs/IRBs have a broader mandate and therefore we also included International Ethical Guidelines for Health-Related Research Involving Humans which is relevant to health research generally (CIOMS, 2016). Thereafter, we identified recommendations for responsible enrolment of this population especially relevant to the ethics review process. We included ethics recommendations that were explicitly directed at pregnant or lactating individuals, or highly relevant to them (e.g. for groups considered vulnerable), and we excluded text that was not specific or highly relevant. Then we organised recommendations according to the popular Emanuel framework (Emanuel et al., 2000, 2004, 2008) which has been used to organise thematic concerns related to RECs/IRBs in previous publications (Silaigwana and Wassenaar, 2019; Tsoka-Gwegweni and Wassenaar, 2014).
While earlier literature has provided useful summaries of ethics guidance on this topic, some gaps persist. For instance, Lyerly et al. (2021) included select recommendations from some ethics guidance but, given the timing of the publication, not HPTN (2021). Joseph Davey et al. (2022) and the PHASES guidance in 2020 included recommendations from ethics guidance, but both focussed on consent, risk levels, and preliminary data from animal studies, omitting other concerns.
Ethics recommendations
Below we set out the detailed ethics recommendations for researchers from our review of guidelines, organised according to components of the Emanuel framework (Emanuel et al., 2000, 2004, 2008). These components include social value and scientific validity, favourable risk-benefit ratio, fair selection, collaborative partnership, informed consent, and ongoing respect. Because these components may be less familiar to a wider audience, we have described in some detail the substance of each component. There-after we set out detailed ethics recommendations from guidance, including verbatim text to capture the rich nuance of ethics recommendations. Also, we cite the specific guidance clearly to assist RECs/IRBs to choose the most relevant recommendation depending on the protocol they are reviewing.
Social value and scientific validity recommendations
According to the Emanuel framework, to have social value, a study should aim to generate knowledge that leads to health improvements (Emanuel et al., 2008). Judgements about social value are prospective and “probabilistic” involving judgement about the potential usefulness of research and the likelihood of results implementation (Emanuel et al., 2008: 127). To have scientific validity, a study should be implemented in a “methodologically rigorous manner” (Emanuel et al., 2000: 2704) that will yield valid and reliable results that can be interpreted and used (Emanuel et al., 2008). Both social value and scientific validity ensure that participants are not exposed to risks and burdens for “no good reason” (Emanuel et al., 2004: 932) or no purpose (Emanuel et al., 2000). Accordingly, we clustered here ethics recommendations from guidance that address the value and rigour of studies with pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to recognise the risk of infection: more specifically to recognise that pregnancy carries an increased risk of HIV acquisition “attributable to social risks” and “biological changes in pregnancy” (UNAIDS, 2021: 32) and that women and gender-diverse persons “should be recipients of safe and effective HIV prevention products” because in many communities (they) are at higher risk of HIV exposure (UNAIDS, 2021: 32).
Additionally, researchers are encouraged to reduce the evidence gap: more specifically to promote research “designed to obtain knowledge relevant to health needs of the pregnant and breastfeeding woman” (CIOMS, 2016: 62) and to recognise the “imperative to design research (. . .) to learn about the currently unknown risks and potential individual benefits” to women and to the foetus/nursing infant (CIOMS, 2016: 62). It is recommended that researchers strive towards a “more equitable evidence base for underrepresented groups” (UNAIDS, 2021: 32); review approved preventives/treatments for evidence gaps and conduct research to address “legacy evidence gaps” (PHASES, 2020: 48); commit to “integrating pregnant women [in trials] wherever possible and optimise opportunities to gather pregnancy-specific data” (PHASES, 2020: 38) and match research into foetal safety outcomes with relevant maternal outcomes assessments (PHASES, 2020). Researchers should recognise that the lack of knowledge about the safety and efficacy of drugs, vaccines or devices can be “dangerous” (CIOMS, 2016: 69).
Favourable risk-benefit ratio recommendations
According to the Emanuel framework, to meet a favourable risk-benefit ratio, a study should ensure that potential risks to individual participants are identified and minimised (Emanuel et al., 2000). Also, potential benefits to individual participants from the research interventions should be delineated and maximised (potential benefits to society in the form of knowledge gains are assumed if the study has social value; Emanuel et al., 2000, 2004). Further, potential risks to individual participants should be proportionate or outweighed by potential benefits to individual participants or society (Emanuel et al., 2000, 2008). Such determinations are “metaphorical” but not necessarily “haphazard” (Emanuel et al., 2008: 129). Accordingly, we clustered here ethics recommendations from guidance that address the risk-benefit calculus of studies with pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to recognise risks of study interventions/ procedures: more specifically to recognise that research may “present risks and potential individual benefits to the foetus as well as to the woman” and to the nursing infant (if breastfeeding; CIOMS, 2016: 62); to recognise “concerns about the well-being of foetuses and breastfeeding children” (HPTN, 2021: 27) and to provide “protections to mitigate” risks (e.g.) partner or family violence (PHASES, 2020: 46).
Also, researchers should implement animal studies timeously. It is recommended that researchers ensure that fertility and early embryonic development (FEED) and embryo-foetal development (EFD) studies are “completed during or no later than the end of Phase 2 registrational trials” for all new agents (WHO, 2021: 5) and to ensure that “prenatal and postnatal development (PPND) studies are completed during early Phase 3 or no later than the end of Phase 3 registrational trials” for priority agents (WHO, 2021: 5).
Further, researchers should consider data from non-pregnant women: It is recommended that researchers initiate research in this population “after careful consideration of the best available data from preclinical research in pregnant animal models, research in non-pregnant women, retrospective observational studies, and pregnancy registries” (CIOMS, 2016: 72). Researchers are encouraged to establish dosing in non-pregnant women before removing contraception restrictions in pre-licensure trials (WHO, 2021); to “commit to pursuing PK studies in pregnancy (. . .) as soon as standard dosing and preliminary safety of a drug is confirmed in non-pregnant individuals” (PHASES, 2020: 41) and to ensure that, where scientifically appropriate, the study product has been “proven safe” in trials with “non-pregnant women” (45 CFR 46; HPTN, 2021: 28).
Also, researchers should transition to data collection in pregnant humans when non-clinical data meets a certain threshold. More specifically, researchers are encouraged to determine pregnancy PK and dosing on all products for HIV treatment and prevention before registration if “no major concern” is raised by non-clinical studies (WHO, 2021: 6); and to ensure that, “where scientifically appropriate,” the study product is “proven safe” in preclinical studies with non-human animals (HPTN, 2021: 28). It is recommended that researchers remove contraceptive “restrictions in (. . .) pre-licensure trials once early non-clinical toxicity data are available without major concerns” (WHO, 2021: 8); give women who become pregnant in pre-licensure trials the choice to remain on study drug and “contribute pregnancy PK and safety data, once non-clinical FEED and EFD studies are completed “with no negative signals” (WHO, 2021: 5) and allow women who become pregnant in trials the chance to remain on study product where “adequate” preclinical toxicology animal safety data are available, and their participation carries “a favourable risk-benefit ratio” (PHASES, 2020: 36).
Furthermore, researchers should transition to data collection in pregnant humans in late-phase pre-registrational trials, recognising this as a critical stage to enrol this population. More specifically researchers are encouraged to recognise that increasing pregnant women’s participation in phase 3 trials can be an “important source of information” to “reduce delays” in “post-approval access” (PHASES, 2020: 35); to identify “ways to encourage enrolment of pregnant women in phase 3 pre-licensure (trials)” for priority agents for HIV treatment and prevention (WHO, 2021: 7); to obtain pregnancy PK/safety for all new drugs in phase 2b or phase 3 (WHO, 2021) and to presume inclusion for “larger trials” where “the potential advantages” of the drug being researched are “greater” (PHASES, 2020: 35).
Importantly, researchers should ensure that enrolment of pregnant and lactating individuals meets favourable risk-benefit ratios: More specifically researchers are encouraged to minimise risks of “interventions or procedures that have potential to benefit either the pregnant or breastfeeding women or their foetus or infant” and ensure that risks are “outweighed by the prospect of potential individual benefit” (CIOMS, 2016: 71) and to recognise that foetal “minimal risk” restrictions do not apply where “research holds out the prospect of a direct benefit to women or the foetus” (HPTN, 2021: 28). Also, researchers are encouraged to minimise risks of interventions/procedures with “no potential individual benefit” for pregnant or breastfeeding women, ensure risks are “no more than minimal,” and ensure that the purpose is to “obtain knowledge relevant to the particular health needs of pregnant/breastfeeding women or their foetuses or infants” (CIOMS, 2016: 71). A “minor increase” above minimal risk is permitted when social value for pregnant/breastfeeding women or their foetus is “compelling” and “the research cannot be conducted in non-pregnant/breastfeeding women” (CIOMS, 2016: 71).
Some guidance recognises the harm of delayed registration of interventions for pregnant and lactating individuals. Researchers are encouraged to ensure that new drugs should “reach market with pregnancy-specific dosing information in hand at the time of licensure, or as soon as possible after regulatory approval” (PHASES, 2020: 40). Researchers should also aim to “have PK and preliminary safety data on all new agents in pregnancy at the time of drug approval” (WHO, 2021: 5) and determine PK and dosing during pregnancy on all agents for HIV treatment and prevention before drug registration if no major concern is raised by non-clinical studies (WHO, 2021). Lastly, researchers should perform relevant studies “as early as possible, ideally before licensure, for all new preventives and treatments anticipated to be used during pregnancy” (PHASES, 2020: 40).
Fair selection recommendations
According to the Emanuel framework, to ensure fair selection, groups and individuals to be approached or enrolled should be determined based on scientific reasons (Emanuel et al., 2000, 2004). Also, from a scientifically eligible pool, individuals should be chosen to minimise risk (Emanuel et al., 2000). Further, those groups and individuals who stand to benefit should bear some of the risks and burdens (Emanuel et al., 2000). Accordingly, we clustered here ethics recommendations from guidance that address the selection of participants in research with pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to strive for inclusion: Researchers should not consider pregnant women as “vulnerable simply because they are pregnant” yet recognise that “specific circumstances, such as risks to the foetus, may require special protections” (CIOMS, 2016: 58). Researchers are encouraged to move towards “intentional assessment” for inclusion including “serious consideration” of needs, potential ethical eligibility and “evidential value” of inclusion (PHASES, 2020: 35); and avoid “arbitrary exclusion” of individuals/populations “based on characteristics including (. . .) pregnancy, lactation or child-bearing potential”’ (UNAIDS, 2021: 31). Researchers should recognise that some research protocols “may need to exclude individuals and groups for safety reasons on the basis of anticipated biological interactions (. . .) or because of anticipated harms” (UNAIDS, 2021: 31). Protocols should “provide justification whenever pregnancy is indicated as a criterion for exclusion or removal from a trial” (PHASES, 2020: 37) and the review process should “systematically require and assess the scientific rationale when pregnant women are excluded from a study proposal and/or protocol” (WHO, 2021: 7). Also, researchers are encouraged to guarantee “fair access to participate in trials and special access programs for experimental interventions that offer potential life-saving benefit in contexts where no or poor alternatives exist” (PHASES, 2020: 45).
Furthermore, researchers should strive for diversity: Researchers are encouraged to include “gender-diverse groups in trials to establish safety, efficacy and/or effectiveness of interventions” (UNAIDS, 2021: 32) and to consider transgender men and gender diverse people even while “guidelines focus specifically on cisgender women” (HPTN, 2021: 28). Further, researchers should consider restricted access to abortion carefully: Researchers are encouraged to conduct studies involving pregnant women that hold out the prospect of foetal harm only in settings with “safe, timely and legal abortion” (CIOMS, 2016: 71), unless an REC/IRB determines that there is compelling social value and information on restrictions, and options, is provided (CIOMS, 2016), as well as recognise that critical prevention efforts could be precluded when trials in pregnancy are limited to settings with “safe, timely and legal abortion” (HPTN, 2021: 29).
Collaborative partnership recommendations
According to the Emanuel framework, to ensure collaborative partnership, a study should engage host communities and policymakers (amongst others) as partners, and seek their inputs through a variety of formal or informal mechanisms to help determine responsiveness to health problems, and to enhance impact on policy and resource allocation. Accordingly, we clustered here ethics recommendations from guidance that address the engagement of stakeholders towards a partnership for studies with pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to engage stakeholders: Researchers are encouraged to ensure “a detailed community engagement plan” (WHO, 2021: 8); to “involve women of childbearing potential affected by HIV from identification of research questions through study design, recruitment, conduct and dissemination of results” (WHO, 2021: 5) and to engage stakeholders in key decisions for example, timing of PK studies (UNAIDS, 2021) and assessing when pregnant persons could receive product (HPTN, 2021). Researchers also have the responsibility to communicate overall study findings in a way that “contextualise[s] potential risks of an intervention against potential benefits” to women and children as well as risk-benefit profiles of alternatives (PHASES, 2020: 47) and contextualise any associations “against baseline rates of adverse pregnancy outcomes” especially miscarriage, birth defects (UNAIDS, 2021: 33). Additionally, researchers should consider legal and gender norms: Researchers are encouraged to be aware of “gender norms” that may constrain autonomy, and inequalities institutionalised in law/policy (UNAIDS, 2021: 32); be aware of “cultural beliefs accord[ing] more importance to the foetus than to the women’s life or health” (CIOMS, 2016: 72) and “determine (. . .) legal grounds for abortion in that jurisdiction” (CIOMS, 2016: 73).
Informed consent recommendations
According to the Emanuel framework, to realise informed consent a study should ensure that potential participants are informed of relevant information, understand the information and its bearing on their own situation, and make a free uncoerced decision to participate (Emanuel et al., 2004). Also, decision-making capacity should exist in the consenting party (Emanuel et al., 2008). Furthermore, consent should be documented (Emanuel et al., 2008). Lastly, these components of informed consent should be sensitive to culture and context (Emanuel et al., 2008). Accordingly, we clustered here ethics recommendations from guidance that address the consent process for studies involving pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to disclose risks: Researchers are encouraged to inform potential participants of “the risks to pregnant women (including future fertility), and their pregnancies, their foetuses, and their future offspring” (CIOMS, 2016: 105); any “potential for teratogenesis and other known or unknown risks to foetus and/or [nursing] infant” (UNAIDS, 2021: 33) and disclose the “availability of (. . .) infant milk substitutes and support services (. . .) [even while] infant feeding formulae can pose risks when there is no clean water” (UNAIDS, 2021: 33). Also, researchers should recognise that incident pregnancy is a circumstance requiring re-informing/re-consenting participants (HPTN, 2021) and should convey, in a re-consent process, risks and benefits of continued participation (if it is potentially acceptable to continue using product during pregnancy; HPTN, 2021).
Further, researchers should facilitate consultation with important others: Researchers are encouraged to provide opportunities for consultation with whomever participants’ wish (UNAIDS, 2021) and permit consulting with fathers of foetuses (CIOMS, 2016) and make “accommodations” to facilitate engagement of fathers/family/personal supports (PHASES, 2020: 46). However researchers are encouraged to recognise that the woman remains “the decision-maker for any interventions that affect her” (CIOMS, 2016: 72); to ensure that the decision is made “alone” (UNAIDS, 2021: 33) or is the “final decision” (CIOMS, 2016: 72); to consider the consent of a woman of “legal standing” sufficient to authorise participation (PHASES, 2020: 46); and to ensure women are “at the centre of decisions” about participation (PHASES, 2020: 46). Researchers should not replace women’s consent “with the permission of another person”’ (CIOMS, 2016: 71); not permit another individual to “override their decision” (UNAIDS, 2021: 33) and be cautious before “considering adding formal paternal consent as a precondition” (PHASES, 2020: 46).
Ongoing respect recommendations
According to the Emanuel framework, to show ongoing respect for enrolled participants, a study should implement various steps to demonstrate how participants welfare will be addressed after they join the study. This includes, but is not limited to, the responses that are unrelated to the scientific study that researchers will implement to help address participants’ medical needs (Emanuel et al., 2004). Accordingly, we clustered here ethics recommendations from guidance that address post-enrolment considerations in studies with pregnant or breastfeeding individuals.
Ethics guidance encourages researchers to address medical needs: Researchers are encouraged to make plans for “how care will be adequately provided for the condition under study” plus “conditions other than those under study” (CIOMS, 2016: 21); make plans to transition participants who continue to need post-study care to “appropriate health services” (CIOMS, 2016: 21); include stakeholders during research planning to develop standards for providing/referring participants for ancillary care, and they should implement pragmatic measures to achieve this (HPTN, 2021).
Researchers should also assess outcomes within, after and across studies: It is recommended that researchers document outcomes of pregnancies occurring inadvertently in trials (UNAIDS, 2021) and analyse foetal and maternal outcomes from exposures (PHASES, 2020); aggregate across studies that gather exposures, and develop data harmonisation protocols (PHASES, 2020). They should include in protocols a plan to monitor outcomes for health of pregnant women and “short and long-term health” of infants/children, and “contribute to pregnancy registries” (UNAIDS, 2021: 33). Furthermore, they should expand surveillance to detect “adverse maternal, pregnancy and birth outcomes, especially rare events” for example, birth defects (WHO, 2021, p5); commit to post-approval safety evaluations (PHASES, 2020) and follow up on outcomes for foetuses, short-term and long-term, and children depending on the intervention and its potential risks (CIOMS, 2016).
Discussion
We aimed to achieve three key objectives: first to identify pregnancy-related ethics recommendations from leading international guidance documents, second, to identify areas of divergence, and third, to make recommendations for how RECs/IRBs could be supported in their review of clinical trials of HIV prevention for the enrolment of pregnant and lactating individuals. Our goal is to impact the efficient and consistent application of ethics recommendations across these research protocols.
First, when identifying ethics recommendations from leading international guidance, we found robust coverage of key components of ethical research. These collated recommendations may assist RECs/IRBs to “identify approvable designs” (PHASES, 2020: 37). Alternatively, these recommendations could support RECs/ IRBs to consider whether – in their view - it would be justifiable to exclude pregnant and lactating women on the grounds that ethics recommendations have not been met. The recently revised Helsinki declaration (WMA Declaration of Helsinki, 2024) notes that protocols must “be submitted for consideration, comment, guidance and approval” by RECs/IRBs (p3), with due consideration of norms in host countries and applicable international norms. A collation of guidelines may assist RECs/IRBs to consider normative recommendations in a systematic way, even while identical review outcomes are not necessarily feasible nor desirable (Abbott and Grady, 2011; Slack, 2016). This paper does not critique the ethics recommendations (nor does it aim to). For example, we do not critique whether it is substantively correct that the risks to the foetus/infant of non-beneficial interventions be capped at minimal or a minor increase over (Bowen, 2006). Critiques of this trade-off have included that minimal risk is not interpreted uniformly across RECs/IRBs (Dey et al., 2025; Little et al., 2021; Shah et al., 2004). RECs/IRBs may wish to discuss how the ethics recommendations best apply to the protocol at hand.
It is worth considering how the proposed collation should work with national ethics guidelines, given that RECs/IRBs will also draw on national guidelines when reviewing protocols. It is possible that RECs/IRBs could use this collation to supplement national recommendations. For example, the South African national ethics guidelines (National Department of Health [NDOH], 2024) address two issues in the resource (related to the risk-benefit ratio and to consent) but are silent on the other issues. Being primed about ethics recommendations that are relevant internationally (in all settings) might address potential concerns that less ethical practices might be exported to low-resource settings, as set out in the TRUST code (2018).
While RECs/ IRBs are the key audience here, it would be remiss to neglect the role of researchers in drafting ethical protocols for review. Researchers may benefit from a “one-stop-shop” of current ethics recommendations so they can carefully consider these and demonstrate to the REC/IRB that their protocol is responsive to the current international ethics framework on this topic (Sullivan et al., 2023). This may help researchers to plan more concretely for the downstream implications of meeting these ethics recommendations for example, the budgeting and staffing needed to implement detailed engagement plans, or the recruitment strategies needed to ensure gender diversity, or the formative evaluation strategies needed to assess legal, gender and cultural norms in the setting.
Second, when examining areas of divergence in leading international ethics guidance, we found strong alignment across most ethics recommendations, with few areas of conflict. This bodes well for the ethics review process, because REC/IRB members’ time need not be spent reconciling opposing recommendations in international guidance. We found some differences in terminology used to refer to pregnant individuals (e.g. “women” or “person”). However, the most notable difference in terminology was between those terms used to assess if data from animal studies suggests acceptable risk for pregnant or lactating humans. More specifically, some guidance recommended that animal studies should show “no negative signals” (WHO, 2021: 5) or show “no major concern” (p6), or that safety data from animals be “adequate” (PHASES, 2020: 36). However, other ethics guidance recommended that acceptable levels of risk in pregnant/lactating humans is when the risks of potentially beneficial interventions are sufficiently minimised, and the foetal risks of potentially non-beneficial interventions are minimal or minor increase over (CIOMS, 2016). Even by waiting to enrol this population in phase 3 trials only (where there would be sufficient evidence of potential individual benefit so that a foetal risk standard of “minimal” would not apply), RECs/IRBs are still faced with the task of bridging the terms above. In this regard, RECs/IRBs may benefit by accessing relevant expertise for the interpretation of animal studies (WHO, 2021) and by accessing translational resources (PHASES, 2020) to enable them to assess if the allowable risk levels in pregnant/lactating humans will be met (White et al., 2021).
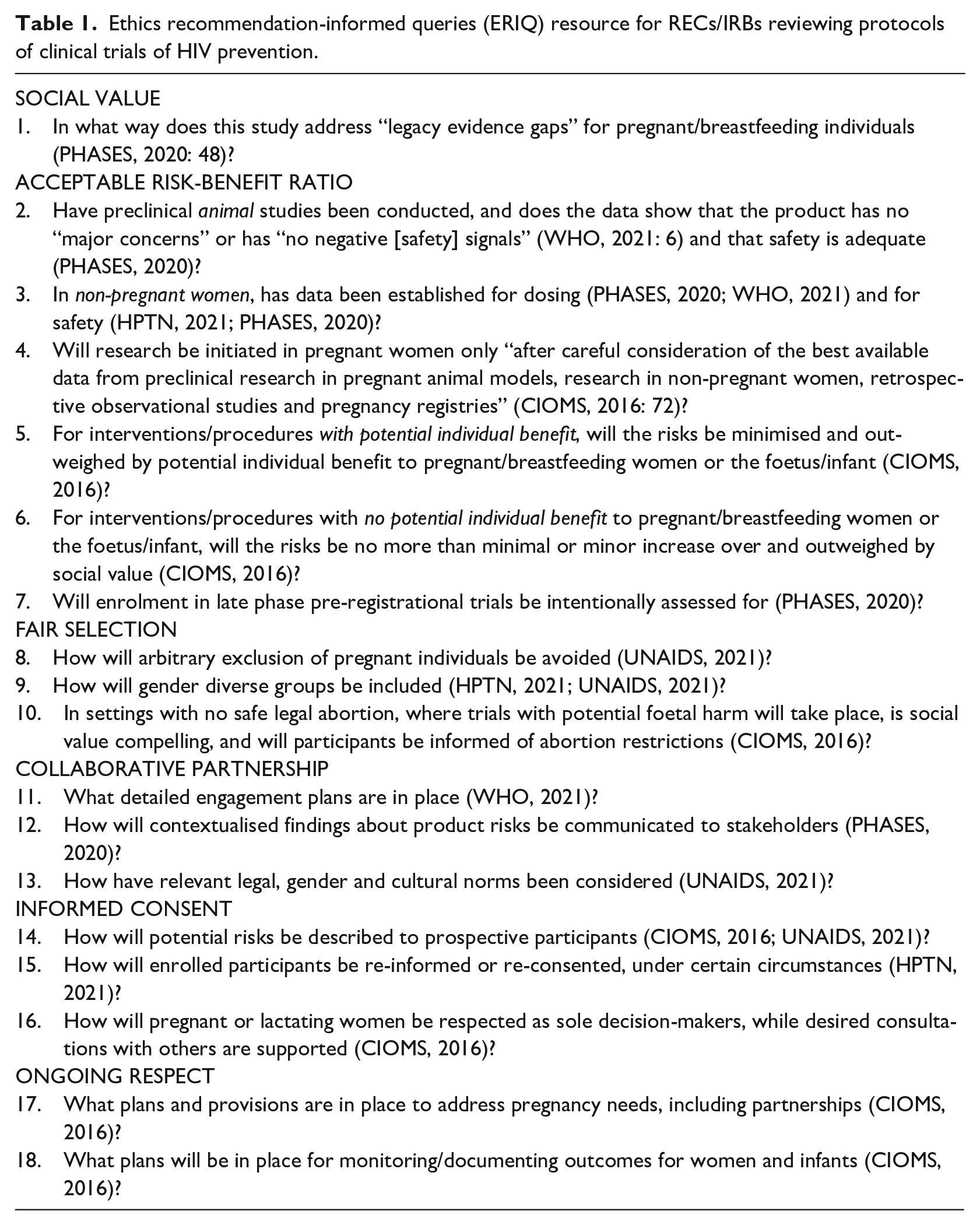
Third, in terms of supporting RECs/IRBs to assess the ethical acceptability of enrolling pregnant or lactating individuals, we noted that the sheer number of ethics recommendations for this topic was large and time-consuming to read. Therefore, we developed a brief resource for REC/IRB-reviewers. The resource sets out guidance-informed questions that reviewers may wish to ask during protocol review – which we have termed the ERIQ resource (
Ethics recommendation-informed queries (ERIQ) resource for RECs/IRBs reviewing protocols of clinical trials of HIV prevention.
Conclusions
The rich, largely synergistic ethics recommendations from leading documents are an asset to RECs/IRBs tasked with judging the ethical acceptability of enrolling pregnant and lactating individuals in clinical trials of HIV prevention. We recommend that RECs/IRBs consider using a concise resource that suggests several guidance-informed queries for researchers. This might assist evaluation of the “ethical acceptability” of protocols under consideration (CIOMS, 2016: 87) and might impact efficient, consistent application of ethics recommendations across protocols.
Footnotes
Acknowledgements
Thank you to Dr Annie Lyerly from PHASES, as well as AVAC and USAID colleagues, for valuable comments. Thank you to Ms Abigail Wilkinson for assistance with manuscript preparation.
Ethical Considerations
No data collection from human participants took place.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was made possible by the generous support of the American people through the US President’s Emergency Plan for AIDS Relief (PEPFAR) and the US Agency for International Development (USAID; co-operative agreement no. AID-OAA-A-16-00031 – Coalition to Accelerate and Support Prevention Research [CASPR]). The contents do not necessarily reflect the views of PEPFAR, USAID, or the US government. This article was supported by the South African Medical Research Council with funds received from AVAC as a primary recipient of a USAID award. The content and findings reported/ illustrated are the sole deduction, view and responsibility of the researcher and do not reflect the official position and sentiments of the SAMRC.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CS served on a DSMB that oversees certain HIV vaccine trials and DSMB members receive an honorarium. CS participated in the consultation hosted by WHO to revise the UNAIDS 2012 guidelines. MC, BL, MK, KS – Nil