
Abstract
The use of psychometric tools to investigate the impact of school-based wellbeing programs raises a number of ethical issues around students’ rights, confidentiality and protection. Researchers have explicit ethical obligations to protect participants from potential psychological harms, but guidance is needed for effectively navigating disclosure of identifiable confidential information that indicates signs of psychological distress. Drawing on a large-scale study examining student, school, and system-based factors that impact the implementation of a school-based social and emotional learning program, we describe patterns of distress attained from quantitative and qualitative questions and describe the process that we evolved to monitor and disclose sensitive mental health information, providing one example of how researchers might effectively address the responsibilities that emerge when collecting sensitive information from students within an education system. The patterns and processes that emerged illustrate that the inclusion of mental distress information can elicit important insights, but also brings responsibilities for minimising risks and maximising benefits.
Keywords
The use of psychometric tools to investigate the impact of school-based wellbeing programs raises a number of ethical issues around confidentiality, students’ rights for privacy, duty of care, mandatory reporting laws and the expectations of parents and schools that students remain protected (Hiriscau et al., 2014; Jaycox et al., 2006). Researchers have explicit ethical obligations to protect participants from potential psychological harms. However, the inclusion of mental health information can result in the need to balance moral, ethical and legal tensions, especially when matters arise in the course of the study that are only identified in retrospect. There is a dearth of professional, scientific and practical guidelines for navigating the ethical issues that arise around disclosing identifiable confidential data when students show evidence of significant psychological distress, suicidality and/or exposure to family violence (Leadbeater et al., 2018). In this paper, we discuss how the responsibility to act upon knowledge about psychological distress was managed in a large-scale study with Australian primary and secondary school students. We suggest that the inclusion of identifiable indicators of distress within wellbeing surveys elicits important and useful insights, but also brings risks and responsibilities that need to be managed to protect student wellbeing and prevent unintentional harm.
Schools at the mental health frontline
Childhood and adolescence are critical periods for the onset of mental health problems, with almost 50% of diagnosed illness emerging by age 14 (Kessler et al., 2010; Lawrence et al., 2015). In Australia, surveys suggest that nearly a quarter of 15 to 19-year-olds may meet the criteria for having a mental illness (Bullot et al., 2017), and one in ten adolescents report having self-harmed in the last 12 months (Lawrence et al., 2015). Despite considerable public health resources dedicated to improving young people’s mental health, the prevalence of mental disorders globally has not reduced, with evidence suggesting that mental illness is being reported at younger ages and more frequently than in previous years (Bullot et al., 2017; Collishaw et al., 2004; Sawyer and Patton, 2018).
Schools are potentially well-placed to address the mental health needs of young people (Greenberg et al., 2003; Midford et al., 2017; Payton et al., 2008; White and Kern, 2018). The majority of school-aged youth attend school. As teachers regularly interact with students, they have opportunities to observe mood and behavioural change, and can therefore play a critical role in identifying, supporting and preventing mental health issues for their students (Graham et al., 2011). Further, many educational institutions value and are held accountable for developing student wellbeing and character (Allen et al., 2018; Seligman et al., 2009).
Indeed, educational institutions are increasingly acting to address mental health issues through their policies, provisions and relational approaches (Graham et al., 2016; Powell and Graham, 2017), with curricular priorities directly addressing emotional and social wellbeing capabilities. For instance, in Australia, wellbeing is now an established part of both national and state-based educational policy (Powell and Graham, 2017). To support these efforts, numerous school-based programs and curricula have been developed (Kern et al., 2017; Slemp et al., 2017). Studies have demonstrated that the provision of universal, evidence-informed strengths-based social and emotional learning (SEL) programs can effectively increase social and psychological wellbeing (Durlak et al., 2011; Greenberg et al., 2003; Kern et al., 2017; Payton et al., 2008); reduce anxiety, depression and drug and alcohol use (Horowitz and Garber, 2006; Merrell et al., 2008; Neil and Christensen, 2007; Payton et al., 2008, Stockings et al., 2016); decrease bullying and gender-based harassment (Hong and Espelage, 2012; Ttofi and Farrington, 2011); improve peer and school connectedness and improve prosocial behaviours (Durlak et al., 2011; Midford et al., 2017); and increase academic engagement and performance (Durlak et al., 2011).
Complexities in measuring student wellbeing
Identifying the impact of SEL, resilience, and other wellbeing-focused programs is essential to ensure efficacy, justify the use of resources and identify areas for further development (Askell-Williams et al., 2013). However, while assessment of student academic ability is commonplace and a largely accepted practice within schools (Thompson, 2013), there is less consensus around assessing wellbeing-related aspects. The known prevalence of mental health concerns among young people worldwide indicates that any large school-based study will include a significant proportion of distressed students. Although identification of potential distress can permit early intervention and the provision of support for the young person and their family, researchers and other stakeholders–including parents, school leaders, ethics committees and community groups–face numerous complexities around the broader moral, ethical and legal implications of mental health information.
First, an ongoing challenge lies in identifying what information does and does not indicate distress. For some students, mental health questions might present minimal risk (Kuyper et al., 2012) or be positively appraised as legitimising their experiences and enabling helpful actions (Haller et al., 2007). But for other students, simply asking such questions might lead to a variety of negative reactions and consequences, including significant levels of psychological distress, stigmatisation or abuse at home or school (Morris et al., 2012; Moses, 2010).
Second, best practices for addressing concerning responses remain unclear. School-based assessments might include validated psychological measures and free response questions that imply various levels of distress. However, such measures are not diagnostic–only a trained professional may diagnose mental illness, so such measures can only suggest mental health concerns. There is little guidance as to when a quantitative score or qualitative comment warrants further action, especially when those responses were provided confidentially. When signs of distress appear, what information should be shared, with whom and how, to maximally maintain both the privacy and safety of the young person?
Third, when surveys include identifiable information, students might alter their responses to align with socially desirable or expected responses, resulting in the over or under reporting of mental health concerns. For instance, Lothen-Kline et al. (2003) found that changing the consent form mid study to include provision for disclosure of positive responses to a question on suicidal thoughts resulted in fewer young people responding affirmatively to the question after revision (1%) versus at baseline (8%). Anonymity may be considered useful in eliciting honest data and securing participation, but also makes it impossible to provide support to those who might need it.
Fourth, if information is disclosed, students, parents, teachers or school leaders who receive sensitive information may need assistance in understanding the information and in taking appropriate follow-up actions. Indicators of abuse or family violence might indicate behaviours or mental states that legally must be reported, requiring additional time and resources. Teachers and school leaders who receive such information may grapple with feeling under-skilled, unprepared and under-supported to respond to student needs (Hanson et al., 2008; Kenny, 2004; Randolph and Gold, 1994), especially among highly demanding and time-limited teaching schedules combined with the emotional burden of exploring sensitive topics with students (Cahill and Dadvand, 2020; Heath et al., 2017; Jaycox et al., 2006).
Given these concerns, it is not surprising that researchers may avoid collecting identifiable sensitive mental health information when conducting school-based research, especially when the study focuses on social and emotional skills, wellbeing and other positive characteristics. Yet the prevalence of mental illness and the complex issues that many young people are struggling with cannot be ignored. Avoiding assessment and identification of these conditions does not change their prevalence, and potentially leaves the affected persons to struggle without support. We propose that including identifiable sensitive information within school-based health research can have numerous benefits which, when managed effectively, outweigh the potential risks to students, school stakeholders and researchers alike. The question then becomes not whether or not to collect such data, but how to do this well, in ways that minimise harm and maximise social contribution and positive processes for the various stakeholders involved (Becker-Blease and Freyd, 2007; Black and Black, 2007).
The current study
To provide guidance for including psychological distress measures within large-scale school-based studies, we draw on research conducted within a larger study investigating the uptake and impact of a school-based SEL and gender education program (Cahill et al., 2019): the Resilience, Rights and Respectful Relationships (RRRR) (Cahill et al., 2016). RRRR was developed for primary and secondary schools in Victoria, Australia. The program focuses on the development of social and emotional skills, along with positive gender relationships and the prevention of gendered-based violence (DET, 2019 for further details and links to resources and training).
Drawing on an implementation science framework, a research project was developed as a partnership between the University of Melbourne, the Victorian Health Promotion Foundation (VicHealth) and the Victorian Department of Education (DET), funded by the Australian Research Council. The research focused on understanding systemic factors that affect implementation of RRRR, with a secondary goal of collecting comprehensive data about child and youth wellbeing that could be used to develop more robust understanding of the kinds of social and emotional challenges faced, the attitudes and exposure towards gender-based violence and the coping strategies that are utilitsed (Cahill et al., 2019 for details on the implementation research framework and approach). The study used a variety of qualitative and quantitative assessments administered over a 3-year period, which included audits of what the school was doing, student focus groups, teacher interviews and self-reported surveys of teachers and students. Here, we focus on the student surveys to provide an example of how researchers might address the responsibilities associated with collecting sensitive information from students within the context of a study conducted in partnership with an education system.
Method
Student surveys were administered in the third or fourth term during the first 2 years of the project (2017 and 2018). Students completed the surveys during school hours, at a time and place determined by the school. A full opt-in consent process was used, which required active informed consent by both students and their parent/guardian. Ethics approval for the data collection was provided by the ethics committees of the University of Melbourne and DET.
Participants
A total of 2421 Year 4 to 10 students (48.7% female, 47.1% male, 4.1% other/not reported) in 2017 and 1209 students (50.0% female, 48.3% male, 1.7% other/not reported) in 2018 completed the student survey. Participants came from 43 government (public) primary and secondary schools across the state of Victoria. Based on the Index of Community Socio-Educational Advantage (ICSEA), an indicator of social disadvantage, schools ranged from 881 to 1170. 1
Measures
The student surveys included demographic information and questions on positive and negative mental and physical health, social relationships, social and emotional skills, views about gender, bullying and victimisation, coping strategies and help-seeking. Most questions were on a five-point Likert style scale, with higher scores indicating higher endorsement of the item. Questions on bullying, coping and help-seeking provided participants with a list of options, and respondents selected all that applied to them. Although the surveys were mostly quantitative in nature, the surveys ended with an open free-response question: ‘Anything else you’d like to tell us?’
The surveys included the Kessler Psychological Distress Scale six-item version (K6), which is a self-reported measure intended to detect the possible presence of anxiety and/or mood disorders, appropriate for use with general populations (Australian Bureau of Statistics, 2012). The scale asks respondents to indicate the extent to which they felt nervous, hopeless, restless or fidgety, depressed, that everything was an effort and worthless over the past 30 days. The items are scored on a five-point Likert scale (1 = none of the time, 5 = all of the time). Total scores are calculated by summing scores across the six items, with higher scores indicating greater psychological distress, and scores 19 and above indicating probable severe distress. 2
The K6 has superior sensitivity and specificity in its ability to identify cases of severe mental illness in adult samples when compared against other validated measures of distress including the General Health Questionnaire (Goldberg and Williams, 1988) and the Composite International Diagnostic Interview (Kessler et al., 2003). While robust evidence around the reliability and validity of the use of the Kessler Scale among child and adolescent populations is still emerging, a number of studies with adolescents have found the measure to have a similar distribution and internal consistency to adult samples (Chan and Fung, 2014; Green et al., 2010; Mewton et al., 2016; Peiper et al., 2015), and suggests that the measure can be useful in identifying struggling adolescents (Mewton et al., 2016). Importantly, the K6 is a screening tool only–while it may be indicative of potential distress, it cannot diagnose mental disorder.
Design considerations
The design of the student surveys was informed by several factors. First, RRRR aims to develop social and emotional wellbeing, positive coping and help seeking behaviours, and respectful relationships. The surveys intended to capture these components, before the schools began implementing RRRR (i.e., 2017) and as the program was in progress (i.e., 2018). However, only a small number of students could be matched across the two time points. As such, the surveys should be considered as two snapshots of student wellbeing and functioning, rather than testing the effects of the program on student functioning.
Second, the target cohort ranged from Year 4 to 10 (ages 9–16). As these ages include a broad developmental period including varying levels of cognitive function and reading abilities, it was essential that scales relevant to both children and adolescents were selected, with question wording piloted and adjusted to be understandable by Year 4 students. To ensure understanding, experts on our team with specialty in child development reviewed all items, refining words that might be harder to understand, and used cognitive interviews with a small number of children to test questionable items. For Year 4 and 5 students, teachers read aloud the questions and explained any unfamiliar terms as their students completed the survey. While we tried to make the questions accessible across literacy levels, it is possible that the questions were challenging for those with low literacy levels, regardless of their developmental stage. We thus considered both quantitative and qualitative data in guiding decisions and actions.
Third, as the surveys were to be administered in the classroom during school time, school staff had to provide sufficient time and support for administration. As such, it was important to balance reliability and fidelity of existing scales with the burden that long surveys create for students and staff. To reduce fatigue, the 2017 survey was administered in two sittings, with each part taking students 11 to 21 minutes to complete. For 2018, we reduced the number of items, using the most reliable and informative items, such that the survey could be completed in a single sitting. In both years, primary students received a shorter version of the survey than secondary students.
Fourth, after providing demographic information, questions were ordered to ask a series of wellbeing-related questions, with indicators of distress and bullying/victimisation in the middle of the survey, followed by additional wellbeing-related questions. This ordering intended to place sensitive mental health information after a sense of trust has been established, while ending on a positive note. The surveys ended with a free-response question allowing students to provide any additional comments.
Fifth, the survey was designed to be administered online, though a few schools opted for paper-based versions. Online surveys are often the preferred method for students (Roberts and Allen, 2015) and allow for collection of data from students in a manner that may take up less class time (Lefever et al., 2007). To increase engagement, we included colour, pictures, and animation. We also added personalisation to the online surveys by automatically piping participants’ first names throughout the survey (e.g., ‘Chris, great job answering those questions. Now we’d like to hear more about how you think and feel’).
Finally, to allow matching to occur, students were asked to provide their full name, date of birth, and school. The traceable nature of each participant meant that it was possible for us to identify respondents, which added a level of knowledge that would be absent with anonymous administration of the survey. In the 2017 survey, students were assured that identifying information was confidential, only accessible by the researchers and used to match responses over time. The 2018 version clarified limits around confidentiality, as detailed below.
Results
Prevalence of psychological distress
Psychological distress scores were available for 2318 students in 2017 and 1164 students in 2018. Figure 1 illustrates the percentage of students with K6 scores of 19 or above. In both years, about one in five students had high distress scores. Distress rates generally increased at each year level, and secondary students were consistently more likely to report high levels of distress (~25%) than primary students (~15%). Prevalence rates of distress in our sample are comparable to existing reports of mental distress of Australian youth, supporting the validity of the data (Carlisle et al., 2019; Lawrence et al., 2015).
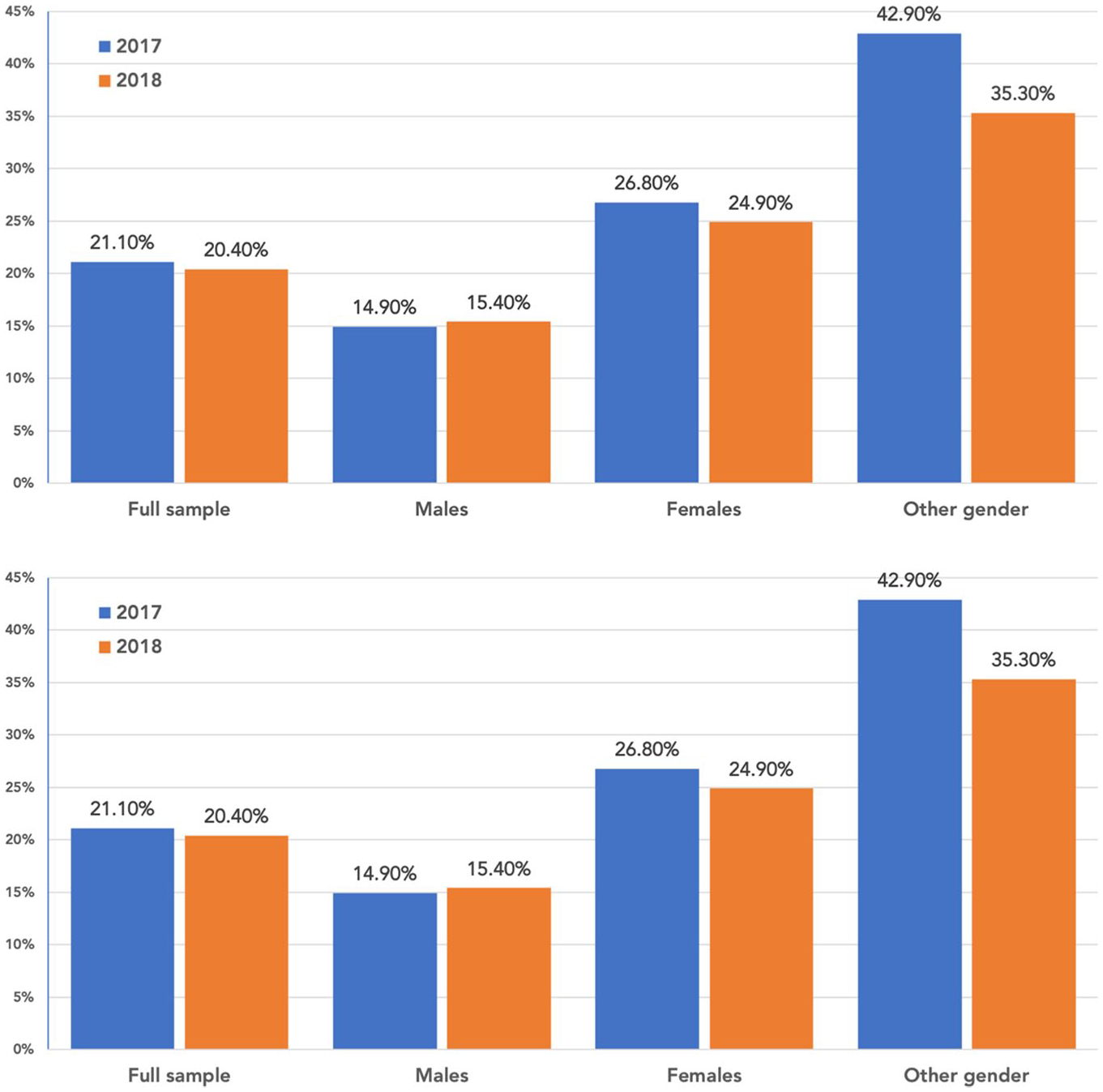
Frequency of reports of high distress as indicated by K6 scores, for the full sample and separately by gender and year level, 2017 to 2018.
Females were approximately 1.5 times as likely as males to report high levels of distress, and the highest rates of distress were reported by students identifying as ‘other’ gender, with 35% to 43% of this latter group indicating probable severe psychological distress. Similarly, studies find higher rates of depressive disorders reported in school-aged young people who identify as transgender, gender non-conforming, and gender diverse, with prevalence rates ranging between 12.4% and 58.2% (Connolly et al., 2016; Rimes et al., 2019; Valentine and Shipherd, 2018). Still, the pattern of results should be interpreted cautiously, as gender diverse students represented only 1.1% of our total sample.
Qualitative indicators of distress
Along with the quantitative K6 scores, a number of responses to the ‘additional comments’ question indicated possible signs of self-harm, exposure to family violence or cries for help. Table 1 provides several concerning examples. Some comments, which were accompanied by high K6 scores, indicated suicidality. Other comments point to family violence and bullying. Importantly, although distressed comments generally accompanied K6 scores of 19 above, distress still appeared at younger ages in students who scored below 19.
Example comments provided by students in the ‘additional comments’ questions indicative of distress.
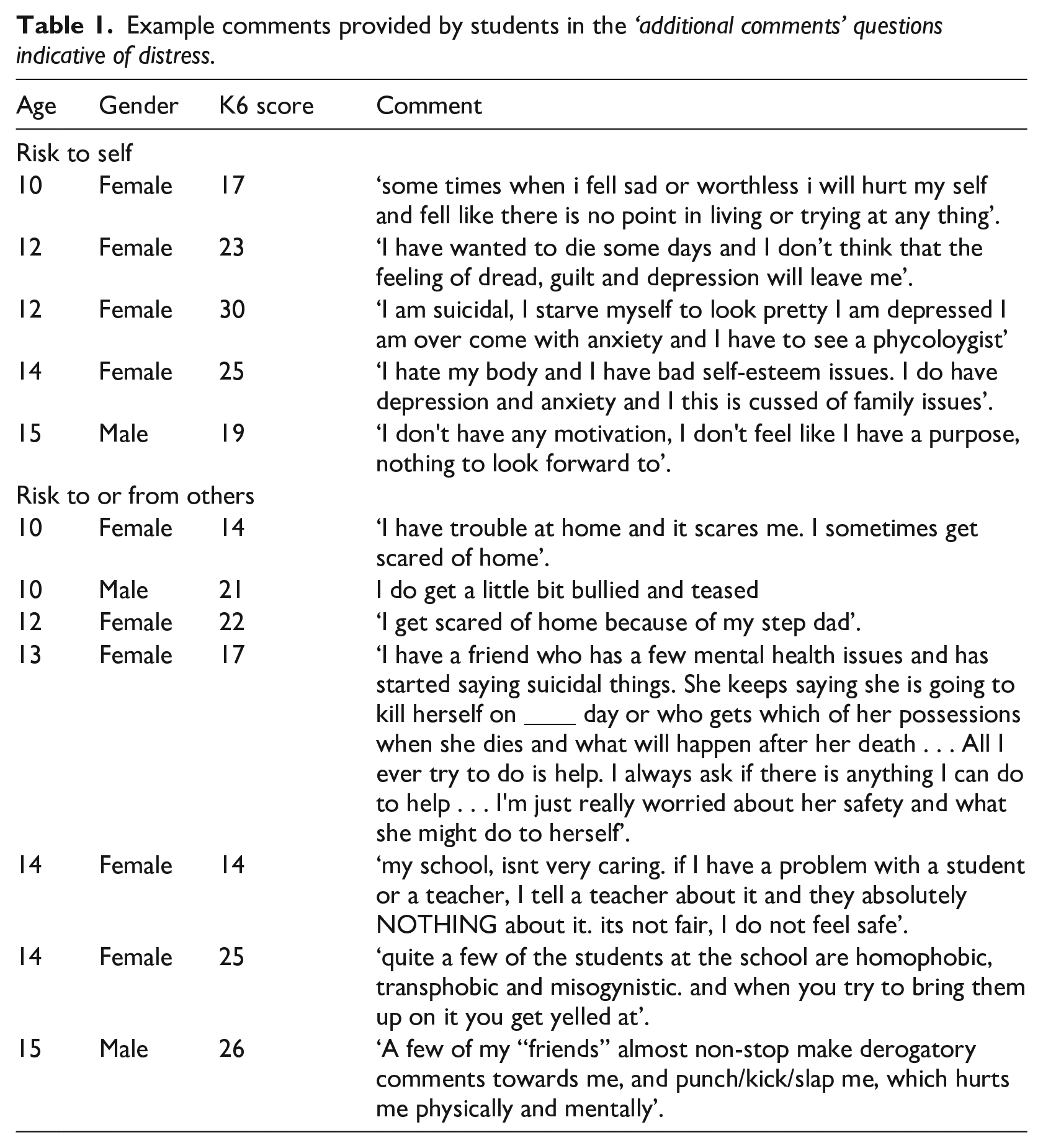
The serious nature of these comments illustrate why concern and hesitation can surround the issue of collecting sensitive mental health data, yet also reflects the importance of doing so. The comments point to the importance of complementing quantitative mental health indicators with qualitative information that allows students add their voice to the quantitative numbers.
Distress and functioning
Table 2 summarises Pearson r correlation coefficients between K6 scores and other variables available in the student surveys, for the full sample and separated by gender across the 2 years. 3 Higher K6 scores were strongly correlated with poor physical and mental health, a lack of meaning/purpose and optimism, feeling unsafe at school and poor body image, and were moderately correlated with a lack of perseverance, disengagement with school, disconnection from peers, teachers, schools and parents, low coping ability and being bullied by others. Only 40% of respondents with high distress scores indicated that they would tell someone when they had a problem, compared to 48% of respondents with lower K6 scores. Distressed students were also less likely to seek help from anyone if serious problems occurred at home (26.3% noted they would seek help from no one, compared to 11.3% of non-distressed students) or if serious problems occurred at school (24.3% noted they would seek help from no one, compared to 9.6% of non-distressed students).
Correlations (Pearson r) between K6 scores and other variables available in the student surveys.
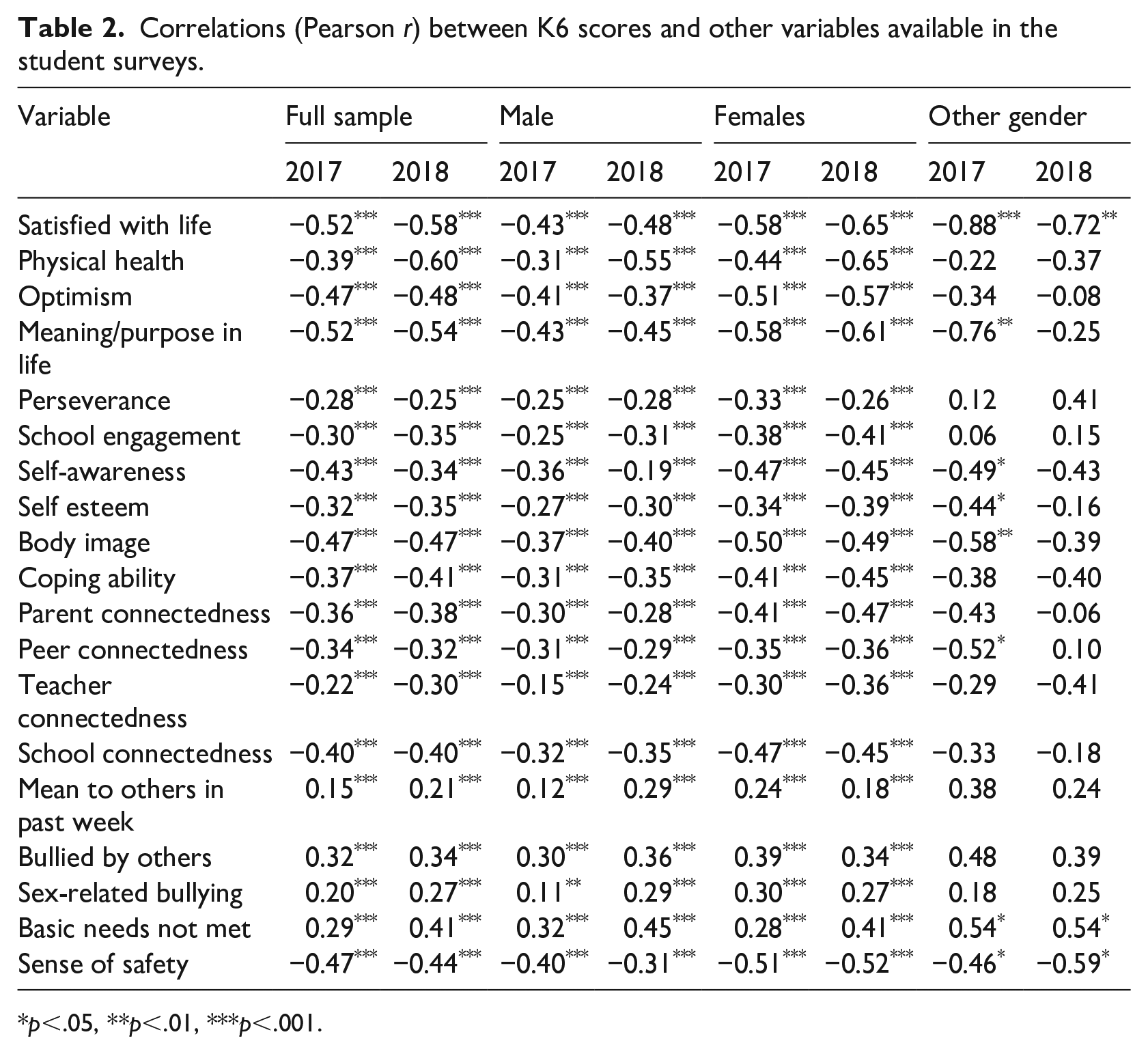
p<.05, **p<.01, ***p<.001.
Given that these students may have fewer coping strategies, were more likely to feel isolated, and had lower intentions toward seeking help from parents, teachers or peers, then it is possible that those with the highest levels of distress may be the least likely to be receiving active social support, and be the least likely to initiate help-seeking on their own behalf. Similar patterns have been identified in other Australian studies on help-seeking (Ciarrochi, 2002). Identifying such students may provide the opportunity for early intervention and needed support.
Development of a disclosure and referral protocol
In accordance with Australian reporting laws, the initial student and parent/guardian consent forms indicated that responses were confidential except where limited by the law. In Australia, mandatory reporting laws require that researchers report to child protection authorities if they hold a reasonable belief that a child has been or is at risk of significant harm as a result of physical or sexual abuse, and that the child’s parents are unlikely to protect that child from abuse (DET, 2018). Beyond these laws, schools and teachers have a duty of care to protect students from risk of injury or harm by themselves or others, and researchers have the ethical responsibility to ensure the safety of research participants.
As the K6 scores indicated high levels of psychological distress for some students, combined with the concerning nature of some of the qualitative comments and the ability to identify students, we felt that we had an ethical responsibility to break confidentiality for cases indicative of possible harm to the student by themselves or others. In consultation with the University ethics committee and lawyers and legal and wellbeing advisors to DET, we developed a protocol for disclosing relevant details to school principals (Figure 2). To ensure timely identification and response, we instigated a weekly checking and reporting system. At each stage, measures were taken to protect student privacy: within the research team, only the chief investigator and clinical psychologist accessed the student names, and only the parties in the designated DET referral pathway and the school principal received the disclosed information. The school principal then worked with the relevant wellbeing staff member or school psychologist to speak with the child and to contact their parents/carers. When flagging students of concern, an explanatory note was provided to indicate that the scores were not diagnostic, but merited follow-up to assess wellbeing and safety and to establish protective supports or services where needed, if not already in place. In cases where a student comment (rather than the K6 score) evoked concern, this was noted in the information provided.
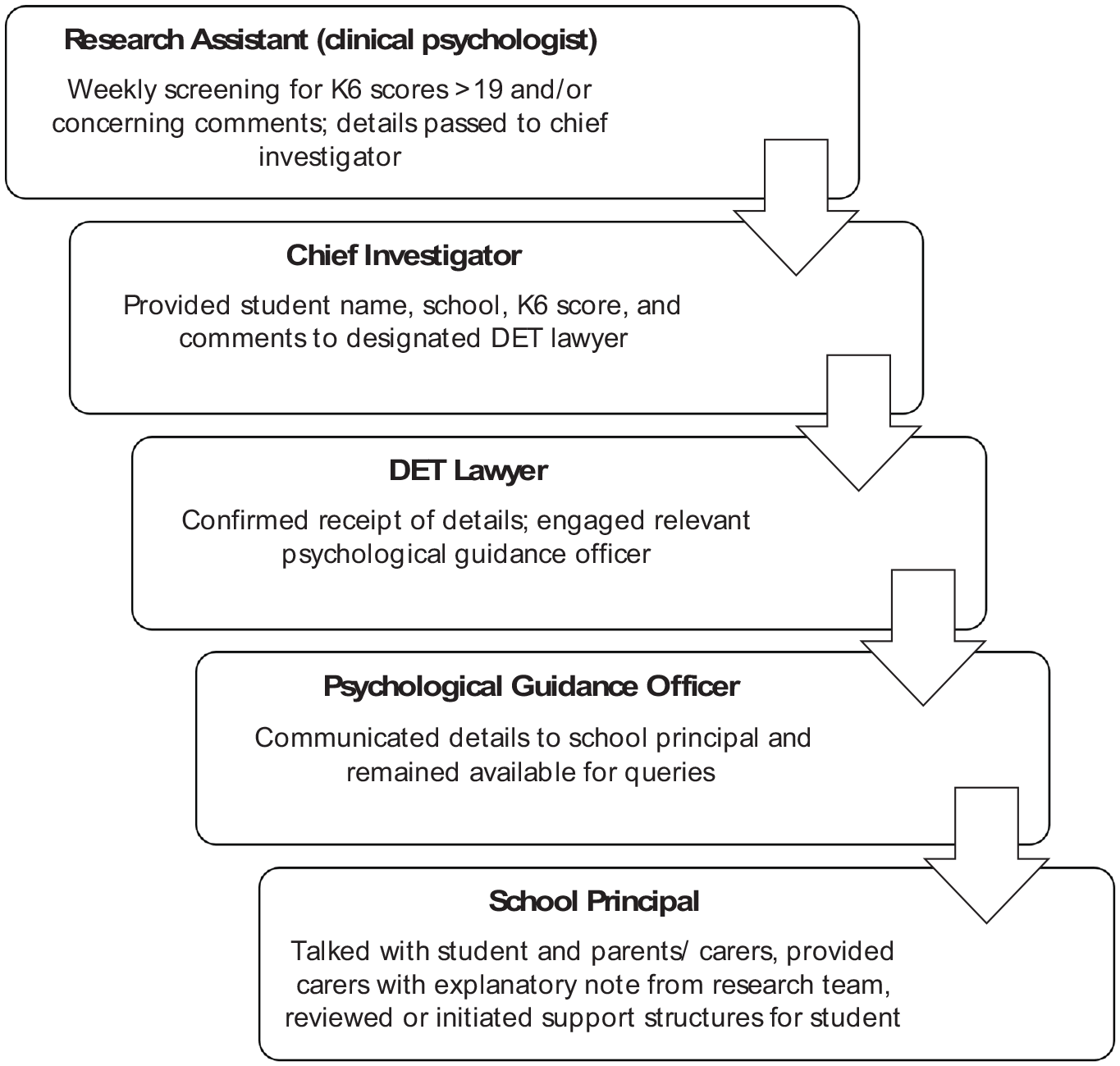
Protocol for disclosing distress details to relevant school principals.
To ensure transparency, a more explicit form of consent was re-obtained from students and parents for the second wave (2018). As illustrated in Figure 3, the revised plain language statement was adjusted in the second wave to clearly indicate that full confidentiality was not ensured in cases of concern for safety and wellbeing, and to describe the reporting pathway that would be used.

Plain language statement about confidentiality across the 2 years.
Reactions to the referral protocol
School principals informed us that many of the identified students had already been identified by the school and were receiving wellbeing support. However, some students came to their attention, providing an opportunity for intervention and support. Some principals reported that parents who had been contacted were appreciative that the information had been communicated out of concern for the wellbeing of their children. Other secondary school principals were initially concerned at the number of distressed students that were identified, wondering if this reflected a school-level problem; however, these concerns were alleviated when we shared Australian prevalence patterns, which aligned with their data.
Discussion
As SEL and other wellbeing programs increasingly are used in schools, the inclusion of self-reported surveys can be helpful for understanding students’ strengths and weaknesses, assessing change in functioning and social and emotional capabilities over time, evaluating program efficacy and informing practices (Kern et al., 2018). Asking about mental health can provide important insights. For instance, in the current study, distressed students also struggled in other social and emotional areas, were more likely to be disconnected from others, and were less likely to feel safe or to endorse reaching out for help and support. As mental illness increases the risk of suicide (Too et al., 2019), early detection and intervention through school-based research could save lives and enhance the quality of lives lived. However, possession of this knowledge also brings a range of challenges and responsibilities.
Identifiable mental health information within school-based online surveys
Identifiable mental health information indicative of potential distress, harm or abuse raises questions around mandatory reporting requirements, privacy concerns and time and resource demands needed for appropriate follow-up. Researchers are met with several options. They might choose to exclude all identifiable information and opportunities for open-ended comments, such that responses are completely anonymous, exclude sensitive mental health information, or carefully collect identifiable sensitive information.
Electing for full anonymity where there is a very real possibility of collecting indicators of potential psychological distress, nonetheless, raises ethical questions about the choice made by the researchers to not know (King and Churchill, 2000). Considering students in our study who recorded high distress indicated lower coping ability and less likeliness to seek help, the inclusion of mental distress measures might identify those struggling individuals who would be the least likely to seek support. Arguably, if the questions elicit information about potential or actual harm to the respondent or to others, then researchers have an ethical obligation to address that information. Yet follow-up with vulnerable children can only occur if students are asked directly (through established psychological screening questionnaires) or indirectly (through qualitative questions that give rise to student voice) about their functioning, and only if that information can be linked to the student.
We found that it was important to have clear structures in place, which provided necessary information but also protected student privacy to the greatest extent possible. For instance, one school requested access to the full set of survey responses from one student of concern, citing the interest of that student’s psychologist. To protect the young person’s privacy, this request was refused, but a copy of the survey instrument itself was provided so that the psychologist could use similar questions in their assessment of the student’s needs and concerns.
Risks and challenges of identifiable mental health information
Ongoing stigmatisation about mental health, family violence, gender-based violence and related issues makes mental health information sensitive in nature, bringing a number of risks and challenges that researchers and schools need to carefully consider and manage.
First, education systems and schools may lack support structures and resources to provide adequate and timely care to students exhibiting signs of high distress in the quantitative or qualitative component of the survey. In many Australian schools, counsellors and school psychologists can only see a limited number of students and are often ill-equipped to manage the large number of students that might disclose distress if a large-scale survey across the school occurs.
Second, the interactive nature of an online survey may create the misleading expectation among participants that disclosure will activate a more immediate, direct and helpful response than is possible (Kauer et al., 2014). It is possible that respondents presumed the online survey to be a reciprocal mode of communication, with expectations that disclosure will be immediately acted upon, aligned with other online experiences. For instance, one student wrote, ‘I hate my life please someone help me’! For some students, their response on a survey might be their first experience of disclosure, and a weak response might diminish the likelihood of seeking help in the future.
Third, disclosure of mental health concerns could lead to stigmatisation. Across cultures, mental illness, sexual abuse and family violence have long been stigmatised, resulting in various forms of discrimination and exclusion that can persist across the lifespan (Hinshaw and Cicchetti, 2000; Koschorke et al., 2017; Patton et al., 2016; Schomerus et al., 2012). Depending on the background, beliefs and experiences of the young person’s parent, such disclosures can also lead to repercussions at home (Kokanovic et al., 2006; Moses, 2010). Even as recent years have brought attempts to destigmatise mental illness, stigmatisation remains a common fear and reality for those experiencing mental health issues (Reavley et al., 2015). Care needs to be taken in the disclosure process to mitigate risk of stigmatisation by peers, teachers, parents and others.
Fourth, the breaching of confidentiality might cause students to lose trust that their privacy is respected, which could lead them to conceal distress in future. For instance, it is possible that the revised consent form that we introduced at Time 2 might have impacted upon willingness to disclose distress. Review of the data showed that for those students with normal range scores at Time 1, 2.9% skipped the distress questions at Time 2. In comparison, 5.2% of students who had high distress scores at Time 1 skipped the distress questions at Time 2. This could indicate that a small number of those who recorded distress scores at Time 1 chose to avoid answering those more sensitive questions in Time 2, precluding any sharing of possible distress. Still, the majority of students who disclosed high distress at Time 1 remained willing to disclose distress at Time 2.
Fifth, the effective management of sensitive information involves additional labour costs to address screening and follow up of survey responses. Our process included weekly checking by a research assistant, communication time for the chief investigator, DET lawyer and guidance counsellor and additional pressure placed on school principals to follow up and put structures in place to provide care to the students, with likely ongoing involvement by wellbeing staff.
Rights and protection of young people
A challenge of research is to respect the rights of young people while protecting them from potential harm. Respondents have the right to confidentiality, but confidentiality is not absolute. The law in many jurisdictions imposes limits, especially when children are involved. But beyond legal obligations, the nature and extent of those limits are, for the most part, reliant on the judgement of the researcher. By virtue of their lack of power relative to adult researchers, young people are afforded special consideration aimed at protecting them from exploitation and harm.
The United Nations’ (1989) Convention on the Rights of the Child informs understandings of children’s participation and protection rights. The articles put forth by the Convention have important implications for research. Children deserve to be properly researched, with respect for their human rights, including rights to privacy, to be protected from harm and for their best interests to be central to all decisions affecting them (Abebe and Besselle, 2014; Beazley et al., 2009; United Nations, 1989). To do this well, researchers are often guided by the ethical principles of beneficence and non-maleficence. Beneficence obliges researchers to act for the benefit of others (King and Churchill, 2000), whereas non-maleficence obliges the researcher to not cause harm and to take steps to stop existing and circumvent foreseeable harm (Beauchamp and Childress, 2001).
However, what constitutes benefit and harm are not clearly defined, and how they are interpreted and applied in different contexts is contingent on the values and beliefs of the researcher (Hiriscau et al., 2014; Williamson et al., 2005), which diverge considerably across researchers (Cashmore, 2006). Finkelhor et al. (2016) describe three broad positions that researchers may orient towards: (1) a minimalist position, in which there are no ethical obligations to offer help as long as the child is no worse off than prior to entering the study; (2) a middle position, in which researchers rigorously assess the level of harm or potential harm both to the participant and more broadly to the study prior to intervening to offer help and (3) a maximalist position, in which the researcher has an ethical obligation as soon as a child discloses potential danger to ensure the removal of that danger. The minimalist position privileges the right of the child to share information, secure in the knowledge that it will remain confidential. But this position can result in under-protection and continuity of harmful circumstances. The maximalist position emphasises protection, which can occur at the cost of privacy. The middle position considers the fundamental right of the young people to the promised confidentiality, the potential negative as well as potential positive consequences of sharing the information with others, and the overall impact on the study aims. We followed the middle position, carefully weighing the issues involved and then opting to break confidentiality, while taking extra steps to protect and respect the participants.
Young people’s views about the correct position may depend in part on their own characteristics and the issues involved. For example, in a study of young child abuse survivors, 90% of respondents wanted absolute confidentiality and 70% said confidentiality should never be broken (Matthew et al., 2019). Notably, the perspectives of children and young people are rarely heard within this debate. Future studies will benefit from including young people in navigating decisions about and tensions around whether, when and how to share concerning information.
Recommendations for ethically incorporating distress measures
We end with recommendations for the ethical incorporation of distress measures within large scale, online school-based surveys, based upon our reflections on our experiences in working through the processes reported here. First, efforts should be taken to carefully examine the tension that exists in maintaining confidentiality, privacy and duty of care obligations. Forward thinking on the part of the research team is needed to clarify the situations in which it would be appropriate to break confidentiality and report potential concerns. We did not initially plan to refer students of concern, but the qualitative comments in association with high psychological distress scores raised considerable concern, and we deemed it ethical to act. It would have been advantageous to have determined and communicated this process before we commenced the research.
Second, consideration should be given to the methods used to pass on information within the constraints and affordances of the given context. We sought guidance from our ethics boards and lawyers to ensure that we referred students of concern in a manner that best managed maintenance of privacy and safety, in ways that were also appropriate to the context and resources of the specific educational system.
Third, timely identification and reporting is necessary to maximise the potential for early intervention and the possible urgency for students who may be suicidal or encountering abuse or family violence. We instigated a weekly process of checking incoming data during the data collection period in the second year of our study, but in hindsight should have instigated this from the beginning.
Fourth, there is a need to consider how referrals will be understood by schools and parents. We provided detailed information about the measures used, emphasising that the K6 is not diagnostic of mental illness. It is possible that our approach for identifying at risk students would result in false positives, with K6 scores indicating distress, but in reality students did not understand the questions being asked or did not take the survey seriously. In corresponding with the schools, we emphasised that while the scores and comments indicated a higher possibility that the young person was experiencing psychological distress that might warrant follow-up and support, dysfunction should not be assumed.
Fifth, labour implications for both schools and research teams should be considered and costed into research projects, along with consideration of methods that might be needed to ensure adequate training and resourcing of staff who may receive such information. Ideally, in the lead up to data collection, the research team would work with the education system and schools to review or develop processes to ensure timely, sensitive and well-managed responses to student disclosures, if and when they occur.
Sixth, student and parent consenting parties need to be fully informed of why and how confidential data may be passed forward. In our study, students and their parents consented that information was only confidential to the point of law. However, in the second round of data collection, we provided a more explicit statement of what this actually meant, detailing the process that would be used to pass on concerns.
Seventh, consideration should be given to the presumptions that young people have when invited to share personal information via online surveys, and how those presumptions might impact upon their willingness to disclose sensitive information or use the survey as a form of help-seeking.
Finally, both in the case of program evaluation and broader research projects, ethics review committees should be aware of the issues raised through our study and consider implications for protocol approvals and reviews. Questions related to mental health and wellbeing, whether focused on positive or negative aspects, potentially can invite disclosures by participants that need to be carefully managed. Consideration should be given to the nature of the information that students might disclose within the medium, with acknowledgment that the mediums themselves continually evolve and may influence the likelihood of disclosures. The importance of hearing cries for distress must be balanced against the risk of eliciting disclosure without providing support. We suggest that risks around sensitive questions should not prevent such questions from being included, but rather protocols should be in place to support student voice, while also ensuring that students and parents understand limitations to privacy and how to access support services if needed.
Conclusion
While online surveys are an efficient and practical method for collecting data for educational research, conducting large-scale online surveys with students raises unique ethical considerations. Our study provides guidance on how to capture sensitive information in ways that minimise potential harms and maximise potential benefits, and how to manage the responsibilities that come with such knowledge. Asking directly about safety and mental health information, in a manner that is identifiable and includes both quantitative and qualitative information, provides a way to identify students who might be in need of protection or additional support. However, eliciting this knowledge also brings a number of responsibilities. Researchers must be prepared to act on this knowledge in a manner that is in the interests of the young person, informed by ethical and legal guidelines, and conducted in partnership with those in ongoing care relationships with the respondents.
Supplemental Material
K6_challenges_benefits_Appendix_1 – Supplemental material for The responsibility of knowledge: Identifying and reporting students with evidence of psychological distress in large-scale school-based studies
Supplemental material, K6_challenges_benefits_Appendix_1 for The responsibility of knowledge: Identifying and reporting students with evidence of psychological distress in large-scale school-based studies by Margaret L Kern, Helen Cahill, Lucy Morrish, Anne Farrelly, Keren Shlezinger and Hayley Jach in Research Ethics
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Australian Research Council Linkage Grant #LP160100428 (Helen Cahill Principle Investigator), with industry partners the Department of Education and Training Victoria and VicHealth Australia. All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]() .
.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.