
Abstract
Incentivising has shown to improve participation in clinical trials. However, ethical concerns suggest that incentives may be coercive, obscure trial risks and encourage individuals to enrol in clinical trials for the wrong reasons. The aim of our study was to develop and pilot a discrete choice experiment (DCE) to explore and identify preferences for incentives. A DCE was designed by including following attributes (and levels) of incentives: value, method, and time involvement. To account for trial benefit and risk, each was included as an attribute with levels low, medium and high. For testing purposes, the DCE was administrated using SurveyMonkey in a population of third level students. A total of 245 students, representative of the general student population, participated in the online DCE. The results provide a template to assess and explore the use of different incentive methods in clinical trials. The template can be used in its current format or adapted to particular scenarios. This pilot study provides a feasible methodology to explore the use of incentives for participation in clinical trials and can be adapted to specific trial requirements to provide information for ethical applications or identify the most favourable incentive for participation in clinical trials.
Introduction/background
According to the 1947 Nuremberg Code, no persuasion or pressure of any kind should be put on clinical trial participants (Moreno et al., 2017). Incentives in research are defined to be payments, recompense and rewards (Bower et al., 2014). In this context, incentives for patients may be seen as coercive, or as exerting undue influence on potential participants’ decisions about whether to take part in research (Singer and Bossarte, 2006; Singer and Couper, 2008). Whereas incentives for physicians are generally well accepted, to compensate for increased workload and/or time, incentives to encourage patients to participate in health research or clinical trials are often disfavoured (Wertheimer and Miller, 2008).
Incentivising the consent procedure has shown to improve recall in participants, particularly in relation to potential serious side effects (Festinger et al., 2009). The research participants’ motivation is superior to the influence of payments and financial rewards do not distort the participants’ behaviour or blind them to the risks involved with research (Ballantyne, 2008). A study using lottery tickets as an incentive to return a mail questionnaire had an opposing effect as the intrinsic motivation of the respondents was already high (Wenemark et al., 2010). Other use of incentives to improve questionnaire return was tested by the inclusion of a dollar note or a lottery ticket with the dollar note and these inducements had a slightly higher impact but either better than no incentive at all (Whiteman et al., 2003). Incentives can also improve the generalisability reflected in a study in which the inclusion of a scratch lottery tickets improved survey response and representativeness through the participation of more respondents who had lower education (Olsen et al., 2012). The use of incentives in questionnaire surveys is an accepted practice and a meta-analysis concluded that researchers should consider including small amounts of money with mailed questionnaires rather than give no incentive at all (Edwards et al., 2005).
Incentives are however more questionable when participants find themselves in a dependency relationship with the researcher (or physician), where the risks are particularly high, where the research is degrading, where the participant will only consent if the incentive is relatively large because the participant’s aversion to the study is strong and where the aversion is a principled one (Grant and Sugarman, 2004). It is therefore important to be transparent and describe any system of payment or reimbursement in detail (Draper et al., 2009).
The use of financial incentives in clinical trials is not well studied and generally less accepted. Hospital- or community-based trials need to take extra care to avoid incentives that may be coercive or unduly influence research participants (Bernstein and Feldman, 2015). Incentivising patients may include payment for time to participate (for its potential motivational benefits), small gifts, payment for incidental expenses, cash or voucher incentives for participation and retention. A recent study reported current practice and future priorities to improve patient recruitment and retention in clinical trials (Bower et al., 2014) and concludes that the scope for testing incentives through formal experimental methods may be limited by ethical and equity considerations. Concern was more often expressed when payment was described as ‘substantial’ compared to ‘tokens’ and gift cards (vouchers) and non-monetary gifts were not considered to influence participation (Largent et al., 2012). Interestingly however, a larger amount offered as an incentive was not found to be more efficacious in motivating a subject to participate (Wertheimer and Miller, 2008). It is important to acknowledge that incentives work both ways: patients feel acknowledged for their participation and are more encouraged to invite eligible patients into a trial (Rendell et al., 2007).
Ethical committees or institutional research board members often struggle with concepts of reimbursement and incentivisation. While members may agree with reimbursement or compensation for time and inconvenience, they may not agree with payment for participation or compensation for risk (Largent et al., 2012). Undue influence as well as coercion were considered to be violated with the offer of payment even though the literature reports payment of participants highly effective and securing participation (Bentley and Thacker, 2004). This paper is of particular interest as it considers if and how monetary payments influences subjects’ participation and risk evaluation. This ‘willingness to pay’ analysis presented three imaginary studies varying the levels of risk and monetary payment and 207 students were asked to answer a number of questions on their study–risk combination. This paper concludes that (higher levels of) monetary payment increased students’ participation in research irrespective of the risk of the study. This study was limited by proposing studies for healthy volunteers, which may have affected the lack of attention to risk.
Difficulties with research to determine the use of incentives for participation include working with ‘example’ studies to convey different levels of risk and the need for large samples. Taking some of the limitations into account, we explored alternative options to study choice and gain a better understanding of the elements involved in choice-making (Hensher et al., 2005). Discrete choice experiments (DCE) are widely used in health economics to assess preferences (Clark et al., 2014). DCEs have gained attention with the increasing interest in public and patient preferences to inform clinical and policy decision-making. One advantage of a DCE is that it does not need to work with scenarios but can allow each participant to interpret the study question in their own context.
DCEs can be used to propose choice sets with hypothetical options in relation to incentives introduced in the context of clinical trials. DCE can disentangle stated preferences, or what an individual says they would do, from observed preferences, what the individuals actually does, and compare these to current practice and standards in clinical trials and health research in general. DCEs involve the generation and analysis of choice data in the context of hypothetical scenarios (Louviere and Lancsar, 2009). The first step of a DCE is to select the attributes of interest and their levels. The second step is to combine attributes into choice sets. The combination relies on experimental plan theory as a full factorial design generally implies proposing too many choices to respondents.
Our aim was to develop and pilot a discrete choice experiment to explore and measure the use of incentives to recruit patients to clinical trials.
Methodology
Development of the DCE
A DCE asks individuals to state their preference of hypothetical alternatives, in this case incentives. Each alternative is described by its attributes or characteristics and responses are used to infer the value placed on each attribute. In stating a preference the individual is assumed to choose the alternative that yields the highest individual benefit (utility) (Hall et al., 2004). The choice made by the individual allows the influence of the underlying characteristics on the individual’s decision to be estimated. Comparing all the choices shows how individuals trade-off one attribute for another.
Following best practice in designing DCEs, a qualitative approach was taken to identify attributes and levels in a two-step process. First, international literature on incentives in clinical trials was reviewed to identify all the relevant attributes. For each attribute, potential levels were recorded. This literature review was then used to inform an expert group including experts in trial methodology, health economics, epidemiology, social marketing and statistics. The expert group defined the final research question and identified the most relevant and attainable attributes (Table 1).
DCE attributes and levels.
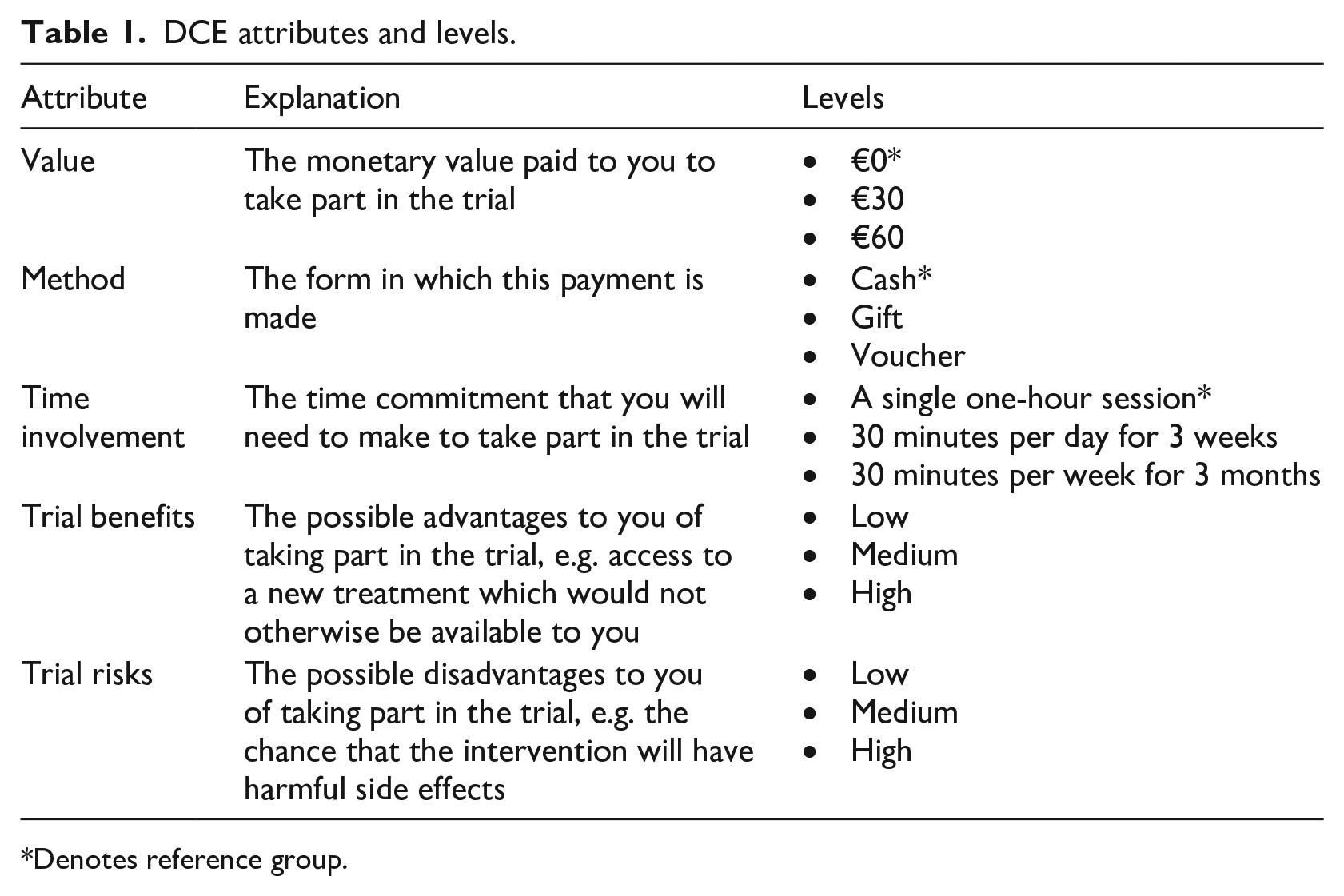
Denotes reference group.
The decision was made to avoid scenarios to confer risk, as interpretation of scenarios is dependent on the individuals’ circumstances (for instance age or gender). A more generalisable approach was taken by introducing the DCE with an introduction to randomised trials. The introduction then includes, ‘for this example, you have been asked to participate in a trial comparing two interventions to improve your health’. Full instructions and an example scenario are provided in Figure 1. To convey a level of risk and benefit, each scenario included these as attributes with three levels (low, medium, high). The attributes ‘benefits’ and ‘risks’ are inherent to each trial, related for instance to the therapeutic effect or adverse effect of an intervention, and cannot be modified by researchers for the purpose of increasing recruitment. However, risk and benefit of the trial influences the decision-making of any prospective participant, so excluding them from the list of attributes would be likely to increase random or unexplainable utility in data analysis (Ding et al., 2007; Halpern et al., 2004). Therefore, risk and benefit were included in the DCE as attributes to allow a correction for these confounders in the final analysis.
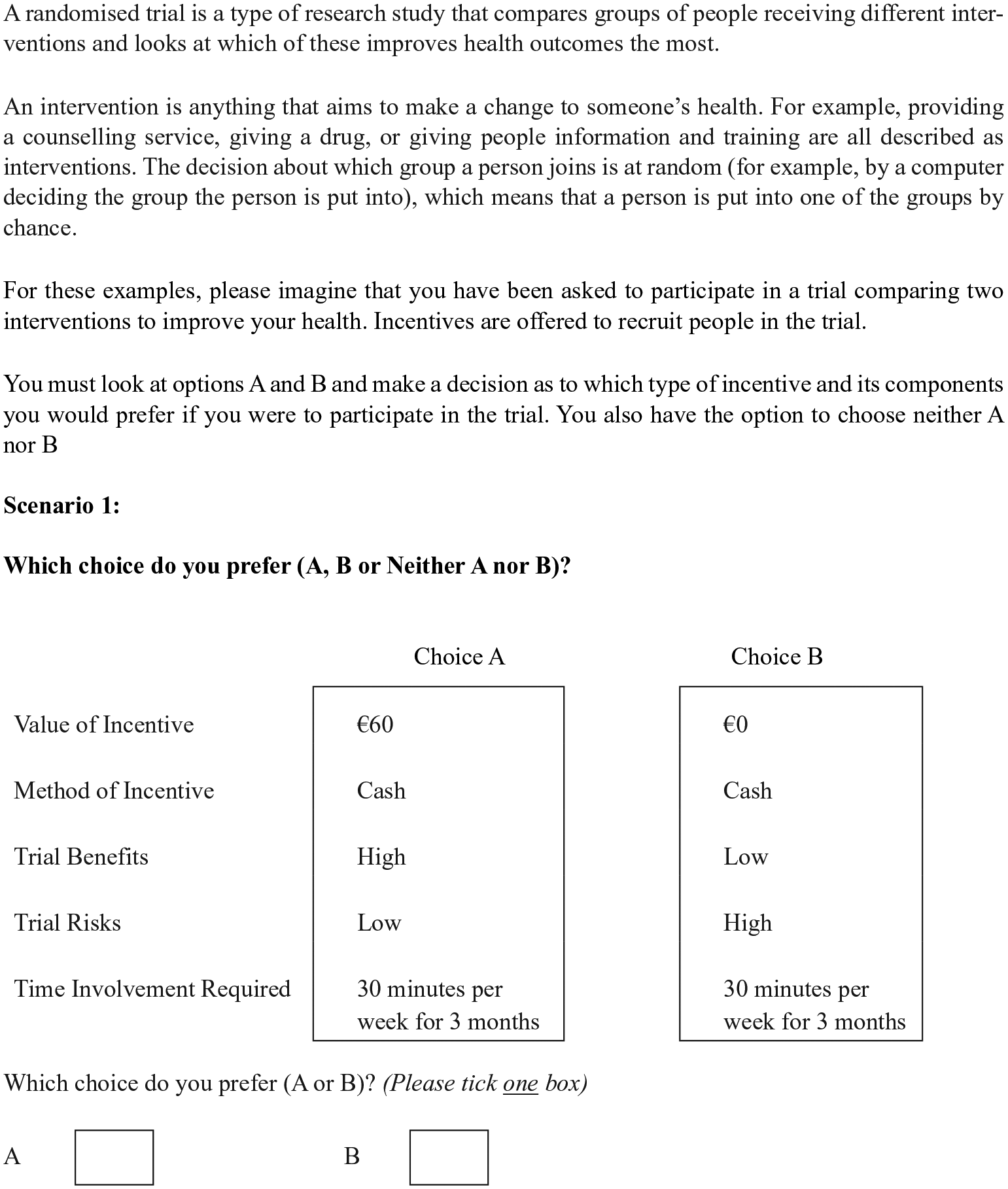
DCE instructions and example of choice set.
To answer the question ‘what preferences encourage people to participate in clinical trials?’ a small-scale study was proposed to test each element of the DCE in a particular population. As each population allows different approaches, the focus of the presented DCE was a student population, allowing for online DCEs and electronic invitations through social media platforms (Facebook, WhatsApp, university mailing list).
Experimental design
The final DCE included the following attributes: value, method, time involvement, trial risk, trial benefit (Table 1). Based on these attributes and levels, a total of 243 (35, 5 attributes with 3 levels) possible options, with a total of 29,403 possible choice sets (i.e. the full factorial design) were generated. We used IBM SPSS version 23.0 to generate the choice sets based on orthogonal arrays. Orthogonal arrays assume that attributes are statistically independent and support the balance of the levels in the final DCE. After discussion, a total of nine scenarios or choice sets with minimal overlap were selected (fractional factorial design) to minimise cognitive fatigue (Bekker-Grob et al., 2012).
The surveys were transferred to SurveyMonkey as images and the individual’s choice (A or B) was recorded electronically. Additional demographic information (age, gender, discipline, educational background, in receipt of study funding, and previous experience with health research) was also collected. Survey links were distributed through the university’s student email system and by sharing the link on Facebook and WhatsApp groups. The survey was live for a seven-day period in respect of the amount of student communication (28 September to 5 October 2017). Ethical approval for the study was obtained from the Social Research Ethics Committee at the University College Cork.
Analysis
The underlying principle of DCEs is based on the consumer theory of demand, which states that when an individual is faced with different choices, he/she will choose the alternative that provides the highest utility (‘happiness’) (Lancaster, 1966). The random utility theory (RUT) is therefore used to analyse and explain choices made in DCEs (Lancsar and Louviere, 2008). The RUT divides utility, a measure of preference, into a random component, due to unobserved attributes or variation between and within individuals or error, and a systematic component. The systematic component is a function of the attributes and its levels and allocates an amount of the variation that can be explained by each attribute.
Each scenario is judged as a bundle of characteristics (attributes/level) to be compared with an alternative scenario. No scenario will present the ideal options, but we assume that the individual will choose the choice set that will provide them with the highest benefit (utility). With each choice set having a different combination, the effect of each attribute level on the chance of the choice set being chosen can be estimated with a random effects logistic regression analysis accounting for multiple answers by each individuals (STATA v13) . The estimated coefficients represent the preference of each attribute level influencing the choice, compared to the lowest (reference) attribute level. This approach limits the number of comparisons and results in two coefficients for each attribute.
A preference heterogeneity analysis was also performed to investigate the influence of selected demographic characteristics. The variability in preferences is investigated by a comparison of the marginal effect of each personal characteristic on the sample level preferences (for instance, what is the marginal effect of studying science on average preference for an incentive). However, this approach results in a large number of comparisons. The use of a reference category as well as restriction in the number of interactions tested, was therefore applied.
Gender (reference: Male)
Discipline (reference: College of Arts, Social sciences and Celtic studies)
Previous experience in clinical studies (reference: No)
In receipt of a study grant (reference: No)
Results
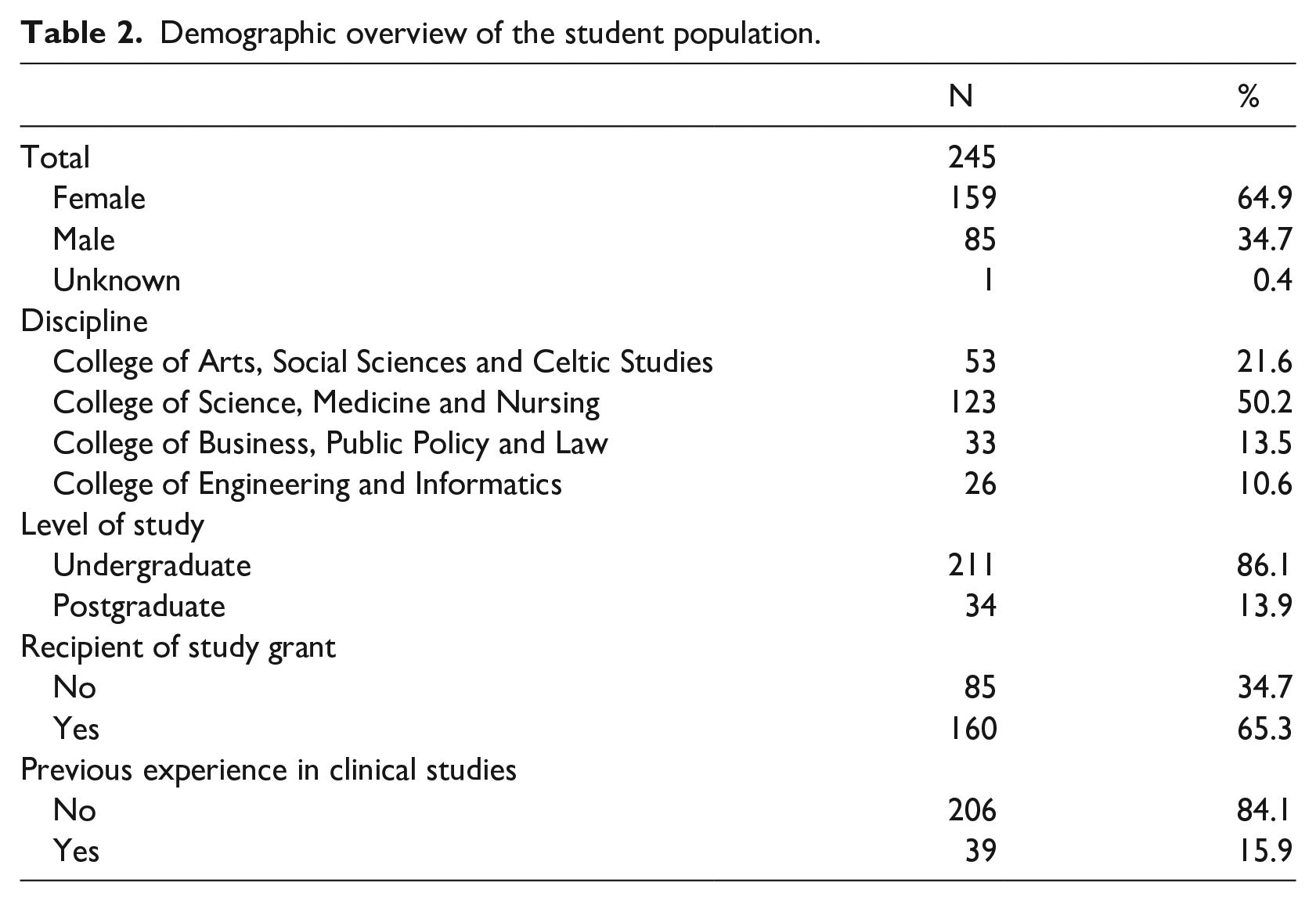
All the questions were answered by 245 students, 159 (64.9%) of whom were female (Table 2). Their mean age was 22, ranging between 17 and 55.
Demographic overview of the student population.
Preference analysis
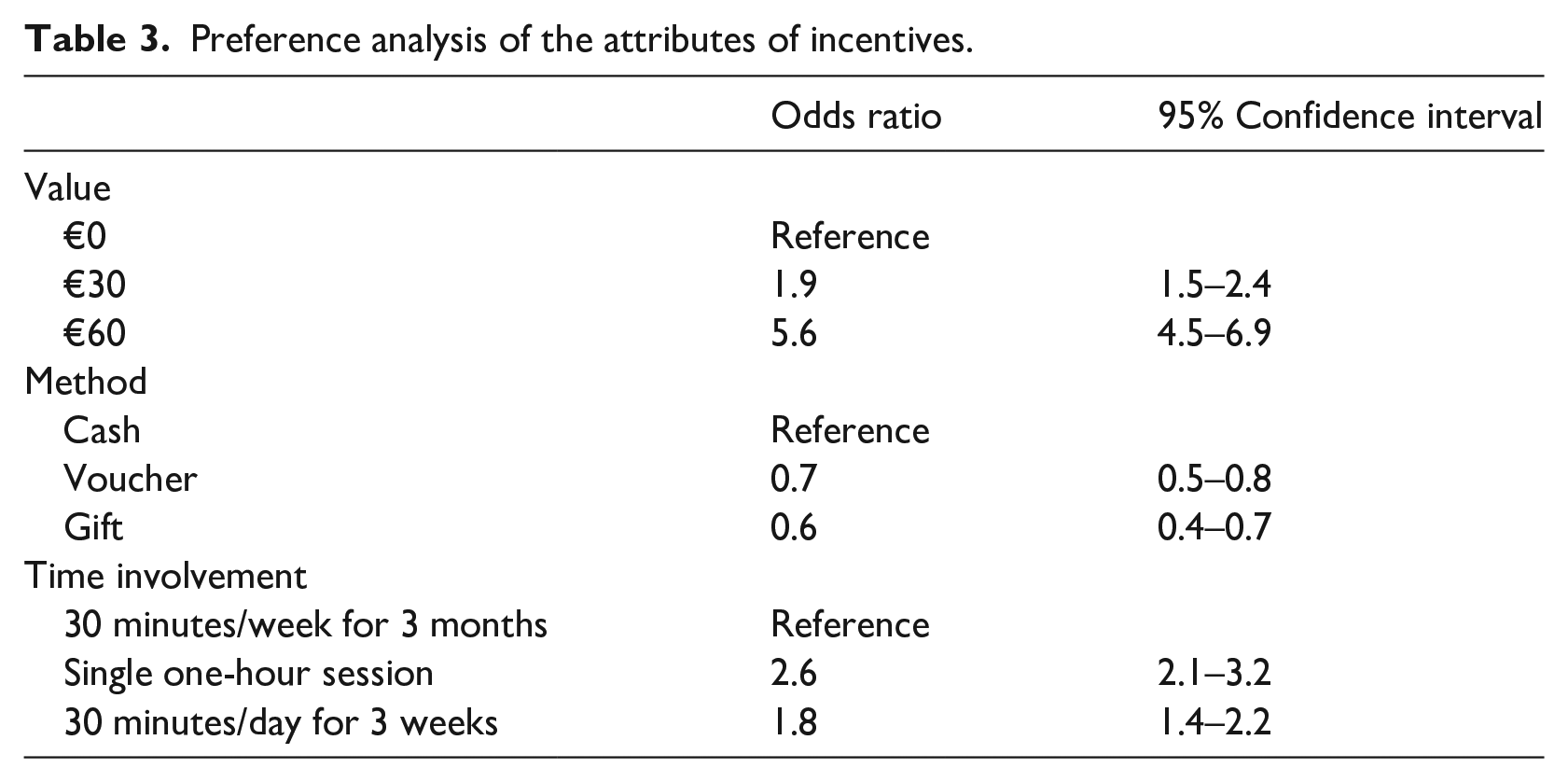
Students prefer an incentive with a higher value and compared to no value, students are 1.9 times more likely to opt for €30 and 5.6 times more likely to choose €60 (Table 3). Students prefer cash compared to vouchers (Odds ratio 0.7) or gifts (odds ratio 0.6). Students prefer a one-off time involvement compared to a 30 minutes per week for 3 months. A shorter duration of time involvement, i.e. daily for 3 weeks versus weekly for 3 months, is also preferred by students.
Preference analysis of the attributes of incentives.
None of the included demographic variables influence the choice of students and no differences between colleges can be observed in relation to value or method of incentive. Engineering and informatics students show a slight preference for a single one-hour session. Level of study, recipients of study grants or previous experiences in clinical studies is not associated with a change in preferences.
Participation in the DCE
A total of 200 out of 245 participants are included in this pilot study; 45 students were excluded as they did not complete the DCE. The largest drop off happened after obtaining the participant information (29); once participants started the survey, most of them finished it (7 drop out after the first scenario, the remaining 9 subsequently).
Discussion
The application of a DCE to assess preferences in incentives has shown to be successful. Despite being a small-scale pilot study, this modified DCE provides insights into how people choose incentives in relation to participation in clinical trials.
The DCE was developed to test, in its broadest application, the variation in the use of incentives, depending on the benefits and risks of the study. For this reason, the DCE did not include a scenario, as previous experiences would be determining the interpretation of risk and benefit. However, the use of scenarios with or without including specific benefits and risks may improve the application of understanding preferences in particular populations or for particular studies. This pilot study provides a template for use in specific studies or trials, or broader implementation to determine preferences.
It is the first time a DCE methodology is applied in this context to explore the value of incentives for participation in a clinical trial. In this study setting the risk and benefit at different levels allows participants’ own personal interpretation of risk and benefit. Other attributes such as levels of monetary incentives, type of incentives and time commitment were pre-set. These attributes as well as their levels could be changed and adapted to other situations to determine preferences for incentives. Limiting the number of comparisons by predetermining the variables of interest as well as setting up models based on pre-specified hypothesis, will help the interpretation and application of a DCE.
In conclusion, we provide a template to explore and determine preferences for incentives for recruitment of participant to clinical trials. The presented methodology will allow researcher to support ethical applications as well as identify the most appropriate incentives for a proposed trial.
Footnotes
Acknowledgements
We would like to thank Dr Darren Dahly, statistician at the HRB Clinical Research Facility Cork and School of Public Health, University College Cork for his help as member of the expert team.
Conflict of Interests
None reported.
Funding
All articles in Research Ethics are published as open access. There are no submission charges and no Article Processing Charges as these are fully funded by institutions through Knowledge Unlatched, resulting in no direct charge to authors. For more information about Knowledge Unlatched please see here: ![]()