
Abstract
How important is the timing of the pretreatment evaluation? If we consider mental health to be a relatively fixed condition, the specific timing (e.g., day, hour) of the evaluation is immaterial and often determined on the basis of technical considerations. Indeed, the fundamental assumption underlying the vast majority of psychotherapy research and practice is that mental health is a state that can be captured in a one-dimensional snapshot. If this fundamental assumption, underlying 80 years of empirical research and practice, is incorrect, it may help explain why for decades psychotherapy failed to rise above the 50% efficacy rate in the treatment of mental-health disorders, especially depression, a heterogeneous disorder and the leading cause of disability worldwide. Based on recent studies suggesting within-individual dynamics, this article proposes that mental health and its underlying therapeutic mechanisms have underlying intrinsic dynamics that manifest across dimensions. Computational psychotherapy is needed to develop individual-specific pretreatment animated profiles of mental health. Such individual-specific animated profiles are expected to improve the ability to select the optimal treatment for each patient, devise adequate treatment plans, and adjust them on the basis of ongoing evaluations of mental-health dynamics, creating a new understanding of therapeutic change as a transition toward a more adaptive animated profile.
Therapeutic change is elusive, but mental-health dynamics are even more so. After several weeks of therapy, many patients wonder whether it is helping them. For example, patients seeking treatment for depression often report having had a few good days, but in the same breath, they add that they also had both good and bad days before the treatment. Are they then in the midst of a positive change or merely following the familiar dynamics of alternating good and bad days as the depression continues? This is a critical question because accurately identifying therapeutic change can motivate patients to continue treatment and confirm for the therapist that the treatment is suited to the patient (Wachtel, 2011). Likewise, both patient and therapist need to know whether exacerbated symptoms are part of the dynamics of depression (“some days are worse”) or an adaptive nonlinear therapeutic process (e.g., Pascual-Leone, 2009), or an indication that the treatment does not work or even causes harm (Castonguay et al., 2010; Cuijpers et al., 2018). Many psychotherapies fall short today not because of a lack of effective treatments but because we do not know how to match the treatment to the patient’s mental health (Delgadillo & Lutz, 2020; DeRubeis, 2019). Despite many recent advances in psychotherapy research (e.g., a variety of algorithms, large samples, repeated measurement during treatment), the improvement of the psychotherapy efficacy has eluded us (Cuijpers et al., 2019; Eskildsen et al., 2020; Nemeroff, 2020; Van Bronswijk et al., 2021). Why?
The Common Design in Psychotherapy Research: Pretreatment Snapshots of Mental Health
The short answer is that even when innovative analytic methods (Z. D. Cohen & DeRubeis, 2018; Huibers et al., 2015; Lutz et al., 2019; Webb et al., 2020) were implemented to assess the patient’s mental state, they were mostly applied to pretreatment measurements taken at a random point in the dynamics of mental health, mostly of one dimension (Hayes & Andrews, 2020). Behind the short answer, however, there might be a theoretical blind spot that needs to be eliminated before the efficacy of psychotherapy research and practice can be further boosted.
Most psychotherapy research conducted in the past 50 years has followed the classical design in which the individual’s mental health is assessed before the start of treatment (Barkham et al., 2021) on the basis of a battery of self-report questionnaires and clinical interviews. These intake assessments capture a snapshot of the patient’s mental health before the start of treatment, after which participants are allocated to a given treatment either by randomization (randomized controlled trials) or by other considerations. The resulting literature in the last decades based on such designs shows that active therapies of many stripes for major depressive disorder (MDD) and other mental-health disorders work for about half the patients, who show adequate improvement in symptoms from pre- to posttreatment (Cuijpers et al., 2021; Nemeroff, 2020), and that active treatments based on widely different mechanisms are about equally effective (Cuijpers et al., 2021) and as effective as drug therapy (Cuijpers et al., 2020). The solution proposed in the last decade was based on precision medicine (Z. D. Cohen & DeRubeis, 2018), according to which, although treatment effectiveness for the average patient does not exceed 50%, for a given patient, the optimal treatment can achieve a much higher efficacy rate (Delgadillo & Lutz, 2020; Zilcha-Mano, 2019).
Great effort has been invested in identifying theory-based moderators that may guide precision medicine. Some of the pretreatment predictors receiving the greatest empirical support are the patients’ interpersonal abilities and tendencies, such as attachment orientation, and symptom severity (Constantino et al., 2021a; Lutz et al., 2021). But these studies continued producing small effects, and researchers (DeRubeis, 2019; Kraemer, 2013; Wallace & Smagula, 2018; Zilcha-Mano, 2019) have argued that focusing on any single variable, however important, amounts to a reduction of the individual. For example, focusing only on attachment orientation, which is an important pretreatment characteristic, reduces an individual to one or two scores and ignores the fact that the given individual with avoidant attachment happens to be male and has a comorbidity of bipolar disorder and poor interpersonal skills. Some have argued that data-driven algorithms may produce better results. Despite some evidence (Z. D. Cohen & DeRubeis, 2018; Constantino et al., 2021b; Friedl et al., 2020; Huibers et al., 2015; Lutz et al., 2019; Webb et al., 2020; Zilcha-Mano et al., 2016, 2018) that this line of research has merit, its benefits are still elusive. Accumulating research suggests that along with its promise (Constantino et al., 2021b; Delgadillo et al., 2021), there are indications that its gains may be limited (Christodoulou et al., 2019; Espel-Huynh et al., 2021; van Bronswijk et al., 2021).
What has been stalling the advance of psychotherapy research? And why can we not substantially and consistently further improve the efficacy of treatment, despite great advances in trial design, measurement, and statistical analyses in the last decades? It is proposed here that one of the critical reasons may be shortcomings in our understanding of mental health. Steady progress has been made in recent decades in both data- and theory-driven approaches, as well as in our strategies for measurement (e.g., repeated measurement of therapeutic change) and analysis (e.g., the use of advanced algorithms). But most of our fundamental theoretical understanding of the individual’s mental health before the start of treatment has remained unchanged. Much of our current understanding describes mental health before treatment on the basis of a single one-dimensional snapshot. It is time for theory in psychotherapy to catch up with our advances in methodology (Hamaker & Wichers, 2017).
Although all mental-health disorders are affected by this lapse, MDD, the leading cause of disability worldwide (Friedrich, 2017) and a highly heterogeneous disorder (Goldberg, 2011), is the focus of this article as a case example. As mentioned above, treatment for MDD fails for about 50% of patients across many types of active therapy (Cuijpers et al., 2021), and this 50% efficacy rate has not changed in decades despite prodigious amounts of research (Cuijpers et al., 2021). The reason is not that evidence-supported therapies are inadequate; after all, they are successful with half the patients. One problem may be with the theoretical assumptions that guide psychotherapy research.
MDD is characterized by a diversity of clinical presentations, possibly reflecting distinct pathophysiologic mechanisms of different individuals (Cuthbert & Insel, 2013; Perkins et al., 2020). It is only natural that treatment applied broadly across these different presentations of MDD (E. I. Fried & Nesse, 2015) is often ineffective. Yet, currently, treatment assignment is mostly guided by a limited evaluation of a snapshot of mental health before treatment that is based largely on self-report measures and clinical interviews (Barkham et al., 2021). There are two problems with this approach: It does not take into consideration the dynamics of mental health, and it does not account for its many trait manifestations. The chances of such a snapshot fully capturing the many fluctuating dimensions of an individual’s mental-health condition are small. We cannot match treatment to a condition we do not properly understand. Our current picture of mental health is based mostly on a static and flattened portrayal of human experience, which in reality has infinite richness and depth. During treatment, when change is anticipated, repetitive measurement is quite prevalent, but before treatment, when no dynamics are anticipated, especially in mechanisms of change, repetitive measurement is still rare.
A Dynamic Multidimensional Understanding of Mental Health
It is now widely acknowledged that mental-health problems, especially MDD, are heterogeneous (Lamers et al., 2012). Two individuals sharing the same diagnosis may differ greatly in many of their traits (Borsboom, 2008; E. I. Fried, 2017; Kotov et al., 2021). It is important to develop an understanding of mental health to guide psychotherapy research that is based on a multidimensional mapping of patient mental-health dynamics. A one-dimensional snapshot cannot fully capture an individual’s mental health before the start of treatment, no matter how representative it may be of the individual’s mean level of mental health. The individual’s mental health is made up of a dynamic configuration of features from a range of domains (psychological, physiological, etc.), each one assessed by its own measure. The theoretical model we use for understanding mental health is fundamental to any understanding of therapeutic change. Challenging the current one-dimensional-snapshot theoretical conceptualization and shifting to one that accounts for the dynamic multidimensional nature of mental health may improve our understanding of how to personalize treatment and increase its efficacy.
The First Pillar of the Proposed Understanding of Mental Health: Mental Health Is Dynamic
It is generally accepted that the stage in the change cycle (Prochaska et al., 2007) in which the individual arrives at a diagnosis and prognosis session may affect clinical decisions (DiClemente & Velasquez, 2002), but the precise timing within a specific stage is considered immaterial, and daily fluctuations may be considered “noise.” Currently, scheduling the intake session before the start of treatment is a technical issue. A meeting is scheduled for the precise day and time when the individual seeking treatment is available and the intake specialist has an open slot. But if mental health is dynamic, the given point at which we measure it may have a decisive effect on the static picture of mental health that emerges.
What does it mean that mental health is a dynamic entity? In a sense, it means that even when an individual’s mental health does not change, it is not a state but rather has its own dynamics and fluctuations (Bringmann et al., 2022; Nelson et al., 2017; Wichers et al., 2015). To capture a dynamic pattern, multiple snapshots or continuous measurements are needed over time (Bringmann et al., 2022; Kalisch et al., 2019; Kuppens & Verduyn, 2017). When asked about their mental health before treatment, individuals may report their sense of the aggregated levels, or outstanding points in the dynamic unfolding of their experience, or be influenced by a primacy or recency effect (Murdock, 1962a, 1962b). Even if they succeed in reliably estimating their most frequent characteristic or its mean level, they fail to report on its dynamic patterns. Indeed, they are seldom asked about it. For example, when individuals are asked to rate their rage attacks, they may refer to mean levels of intensity, so that a person having an extreme attack once a month and one having minor attacks daily may report the same average score, although there is a world of difference between them. The same is true of suicidal ideation and other aspects of mental health (Ben-Zeev et al., 2012; Hallensleben et al., 2018). If we adopt a dynamic understanding of mental health, a new understanding of therapeutic change is required as well. It is no longer sufficient to calculate change only as the delta from one pretreatment snapshot to the next (in treatment or posttreatment); we must also complement such a delta by redefining therapeutic change as a change in the individual’s dynamic itself from a maladaptive dynamic to another, more adaptive one.
One of the most commonly used measures of depression, the nine-item Patient Health Questionnaire (PHQ9; Kroenke et al., 2001), may serve to demonstrate the difference between what is currently assessed and what is proposed here. The PHQ9 inquires about the frequency of depressive symptoms over a period of time. The questions are formulated as follows: “Over the last 2 weeks, how often have you been bothered by any of the following problems?” The options are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). Item 9, for example, includes “thoughts that you would be better off dead, or of hurting yourself.” However, the PHQ9 does not include an evaluation of the dynamic patterns of depression. For example, two patients may both rate Item 9 as 2 (more than half the days). Jack moves during those days, dynamically within hours and even minutes, from not having such thoughts at all to having them with great intensity, unable to think about anything else. Rachel, who also rated Item 9 as 2, shows a different pattern of having these thoughts nonstop, but more peripherally, being able to concentrate on many things while having these thoughts in the back of her mind. Clinicians may understand the depression of each of these two individuals differently and choose to work with them differently (Fig. 1).
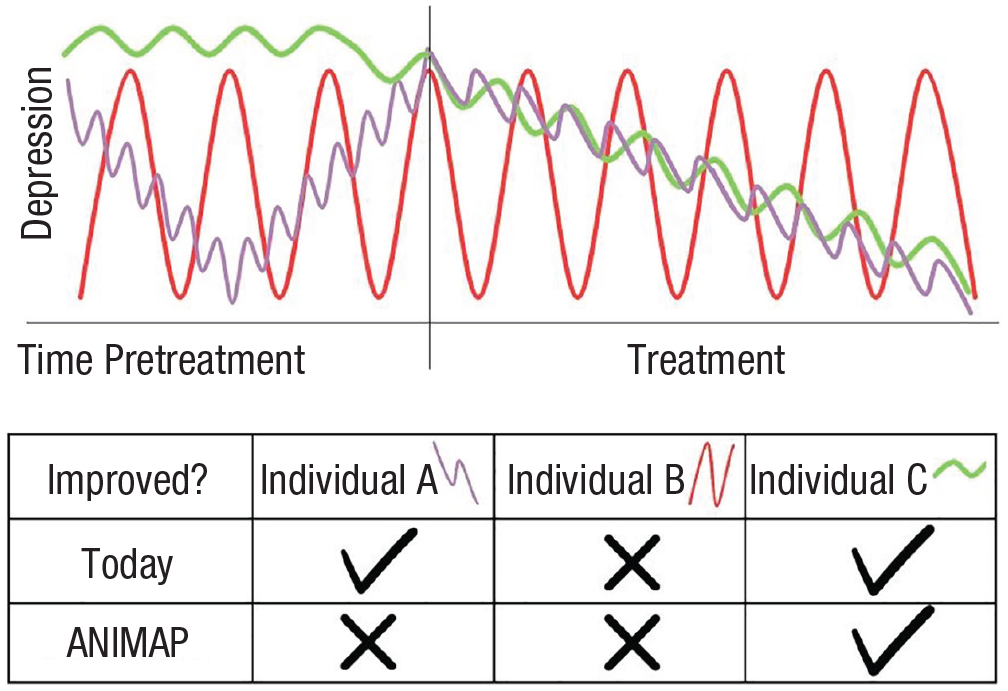
Illustration of how different dynamics may result in an inaccurate evaluation of change during treatment. Although the three individuals may show the same levels of depression pretreatment (depending on when exactly the pretreatment “snapshot” is taken) as well as the same delta of change from pre- to posttreatment (again, depending on when exactly the pre- and posttreatment snapshots are taken), their dynamics patterns are meaningfully different. ANIMAP = individual-specific animated profile.
The potential unique utility of the dynamic fluctuations of levels of depression can be demonstrated using a recent study in which we (Berko et al., 2022) collected patient reports on the levels of their general tendencies to experience depressive symptoms and their daily reports on the experience of symptoms for the past 24 hr over 28 days on a digital image-based assessment of the Hamilton Rating Scale for Depression (Berko et al., 2022). Although a once-a-day report may fail to capture within-day dynamic patterns and restrict the ability to observe complex dynamic patterns, the findings were still able to capture meaningful within-individual fluctuations. A high correlation was found between the general tendency to experience depression and the monthly average of daily scores, supporting a relatively high stability in depression (r = .82, p < .001). Together with the relatively high stability, there were also meaningful fluctuations around this stable level. Specifically, the average intraclass correlation coefficient was .57. This suggests that, on average, 57% of the variance in the daily manifestation of MDD symptoms can be attributed to individual differences, whereas the remaining 43% can be attributed to daily fluctuations. These fluctuations seem to be a meaningful characteristic of the individual rather than random noise. Not only were the levels of symptoms found to be stable over weeks, but the levels of fluctuations also displayed moderate stability rates from one week to the next. This suggested that the observed individual differences in mean levels of MDD symptoms and levels of fluctuations present different stable and meaningful patterns of symptomatology of the individual at baseline.
In addition to the finding that the fluctuations were a trait-like characteristic of the individual rather than random noise, further analysis (see the Supplemental Material available online) supports their utility in predicting treatment outcome. Both the general levels and dynamic-fluctuations components, as measured pretreatment, and even their interaction, were found to be useful in predicting subsequent treatment outcome, as evaluated weekly by trained diagnosticians from the first week of treatment to its end (Week 16). The clinical meaning of the interactions may also differ from one symptom to the next. For example, as can be seen in Figures S1 and S2 in the Supplemental Material, for depressed mood, individuals showing higher levels of depressed mood pretreatment show greater reduction in symptoms over the course of treatment if they showed greater pretreatment dynamic fluctuations in depressed mood. By contrast, for feelings of guilt, individuals showing lower levels of feeling guilt pretreatment show greater reduction in symptoms over the course of treatment as rated by a diagnostician if they showed lower pretreatment dynamic fluctuations in feeling guilt. The importance of both the levels and the dynamic fluctuations in symptoms have been further demonstrated by research suggesting that both contribute uniquely to predicting health and life outcomes (A. J. Wright & Jackson, 2023b). This is not to argue that existing measures of symptomatic levels should be abandoned. Rather, they should be complemented by additional information, shedding light on pretreatment dynamics.
The focus on pretreatment within-individual processes is critical. People are often confronted with changing circumstances to which they must adapt. From an evolutionary perspective, within-individual variation (adaptive phenotypic plasticity; Nettle, 2006) provides a selective advantage, such that adaptive traits are context-dependent (Kuzawa & Bragg, 2012). Within-individual variation, manifested as trait-like dynamics, is critical for meeting the shifting demands of the environment (Block & Kremen, 1996; Kashdan & Rottenberg, 2010) and adapting to environmental challenges (Kuzawa & Bragg, 2012).
A dynamic understanding of mental health perceives temporal fluctuations in it as an important intrinsic trait of each individual. The term “trait” does not refer to permanent traits but rather to a trait-like characteristic that may change to become more or less adaptive, either during treatment or in the course of other meaningful life-changing experiences. Indeed, findings suggest that interventions may incorporate a change in what has previously been considered permanent traits (e.g., Allemand & Flückiger, 2022; Bleidorn et al., 2022; Olaru et al., 2023; A. J. Wright & Jackson, 2023a, 2023b). Given its potential dynamic patterns, mental health, before treatment as well, needs to be assessed over time, addressing its dynamic features and variability. Research in psychopathology (A. J. Fisher et al., 2018; Hamaker et al., 2017; A. G. C. Wright & Woods, 2020) and psychotherapy (A. Fisher et al., 2019; Zilcha-Mano, 2019, 2021; Zilcha-Mano & Webb, 2023) has suggested that it is not possible to infer from between-individuals differences to within-individual processes (Curran & Bauer, 2011; Molenaar, 2004). For example, cognitive reactivity, the tendency to have negative thoughts in response to negative emotional states, was associated with depressive symptoms only at the within-individual level and not in the between-individuals level (Cole et al., 2021). Yet most psychotherapy research focuses on static differences between individuals’ pretreatment mental health.
The exceptional studies that explored the unique contribution of a dynamic understanding of mental health before the start of treatment or early in treatment to the process and outcome of treatment yielded promising results. For example, using a multiple baseline design in a single-case series study, Holmes et al. (2016) suggested that it was possible to model daily mood instability across 28 days pre- and posttreatment in individuals with bipolar disorder. Likewise, Höller et al. (2022) showed that network connectivity increased and the associations between symptoms and their centrality changed during the course of therapy. Another study was based on 10 individuals diagnosed with generalized anxiety disorder completing once-a-day reports on their symptoms over 60 days (A. J. Fisher, 2015). The collected symptomatic data were subjected to person-specific exploratory and confirmatory factor analysis and then used to formulate targeted interventions. Promising findings were also reported by Lutz et al. (2018), who showed that centrality measures derived from individual dynamic networks added value to predicting patient dropout. These studies demonstrate the potential contribution of a dynamic understanding of mental health to psychotherapy, although they have been limited mainly to symptoms, and these approaches are yet to be implemented to understand the potential dynamics of mechanisms of change pretreatment.
The Second Pillar of the Proposed Understanding of Mental Health: Mental Health Is Multidimensional
According to the dynamic multidimensional understanding of mental health, mental health is inherently a multidimensional entity. To form a comprehensive dynamic configuration of an individual’s mental health, its characteristics need to be assessed along several dimensions over time. For example, depression can be conceptualized as the clinical expression of dysfunction in cognition, behavior, affect, and so on. This view is consistent with the U.S. National Institute of Mental Health’s Research Domain Criteria initiative, which calls for integrating many units of analysis to investigate mental-health disorders and achieve a better understanding of their etiology and treatment (Cuthbert & Insel, 2013).
The utility of the multimodal approach has yet to be systematically explored to determine whether it adds more clarity or noninformative complexity. Focusing as an example on one of the research areas receiving most of the empirical attention recently, the patient–therapist synchrony during psychotherapy sessions (Zilcha-Mano, 2024), the different modalities seem to reveal both shared and different information and are not highly correlated at the sample level (e.g., Altmann et al., 2021; Schoenherr et al., 2021). Rather, they happen to interact, so that one modality may serve as the context in which synchrony in another modality is associated with the process and outcome of treatment (e.g., Bar-Kalifa et al., 2023; Kykyri et al., 2019; Tal et al., 2022). Each modality is processed in different areas of the brain, and multimodal integration requires communication between different areas in the brain, within the individual and between the individuals interacting with each other. Thus, the different modalities may reveal distinct, potentially complementary pieces of information (Palumbo et al., 2017; Suveg et al., 2016).
The distinct modalities cannot be simply combined to create an understanding of mental health without a coherent underlying theory, lest mental health is reduced to its psychological elements or its biological phenomena (Miller, 2010; Schwartz et al., 2016), or alternatively, mixing not only apples and oranges but even turnips and raspberries. The question of how dynamic patterns across distinct dimensions can be integrated effectively is a conceptual one that crosses the boundaries of scientific disciplines. A systematic doctrine is needed for integrating the psychological, physiological, hormonal, acoustic, and motional manifestations of mental health. One possibility is that the dimensions are manifestations of an underlying intrinsic dynamic that binds them together.
If such a multidimensional understanding of mental health is correct, even if in a given case we happen to be interested in only one dimension, say, the hormonal, we still need to take into account the multidimensional nature of mental health and assess other dimensions as well. This is because to capture the dynamic of any given dimension, we must disentangle its dynamic pattern (the signal) from measurement error (the noise), which can be done only with reference to another measured dimension that serves as an index. Examples of this can be found in many fields of science. For example, in marine research, animal tracking is combined with bathymetric, meteorological, sea-surface-temperature, and animal-habitat data to understand habitat utilization and animal behavior in response to external forces. These data sets all have different characteristics (e.g., spatial grid, sampling rate), so a simple combination would make analysis impossible and confound the results. By using strategies that take into account the dynamic of each dimension and the way they are integrated, all data and attributes can be brought together under a single view for a comprehensive understanding of the environment, enabling researchers to form new insights about the interactions between the environment and animal behaviors (Wilmers et al., 2015).
Likewise, to capture a true dynamic of mental health, we cannot restrict our measurement to only one dimension, which includes both signal and noise (e.g., measurement noise). For example, air conditioning may introduce noise into the acoustic measurement (Rochman & Amir, 2013) but not into movement measurement. When searching for individual-specific dynamics, another source of “noise” is caused by between-individuals dimension-specific dynamics, such as the diurnal cycle in cortisol. Therefore, assessment requires the systematic integration over time of separate dimensions that together act to wash out noise and strengthen the signal. Because each dimension sheds light on a portion of the dynamics, it differentiates dimension-specific noise from the individual-specific intrinsic dynamics of interest. This minimizes the risk of mistaking noise for signal, exaggerating trivial effects, and overlooking true effects.
According to the proposed understanding of mental health, the dimensions of mental health affect and interact with each other, resulting in an integrated matrix of mutual relations that can be studied effectively only as a whole. Examples of such a matrix from a different field of science are models predicting snakebites in high-risk landscapes (Goldstein et al., 2021) that integrate parameters of time and space, differentiating, for example, between land-cover types of rice, tea, and rubber; climatic factors such as amounts of precipitation and humidity; habitat types; and more. Time of day and month of the year are additional factors taken into account. The predictive model emerges only by integrating the dynamically changing data pertaining to the various dimensions. Likewise, to create a model that predicts individual-specific mental-health dynamics, we need to integrate data measured across time of the many dimensions of mental health.
The process has some similarities with weather forecasting, in which thousands of measurements over time are reduced to produce an hour-by-hour forecast of temperature, wind, and humidity for the next few days. Likewise, using recently developed computational methods adapted to psychotherapy (for one potential example, see the Supplemental Material), it is possible to distill the thousands of hormonal measurements, acoustic measurements, motional measurements, and so on into individual-specific profiles that describe the individuals’ mental health. It will then be possible to investigate how treatment could target these individual-specific profiles to make them more adaptive.
The dynamic individual-specific profiles of mental health are expected to provide a more accurate description of that individual’s mental health than random snapshots of one dimension or another or the mean values of snapshots of individual dimensions acquired over time. These dimensions are interrelated and are expected to represent manifestations of one intrinsic dynamic as opposed to a collection of disparate, unrelated entities.
Table 1 shows a preliminary set of candidate dimensions chosen on the basis of research attesting to their role in MDD and its treatment. The implementation of this set of dimensions in psychotherapy research both poses challenges and offers advantages. Some of the challenges include the requirement to use wearable devices that carry a financial cost and require some additional engagement (e.g., battery charging), even though technological solutions, based on widely used devices (e.g., smartphones), are being developed at a fast rate (e.g., smartphones capturing mood dynamics on the basis of social communication, electronically activated recordings capturing “acoustic diaries”; Kaplan et al., 2020; Li et al., 2023; Mehl, 2017). There are also clear advantages in these automatically measured dimensions when the aim is to explore dynamic patterns of mental health, especially given that abundant data from the same individual (e.g., 200 time points or more) are needed to capture change (see Bringmann et al., 2018; Cabrieto et al., 2018a, 2018b). Passive rather than active data collection is characterized by the lowest burden possible for intensive, ecological moment-to-moment data collection over long periods of time, when individuals naturally engage with their real environments. Thus, it has the potential to complement active data collection, such as ecological momentary assessment, which is limited in the time points, number of items, and time intervals that can be used without increasing the burden on patients (Hayes & Andrews, 2020). The limitations in the need to rely on the patient’s cooperation are especially notable in mental-health disorders, such as MDD (Smith, 2013; Treadway et al., 2012).
Preliminary List of Candidate Dimensions of MDD Chosen Based on Their Role in MDD Psychopathology and Its Treatment
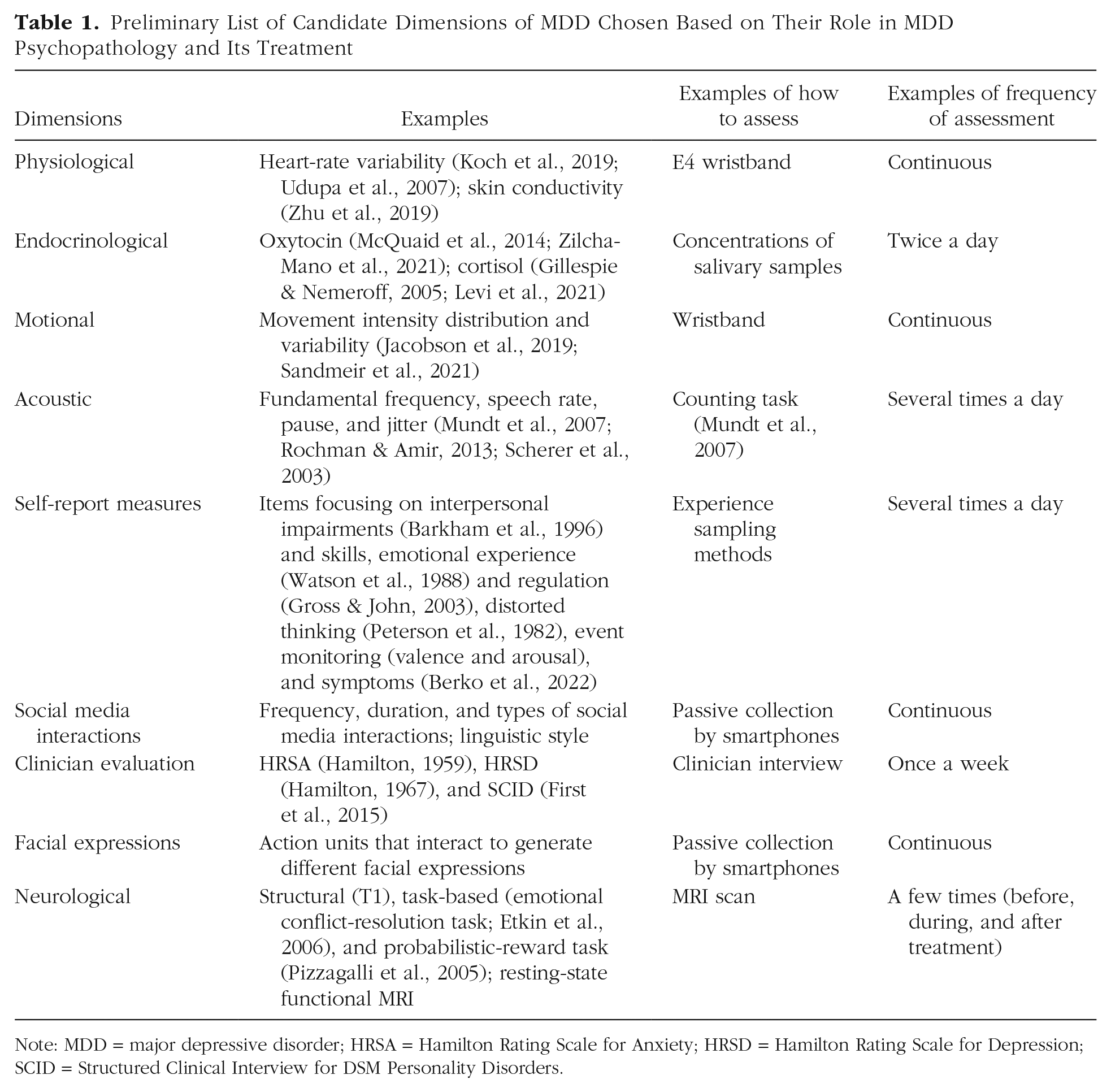
Note: MDD = major depressive disorder; HRSA = Hamilton Rating Scale for Anxiety; HRSD = Hamilton Rating Scale for Depression; SCID = Structured Clinical Interview for DSM Personality Disorders.
Although the utility of interdisciplinary measures has not been fully validated, its promising potential is starting to be revealed (Zilcha-Mano, 2024; Zilcha-Mano & Ramseyer, 2020). For example, research stresses the importance of baseline observations of hormones (Zilcha-Mano et al., 2020, 2023), acoustic characteristics (Nof et al., 2021), neuroimaging (Drysdale et al., 2017; Zilcha-Mano et al., 2019), and so on, in predicting the process of treatment. Research further demonstrates the importance of therapeutic changes and levels during treatment in hormones (H. Fisher et al., 2023; Levi et al., 2021; Zilcha-Mano et al., 2018, 2021), motion (Altmann et al., 2020; Deres-Cohen et al., 2021; K. Cohen et al., 2021; Ramseyer, 2020; Ramseyer & Tschacher, 2011, 2014; Shapira et al., 2022), acoustics (Bar-Sella et al., 2023; Bryan et al., 2018; Dolev-Amit et al., 2022), neuroimaging (Zilcha-Mano et al., 2022), and so on, in predicting the process of treatment. However, almost no study to date has explored the multidimensional dynamics of mental health before the start of treatment, when no therapeutic change is anticipated. Although each one of these dimensions receives at least minimal scientific attention, with some receiving more than others, little is known about how they integrate to form mental health, and even less is known (if anything) on the potential glue binding these dimensions together: the individual-specific intrinsic dynamic profiles.
The Individual-Specific Mental-Health Dynamics
Building on these two pillars, a valid portrayal of an individual’s mental health is dynamic and multidimensional, being able to better capture the complexity of human mental health than one unidimensional snapshot. Individuals have a trait-like intrinsic dynamic that represents their mental health. A comparison of the cross-dimension relations between dimension-specific dynamic patterns provides a more accurate description of the individual’s mental health than do random snapshots of this or that dimension or the mean values of snapshots of individual dimensions acquired over time (see Fig. 2). These dimensions are expected to form one complex dynamic whole, where they affect each other. In such individual-specific profiles, the whole is more revealing than the sum of its parts. For example, the extent to which the mental-health profile of the individual coherently reflects the same pattern of dynamics across dimensions is an important facet of mental health that cannot be evaluated when focusing on one or even two dimensions each time. To extract the individual-specific intrinsic dynamics of mental health, computational approaches are needed that can reach beyond measurement noise and between-individuals patterns that characterize each dimension (e.g., the between-individuals diurnal cycle for cortisol).
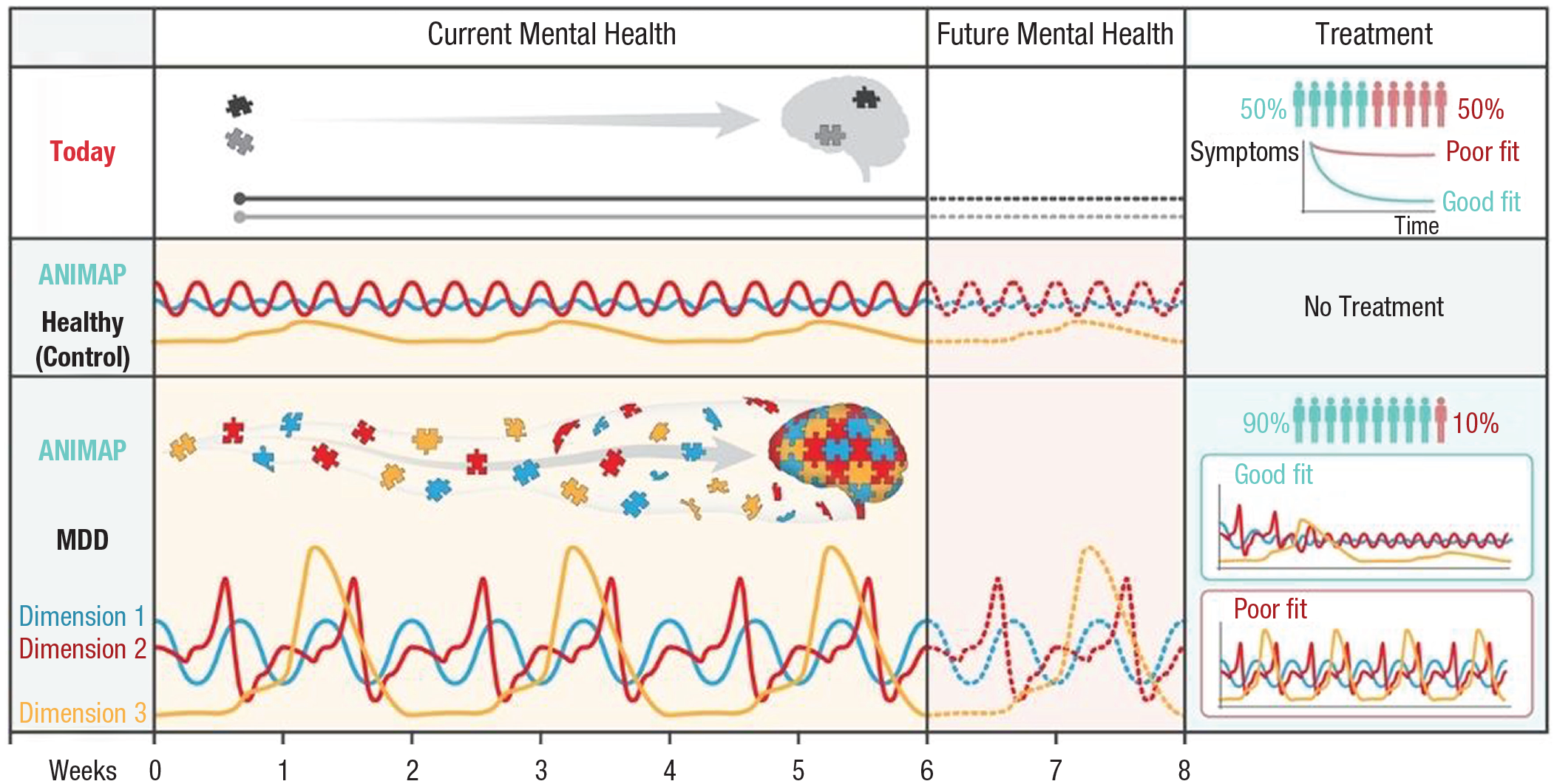
From a static unidimensional representation of mental health toward a dynamic multidimensional understanding of mental health. Mental health is captured over time and used to draw predictions about the future, and with the use of mental-health evaluations, the optimal treatment for the individual is identified. ANIMAP = individual-specific animated profile; MDD = major depressive disorder.
What Types of Individual-Specific Dynamics of Mental Health Can We Expect?
It may be too early to propose a closed list of the types of dynamics of mental health displayed by different individuals before further empirical data will be gathered. But it is possible to formulate several critical hypotheses on the basis of theory and research in related disciplines. It can be suggested that individuals differ in the extent to which their mental health is dynamic as well as the extent to which the various dimensions are mutually coherent. At least three parameters may be suggested to account for individual differences in the individual-specific profiles: level of reactivity, type of stimulus, and level of coherence between dimensions.
The level of reactivity reflects the extent of fluctuations in mental health over time. These fluctuations can be explained at least in part by the level of activation the individual shows in response to stimuli. The type of ecological stimulus may be internal or external (e.g., Kuppens et al., 2010). For example, interpersonal interactions are external stimuli, whereas repetitive thoughts of worthlessness or preoccupation with concerns about the future are internal. Some individuals may deactivate their responses to these stimuli, seeking to “shut down” in response to them, whereas others may respond by hyperactivation of the system, seeking to “raise alarms.”
Such individual differences may correspond with other personality and interpersonal theories, such as attachment theory, according to which although any individual has an inborn attachment system, individual differences exist in the pattern of activation of the system. Such individual differences in the level of activation are theorized to be a product of genetic factors (Gillath et al., 2008) and experiences with attachment figures, especially early in life (Bowlby, 1982). As a result of distinct developmental trajectories (Cassidy & Berlin, 1994), some individuals show hyperactivation of the attachment system, as manifested by energetic attempts to attain greater proximity, support, and love, combined with a lack of confidence that it will be provided. Others show deactivation of the attachment system, as manifested by inhibition of proximity-seeking tendencies, denial of attachment needs, maintenance of emotional and cognitive distance from others, and compulsive reliance on oneself as the only source of protection. Such individual differences, ranging from deactivation to hyperactivation, can be found across behavioral systems (Mikulincer & Shaver, 2010). Differences in individual-specific profiles of mental health may also show some consistency with approach and avoidance theories of behavior (Corr, 2013; Lewin, 1935).
Despite individual differences (Okur Güney et al., 2022), all individuals are expected to show some level of coherence between the dimensions, such that their dynamic in one dimension is expected to be indicative of their dynamic in another. Yet the level to which the dimensions show coherence may differ between individuals. Some individuals may show greater similarity between the levels of activation across dimensions than other individuals who may display a disorganized pattern that incorporates both hyperactivation and deactivation dynamics. Condon and Ogston (1966) made the distinction between what they defined as “harmony between speech and body motion” and what they called “dyssynchronous patterns.” New technological and methodological developments make it more feasible than ever before to quantify coherence across modalities and over time, not only linearly but also to capture more complex nonlinear associations. Together, these three parameters, potentially alongside additional ones, create a matrix of individual differences between people. It is too early to propose a definite model of how distinct profiles of MDD may emerge on the basis of these parameters, but it can be expected that coherent profiles characterized by uniform hyperactivation or deactivation and incoherent ones characterized by inconsistent patterns of activation may be among the main profiles that characterize MDD. A coherent profile of regular activation may characterize healthier individuals with more adaptive profiles.
Expected Outcomes of a Dynamic Multidimensional Understanding of Mental Health
A dynamic multidimensional understanding of mental health raises several new questions, such as (a) which multidimensional dynamic profiles define mental health disabilities, (b) whether different mental-health disorders are represented by different profiles (e.g., MDD vs. generalized anxiety disorder), (c) whether it is possible to develop new treatments that are specific for bringing therapeutic change in dynamics that are characterized by hyper- versus deactivation, (d) whether neurofeedback (Fernández-Álvarez et al., 2022) can help bring individuals from noncoherent dynamics across dimensions to coherent ones, and (e) whether an individual-specific profile changing into a more adaptive one can be assessed.
Building on a dynamic multidimensional understanding of mental health, several directions for future theoretical developments and empirical research can be delineated:
A dynamic multidimensional understanding of psychopathology
A dynamic multidimensional understanding of mental health may shape our understanding of psychopathology as a complex of dynamic entities rather than fixed phenomena. If the proposed dynamic multidimensional understanding of psychopathology receives empirical support, instead of defining an individual as being depressed, we will describe a dynamic characteristic of that individual. A valid remote and ecological evaluation of mental health is even more critical in an age of increased reliance on remote treatment (Békés et al., 2023; Swartz, 2021).
Promising demonstrations of the utility of such direction already exist (Edershile & Wright, 2021; Roefs et al., 2022; Webb et al., 2022). Most of these studies are based on network analyses and dynamic-systems approaches to mental health. Although mainly focusing on symptoms as rated by the individuals, studies suggest differences between individuals with MDD and healthy controls in the density of their network of negative affect (Pe et al., 2015), as well as within-individual changes pointing to early warning signals of depression (e.g., Wichers et al., 2016), or as a result of other change facilitators, such as COVID-19 (M. W. Fried et al., 2021). Like the proposed conceptualizations 1 from a dynamic-systems perspective, the trait-like dynamic patterns may be understood as having some properties similar to those of attractor states, whereas changes in the dynamic patterns can be understood as destabilizing the pathological attractor and developing new, more healthy patterns of functioning, switching from a pathological to a healthier attractor, or making minor adjustments to maladaptive patterns (Hayes & Andrews, 2020). From a network-analysis perspective, causal interactions between symptoms in the network (Borsboom & Cramer, 2013) may have some commonalities with the trait-like dynamic patterns proposed here. A within-individual repeated network analysis may provide an intuitive story of individuals with mental-health problems (Bringmann et al., 2022). A change in the network may take different forms. For example, it has been suggested that identifying the most central nodes (symptoms) in the network may be instrumental in guiding the search for intervention targets, although there are many different centrality measures, and even the mere idea that centrality measures could suggest promising intervention targets is debatable (Bringmann et al., 2019; Dablander & Hinne, 2019; Hallquist et al., 2021).
Even when focusing only on patient-rated symptoms (rather than psychotherapy-based mechanisms of change), still little is known about their contribution to enhancing treatment efficacy. This is so partly because of potential modeling challenges (e.g., nonstationarity) and partly because of a need for clear theoretical conceptualizations that can guide the building and application of parsimonious and targeted modeling strategies (Bringmann et al., 2022). For example, Bringmann et al. (2022) stressed the need to answer questions such as which specific edges or node centralities provide optimal target points for interventions. It has been proposed that current network-approach applications to clinical practice are mainly exploratory (data-driven) and that there is a need for devising confirmation and falsification approaches on the basis of conceptual models (Bringmann et al., 2023). Different methodological solutions may represent various understandings of mental health and thus may yield distinct patterns of results (Bastiaansen et al., 2020). Given the extensive research on mechanisms of change during treatment (Crits-Christoph & Gibbons, 2021), and the little that is known about their development before the start of treatment, it can be suggested that the underlying implicit assumption is that assessing mechanisms of change before treatment is not relevant because they are not conceptualized as changing outside of treatment. When mechanisms of change are measured before treatment, they are designed mainly to measure their stable baseline level rather than their dynamics. Measuring insight is a good example. Insight is measured mainly before the start of treatment only once because as a mechanism of change insight is not conceptualized as changing before treatment started (Jennissen et al., 2018). Thus, almost nothing is known about dynamic patterns of mechanisms of change before the start of treatment as potential representations of mental health.
A dynamic multidimensional understanding of therapeutic change
Psychotherapy research is increasingly interested in in-treatment between sessions, fluctuations and dynamic patterns in symptoms (e.g., Lutz, Schwartz, & Delgadillo, 2022), and mechanisms of change (e.g., Zilcha-Mano & Fisher, 2022). Yet we know little about the dynamics that characterize the individual before the start of treatment and therefore are limited in our evaluation of change. A dynamic multidimensional understanding of mental health may require transforming our understanding of therapeutic change from a delta in symptoms to a shift from one multidimensional dynamic to a new, more adaptive one. Much of what we know today about the efficacy of psychotherapy may be based on a biased measure of change because it treats mental health as a fixed entity. To adequately estimate the efficacy of treatment, a new framework for evaluating the extent to which individuals benefit from treatment may need to be established to complement the existing knowledge.
A dynamic multidimensional understanding of mental health may contribute to increasing the treatment success of “stubborn” mental-health conditions
A dynamic multidimensional understanding of mental health may enable a better match between individuals and their optimal treatments, resulting in increased efficacy and effectiveness. The field of psychotherapy research will be better able to predict differential effects of treatments and assign individuals to the treatment most effective for them on the basis of the full range of their mental-health dynamics.
Some of the most effective approaches to improving treatment efficacy today could be integrated into the proposed conceptualization to achieve further gains. Some of the noted approaches are routine outcome monitoring (ROM) and systematic matching of patients with their optimal treatments and therapists. ROM refers to the process of implementing measures (mainly patient-reported outcome measures) for routine data collection from patients, generally session by session, feeding back the data to the therapist, and when needed, tailoring the treatment to improve outcome in light of the feedback (Barkham et al., 2023; Pinner & Kivlighan, 2018). A meta-analysis by de Jong et al. (2021) supports the benefits of using feedback systems, suggesting that they improve symptom reduction and reduce dropout by 20%. In recent years, ROM has further developed through the use of advanced algorithms to determine when a patient is not on track and offer treatment decision-making tools, for example, the Trier Treatment Navigator (Lutz, Deisenhofer, et al., 2022). Together with its great potential, some of the main limitations of ROM are that it is seen as too narrowly focused and not suitable for patients presenting with multiple problems. These concerns predict poorer uptake of standardized ROM measures (Rye et al., 2019). Inspired by current applications of ROM, it can be cautiously suggested that the patient’s dynamic profile, as well as adaptive and maladaptive deviations from it, may also be used as a potential source of feedback to complement existing feedback approaches. Because these profiles are based on automatic rather than on patients’ self-report measures, they may also be used to alert the therapists within sessions and provide real-time warning signals during the session rather than only between sessions.
Additional effective approaches that can be integrated into the proposed conceptualization are the matching of patients with treatments and treatment providers. Studies have implemented advanced data-analysis approaches to identify the most effective treatments (Delgadillo et al., 2022) and therapeutic techniques (Webb et al., 2022) for a given individual on the basis of the individual’s pretreatment characteristics (DeRubeis, 2019). On the basis of these studies, it can be suggested that the patients’ pretreatment dynamic profiles could be used to identify the most effective treatment for individuals. Likewise, advanced data-driven methods have been shown to be effective in prospectively matching therapists’ strengths (on the basis of their previous performance and track records) with patients’ specific mental-health problems (Constantino et al., 2021a). It can be cautiously suggested that some of the observed variability between therapists in their efficacy (Wampold & Owen, 2021) can be explained by their ability to intuitively identify individuals’ mental-health dynamics and tailor the treatment to their needs and characteristics. Inspired by Constantino et al. (2021a), a complementary application matches patients with therapists better capable of working with patients who have a certain dynamic profile or matches patients with therapists on the basis of the latter’s profiles.
A dynamic multidimensional understanding of mental health may contribute to the emergence of a field of computational psychotherapy specializing in the analysis of the many types of data collected across dimensions and time
Computational psychotherapy is a new approach that to date has been used only sporadically to assess particular aspects of therapy, such as the linguistic one (Imel et al., 2015). Formulating and investigating the validity of a comprehensive mental-health theory using the abilities of computational psychotherapy is important for exploring the dynamics of mental health.
The Next Step Forward: How Can the Proposed Understanding of Mental Health Serve Treatment Personalization? Integrating Theory-Driven Conceptualization With Data-Driven Methodology
We know very little about the dynamic and multidimensional characteristics of an individual’s mental health before the start of treatment. Therefore, at this point, it is important to integrate theory-driven (top-down) conceptualizations with a data-driven (bottom-up) methodological framework. The theory-driven ingredients are the hypotheses that mental health is a dynamic entity as manifested in interrelated dimensions and that a dynamic representation of mental health will be more accurate than a static one and will outperform and complement a static representation in predicting future mental health and in matching individuals to their optimal treatments. As part of the theory-driven approach, it can also be anticipated that at least some of the critical parameters that will differentiate between individuals in their dynamics are level of activation (hyper- vs. deactivation) in the face of stimuli (internal vs. external) and level of coherence (high vs. low) between dimensions. The proposed theoretical assumptions are yet to be empirically tested. For example, it may be that lower rather than higher levels of coherence indicate better mental health. A low level of coherence may indicate an individual’s ability to integrate and adapt to a variety of internal and external demands and respond flexibly to adverse changes (Bakhchina et al., 2018). Indeed, a greater level of complexity was found to be associated with a variety of adaptive functioning and better health outcomes (Lanata et al., 2015; Rajendra Acharya et al., 2006; Stange et al., 2023), including better affect regulation (Stange, Hamilton, Fresco & Alloy, 2017) and a better course of depression (Panaite et al., 2016; Stange, Hamilton, Olino, et al., 2017).
The extent to which the emerging dynamic multidimensional understanding of mental health will correspond to existing theoretical constructs in psychotherapy is open to exploration. It is first imperative that future research shed light on critical ingredients of the individual’s pretreatment mental health that have received little systematic research so far. This new knowledge will enable the integration of theory- and data-driven approaches. After individual-specific profiles are identified, it will be possible to explore their connections with theories of psychotherapy research. For example, findings may reveal that some individual-specific profiles reflect maladaptive affect experiencing and regulation strategies characterized by coherent hyperactivation in response to both external and internal stimuli across dimensions (e.g., self-report, acoustic, cortisol). For these individuals, a latent variable of affect may emerge in their individual-specific profiles that will be the variable most closely associated with severe symptoms and the one that precedes other dynamics, similarly associated with severe symptoms. For example, feelings of shame, as manifested in high and stable levels of jitter, low levels of F0 with high variability (specific levels of pitch), increased heart rate, and low stable levels of movement, will precede an increase in behaviors of social isolation. The feelings of shame are expected to result in more severe symptoms of depression, both directly and indirectly, through their effect on social isolation. For those individuals, a combination of data-driven models (the creation of the individual-specific profile; e.g., Ernst et al., 2021) and theory-driven ones (theories of the role of affect in psychopathology and how it can be used as a mechanism of change in treatment) may lead to the conclusion that they could benefit most from treatments targeting maladaptive emotional tendencies as the main mechanism of therapeutic change (e.g., emotion-focused treatment). This conclusion is facilitated by the individual-specific profiles because the maladaptive dynamic pattern of affect, as it manifests across dimensions, could have been lost if instead of the dynamics we were to focus on a snapshot, or even on the mean level of a single dimension, which may not even be related to symptom severity. The maladaptive dynamic pattern is a critical characteristic, and it may manifest only across dimensions.
The individual-specific profiles of other patients may be characterized mainly by coherent hyperactivation across dimensions to the external stimuli of interactions with others. Therefore, a latent variable of maladaptive interpersonal patterns may emerge as the one most closely associated with severe symptoms and precede other dynamics that are also associated with severe symptoms. For example, maladaptive interactions with others may precede increased feelings of worthlessness. For these individuals, a combination of data-driven models (the creation of the individual-specific profile) and theory-driven ones (theories concerning the role of maladaptive interpersonal patterns and schemas in psychopathology and how their modification can serve as a mechanism of change in treatment) may lead to the conclusion that these individuals could benefit most from treatments targeting maladaptive interpersonal patterns as the main mechanism of therapeutic change (e.g., interpersonal therapy, supportive-expressive treatment).
In the future, individuals with a history of mental-health disorders may develop, together with their treatment providers, a good understanding of their adaptive and maladaptive individual-specific profiles (e.g., when they are in their best and worst mental-health conditions). Identifying the individual-specific profile will enable determining whether and when preventive interventions should be implemented in a scalable way before a full treatment is needed. When a treatment is needed, the understanding of the individual-specific profile will make it easier for patients to know their personalized goals for a successful treatment (their healthy individual-specific profile), to be implemented along with their preferences. Agreement between patient and therapist on such an understanding will strengthen the therapeutic relationship between them because agreement on the goals of treatment is one of the three components determining the strength of the therapeutic relationship (Bordin, 1979). They will also have a good understanding of which strategies—treatment-related (therapeutic techniques used in the session or homework assignments) or not directly related to treatment (e.g., exercise, spending time with significant others)—contributed to the change from one individual-specific profile to another. This understanding will provide a clear personalized program of treatment and strengthen the alliance, given that the second component of the alliance is the agreement between the patient and the therapist on the tasks needed to achieve the goals of treatment (Bordin, 1979).
Supplemental Material
sj-docx-1-pps-10.1177_17456916231226308 – Supplemental material for Individual-Specific Animated Profiles of Mental Health
Supplemental material, sj-docx-1-pps-10.1177_17456916231226308 for Individual-Specific Animated Profiles of Mental Health by Sigal Zilcha-Mano in Perspectives on Psychological Science
Footnotes
Acknowledgements
I would like to thank Laura Bringmann for her insightful feedback on the manuscript. The writing of this paper was supported by the European Research Council (ERC) under the European Union’s Horizon Research and Innovation Programme (grant agreement no.101123661 SynSig) and by two grants from the Israeli Science Foundation (Grant 186/15; 395/19).
Transparency
Action Editor: Joanne Davila
Editor: Interim Editorial Panel
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.