
Abstract
The interpersonal distance (IPD) theory provides a novel approach to studying autism spectrum disorder (ASD). In this article, we present recent findings on the neurobiological underpinnings of IPD regulation that are distinct in individuals with ASD. We also discuss the potential influence of environmental factors on IPD. We suggest that different IPD regulation may have implications for cognitive performance in experimental and diagnostic settings, may influence the effectiveness of training and therapy, and may play a role in the typical forms of social communication and leisure activities chosen by autistic individuals. We argue that reconsidering the results of ASD research through the lens of IPD would lead to a different interpretation of previous findings. Finally, we propose a methodological approach to study this phenomenon systematically.
Imagine a situation in which people are together in an elevator. They avoid eye contact, and their movement is stiff and constrained; most of them either travel in silence or start a conversation about a superficial topic. If experts in autism diagnostics were to observe our imaginary passengers, they would notice behavioral traits that could be reminiscent of autism spectrum disorder (ASD). However, if the same group of neurotypical people were to interact in an office break room or at a cocktail party (with enough space to stand at a comfortable distance or move away if necessary), they probably would have a good time making small talk, sharing stories while gesticulating vigorously, expressing clear emotions, and making prolonged eye contact. It is unlikely that the observed individuals suddenly lost their social-communication competence in the elevator. Although many other elements of cultural norms influence whether we initiate a conversation in certain situations (e.g., people’s lack of prior acquaintance or reason to interact), which cannot be completely ruled out as explanations for this phenomenon, the preceding examples highlight the impact of interpersonal distance (IPD) on social and cognitive functioning. We believe that IPD is a simple but crucial element of social interactions in real-life situations that influences how effectively we can use our skills and strengths. The extent to which this effect is observed and the preferred size of IPD varies between individuals, and we believe that people with ASD are more affected than neurotypical people; however, a systematic examination is needed to explore the role of IPD in social interactions and how this affects people with ASD compared with neurotypical people.
Neurobiology and Neurodevelopment of Distance Regulation
IPD is modulated by many external and internal factors, and its regulation can be altered or impaired in several conditions (Candini et al., 2021; Kennedy et al., 2009). Functional brain-imaging studies revealed a different pattern of brain activity and connectivity in ASD and neurotypical individuals when measuring IPD (Massaccesi et al., 2021; Perry et al., 2015). In neurotypical people, activation of the dorsal intraparietal sulcus (DIPS), prefrontal and orbitofrontal cortices, ventral premotor and somatosensory cortices, and amygdala may play a role in IPD regulation during computerized versions of the stop-distance paradigm (in which participants are instructed to stop or tell the experimenter to stop at a preferred distance) and comfortable IPD task (in which participants are instructed to indicate the most comfortable distance as someone approaches them from the perimeter of a circle; Huang & Izumi, 2021). In addition to neural activity, functional connectivity was measured. In certain studies primarily involving neurotypical participants, significant connectivity was found during IPD tasks among the DIPS, the ventral premotor cortex, the dorsal striatum, and—in the case of social stimuli—the midbrain, the premotor cortex, and the right dorsolateral prefrontal cortex (Holt et al., 2014). In participants with ASD, Massaccesi et al. (2021) found not only reduced activity in parietal and visual regions in parallel with observed elevated discomfort in an interpersonal space task but also the dysregulation of effective connectivity between the amygdala and the DIPS and the fusiform face area (FFA). The authors argue that the dysregulation of this network might prevent information integration. The amygdala is important in signaling the motivational relevance of spatial information, and in integration with the spatial attention network, forming a salience map directing attention (Egner et al., 2008). In people with ASD, the increased effective connectivity from the amygdala to the DIPS and FFA and the decreased connectivity from the DIPS to the amygdala were associated with higher discomfort that might reflect an elevated perceived saliency. Massaccesi et al. (2021) speculate that the differential effective functional connectivity emphasizes the varying relevance of spatial (where) and visual (what) information in people with ASD, who compensate for the perceived discomfort by keeping a greater IPD.
The amygdala is a complex subcortical structure, a hub of distinct neuronal networks. It contributes not just to emotional valence, salience, and reward processing, it also plays an important role in social learning and other cognitive functions by assigning attention and coordination of top-down and bottom-up processes (Hennessey et al., 2018, Janacsek et al., 2022). In addition to its above-mentioned functions, the amygdala is a crucial area in IPD, as it is involved in emotion and face processing, and it plays a role in avoidant behavior through the regulation of arousal, both of which are essential in social situations. It is difficult to map its specific dysfunction in people with ASD. We know, however, that the amygdala and its connections with other distinct brain areas develop throughout the life span, but its development is altered in people with ASD (Stanfield et al., 2008). Studies have shown amygdala enlargement in early childhood of people with ASD, which decreased or reversed in adolescence (Barnea-Goraly et al., 2014; Schumann et al., 2009). The change in size might be a consequence of the amount of social interactions, so it could be a potential biomarker of the effectiveness of therapeutic interventions (Hennessey et al., 2018; Zalla & Sperduti, 2013). Furthermore, neuroimaging studies have found increased amygdala activation during face-processing experiments (Tottenham et al., 2014) and reduced habituation of the amygdala in people with ASD (Kleinhans et al., 2009). The overresponsivity, hyperreactivity, and consequent hyperarousal might contribute to social avoidance and support the developmental model of hyperactivity-induced excitotoxic changes (Nacewicz et al., 2006). Decreased habituation to social stimuli can lead to difficulty discriminating salient stimuli, especially in social situations (Kleinhans et al., 2009).
Overall, altered activation of the amygdala and related functional networks in people with ASD might contribute to social dysfunction in two ways: (a) The functional connectivity differences can lead to higher discomfort at shorter IPDs, and (b) decreased habituation of the amygdala leads to the maintenance of hyperarousal and directs attention to social stimuli for longer than necessary. We argue that the effect of amygdala dysfunction on social cognition and behavior might be overwhelming for people with ASD and withdraw valuable resources from other cognitive processes during social interactions. If we measure the intellectual and cognitive performance of people with ASD while they are in person with the experimenter, there is a risk that we will get inaccurate, unreliable results.
Altered IPD Regulation as a Response to Adverse Environmental Stimuli
The phenomenon described above may be the result of atypical neurodevelopment, but we cannot rule out the possibility that environmental factors and early life experiences also have an impact on IPD regulation. Unfortunately, adverse childhood experiences or traumatic events are common in people with ASD (Kerns et al., 2015; Ng-Cordell et al., 2022). Because of difficulties in social communication, autistic children often become victims of bullying or abuse (Haruvi-Lamdan et al., 2018). Furthermore, because of sensory hypersensitivity, tactile or olfactory stimuli that are typical for other people may be unpleasant or uncomfortable for them (Wood et al., 2021). One possible coping strategy is disengaging with trauma, which can be manifested in social withdrawal, problem avoidance, self-protective behavior, emotional avoidance, learned helplessness, or wishful thinking (Ng-Cordell et al., 2022). These factors might lead to a greater preferred physical distance. However, engaging with traumatic events or maladaptive self-regulatory strategies such as emotional outbursts with aggressive behavior or sensory-seeking behavior (if touch or tactile stimuli are pleasant) might result in even closer but unwanted physical proximity. At the same time, aggressive behavior or undesirable physical contact could indirectly lead to feelings of rejection and isolation through avoiding other people in their environment. Distancing initiated by either the autistic person or the other person might lead to fewer positive interpersonal proximity experiences, which could hinder the acquisition of other social skills.
To have the appropriate attitude toward children with autism, we need to understand the origin of atypical IPD preferences. Mothers of autistic individuals often report that they had the impression that their autistic child was different, resistant, or even distant. In addition to this anecdotal evidence, a prospective study that assessed attachment style at an early age (15 months) found that infants with a high likelihood of ASD and insecure-resistant attachment were over 9 times more likely to be diagnosed later with ASD than those with a high likelihood but secure attachment (Martin et al., 2020). However, this result does not provide evidence as to whether atypical IPD was also present in autistic infants or whether it develops as a result of negative experiences. It is also possible that neurobiological and environmental factors are not independent but enhance each other’s adverse effects on IPD regulation, which would be in line with the concept of autism as a condition of generalized imbalance in adaptation (Gernert et al., 2020). To understand this relationship in more depth in terms of IPD, we need anamnestic information about traumatic experiences as well as longitudinal studies.
In this article, we highlight the importance of cross-sectional studies to measure (a) whether there is a disturbance in IPD regulation in autism and (b) how it affects performance in other areas, especially cognitive functioning. Because ASD is a highly diverse and heterogeneous condition, it is likely that individuals will be affected to different degrees. Some people with ASD may be perfectly comfortable with a closer personal distance, whereas others may prefer a greater distance. We argue that during the systematic cognitive and/or psychological assessment of autistic people, it is necessary to consider the IPD at which the study is conducted.
Results of Behavioral Measures of IPD in People With ASD
The underlying neural processes are challenging to study in ecologically valid settings at the moment. Neuroimaging and electrophysiological studies are capable of examining only the cognitive component but, unfortunately, cannot focus on the kinetic component of IPD regulation. Only a handful of studies measure the preferred IPD of people with autism in a real physical environment. Greater IPD (lower permeability of personal space) and/or altered flexibility of its regulation has been found in most of the studies (Candini et al., 2017, 2020; Farkas et al., 2023; Gessaroli et al., 2013; Kennedy & Adolphs, 2014; Perry et al., 2015). Only one study from Japan found that people with autism preferred less personal space than did neurotypical individuals (Asada et al., 2016), which raises the possibility of cultural effects on IPD regulation. In summary, not only do neuroimaging studies suggest altered neural activation in people with ASD, but also behavioral studies show that IPD preferences and/or IPD regulation are different in people with autism.
Cognitive Functions and Distancing in People With ASD
As the concept of autism has evolved over the past decades, so has the extent to which cognitive dysfunction (including executive functions) can be considered specific to it (Demetriou et al., 2019; Friedman & Sterling, 2019; Hill, 2004; Ozonoff et al., 1991, 2007; Ozonoff & McEvoy, 1994; Zhang et al., 2020). Accurate and reliable measurement of the cognitive profile of individuals with autism is critical to clinical diagnosis, treatments, and therapy as well as educational settings. However, the measurement may not be reliable and accurate without consideration of the distance between the investigator and the autistic individual. Previous studies have not reported these data, even though they might significantly affect cognitive performance. Weismer et al. (2018) found that deficits in executive functions (e.g., shifting, inhibition, working memory update) diminished after controlling for social communication characteristics; they assumed that difficulties in verbal communication and the verbal instructions might result in task impurity. Participants matching criteria are not uniform across studies (age vs. nonverbal IQ, or language level), which can be problematic, especially in studies involving children; and finally, social interaction with the experimenter might have an impact on performance, which is eliminated in computerized measurements (Weismer et al., 2018). A systematic review on executive control in ASD showed that impaired executive control, planning, or cognitive flexibility on both the Wisconsin Card Sorting Test and tower tasks are attenuated with computer administration. These findings suggest that dealing with social feedback and rules is difficult for individuals with autism (Kenworthy et al., 2008). A recent meta-analysis studied the characteristics of executive dysfunction in people with ASD. The authors found robust overall group differences between neurotypical and autistic participants across a wide range of potential mediators; however, the effect size was reduced after they excluded self-report/questionnaire data (Demetriou et al., 2018). They also found an attenuating effect on executive dysfunction of the computerized assessment format overall and on concept formation and response inhibition subdomains (Demetriou et al., 2018). Because different conditions might result in various outcomes, it is important to take results from many scenarios into account in order to accurately quantify executive functions in autism.
The IPD theory proposes that the IPD preferred by people with ASD is a key aspect that needs to be considered. We think that the change in perceived group differences is due to not only the more predictable, standardized form and the visual instructions in computerized tests but also the greater distance from the experimenter in these situations. Because the information on this parameter is not available in most of the previous studies, it is not possible to systematically investigate the already existing studies on the effect of IPD with meta-analyses. In the future, studies with experimental distance manipulations are warranted to address this issue.
Technology-Based Interventions Provide Comfortable IPD
Cognitive training and cognitive remediation
On the basis of our IPD theory, we suggest that technology-based interventions could help improve skills in people with autism and other neurodevelopmental syndromes. In studies using computer-based remote solutions, the IPD is certainly large enough to ensure that existing competences are available to achieve the right performance. The benefits of computerized solutions are obvious in many areas, but can this approach work in situations that were previously explicitly human-assisted, such as education, skills development, and therapy? Systematic reviews and meta-analyses found that technology-based interventions (via a desktop computer, interactive DVD, shared active surface, and virtual reality) were effective overall at improving social and communication skills in people with ASD; however, the results on generalizability and maintenance of the effect or improvement on standardized tests remain controversial (DiGennaro Reed et al., 2011; Grynszpan et al., 2014; Ramdoss et al., 2011; Wainer & Ingersoll, 2011).
In a recent review, Pasqualotto et al. (2021) examined the effect of cognitive training programs on executive functions, comparing the computerized and noncomputerized interventions in people with ASD. Noncomputerized training had positive effects on executive functions (shifting, flexibility, and problem solving) when delivered at home or school (ecologically valid environments), whereas cognitive remediation contributed to the improvement of working memory and verbal fluency. In the case of computerized training, attention (divided and sustained), working memory, and inhibition control improved more among participants than in the control group. However, without human interaction, the improvement of executive functions seemed to be less generalizable to other (e.g., social and communication) skills (Pasqualotto et al., 2021). Yet the benefits of digital technology are not negligible. Computerized methods are more predictable, and they offer clearly defined and often visually supported instructions or visual or auditory feedback. The setting decreases sensory stimulation, requires less social interaction, and provides self-paced application. Moreover, in line with our theory, they provide comfortable-enough IPD. All of the above can help reduce experienced stress and arousal, providing the best learning environment and cognitive performance (D. K. C. Murray, 2011; A. Murray et al., 2022; Pasqualotto et al., 2021).
Gamification and gaming culture
In line with computerized cognitive training, IPD theory promotes gamification to support treatments by providing a large-enough IPD. Computers, computational tools, and gamification have become increasingly widespread to support treatments of a wide variety of diseases. Recently, mental health professionals have also started to contribute to the development of gamified tools for ASD. The aim of these experiments is to make certain that therapeutic or skill-training elements are playful while providing a good gaming experience. Games would provide a safe environment for facilitating collaboration and social interactions (e.g., Benton et al., 2012; Parsons et al., 2004; Whalen et al., 2010); the gamification of classical therapeutic elements, however, is not yet engaging enough (Malinverni et al., 2017), and their applicability is limited (Ben-Sasson et al., 2013; Marwecki et al., 2013). However, the development of video games and virtual reality environments to improve social communication and other skills is becoming increasingly popular (e.g., Kim et al., 2020; Terlouw et al., 2020, 2021); for a recent review, see Atherton & Cross, 2021).
Children, adolescents, and adults with ASD have a well-developed gaming culture in an extensive range of computer or video games (Mazurek & Engelhardt, 2013); however, their preferences and habits are different from those of their neurotypical peers (Craig et al., 2017; A. Murray et al., 2022). They perceive the benefits of computer-mediated communication, but they use it in specific ways (Gillespie-Lynch et al., 2014). An ethnographic case study of three children with ASD has shown that social interactions in online multiplayer games, such as sharing information; making requests; communicating rules; maintaining engagement; or using, interpreting, and mirroring gestures in virtual spaces, might support their capacity to initiate and sustain social interactions in physical spaces (Stone et al., 2019). Another interesting exploratory case study used a multiplayer online role-playing game to explore the emotional awareness and expression skills of five young adult participants with ASD. The authors suggest that advancements in virtual environments might help with the development of social skills in the future (Gallup & Serianni, 2017). A semi-structured interview with three adolescents and young adults with ASD revealed that participants perceived the virtual platform of video games as a safe environment and had an increased level of comfort and self-awareness. However, children with ASD tend to play more role-playing games than first-person shooting games, avoiding the sensory overload of fast-paced, audiovisually intense, and psychologically arousing violent games (Mazurek & Engelhardt, 2013). By avoiding the unpredictable and anxiety-provoking face-to-face interactions of the physical world, they could cooperate, develop conversations, and even maintain relationships from a distance (Gallup et al., 2016). These findings support our hypothesis that the impairments in the functioning of people with ASD are not solely due to a lack of competence but also to the overwhelming and suboptimal environment in which their performance is significantly below the best possible.
Downsides and differences of computer-mediated communication and gaming in people with ASD
Individuals with ASD might prefer computer-mediated communication because it allows interactions from a safe distance with higher control and fewer contextual and sensory distractions; however, they do not necessarily profit from it in real-life social situations (Paulus et al., 2020). Moreover, a longitudinal study has shown that although more autistic traits in general do not relate to the overuse of the Internet, gender is a risk factor: Women with more autistic traits are at higher risk for compulsive Internet use (Finkenauer et al., 2012). A recent study reported that individuals with ASD play more often by themselves rather than in multiplayer mode. In their study, they found that young participants with ASD are vulnerable to gaming disorders (Paulus et al., 2020), and a recent systematic review has confirmed that children and young adults with ASD spend more time playing video games and have a higher risk for problematic gaming (A. Murray et al., 2022).
Results so far suggest that individuals with autism prefer a safe distance; reduced sensory information load; slower, self-paced tempo; and written/visual instructions in computerized communication or gaming. Despite the presumably lower levels of stress, they cannot fully exploit the social benefits of these activities. It is possible that, in some cases, the distance is no longer safe but is so large that it leads to a permanent withdrawal, and isolation, from which it is very difficult to establish contact. However, video games are sometimes the first or only opportunity for social interaction. They provide an opportunity not only to communicate casually with other players in the game but also to build friendships between people from distant parts of the world and to use the game as a common topic to start a conversation in offline gaming-themed gatherings or in general social situations (Finke et al., 2018). To sum up, on the basis of IPD theory, computer-game-based treatment methods may be applicable to children and adults with ASD. More studies are warranted to discover and develop guidance to avoid the negative effects of computer games.
Challenging factors and counterarguments
Although the importance of IPD or even preference for larger IPD can be seen in a wide range of situations, there are two extreme scenarios in real life: when someone is at zero distance with full skin contact (e.g., sexual intercourse) or when the other person is not present at all. Social interactions are inherently complex and in addition to the spatial dimension (e.g., preferred IPD), additional factors need to be considered. The sensory preferences (e.g., hypersensitivity) and the ability to communicate them are highly relevant while having sex (Gray et al., 2021). We think that low IPD could more easily result in sensory overstimulation and that some autistic people can cope with this difficulty and enjoy sexual activity, whereas others voluntarily deprive themselves of sexual experiences, at least partly, to avoid sensory overstimulation. Furthermore, we believe that even autistic people who can cope with sensory stimulation have different preferences than neurotypical individuals considering the pace of a romantic relationship. Autistic people possibly need a longer time period to get to know a new partner, develop trust, and be ready for sexual intercourse. Moreover, communicating their preferences to their partner can also be more challenging for autistic people. In addition, these difficulties and a preference for a slower pace can also emerge in nonsexual intimate relationships, such as with close family members, friends, and peers. Further studies are warranted to investigate this topic, especially because the well-being of autistic people could benefit from the implications of such studies. However, a deeper discussion of this topic is beyond the scope of the present article.
The other extreme situation is when the other person is absent. A recent study on communication-mode preferences in people with ASD shows that they generally avoid phone calls (Howard & Sedgewick, 2021). If IPD is the only defining factor for people with ASD, this would be contradictory: During phone calls, IPD is large, so it should be pretty comfortable. But this is not the case. The narrative analysis revealed that partial information (visual metacommunicative signs are missing but difficult-to-interpret vocal signs remain), expectations of instant replies, difficulty with appropriate timing, or the unpredictability of an unknown person might be relevant as well (Howard & Sedgewick, 2021). Individuals with autism preferred face-to-face over written communication only when the setting was safe and settled for a longer time (family, friends, education, or employment). In this study, video chat and video conference platforms were not included; they became widely used during the COVID pandemic. One would assume that if IPD were the only thing that mattered, lockdown and online communication would be seen as a positive change. A recent study (Pellicano et al., 2020) highlights that a reduction in face-to-face activity (e.g., education, work, commuting, therapy sessions) is not a problem to a certain degree and for a certain type of autistic person, but it also has drawbacks and is not easy for everyone (Pellicano et al., 2020). It raises the issue that during video conferences the other person’s face on the screen may seem too close or the distance cannot be controlled, and more people can be in front of the viewer at the same time than in real-life situations.
Overall, in addition to distance, the following factors require further investigation. In terms of temporal dynamics, the social relationships in ASD can develop either extremely slowly (a lot of patience is required even in therapeutic relationships) or uncomfortably quickly. Here, again, the disruption of the adaptive capacity of approaching behavior and the diversity of ASD seem to be important factors. In the quality of relationships, factors such as trust, safety, and familiarity (caregiver, spouse, very close friend, professional helper, acquaintance, unknown person) and the number of people who can fit in each category or can be present at the same time (limited by the mentalization capacity) might also be considered relevant.
We think there may be other processes involved in fine-tuning IPD than the basic discrepancies mentioned above. For example, it should involve appropriate timing, verbal and nonverbal reciprocal communication, and mentalizing (reading and expressing nonverbal, metacommunicative cues). Difficulties in these areas are also characteristic of autism. We consider IPD as a separate, potentially atypical “symptom” dimension. In this article, we emphasize the importance of systematic measurement of IPD in a time-limited, cross-sectional setting by an unknown investigator, which is a laboratory prototype for many everyday situations.
Recommended Study Design to Test Cognitive Functions in Different Settings
Recommended study design
Given the empirical evidence discussed above, IPD seems to be an important factor to consider in people with ASD; however, systematic studies are warranted. We suggest comparing cognitive, social, and communication performance with well-established methods in five different settings: (a) in-person task administration (with a measured distance), (b) computerized versions of the same tests in the presence of the experimenter (with a measured distance), (c) the examiner at a higher distance, (d) under laboratory conditions with the participant and experimenter in separate rooms, and (e) without social interaction, by remote online participation at home (Fig. 1). The five different settings allow the following comparisons: The difference between settings (a) and (b) provides information about the effect of the human, verbal, and acoustic versus the computerized, written, and visual instructions and feedback; the (b) versus (c) comparison shows the effect of greater distance; the (c) versus (d) comparison reflects the difference between the presence (distant but physically perceptible) or absence (only a mental representation available) of the experimenter; and the (d) versus (e) comparison marks the difference between a laboratory, unfamiliar environment (including potential sensory distractors) and the natural, familiar environment.
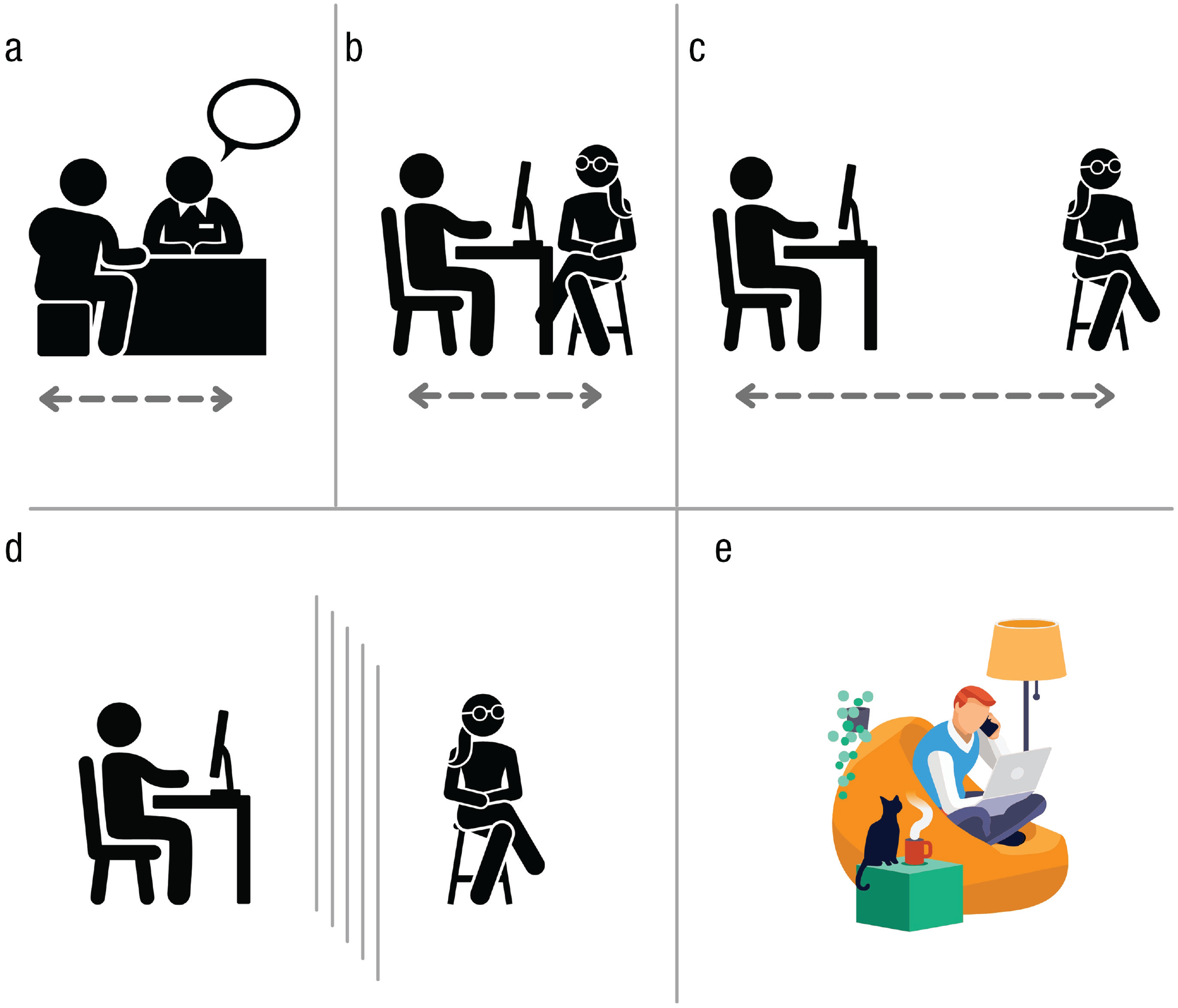
Measuring performance in five different settings: (a) in-person task administration, (b) computerized task administration with the same measured distance between the participant and experimenter as in (a), (c) computerized task administration with a larger distance, (d) computerized task administration with the participant and experimenter in separate rooms, and (e) remote task administration (i.e., online participation from home).
Potential relevance, real-life implications
If behavioral and neuropsychological studies support the IPD theory in autism, namely, that IPD does indeed play a role in the social and cognitive performance of autistic people, it will be worth taking this into account in interactions with people with ASD in many areas of life. First, it might be necessary to provide more interpersonal space during therapy and education for people with special needs: teaching and applying the techniques needed for social interaction, first without face-to-face interaction (from an age rife with electronic device use) and then from a greater distance. However, it might be generalized even to intellectually disabled, nonverbal individuals with autism as well. To determine the comfortable distance in their case and how this information could be used properly requires further consideration. The message for them might be that caregivers and helpers should keep in mind that preferred IPD might vary in different situations, and it might affect the motivation and performance of these people, too.
It could be especially important to provide space for withdrawal after or during emotionally demanding situations, for example, at school, and at workplaces. This would be beneficial not only because it might prevent (or help manage) potential meltdowns, shutdowns, or tantrums but also because it might help use existing skills and resources or even achieve optimal performance for individuals with ASD (Fig. 2). IPD theory can be used to explore the issue of competence versus performance in neurocognitive functions in this population. Specifically, using IPD theory, we can disentangle whether a cognitive or social function in people with ASD is truly severely impaired at the level of competence or whether an overwhelming social factor, such as a preference for short IPD, is impeding their performance.
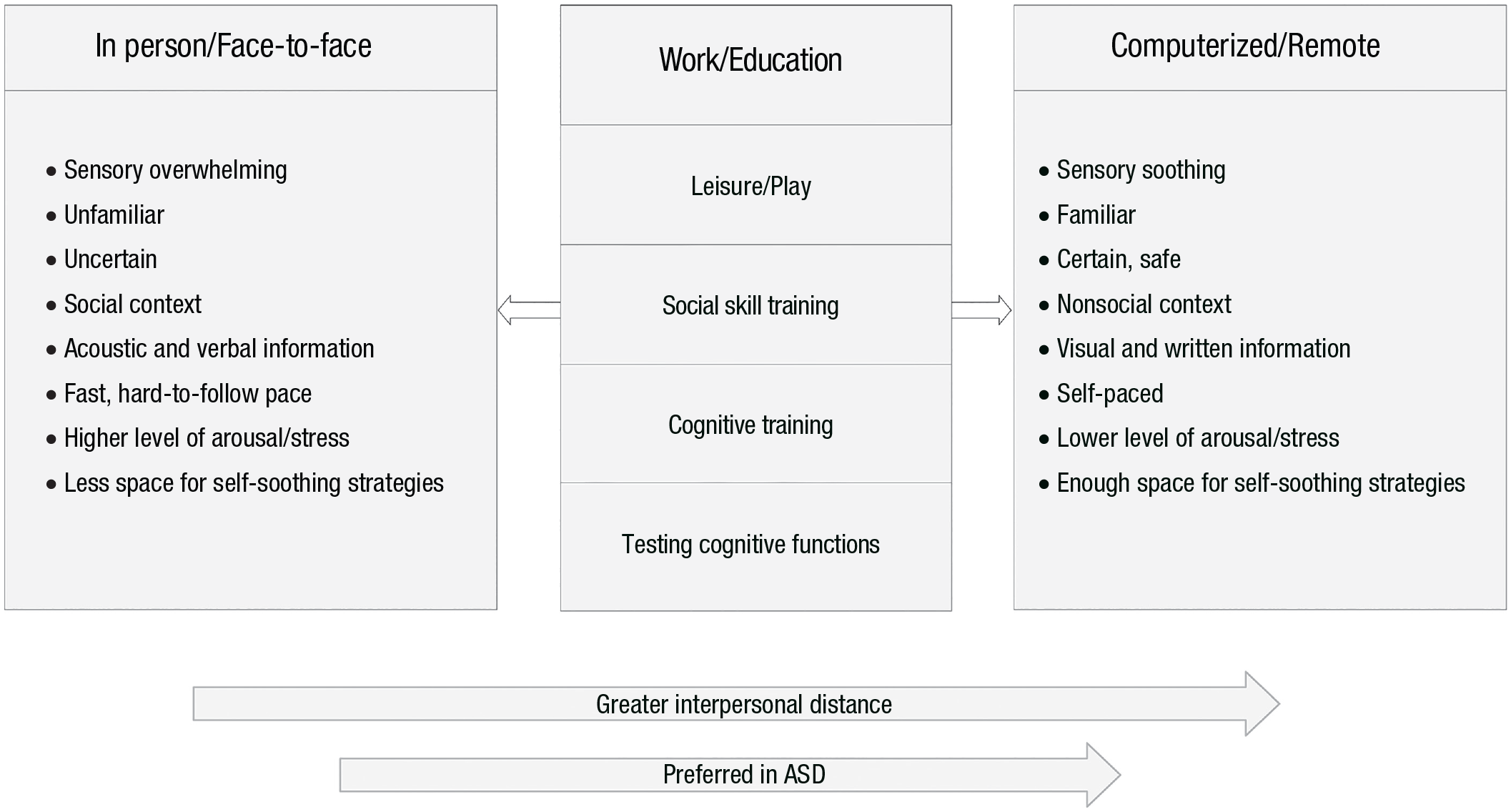
Summary of the differences between in-person and remote activities. ASD = autism spectrum disorder.
Conclusion
Here, we have described the IPD theory of ASD, which implies that autistic traits (including social difficulties and cognitive dysfunctions) might be affected by social context involving uncomfortable IPD. The IPD theory explains inconsistent empirical findings on several measures, such as executive functions or social communication, and provides a context for the typical gaming culture in people with ASD. Moreover, it provides a framework for therapeutic and educational approaches, suggesting that these processes might benefit from the adjustment of IPD.