
Abstract
Genital prolapse is very rare in neonates. In neonates affected by spina bifida, genital prolapse can occur due to improper nerve supply to the pelvic diaphragm. When genital prolapse occurs in neonates, it can be associated with severe morbidity as time goes on, since inflammation and infection can develop. This study reports a 3-day-old female neonate who presented with genital prolapse associated with meningomyelocele, which was successfully treated with bottle nipple support left for 5 days after digital reduction and surgical repair of the meningomyelocele. Type one genital prolapse in neonates can be successfully treated with surgical meningomyelocele repair, digital reduction of the prolapse, and leaving a bottle nipple in the vaginal canal. However, given that the meningomyelocele repair was performed shortly before reduction and that spontaneous resolution after spinal repair has been reported, the success of bottle nipple device use can be associative rather than causal. After leaving a bottle nipple in the vaginal canal, the following precautions should be taken to decrease the risk of vaginitis. A new bottle nipple, which has never been previously used for feeding, should be used, and the bottle nipple insertion should be done using sterile gloves. The perineal area should be cleaned with sterile saline during routine diaper changes. Last but not least, the genital area should be closely inspected for any change of color, swelling, discharge, or expulsion of the bottle nipple.
Plain language summary
Genital prolapse is a condition where pelvic organs descend from their normal position and bulge into or out of the vagina. This condition is very rare in newborns. In newborns affected by spina bifida, genital prolapse can occur due to improper nerve supply to the pelvic diaphragm, which is a very important supporting structure. When genital prolapse occurs in newborns, it can be associated with severe complications as time goes on, since progressive injury and infection can develop. This study reports a 3-day-old female neonate who presented with genital prolapse associated with meningomyelocele (a type of open spina bifida), which was successfully treated with bottle nipple support left in the vaginal canal for 5 days after digital reduction and surgical repair of the meningomyelocele. Type one genital prolapse in newborns can be successfully treated with surgical meningomyelocele repair, digital reduction of the prolapse, and leaving a bottle nipple in the vaginal canal. However, to decrease the risk of infection, the following precautions should be taken. A new bottle nipple, which has never been previously used for feeding, should be used, and the bottle nipple insertion should be done using sterile gloves. The genital area should be cleaned with sterile saline during routine diaper changes. Last but not least, the genital area should be closely inspected for any sign of infection, or expulsion of the bottle nipple.
Introduction
The supportive role of the pelvic diaphragm is affected when factors impact its muscles or nerves. 1 In this regard, meningomyelocele is a potential cause of prolapse. 1 Nulliparous young females with spina bifida have a higher likelihood of experiencing genital prolapse. 2 The number of motor neurons innervating the levator ani muscle in fetal rats with spina bifida is smaller, and their distribution is irregular. 3 Sacral neuromodulation was found useful in the management of urogynecologic dysfunctions, showing the role of sacral nerves in urogenital function. 4
Females with genital prolapse usually have impairment of the pelvic diaphragm. 1 The pelvic diaphragm is in a tonic contraction, and when intra-abdominal pressure rises, so does its tone. 1 This key function of the pelvic diaphragm is dependent on its innervation, which is from the pelvic plexus with nerves originating from sacral segments 4 and 5. 1
Genital prolapse is commonly seen in older multiparous women since vaginal delivery can lead to harm to the support structure, including pelvic floor muscles and nerves. 1 However, we couldn’t find any study that compares in vitro fertilization with natural conception regarding the risk of genital prolapse. Its occurrence in neonates is exceedingly rare.1,5–8 In newborns affected by spina dysraphism, pelvic organ prolapse is considered to occur due to improper nerve supply to the pelvic diaphragm.5,6,9
Genital prolapse in neonates is associated with greater morbidity as time goes on, since inflammation and infection can develop.10,11 In this study, we report a 3-day-old female neonate who presented with genital prolapse associated with meningomyelocele, which was successfully treated with bottle nipple support left for 5 days after digital reduction and surgical repair of the meningomyelocele. This case report conforms to the CARE guidelines. 12
Illustrative case
A 3-day-old female neonate presented with swelling in the lower back and a mass protruding through the vagina since birth. She was the first child of non-consanguineous parents. She was born to a 27-year-old mother at a gestational age of 39 weeks via spontaneous vertex delivery. The labor lasted for around 1 hour. Her birth weight was 2900g, and her head circumference was 35 cm. The mother had regular antenatal care and received an iron supplement and a tetanus vaccination during pregnancy. However, no antenatal ultrasound was done. There was no history of connective tissue diseases in the family. On examination, there was a meningomyelocele located on the thoracolumbar region, bilateral club foot, and a reducible genital prolapse with vaginal mucosa and cervical os visible (Figure 1). There was no movement of the lower extremities. The baby had normal sucking and Moro reflexes. Abdominopelvic ultrasonography showed two normally positioned kidneys, with no hydronephrosis or hydroureters. The uterus could not be visualized on the ultrasonography. Echocardiography and transfontanel ultrasound were normal. Meningomyelocele repair was done on the 4th day of life. Preoperative picture that shows thoracolumbar meningomyelocele (red arrow), genital prolapse (black arrow), club foot (yellow arrow), and cervical os (purple arrow).
Around 5 hours after the completion of the meningomyelocele repair, digital reduction of the prolapse was done, and a nasogastric tube was inserted as a urinary catheter. Then, a new bottle nipple was inserted into the vaginal canal (Video 1 and Figure 2(a)). It was handled with sterile gloves during insertion (Video 1). Before insertion, the bottle nipple was inserted in boiling water for 10 minutes. The perineal area was being cleaned with sterile saline during routine diaper changes. On the 5th day after bottle nipple insertion, there was no sign of infection or expulsion of the bottle nipple (Figure 2(b)). Then the bottle nipple was intentionally removed. Three weeks after meningomyelocele repair, the child was reassessed, and there was no genital prolapse even during crying and defecation (Figure 3 and Video 2). The child had no recurrence of the prolapse at 6 months of follow-up. (a) Shows the bottle nipple used for temporary support to avoid the recurrence of genital prolapse (red arrow). (b) Shows the bottle nipple placed inside the vaginal canal after 5 days of insertion, just before the removal (blue arrow), and a nasogastric tube inserted into the urinary bladder (green arrow). A picture that was taken 3 weeks after meningomyelocele repair that shows the absence of genital prolapse while the patient is defecating.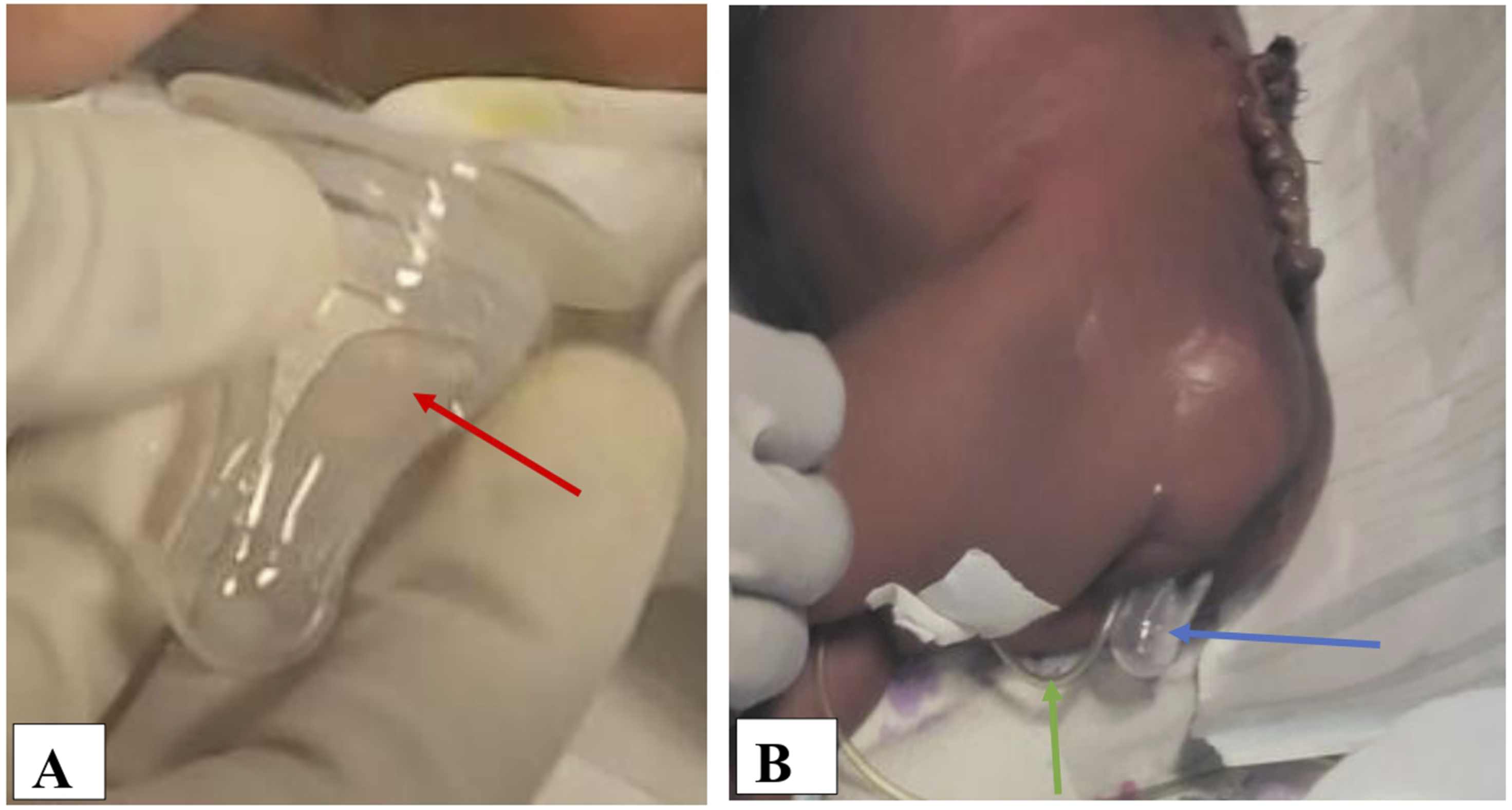

Discussion
Neonatal genital prolapse appears as a tumor that protrudes from the vulva. 8 The differential diagnosis encompasses vaginal polyps, urethral prolapse, paraurethral cysts, and rhabdomyosarcoma.13,14 Cervical and vaginal polyps typically resolve on their own; they are distinguishable by the lack of the cervical os and exhibit normal findings on pelvic ultrasound or computed tomography.13,14 Rhabdomyosarcoma is identified by a fleshy, lobulated tumor that usually has regions of bleeding and tissue necrosis, and it is also not reducible; confirmation is by tissue biopsy.13,14 In our patient, there was a prolapsed vagina and uterus, and the cervical os and the circumferential arrangement of the vaginal mucosa were clearly visible (Figure 1). Moreover, there is no tissue necrosis or bleeding (Figure 1).
Urethral prolapse and paraurethral cysts primarily manifest with urinary symptoms while the vaginal introitus appears normal.13,14 In one study, a neonate with two duplex kidneys, exhibiting hydronephrosis along with a ureterocele in the bladder and genital prolapse, was discussed, and the mass was confirmed to be an ectopic ureterocele on an ultrasound. 15 In our patient, the clinical evaluation and the ultrasound findings confirmed that the diagnosis was genital prolapse, and there was no abnormality of the urinary tract.
There are two types of genital prolapses in neonates. Type 1 refers to prolapse associated with spina bifida, while type 2 is not associated with spina bifida. 5 In type 1 cases, a more complex reduction process is often necessary to prevent recurrence.5,7,10,14 Breech presentation, nutritional deficiencies during intrauterine life, prematurity, prolonged dexamethasone use, and neonatal tetanus are raised as associated factors in type 2 neonatal genital prolapse.7,8,16 Breech presentation may cause muscular weakness and underdevelopment of pelvic suspensory and supporting tissues. 8 The significance of nutritional deficiencies during intrauterine life, prematurity, and prolonged dexamethasone use was highlighted in a case report about an infant born at 26 weeks of gestation with a birth weight of 565g. 16 From the works of literature Henn et al. (2015) reviewed, they found that newborns with genital prolapse associated with spina bifida usually have cephalic presentation. 5 The genital prolapse of our patient is type one, and she had cephalic presentation, normal birth weight, and was born at term.
A prenatal diagnosis of genital prolapse by an ultrasound has been reported. 8 In prenatal ultrasound, fetal ambiguous genitalia is a competing differential diagnosis for a genital prolapse. In this case, determining androgen levels in the maternal blood, assessing the CYP21 gene of the parents, and fetal karyotyping are highly beneficial. 8 In our patient, there was no prenatal ultrasound done, and both the meningomyelocele and genital prolapse diagnoses were made after birth.
The management of neonatal genital prolapse includes digital reduction, the use of pessaries, meningomyelocele repair, labial suturing, purse-string suturing of the vagina, cervical amputation, uterine ventrosuspension, and, in some cases, hysterectomy.6,17,18 Although digital reduction is usually done without anesthesia, it can also sometimes be done under general anesthesia, mainly if the prolapsed tissue is edematous.10,11 We did digital reduction around 5 hours after completion of the meningomyelocele repair, after the anesthesia wore off.
The use of a pessary is recommended mainly in neonates with an associated spina bifida, since manual reduction alone can result in recurrence. 7 After a few days, when the pessary is removed, the possibility of recurrence is low, the possible reason being the effect of the maternal hormones, which results in the laxity of the fetal pelvic floor diminishing. 7 As an alternative to pessaries, bottle nipples can be used. 7 For our patient, we used a bottle nipple inserted after digital reduction. However, since the meningomyelocele repair was performed shortly before reduction, the prevention of recurrence of the prolapse with a pessary can be associative rather than causal.
The use of nipple for the treatment of neonatal genital prolapse with an associated meningomyelocele has been reported. 9 The authors illustrated the resolution of the prolapse 3 days after meningomyelocele repair, and the repair was done on the 3rd day of age. The authors suggested that, most of the time, conservative management with temporary mechanical support using a nipple or a pessary is an effective solution. 9 In our setup, there is no protocol to choose a commercially available pessary over a bottle nipple device. We chose a bottle nipple device because a commercial pessary was unavailable.
The duration that is recommended to leave the pessary in situ is not clearly known, and prolonged use may lead to vaginitis.10,19 Johnson et al. (1984) reported that they removed the pessary after 1 week. 10 When pessaries are used for the treatment of neonatal genital prolapse, topical estrogen and antibiotic creams can be applied.10,14 In a case report by Dixon et al., the Penrose pessary they used resulted in yellowish discharge around the 3rd day, at which time they removed the pessary and reinserted another for an additional 2 days. 19 Even though we were not certain for sure for how long the bottle nipple device should be left, we kept the device in the vagina for 5 days. To decrease the risk of infection, we used a new bottle nipple that had never been used for feeding. Moreover, the bottle nipple was put in boiling water for 10 minutes and inserted using sterile gloves.
A genital prolapse in a newborn that was successfully treated with digital reduction and then application of bandage straps over both thighs and the buttocks for 3 days is reported. 20 Even if the authors raised the method is easy to adopt, they shared their concern regarding the possibility of recurrence since the baby in their case report died within around a week due to meningitis. 20 Therefore, long-term follow-up was not possible. 20 We didn’t use this mode of treatment for fear of a possible high risk of recurrence.
Abdelsalam et al. (2006) utilized a Foley catheter to reduce genital prolapse permanently. 14 They inserted an eight French Foley catheter intravaginally after digital reduction of the genital prolapse, then they inflated the catheter with 4 mL of normal saline. They left the catheter for 2 weeks. The baby didn’t develop recurrence. 14 The authors recommended initial digital manual reduction and recommended the use of a Foley catheter if it is recurrent or associated with spinal dysraphism. 14 We didn’t use a Foley catheter for vaginal support since the bottle nipple was more easily available, and it was successful. Moreover, there is a case report that showed using a Foley catheter for vaginal support may lead to agitation and rectal prolapse. 6
In infants with spina bifida, the recurrence rate remains elevated until the spinal defect is surgically corrected. 5 Aykanat et al. (2020) described a newborn experiencing genital prolapse associated with meningomyelocele, where the prolapse improved on its own following the surgical repair of the meningomyelocele. 18 Initially, it was treated with manual reduction multiple times. 18 The neonate was operated on for meningomyelocele at the age of 13 days. Four days after the surgery, the genital prolapse recurrence ceased to exist. 18 The authors suggested that surgical intervention for meningomyelocele, along with monitoring natural recovery of the genital prolapse, appears to be the most effective and conclusive approach for neonates experiencing genital prolapse with associated meningomyelocele. 18 In our patient, the meningomyelocele repair may have had a major role in the successful treatment.
On the contrary, Yildizdaş et al. (2019) reported a neonate with genital prolapse after meningomyelocele repair surgery. 6 The neonate was operated on on her 3rd day of life for meningomyelocele, and then she developed genital prolapse on the 6th day. They did digital reduction, but the prolapse reoccurred. 6 Later, they inserted an 8-F Foley catheter and inflated the balloon after digital reduction. However, the authors removed the catheter since the child became agitated and developed rectal prolapse. 6 She had recurrent genital prolapse until the age of two months, but it was reducible. After the age of 2 months, the prolapse spontaneously resolved. The authors attributed the meningomyelocele repair surgery as a risk factor for the prolapse in their report. 6 The occurrence of neonatal genital prolapse around two days after meningomyelocele repair is also reported. 19 The finding in our patient rather suggests the benefit of meningomyelocele repair in the resolution of the prolapse.
Surgeries other than meningomyelocele repair in the region of the sacral spine can lead to genital prolapse. A newborn who developed genital prolapse after resection of sacrococcygeal teratoma is reported. 13 The authors suggested that the method used during surgery for the sacrococcygeal teratoma resection might impact the neonate’s pelvic anatomy and lead to vaginal prolapse. 13 When colposacropexy is decided, the mini-laparoscopic technique is more advantageous than the robotic method regarding the duration of the surgery, amount of blood loss during the procedure, level of pain after the surgery, and cosmetic results. 21
Surgical treatment for neonatal genital prolapses can be necessary when conservative approaches fail or when there are signs of vaginal mucosal hypertrophy or ulcerations.6,13,14 Various fixation methods have been established. More extreme surgical alternatives like hysterectomy or cervical amputation are seldom performed these days. 14 Saksono et al. (2015) reported a case of neonatal genital prolapse not associated with spine dysraphism that was managed with a purse-string suture of the vaginal wall. 11
Genital prolapse in newborns generally occurs within the first few days after birth. 22 Late presentation can make the prolapse manually non-reducible. A 3-month-old infant for whom uterine ventrosuspension was performed due to the delayed presentation has been reported. 22 Our patient presented within 3 days, and manual reduction was possible; nonsurgical treatment of the genital prolapse was also successful.
Genital prolapse can lead to stress urinary incontinence, which is linked to a reduced frequency of sexual intercourse, lower satisfaction, and reduced quality of life.23,24 Resection of the uterus, preferably with a minimally invasive approach, 25 as a treatment for genital prolapse, can be done, but it will affect fertility. Gender bias should be avoided in the approach to infertile couples, which will be quite troublesome in women with genital prolapse. 26 To restore fertility after uterine resection, uterine transplantation can be done. 27 Uterine transplantation eliminates the debates linked to surrogacy. 27 The success is better if the donor is a living woman. 27 However, transplantation forces the use of immunosuppressive drugs. In the future, tissue engineering might obviate the use of immunosuppressive drugs. 27
Lessons
This case shows the potential of meningomyelocele, a type of open spina bifida, to result in genital prolapse. Moreover, it shows that type one genital prolapse in neonates can be successfully treated with meningomyelocele repair, digital reduction of the prolapse, and leaving a relatively easily available bottle nipple in the vaginal canal. However, given that the meningomyelocele repair was performed shortly before reduction and that spontaneous resolution after spinal repair has been reported, the success of bottle nipple device use can be associative rather than causal. Moreover, to decrease the risk of vaginal infection, the following precautions should be taken. A new bottle nipple that has never been used for feeding should be used, and the bottle nipple insertion should be done using sterile technique. Before using the bottle nipple, inserting it in boiling water for 10 minutes may help. The genital area should be cleaned with sterile fluid during diaper changes. In addition, the genital area should be closely inspected for signs of infection and expulsion of the bottle nipple frequently. In this patient, no recurrence was observed with 6 months of follow-up, but still, late recurrence is possible, and indefinite absence of recurrence cannot be assured.
Supplemental material
Supplemental material
Footnotes
Author note
This study has never been presented or published in part or whole.
Acknowledgements
The authors gratefully acknowledge the mother of the child described in this report for her informed consent to publish these clinical details. We would like to thank our patient’s mother for her permission to publish this case and use the diagnostic images.
Ethical considerations
No ethical approval is required for this study since it is a case report. The patient’s anonymity is kept, and identifying details are omitted.
Consent for publication
Written informed consent was obtained from the patient’s mother for the publication of this case report and any accompanying images and videos.
Author contributions
Conceptualization: EFY, HTM, GDT; Methodology: YGZ; Data curation: EFY, HTM, YGZ, AZZ, MYS; Investigation: EFY; Validation: EFY, GDT, YGZ, AZZ, MYS, AAM; Supervision: EFY, HTM, GDT, AZZ, MYS, AAM; Visualization: EFY, HTM, GDT, YGZ, AZZ, MYS, AAM; Project administration: EFY; Writing original draft: EFY, HTM, GDT, YGZ, AZZ, MYS, AAM; Writing review & editing: EFY, HTM, GDT, YGZ, AZZ, MYS, AAM.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the necessary data and materials can be accessed from the corresponding author.
Disclosure
We, the authors, declare that in this manuscript, there was no use of a generative Artificial Intelligence in creating text, references, images, or other content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.