
Abstract
Background
Physiotherapy treatment for women with pelvic organ prolapse (POP) requires a holistic approach based on tensegrity theory and fascial connections.
Objective
The study examined the tension of transverse body structures (transverse diaphragms) in healthy women and women with pelvic organ prolapse. To draw attention to the fact that treating women with pelvic organ prolapse requires a holistic approach and not just pelvic floor muscle exercises.
Design
A cross-sectional studies.
Methods
The women were divided into an experimental group with pelvic organ prolapse (POP) n=31 and a healthy control group n=29. Measurements were taken with eyes open and eyes closed. The tension force of each diaphragm and the simultaneous tension of the three diaphragms were compared.
Results
A significant difference was identified between diaphragm tension with eyes open and closed p<0.0001 in both study groups. In both groups, there was no statistical relationship between the diaphragm muscle and the diaphragm of the foot with eyes closed; in the group with POP p=1, and in the control group p=0.2291. The values for the tentorium cerebelli/tongue (clamping force between the maxilla and the mandible) were similar with open and closed eyes in both groups. For open eyes p=0.486 and closed eyes p=0.0929. The Permanovas for the open-eyes and closed-eyes test showed that the two groups had different effects in terms of the traits studied p<0.0001. PCA-biplots show that the group of women with pelvic organ prolapse differs in terms of simultaneous tension of the three diaphragms compared to the control group of healthy women with eyes open and closed.
Conclusion
The results obtained from preliminary observations suggest that assessment of the transverse structures in women experimental group with POP may indicate that physiotherapy should involve working with the whole body.
Introduction
All structures in the human body are a unity that can influence each other with their tension. 1 According to the theory of tensegrity proposed by Richard Buckminster Fuller and Kenneth Snelson, an increase in the tension of one element of a structure causes a corresponding increase in the tension of its other elements that are in mutual structural contact. 2 This theory assumes that elastic elements remain taut or relaxed depending on where the force is applied and its vector. 2 In the tensegrity model of the human body, the bones form a compression system suspended within a network of constant tensions created by the musculo-fascial system. Fascia, as a connective tissue, plays a key role. It surrounds the body’s organs like a scaffolding and transmits tension along its fibers. 3
A significant role is played by the fascial system, which has important functions in the human body, as fascia has the ability to contract like muscles. 4 The fascia has a protective, supportive and cohesive role for the various components, thus enabling the body to function properly as a whole. 5 Its function is to maintain the proper alignment of organs and tissues and to transmit forces during movement. 5
In the human body, we also have transverse diaphragms (formed mainly of soft tissues) like the tentorium cerebelli, tongue, thoracic outlet, thoracic diaphragm and pelvic floor). These five diaphragms are in close relationship with the fascial system. 6 The feet can also be thought of as a diaphragm in the body, as they are the first structure when the foot makes contact with the ground, they are an important sensory structure. A fascial connection with the feet means that the fascial tissues in the feet are linked to the fascia in other parts of the body, forming fascial ‘chains’ that can transmit tension and influence different areas of the body. 7 Myers indicates that there is a fascial connection from the tongue to the feet. Following this line of thought and taking the tensegrity theory into account, we adopted a classification of the body’s transverse anatomical structures as “diaphragms”. 8 Taking into account the anatomical attachments of the tentorium cerebelli - including those on the temporal bone, which forms the temporomandibular joint with the mandible - as well as fascial connections and the tensegrity theory, which describes the transfer of tension forces from one structure to another, we adopted the measurement of clenching force between the maxilla and the mandible. 9
Ultrasound studies have shown a decrease in type I collagen with an increase in type III collagen and fragmentation of elastin fibres in the intracellular matrix of the fascial-muscular structures of the pelvis in women with POP (pelvic organ prolapse), which in turn promotes increased elasticity of pelvic floor structures. 10 It is worth emphasising that maintenance of proper genital statics is significantly influenced by correct body weight, physical activity, healthy daily habits (regular emptying of the bladder and rectum). Proper posture is also important, namely, correct distribution of forces, avoidance of excessive ‘up and down’ pressure, pelvic floor muscle exercises, and hormone replacement therapy during menopause.11,12
An increase in the incidence of pelvic organ prolapse has been observed in women with their age. 13 The average age of women presenting for a medical appointment due to POP is 61 years, while women aged 30-39 years also benefit from medical attention. 13 It is believed that vaginal delivery, pregnancy, birth weight of the baby, the age of the woman, body mass index, levator defect, and levator hiatal area are risk factors for POP. 14 In contrast, caesarean section and smoking are protective factors for primary prolapse. 14
Taking into account the importance of the fascial system and the five diaphragms in the body and the anatomical connections in which one structure can influence another, we decided to investigate whether the tension of the tentorium cerebelli/tongue, the thoracic outlet/diaphragm muscle tension and the measurement of the ground reaction of the feet could provide an answer as to whether the simultaneous tension of the diaphragms being checked could be related to the medical diagnosis of pelvic organ prolapse in women who were qualified for surgery and were assigned a score of 3-4 on the POP-Q (the Pelvic Organ Prolapse Quantification) scale.15,16
Prior to the study, the research hypothesis was defined:
(H1) – Group Differences in Transverse Structure Tension: Women with pelvic organ prolapse (POP) will exhibit significantly different tension patterns in transverse myofascial structures, including the maxilla–mandible bones, diaphragm, and feet, compared with healthy controls group.
(H2) – Visual Condition Modulation: The differences in transverse structure tension between women with POP (experimental group) and controls will be more pronounced under altered sensory conditions (eyes closed), indicating a role of visual input in postural and myofascial compensation.
(H3) – Systemic Integration Consistent with Tensegrity Theory: Altered tension in the transverse myofascial system in women with POP will demonstrate systemic adaptations consistent with tensegrity theory, showing functional interdependence between feet, diaphragm, and the maxilla–mandible bones.
Methods
This study was designed as cross-sectional studies aimed at evaluating tension in transverse structures in women with pelvic organ prolapse (POP) – experimental group compared with healthy women without POP – control group. The study followed the STROBE list. 17
Study setting and period
The study was conducted at the Department of Physiotherapy, Faculty of Physical Culture in Gorzow Wielkopolski, Poznan University of Physical Education, Poland. Data collection took place between October 2023 and May 2024. All examinations were performed in a controlled clinical environment to ensure consistent testing conditions.
Participants
Demographic characteristics of women.

Participants were divided into two groups: experimental group: women diagnosed with pelvic organ prolapse n=31 a score of 3-4 on the POP-Q scale (the assessment based on POP-Q was conducted by a gynecologist), a Body Mass Index (BMI - is a measure used to assess whether a person’s body weight is appropriate for their height. It helps determine if a person is underweight, has a normal weight, is overweight, or obese) value of 27.21±7.41 (Table 1). Control group: healthy women without pelvic organ prolapse and without symptoms of pelvic floor dysfunction n=29, a BMI value of 26.49±4.32 (Table 1). The women in the control group were healthy individuals who reported engaging in physical activity once a week, such as long walks, yoga, or swimming.
All eligible women with POP admitted during the study period who met the inclusion criteria were considered; 55 were assessed, and 31 were included in the final analysis. Participants were recruited during routine clinical visits, and informed consent was obtained prior to enrollment. The control group comprised 29 healthy women from the general population meeting the inclusion and exclusion criteria. Convenience sampling was used.
Participants in the experimental group, after prior qualification according to the POP-Q scale by a gynecology specialist, were referred to the Department of Physiotherapy, Faculty of Physical Culture in Gorzow Wielkopolski, Poznan University of Physical Education, Poland for assessment of transverse structure tension. Participants in the control group were recruited through community advertisements. The researchers obtained written, informed consent to participate in the study from all participants in both groups, in accordance with the guidelines of the Declaration of Helsinki.
Inclusion criteria
Participants were eligible for inclusion if they met the following criteria: female sex, age ≥18 years, a clinical diagnosis of pelvic organ prolapse confirmed during gynecological examination (a score of 3-4 on the POP-Q), ability to understand the study procedures and provide informed consent.
Exclusion criteria
Were: pain in the temporomandibular joint(s) and snapping/snapping symptom, dental treatment, use of dentures/bridges, foot deformities that prevented the participant from assuming a standing position on the platform for the measurement, neurological disorders affecting motor control or balance, abdominal hernias, abdominal surgery, musculoskeletal disorders significantly affecting posture or gait, inability to perform the examination procedures, hypertension, use of physiotherapy, malignancy, and no written consent to participate in the study.
Study procedures
All the women in the pelvic organ prolapse experimental group and the control group received a diaphragm tension strength assessment. This examination was carried out between 10.00 a.m. - 1.00 p.m. All women in the study were informed before the measurements were taken. The women being examined were instructed to unintentional breathing during the measurement. Each woman underwent the measurement only once. The measurement was performed with the eyes open and closed. Eyes open (EO) – participants maintained a natural upright posture while looking straight ahead at a fixed point located at eye level approximately 2 meters away. Eyes closed (EC) – participants maintained the same upright posture with their eyes gently closed in order to eliminate visual input. The authors referred to clinical observations during childbirth, where women often close their eyes while bearing down. As well as to observe whether the measurement results with eyes open and closed would differ significantly. During the measurement, the women wore comfortable sports clothing (a T-shirt and leggings), and the measurement on the platform was performed barefoot. The platform surface was disinfected after each participant.
Assessment of tension force between the maxilla-mandibula bones, diaphragm muscles and feet (Figure 1)
The tension of the three diaphragms was measured simultaneously, i.e. the tension force between the maxilla-mandibula - tentorium cerebelli/tongue, push force - tension of the diaphragm muscle and feet (reaction of the ground forces) were evaluated, with the measurement time set at 30 seconds. Measurements were carried out with eyes open and closed, and the female subject had 5 minutes of rest after each measurement. The subject was dressed in comfortable sportswear, stood freely in an upright position, with her hands holding a device in her mouth used to assess the tension force between maxilla and mandibular tension. Of course, this measurement is an indirect one. The authors base it on the fascial connections present in the human body and the tensegrity theory (Figure 1). Evaluation of the maxillary-mandibular clamping force, diaphragm muscle and feet (own source).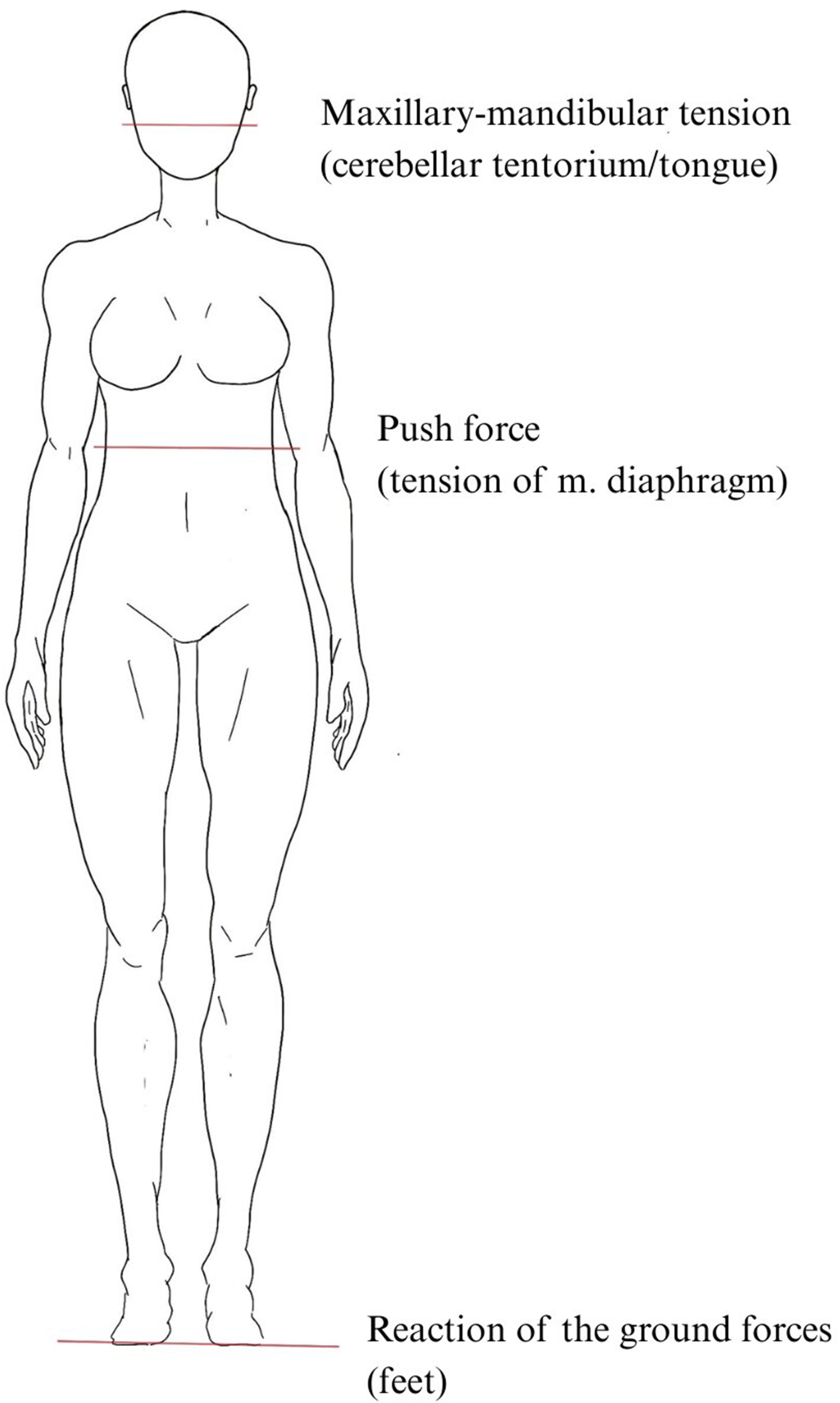
Evaluation of the maxillary-mandibular clamping force, diaphragm muscle and feet (Figure 1)
The level of tension between the maxillary-mandibular bones corresponds to the anatomical position of the tentorium cerebelli and tongue. 9 The authors designed a dedicated measuring device to check the clamping force between the maxillary-mandibular bones (patent W.132167). The design consists of two parallel beams, between which strain gauges were placed to record their deformation under clamping force. The signal from the strain gauges was then transmitted to a force meter, which presented the result in units of mass (kilograms). 18 The readout result was entered into an Excel spreadsheet (Figure 1).
Assessment of diaphragm muscle tension - push force (Figure 1)
The measurement of diaphragm muscle tension should correspond to the push force. As it was not possible to check the thrust force for the entire abdominal compression, only measurement of the diaphragm muscle tension was adopted. To verify this measurement, a device consisting of a belt to which a force gauge was attached was used. The belt was fixed on the test person at the height of the lower ribs, corresponding to the level of the diaphragm. 19 The study used a Conductive Elastomeric Extensometer (US3820529A). The force meter recorded the force value, presenting the result in units of mass (kilograms) 20 (Figure 1).
The readout results were then entered into an Excel spreadsheet for further analysis.
Assessment of ground reaction forces - feet (Figure 1)
The Computerised Stability Platform CQStab2P-vUSB-1506 was used to assess ground (foot) reaction forces. The platform was manufactured by the Polish company Koordynacja. Anterior-posterior and medial-lateral swings were considered for statistical analysis. The results obtained were entered into an Excel file.
The measurements of the transverse diaphragm were performed by experienced physiotherapists with over ten years of professional experience, in a quiet and warm room.
Statistical analysis
The data were statistically analysed. As the normal distribution was not met for any data set, the Friedman Test for repeated data and the pairwise Wilcoxon rank sum test were used for multiple comparisons, i.e. a post-hoc test. These tests were applied to establish whether there was a significant statistical difference for the three diaphragms analysed simultaneously between the group of women with pelvic organ prolapse and the control group (healthy women). The pairwise Wilcoxon rank sum test was also applied to compare the three diaphragms stretched simultaneously between the group with pelvic organ prolapse and the control group, in order to see if these groups differed.
In order to compare between a group of women with pelvic organ prolapse and a group of healthy women (control group) of each diaphragm during simultaneous tension, the Permanova test was applied, which is a non-parametric test based on distances using permutation.
In the final stage of the analysis, multivariate principal component analysis (PCA) was used, and the results were presented as biplots.
The results were also presented in tabular and figure form. The R statistical package was used for this analysis. 21
Ethics statement
The study was carried out with the approval of the Bioethics Committee of Poznan University of Medical Sciences, no. 305/23, and was registered as Clinical Trial NCT05978414.
Results
Simultaneous diaphragm tension with eyes open in the experimental group of women with pelvic organ prolapse and a control group (P value adjustment method: Bonferroni); open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf), open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap), open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa), open eyes MAXILLA-MANDIBULA-diaphragm-feet (oeMMdf).
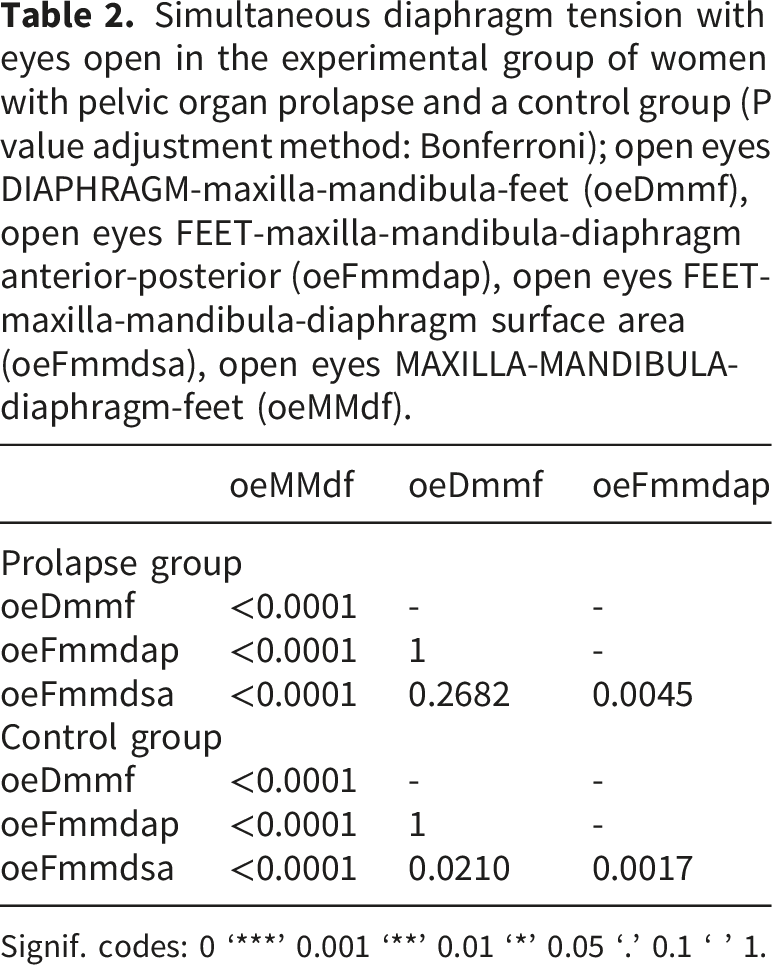
Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1.
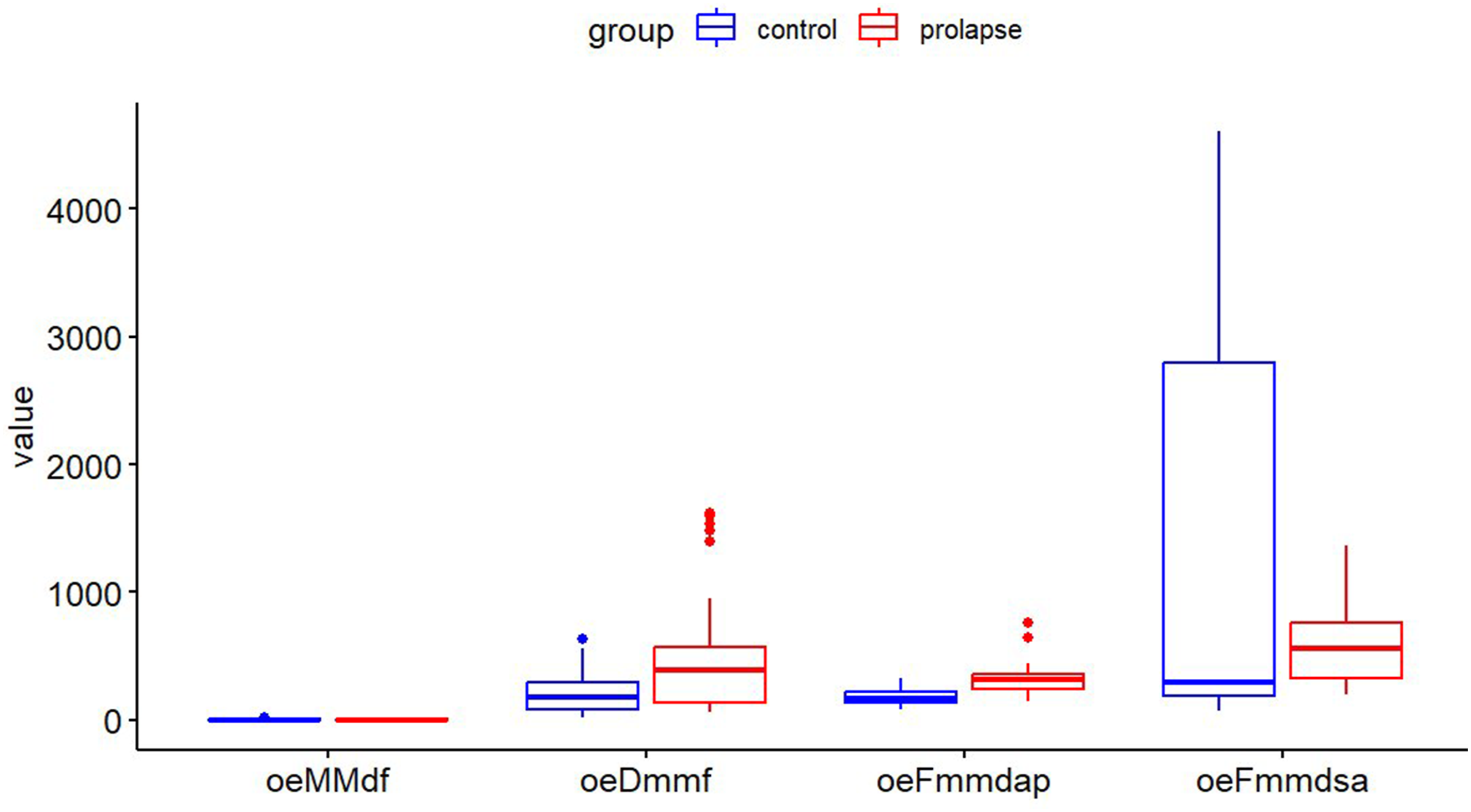
Simultaneous diaphragm tension with eyes open in the experimental group and control group; open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf), open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap), open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa), open eyes MAXILLA-MANDIBULA-diaphragm-feet (oeMMdf).
The results show that there is a very strong statistical relationship between the diaphragms. Bearing in mind the theory of tensegrity, this means that the tension of the diaphragms influences each other (Table 2, Figures 1 and 2): 1. with the diaphragm of the cerebellar sickle (clamping force between the maxillary-mandibular bones): open eyes MAXILLA-MANDIBULA-diaphragm-feet (oeMMdf) between: • diaphragm muscle (pushing force): open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf) p<0.0001 in the experimental and control groups, • foot diaphragm (ground force response in anterior-posterior tilt:) open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap) p<0.0001 in the prolapse and control groups, • foot diaphragm (ground force response for area): open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmds) p<0.0001 in the experimental and control groups, 2. foot diaphragm (ground force response in anterior-posterior pivot): open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap) between: • foot diaphragm (ground force response for area): open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa) p=0.0045.
The lack of a statistical relationship (Table 2, Figures 1 and 2) between diaphragm muscle (push force) means that, with tensegrity theory in mind, the tension in the three diaphragms does not affect each other: open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf) between: • foot diaphragm (ground force response in anterior-posterior tilt): open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap) p=1, • foot diaphragm (ground force response for area): open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa) p=0.2682.
In the control group, a highly significant relationship was also observed between the three diaphragms stretched (tested) simultaneously. The value obtained from the Freidman test performed is p-value<0.0001. The results obtained from the pairwise Wilcoxon rank sum test with continuity correction indicate the presence of a highly significant relationship between the following diaphragms, which means that, in view of the theory of tensegrity, the tension of the diaphragms influences each other between (Table 2, Figures 1 and 2): 1. diaphragm between the diaphragm muscle (push force): open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf) between: • foot diaphragm (ground force response for surface area): open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa) p=0.0210, 2. foot diaphragm (ground force response in anterior-posterior pivot): open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap) between: • foot diaphragm (ground force response for area): open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa) p=0.0017.
There is no statistical relationship (Table 2, Figures 1 and 2) between the diaphragm muscle diaphragm (push force) open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf) and the foot diaphragm (ground force response in anterior-posterior pivot:) open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap) p=1. Bearing in mind tensegrity theory, this means that diaphragm tension does not affect each other.
After performing the Friedman test for closed-eye data, a p-value<0.0001 was obtained in the experimental group, and a p-value<0.0001 was also obtained in the control group. This indicates a significant difference between the simultaneously stretched diaphragms in both study groups.
The results from the pairwise Wilcoxon rank sum test with continuity correction indicate that there is a highly significant relationship in the experimental group and the control group. Bearing in mind tensegrity theory, this means that diaphragm tension indicates a mutual influence between the following (Table 3, Figures 1 and 3): 1. with the diaphragm of the cerebellar sickle (maxilla-mandibula clamp force): eyes closed MAXILLA-MANDIBULA-diaphragm-feet (ecMMdf) between: • diaphragm muscle (pushing force): eyes closed DIAPHRAGM-maxilla-mandibula-feet (ecDmmf) for the experimental group p<0.0001 and for the control group p<0.0001, • foot diaphragm (ground force response in anterior-posterior tilt:) eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap) p<0.0001 in both study groups, • foot diaphragm (ground force response for area): eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa) p<0.0001 in both study groups, 2. diaphragm muscle (pushing force) between: • foot diaphragm (ground force response for area): eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa) p=0.0008 for the experimental group and p<0.0001 for the control group of women, 3. foot diaphragm (ground force response in anterior-posterior pivot:) eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap) between: • foot diaphragm (ground force response for area): eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa) p<0.0001 for the experimental group and p=0.0014 for the control group of women. Simultaneous diaphragm tension with eyes closed in the experimental group and control group (p-value adjustment method: Bonferroni); eyes closed DIAPHRAGM-maxilla-mandibula-feet (ecDmmf), eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap), eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa), eyes closed MAXILLA-MANDIBULA-diaphragm-feet (ecMMdf). Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1. Simultaneous diaphragm tension with eyes closed in the experimental and control groups; eyes closed DIAPHRAGM-maxilla-mandibula-feet (ecDmmf), eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap), eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa), eyes closed MAXILLA-MANDIBULA-diaphragm-feet (ecMMdf).
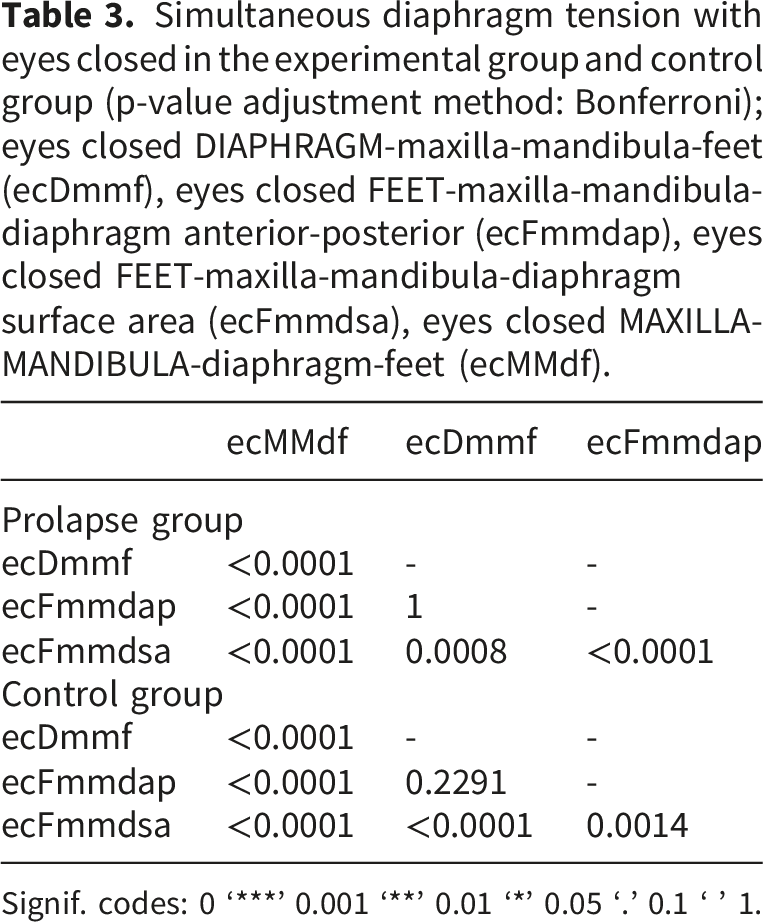
No statistical relationship was observed in the two study groups between the diaphragm muscle (push force) eyes closed DIAPHRAGM-maxilla-mandibula-feet (ecDmmf) and foot diaphragm (ground force response in anterior-posterior pivot:) eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap) in the experimental group p=1 and in the control group p=0.2291 (Table 3, Figures 1 and 3). This means that, bearing in mind tensegrity theory, diaphragm tension does not exert a mutual influence on these diaphragms.
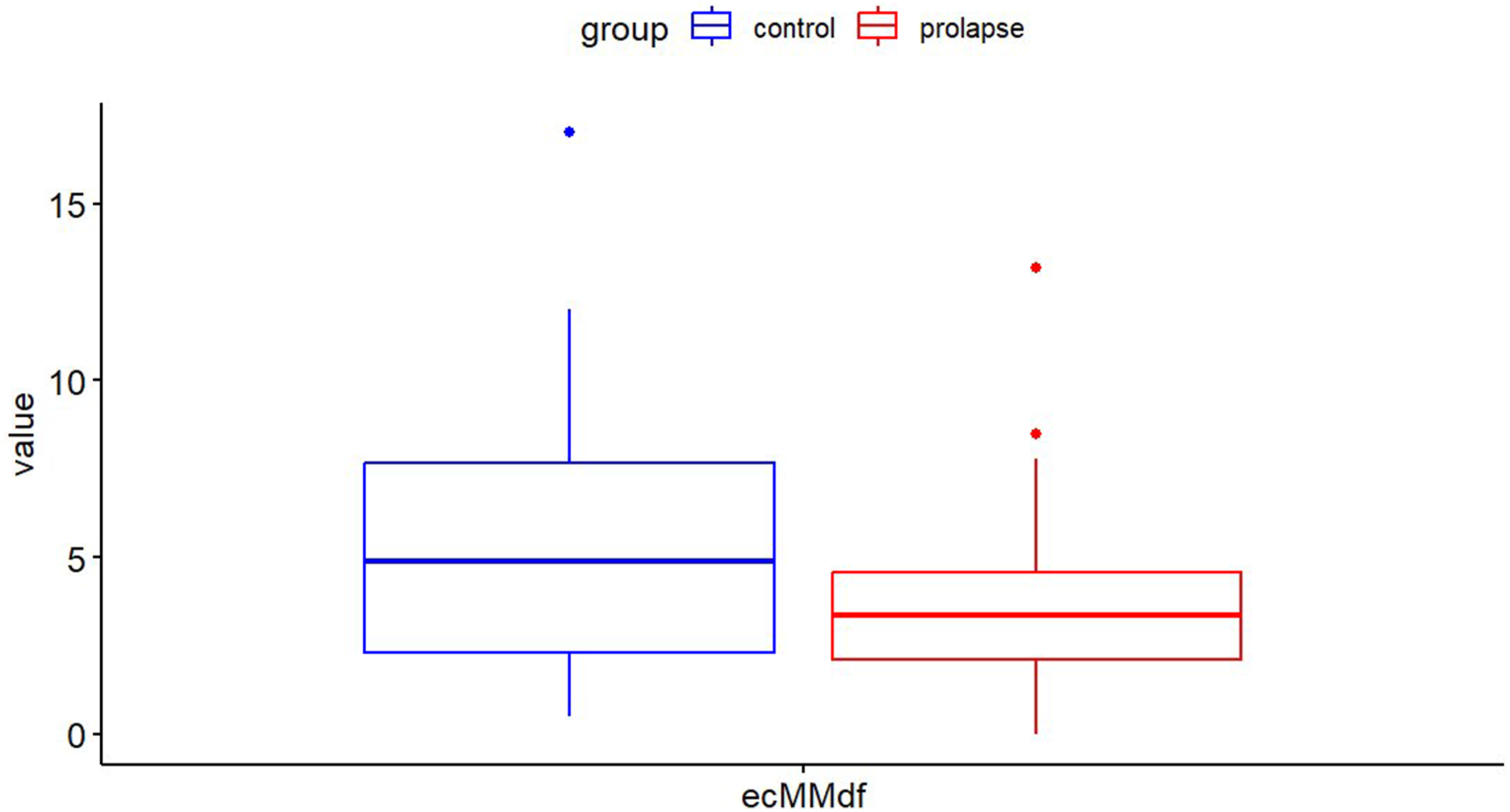
As the values for the tentorium cerebelli/tongue (maxilla-mandibula clamp force) were similar in both groups experimental and controls with eyes open and eyes closed (Figures 1 and 3), it was decided to test whether the study groups differed statistically significantly. For this purpose, the pairwise Wilcoxon rank sum test was used. For the open eyes test, a p-value=0.486 was obtained (Figures 1 and 4), indicating that the study groups did not differ significantly from each other. This indicates that the strength of tension in both groups was similar. Moreover, for the measurement with eyes closed, a p-value=0.0929 was obtained (Figures 1 and 5), indicating that the groups also did not differ. Cerebellar tentorium/tongue diaphragm tension (clamping force between the maxilla-mandibula) with simultaneous tension of three diaphragms with eyes open in the experimental and control groups; open eyes MAXILLA-MANDIBULA-diaphragm-feet (oeMMdf). Tension in the cerebellar tentorium/tongue diaphragm (clamping force between the maxillomandibular bones) with simultaneous tension of the three diaphragms with eyes closed in the experimental and control groups; eyes closed MAXILLA-MANDIBULA-diaphragm-feet (ecMMdf).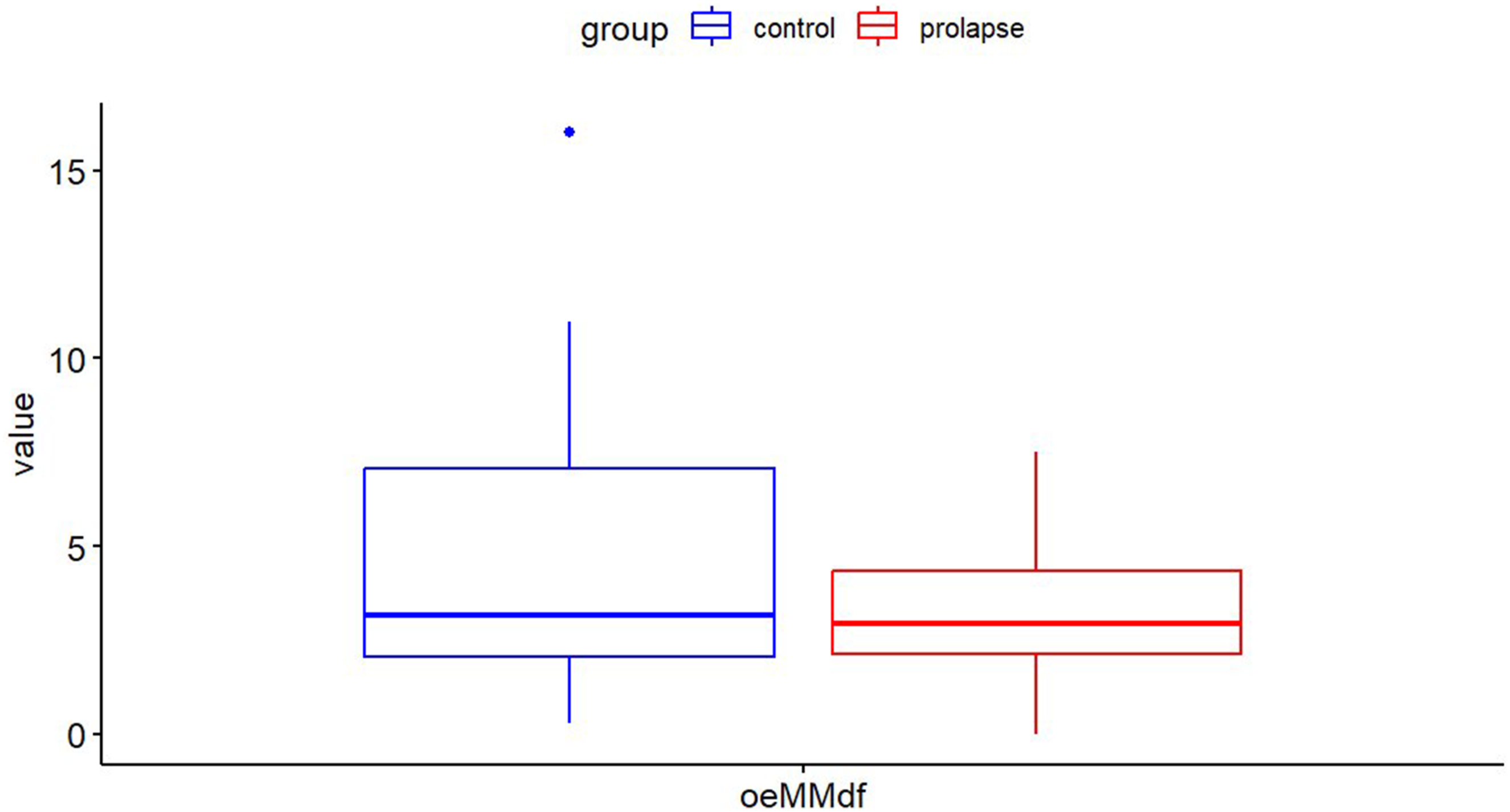
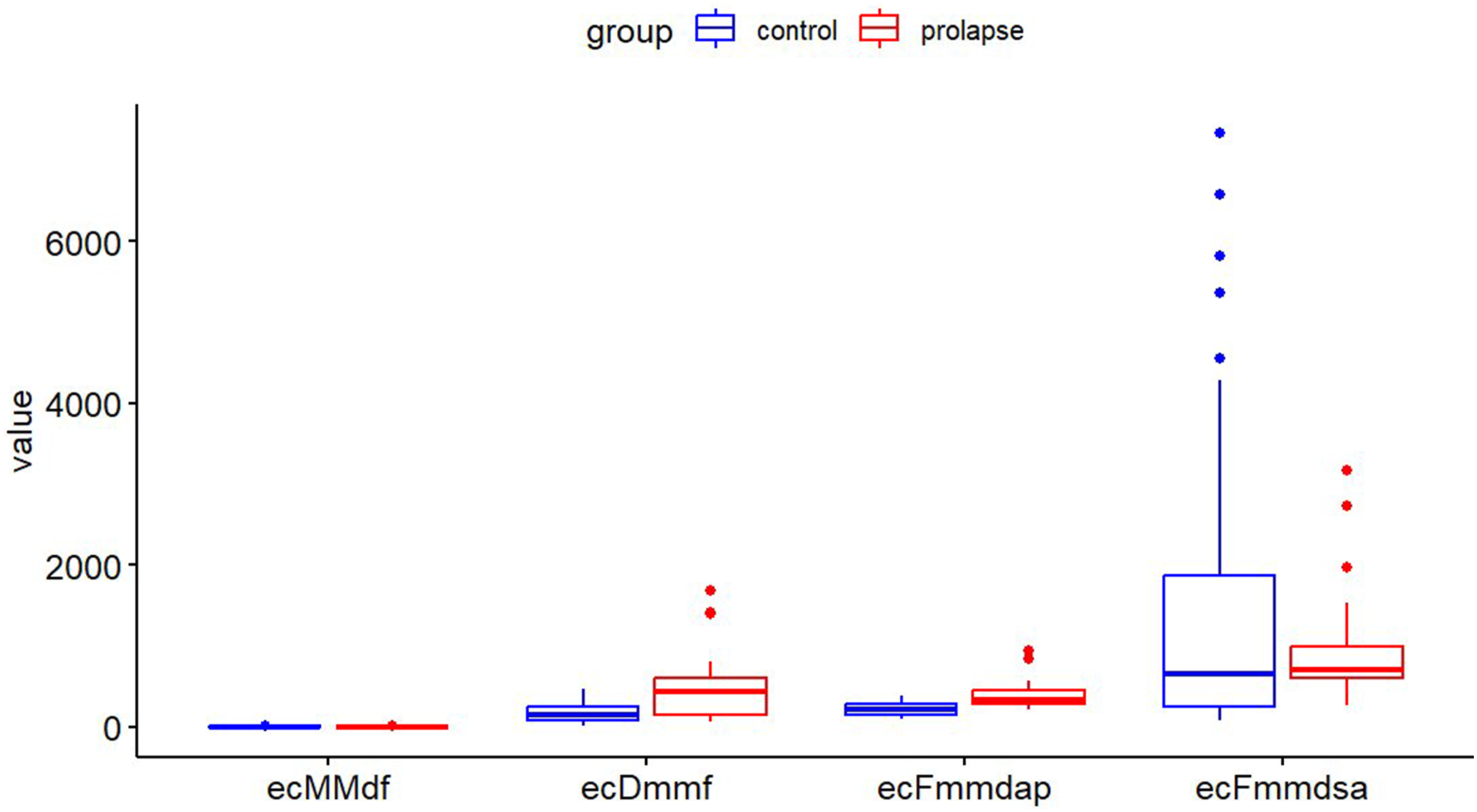
Comparison of diaphragm tension between the experimental group and the control group with eyes open and closed; experimental open eyes MAXILLA-MANDIBULA-diaphragm-feet (E_oeMMdf) vs control open eyes MAXILLA-MANDIBULA-diaphragm-feet (C_oeMMdf), experimental open eyes DIAPHRAGM-maxilla-mandibula-feet (E_oeDmmf), vs control open eyes DIAPHRAGM-maxilla-mandibula-feet (C_oeDmmf), experimental open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (E_oeFmmdap) vs control open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (C_oeFmmdap), experimental open eyes FEET-maxilla-mandibula-diaphragm surface area (E_oeFmmdsa) vs control open eyes FEET-maxilla-mandibula-diaphragm surface area (C_oeFmmdsa), experimental eyes closed MAXILLA-MANDIBULA-diaphragm-feet (E_ecMMdf) vs control eyes closed MAXILLA-MANDIBULA-diaphragm-feet (C_ecMMdf), experimental eyes closed DIAPHRAGM-maxilla-mandibula-feet (E_ecDmmf) vs control eyes closed DIAPHRAGM-maxilla-mandibula-feet (C_ecDmmf), experimental eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (E_ecFmmdap) vs control eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (C_ecFmmdap), experimental eyes closed FEET-maxilla-mandibula-diaphragm surface area (E_ecFmmdsa) vs control eyes closed FEET-maxilla-mandibula-diaphragm surface area (C_ecFmmdsa).
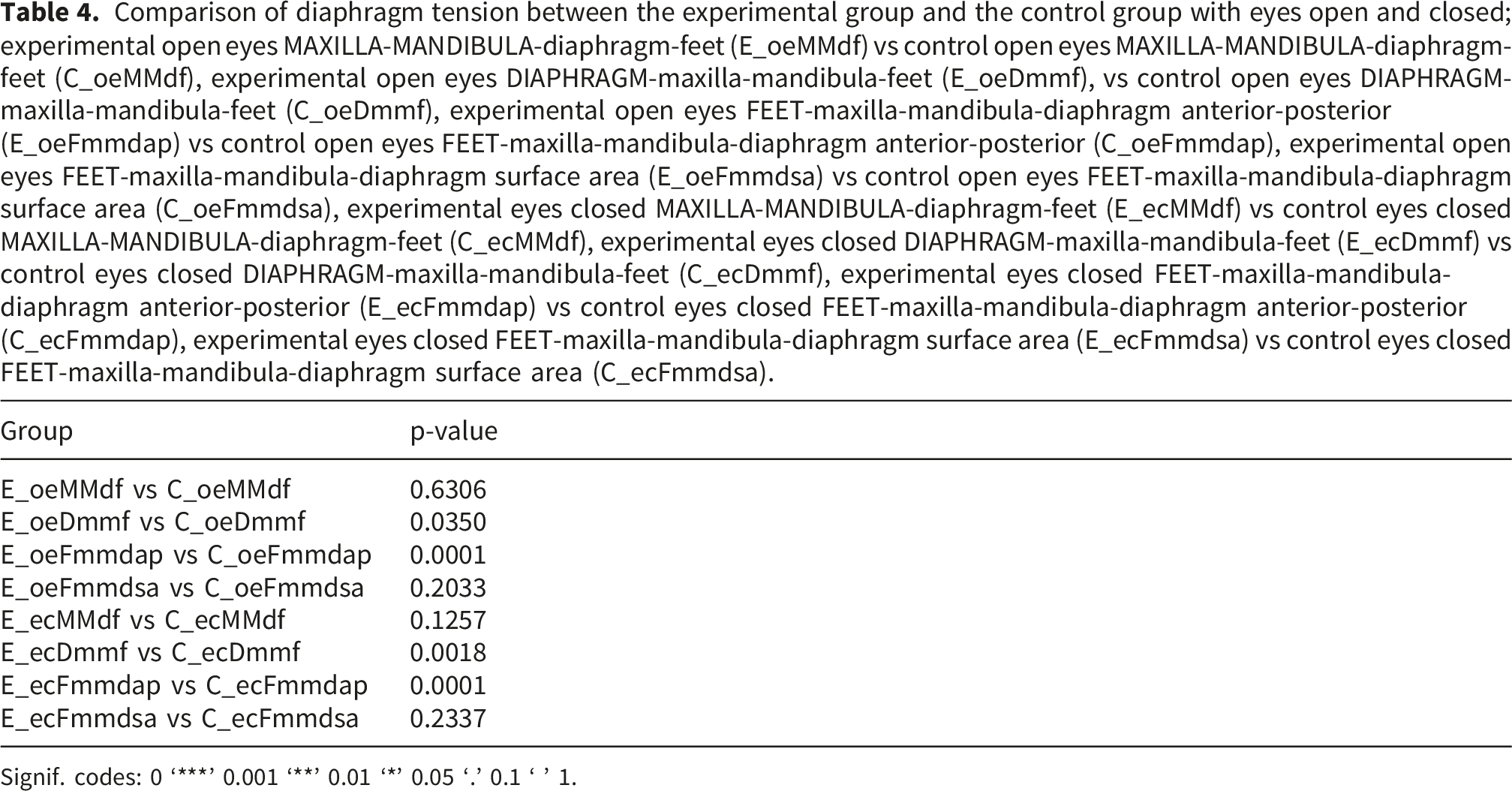
Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1.
Comparing the maxilla-mandibula diaphragm tension (Figure 1, Table 4) for the experimental open eyes MAXILLA-MANDIBULA-diaphragm-feet (E_oeMMdf) vs C_oeMMdf (control open eyes MAXILLA-MANDIBULA-diaphragm-feet) groups yielded a non-significant statistical result of p=0.6306, meaning that the diaphragm tension in both groups was similar.
When analysing the tension of another diaphragm, i.e. the diaphragm muscle (Figure 1, Table 4) for the experimental open eyes DIAPHRAGM-maxilla-mandibula-feet (E_oeDmmf, vs. control open eyes DIAPHRAGM-maxilla-mandibula-feet (C_oeDmmf) groups, a significant statistical value of p=0.0350 was obtained, indicating that the tension of this diaphragm, i.e. the diaphragm muscle, differed between the two study groups. Moreover, a significantly statistical value of p< 0.0001 was obtained for the foot diaphragm (Figure 1, Table 4) in anteroposterior tilt in both study groups experimental open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (E_oeFmmdap) vs control open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (C_oeFmmdap). The value obtained indicates that the groups differed in the tension of the diaphragm muscle. For the diaphragm of the feet (Figure 1, Table 4) for the area in both study groups experimental open eyes FEET-maxilla-mandibula-diaphragm surface area (E_oeFmmdsa) vs control open eyes FEET-maxilla-mandibula-diaphragm surface area (C_oeFmmdsa) a statistically insignificant value of p=0.2033 was obtained, i.e. diaphragm tension was similar in both groups of women.
The analysis then proceeded with eyes closed. The maxilla-mandibula diaphragm tension (Figure 1, Table 4) for the groups E_ecMMdf experimental eyes closed MAXILLA-MANDIBULA-diaphragm-feet (E_ecMMdf) vs control eyes closed MAXILLA-MANDIBULA-diaphragm-feet (C_ecMMdf) is similar at p=0.1257. Diaphragm muscle tension (Figure 1, Table 4) in both study groups experimental eyes closed DIAPHRAGM-maxilla-mandibula-feet (E_ecDmmf) vs control eyes closed DIAPHRAGM-maxilla-mandibula-feet (C_ecDmmf) was significantly different p=0018. Moreover, foot diaphragm tension in the anteroposterior pivot (Figure 1, Table 4) in both groups of women experimental eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (E_ecFmmdap) vs control eyes closed FEET-maxilla-mandibula-diaphragm anterior-posterior (C_ecFmmdap) was significantly different p< 0.0001, indicating that the women’s study groups differed in diaphragm tension. However, the diaphragm tension of the feet (Figure 1, Table 4) for the area in both study groups of women experimental eyes closed FEET-maxilla-mandibula-diaphragm surface area (E_ecFmmdsa) vs control eyes closed FEET-maxilla-mandibula-diaphragm surface area (C_ecFmmdsa)did not differ p=0.2337.
The final stage of the analysis took a holistic view of the problem by simultaneously analysing all the diaphragms studied in the experimental and control groups with eyes open and then in the group with eyes closed (Figures 6 and 7). Simultaneous analysis of diaphragms in the experimental group and the control group with eyes open; open eyes DIAPHRAGM-maxilla-mandibula-feet (oeDmmf), open eyes FEET-maxilla-mandibula-diaphragm anterior-posterior (oeFmmdap), open eyes FEET-maxilla-mandibula-diaphragm surface area (oeFmmdsa), open eyes MAXILLA-MANDIBULA-diaphragm-feet (oeMMdf). Simultaneous analysis of diaphragms in the experimental group and a control group with eyes closed; eyes closed DIAPHRAGM-maxilla-mandibula-feet (ecDmmf), eyes closed FE-ET-maxilla-mandibula-diaphragm anterior-posterior (ecFmmdap), eyes closed FEET-maxilla-mandibula-diaphragm surface area (ecFmmdsa), eyes closed MAXILLA-MANDIBULA-diaphragm-feet (ecMMdf).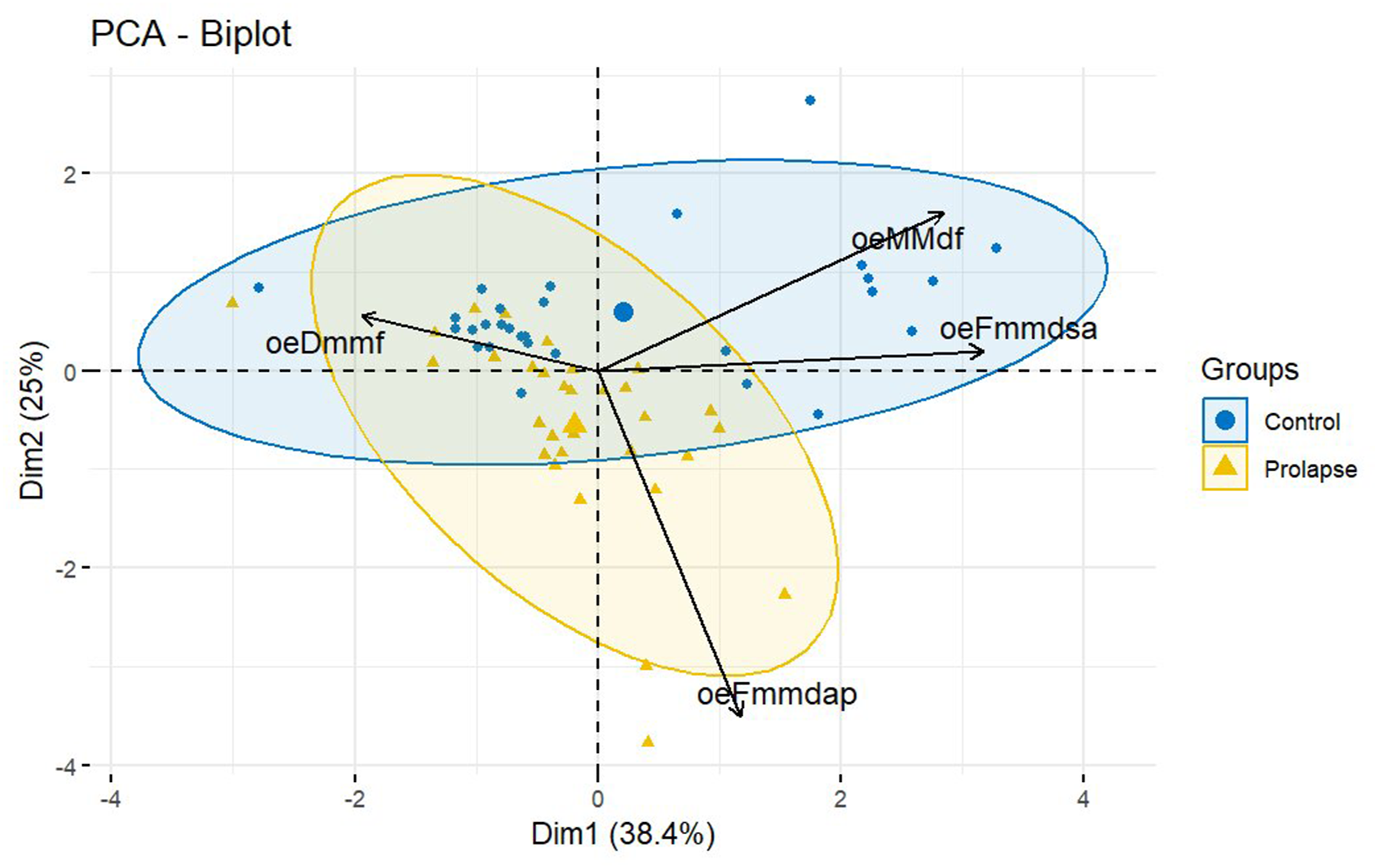
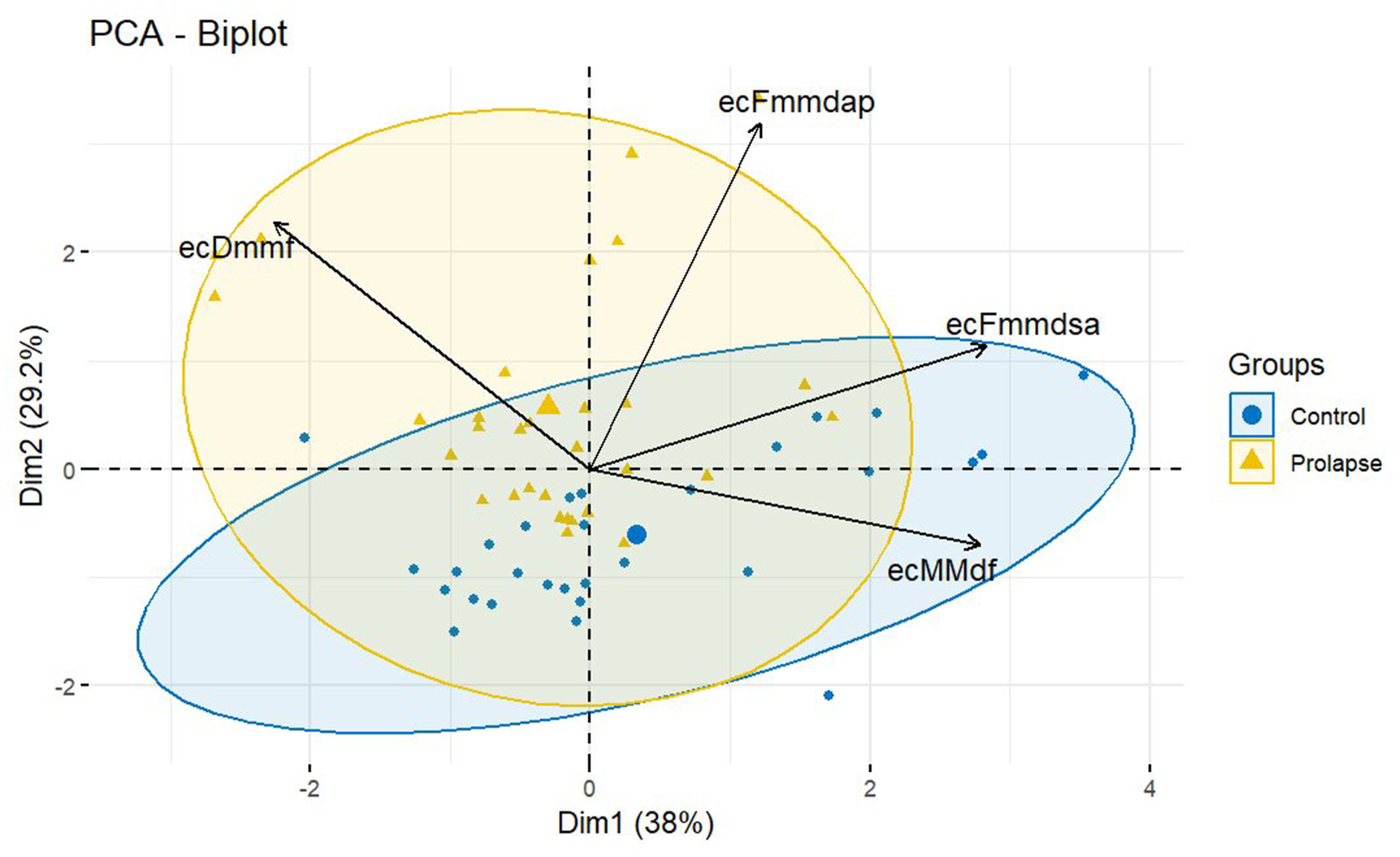
The results of the diaphragm observations (circles and triangles) and their vectors indicate that the experimental group differs in terms of the simultaneous tension of the three diaphragms compared to the control group of healthy women control group with eyes open and closed (Figures 6 and 7).
Discussion
The tensegrity theory conceptualizes the human body as a continuous tension network in which forces are distributed throughout interconnected structures. According to this framework, changes or dysfunctions in one region can influence distant regions via myofascial connections. In the context of POP, increased or altered tension in the pelvic floor may propagate along the transverse myofascial system, affecting postural control, diaphragmatic function, and craniofacial structures. The present study investigated tension in transverse structures in women with pelvic organ prolapse (POP) compared with healthy controls. Our findings provide novel insights into the functional integration of the maxilla–mandible system, respiratory diaphragm, and feet, supporting the concept that pelvic floor dysfunction is associated with alterations in global myofascial tension.
Our results demonstrate that women with POP exhibit significant differences in transverse structure tension compared with healthy controls, particularly under altered visual conditions (eyes closed), suggesting that visual input may modulate postural adaptations in the presence of pelvic floor dysfunction. These findings support the hypothesis that POP is not only a localized pelvic pathology but also involves systemic changes in myofascial tension, consistent with the tensegrity model.
The results of our study show that assessing the simultaneous tension of the diaphragms in the body (sickle of the cerebellum/tongue - measuring the tightening between the maxilla-mandibula bones, diaphragm muscle - measuring the push-up force and foot - measuring the ground force response) with eyes open and closed has a significant impact on their tension, which, in turn, is possibly a contributory factor to pelvic organ prolapse (POP). To date, studies on pelvic organ prolapse refer only to the pelvic region. 22
The human body can be regarded as a tensegrity structure because its stability depends on the balance between muscle tension and the resistance provided by rigid bones. The influence of mechanical forces on the control of cell shape and function began to be observed in the late 1970s. 2 Changes in the mechanical properties of tissues are often the reason a patient seeks medical attention. Many disorders are considered “mechanobiological diseases,” and they share a common etiology or clinical presentation resulting from alterations in cell mechanics, changes in extracellular matrix (ECM) structure, or dysregulation of cellular mechanotransduction. 2
According to the theory of tensegrity, when tension in the tissue becomes excessive, a damaging stimulus arises, which then spreads linearly throughout the body. As a result, symptoms may appear at a location distant from the site of the stimulus. According to Still, fascia represents a place in the human body where the causes of diseases can be found, and its proper functioning ensures life, whereas its dysfunction leads to the death of the organism. 3
Anatomical structures are closely interconnected through vascularisation, innervation and fascial continuity.4,5 The current definition of the fascial system is that its components are the superficial fascia, musculo-scelatel (deep) fascia, visceral facia and neural fascia, which have connections with anatomical structures. 5 The fascial system is a layer encompassing the entire body that is subjected to mechanical loads resulting from the mobility of the human body. 5 Previous ultrasound studies have shown that during oscillatory movements, such as walking, the fascia often serves as a reservoir of mechanical energy. 3
Using the term diaphragm is a convention. Zink assessed four diaphragms, i.e. the position of the respiratory diaphragm, the thoracic outlet or high thoracic diaphragm, the pelvic floor or pelvic diaphragm, and the tentorium of the cerebellum or cerebellar diaphragm. 23 The assessment consisted of the operator performing rotational movements and observing whether there were restrictions in mobility. 23 Bordoni et al. point out that the fifth diaphragm may be the tongue. 24 Manual treatment of diaphragmatic tension disorders is currently being discussed, 24 and may also be relevant for treating women with POP.
The cerebellar tentorium is a bifurcation of the dura mater and separates the brain from the cerebellum 9 and provides a support for the occipital lobes, splitting and encompassing the scalene part of the temporal bone and the scala of the occipital bone and part of the parietal bone. 9 The innervation in the supra-occipital part is provided by the optic branch of the trigeminal nerve and the nervus tentoria. 9 In contrast, the subepithelial part is innervated by spinal nerves from the C1-C3 level through the vagus and sublingual nerves. 9 The suboccipital are connected to the dura by a myodural bridge in the proximity of the foramen magnum, through vertebral dural ligaments.25–29 The myodural bridge has proprioceptive receptors and can transmit strong traction to the dura mater during head movements. 29 Connected to the dura are the ligamentum nuchae near the nuchal region 30 and the ligaments of Hoffman attaching to the deep layer of the posterior longitudinal ligament. 31 These anatomical relationships should allow adequate pressure for CSF mobility and prevent overstretching of the spinal nerves and prevent pain. 31 The yellow ligament located behind the meningeal sac exhibits strong meningeal connections 32 and its functional disruption can cause cervical pain syndromes. 33
The thoracic aperture or upper thoracic diaphragm is characterized by musculo-fascial continuity with the cerebellar tentorium and lingual complex through the quadriceps and cervical muscles - constituting the thoracolumbar fascia system. 34 In turn, the fascia that covers the lower diaphragm (fascia transversalis) connects viscerally through connective tissue or ligaments. Glisson’s pouch surrounds a large portion of the diaphragm muscle, as well as the diaphragmatic-gastric ligament, the diaphragmatic-circumferential ligaments and the hepatic ligaments. 24 There is also a connection between the fascia transversalis and the epimysium of the iliac and quadratus lumborum muscles, as well as the thoracolumbar muscle-fascia complex. 35 The fascia transversalis covers the pelvic viscera, transforming into the mediastinal fascia, which is divided into the mural and visceral fascia. 35 The intramedullary fascia covers the muscles that make up the pelvic floor, connecting to the fascia prevertebralis and the periosteum of the pubic bone. 36
In the pelvic fascia, there is the Denonvilliers fascia, which is located in men between the anus and seminal vesicles, and in women between the anus and vagina. The area also includes the rectovaginal fascia, the Walderer’s fascia, which is located between the posterior rectum and the preanal fascia or rectovaginal fascia. 37 The transverse fascia connects to Toldt’s fascia, which covers the abdominal and pelvic organs, and then connects to the mediastinal fascia, and Fredet’s fascia, covering the visceral peritoneum of the pancreas and ascending mesentery of the colon. 38 The fascial system has connections with the visceral ligaments. 39 The connection between the thoracolumbar diaphragm, which has a connection with the muscular part of the respiratory diaphragm is through the muscles: lumbosacral, biceps femoris, tubercle, gluteus maximus, multifidus, thoracic longest, lumbar iliac ribs, and dorsal extensor.39–41 Fascial tension does not depend solely on muscle tension. This is due to the presence of autonomic nerve fibers, which regulate the baseline tension of the fascia by utilizing the contractility of smooth (non-striated) muscles. 3
In our study, the pelvic floor diaphragm was not assessed, as measurements were conducted in the standing position, whereas previous POP-Q scale was typically performed supine15,16 Instead, the feet were considered as one of the diaphragms and simultaneously the first part of our body that come into contact with the ground and are often presented in scientific studies in gait analysis or balance (postural stability) assessment.42–45 Maintaining body weight relies on the feet. They are also the endpoints of muscle chains, whose role - according to the theory of tensegrity - is to transfer loads to higher anatomical structures, which may lead to disturbances in proper body posture. 46
It has also been proven that stress can affect the expression of myofascial pain. 3 POP can be regarded as a kind of stress for women. 47
Physiotherapeutic management depends on the POP-Q scale value. If women have been classified in the POP-Q 1-2 scale assessment, the most common treatment is to perform exercises to strengthen the muscles of the lower pelvic floor, i.e. pelvic floor muscle training (PFMT).15,16,48 Although other forms of physical activity such as yoga and tai-chi are also applied with no clear consensus on the most effecitve protocol. 48 More advanced stages of POP (POP-Q score of 3-5) generally require a surgical treatment.15,16 The issue of postural stability in women has been also well studied previously in cases of urinary incontinence, breast cancer, mastectomy, and osteoporosis49–52 In women with POP, stress urinary incontinence often co-occurs. Both conditions contribute to reduced sexual satisfaction and quality of life. 53
This also translates into avoidance of physical activity by women who have POP combined with stress urinary incontinence. 54 Therefore our study regarding diaphragmatic tension in the body may point a good direction of the therapy in women with POP who have been qualified for physiotherapy. Application of the fascial system therapy provides a holistic approach to the body where the structures remain in relation to each other in tension and the fascial therapy is the most common and effectively used protocol in case of muscular etiology pain. 55
There is a need to develop physiotherapeutic management algorithms for women with POP, as most existing protocols focus primarily on strengthening the pelvic floor muscles.56–58 Despite the increasingly common use of surgical treatment with robotic assistance,59,60 it should be remembered that scars remain in the soft tissue, which also require urogynecological physiotherapy. 61 An excellent complement to the treatment of women may be supplementation with vitamins and nutraceuticals. 62 The treatment of women with pelvic organ prolapse requires an interdisciplinary approach and collaboration among multiple specialists.
Limitations
A limitation of our study is the small group of women who were in our research. Because we assumed that the measurements would be taken in a standing position that is, the position in which women spend most of their time during the day we were unable to assess pelvic floor muscle contraction strength, which is evaluated in a lying position. We related our study to the theory of tensegrity and fascia. Finally, while our measurements provide functional insights, they do not directly quantify tissue properties such as stiffness or elasticity. Since our study consists of preliminary observations, we did not perform a power analysis. Due to limitations related to the sample size, a power analysis was not conducted.
Conclusion
The results obtained from the preliminary observation suggest that assessing the transverse diaphragm tension strength in women with pelvic organ prolapse may serve as a tool to indicate the risk of pelvic organ prolapse in women. Women with POP demonstrate altered tension in transverse structures, supporting the concept of systemic myofascial adaptations consistent with tensegrity theory. These findings emphasize the importance of a holistic, multi-level approach in both assessment and physiotherapy of pelvic floor disorders. Due to the lack of similar studies, it is difficult for us to compare our results with those of other researchers.
Recommendations
Apart from the examination by a gynecologist, who determines the degree of pelvic organ prolapse, the measurement of the transverse diaphragms in a woman’s body should also be taken into account.
Clinical implications
Our findings have several important clinical implications: Holistic assessment: Clinicians should consider postural and myofascial evaluations (transverse structures) as part of the standard assessment for women with POP. Physiotherapist strategies: Considering the myofascial chains present in the human body, physiotherapeutic treatment should include not only work with the pelvic floor muscles but also with the transverse diaphragms. Vision-dependent adaptations: The modulation of tension under eyes-open vs eyes-closed conditions suggests that sensory input plays a role in postural compensation, which may be relevant for physiotherapy.
Footnotes
Acknowledgements
We would like to thank the participants of our research for taking the time to participate.
Ethical considerations
We obtained ethical approval for the study from the Bioethics Committee of Poznan University of Medical Sciences, no. 305/23, and was registered as Clinical Trial NCT05978414.
Consent to participate
We obtained written informed consent from the participants after explaining the purpose of the study and the ethical considerations guiding it.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Rehabilitation procedures in patients after neurosurgical interventions Ministry of Education of the Slovak Republic (project No KEGA 005KU-4/2024).
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.