
Abstract
Background:
Continuous educational programs based on the PRECEDE-PROCEED model are recommended for women with gestational diabetes to improve their knowledge and awareness of the condition. These programs should address individual, organizational, and healthcare-related factors.
Objectives:
This research aimed to evaluate the effect of a nursing approach based on the PRECEDE-PROCEED model on health behaviors and sleep quality among women with gestational diabetes.
Design:
This study is a quasi-experimental research (pre-posttest design for control and study groups).
Methods:
This study includes a purposive sample of 90 pregnant women. This study was carried out in obstetrics and gynecology outpatient clinic at Al-Basheer hospital in Jordan. Data were collected through face-to-face interviews using a structured questionnaire, the questionnaire incorporated constructs from the PRECEDE-PROCEED model, along with the health-promoting lifestyle profile-II and Pittsburgh sleep quality index.
Results:
Following the intervention, participants in the study group achieved higher overall health-promoting lifestyle scores than those in the control group. The mean score in the intervention group was 97.02 ± 15.27, compared with 77.71 ± 11.55 in the control group, indicating a statistically significant difference. Significant improvements were also observed in key lifestyle domains, including nutrition (28.04 ± 5.52), physical activity (17.08 ± 3.34), and stress management (18.46 ± 2.69). In addition, sleep quality improved in the intervention group, as reflected by a reduction in the mean sleep disturbance score to 8.20 ± 2.65 compared with 11.24 ± 5.32 in the control group.
Conclusion:
The PRECEDE-PROCEED model was effective in improving knowledge, attitude, sleep quality, and health behaviors among pregnant women diagnosed with gestational diabetes.
Introduction
Gestational diabetes mellitus (GDM) is a broadly distributed metabolic disorder that occurs during pregnancy and is marked by disrupted glucose regulation identified at this time. In the majority of instances blood glucose levels normalize after childbirth. GDM can arise at any point in time during pregnancy, but it is commonly identified during the second and third trimesters because of heightened insulin resistance. This condition is associated with significant maternal and neonatal issues and contributes to higher mortality worldwide. 1
The global incidence of GDM has increased overtime, a trend attributed primarily to advanced maternal age, overweight, physical inactivity, diagnosed with prediabetes, who previously experienced gestational diabetes, with a hormone disorder known as polycystic ovary syndrome, a previous macrocosmic child, and a positive family history of type 2 diabetes mellitus. 2 GDM is correlated with unfavorable pregnancy outcomes such as, high blood pressure and preeclampsia, higher risk of getting type 2 diabetes, high birth weight, premature labor that elevates the likelihood of a premature delivery, and cesarean birth or birthing trauma caused by excessive fetal weight. Uncontrolled gestational diabetes could contribute to stillbirth or early neonatal death.
One of the most prevalent medical conditions that make pregnancy more difficult in the 21st century is GDM, with reported incidence rates varying between 1.4 % and 18.5% across various nations, its prevalence has increased globally in recent years. 3 The prevalence of diabetes varies significantly by regions, according to reports from, with rates ranging from as low as 2% to more than 30%. Research worldwide points to a consistent increase in GDM cases. The world health organization estimates that globally, and approximately one in six pregnant women experiences hyperglycemia, based on its diagnostic criteria. 4
In Jordan, there are discrepancies in reported GDM rates. According to WHO criteria, a hospital-based investigation performed at Jordan University Hospital during the years 2015 and 2016 found that GDM was identified in 13.5% of pregnant women tested. 5 On the other hand, a comprehensive assessment and combined evaluation of studies carried out across the Middle East and North African region indicated that the general occurrence rate of GDM in Jordan is roughly 4.7%. 6 This variation is likely due to the different approaches taken in research, the kinds of diagnostic techniques employed, the evaluation methods used, and the unique characteristics of individuals, such as their background and health condition. In summary, the research emphasizes the growing health issue that GDM poses for the population of Jordan, despite the discrepancies in the data offered.
The lack of enough insulin made by the body when someone is pregnant leads to gestational diabetes. Insulin is released by the pancreas and helps control blood sugar by allowing cells to take in and use it for energy. During pregnancy, the body experiences various changes, such as producing more hormones and gaining weight. Due to these changes in the body, insulin resistance happens, meaning insulin is less effective at helping cells take in glucose. This insulin resistance creates a higher demand for insulin to keep blood sugar levels normal. 7
Choosing a healthy lifestyle is crucial for controlling GDM. A key aspect of controlling GDM involves altering one’s behaviors, particularly by enhancing dietary choices and engaging in consistent physical activity. While dietary habits are the main factor influencing blood sugar levels, other elements such as exercise, stress management, health responsibilities, social connections, and personal development are also important for maintaining blood sugar stability. 8 Given the variety of elements that play a role in GDM, making significant alterations to everyday routines related to these elements has been shown to positively impact the health of both mothers and their babies.
People dedicate roughly one-third of their existence to sleeping, which is crucial for their well-being and aids in both mental and physical abilities. Sufficient sleep greatly enhances life quality by encouraging mental wellness and reducing the risk of various health issues. Issues with sleep are strongly connected to how the body manages glucose and increase health dangers for both mothers and babies in pregnancies affected by diabetes. 9
Given the various elements that lead to GDM, comprehensive health promotion approaches are essential to combine lifestyle, behavior changes, and educational efforts. The ΡRECEDE-ΡR0CEED model, created by Green 10 in 1974, provides a structured way to assess the costs and benefits of programs, aiding planners and evaluators in identifying the best strategies to enhance health. It acts as a broad guideline for understanding people’s quality of life requirements while assisting in the planning, execution, and assessment of health promotion initiatives and public methods to address those needs. 11 This framework is essential in countries such as Jordan where healthcare services emphasize prevention and community-focused approaches to reduce the impact of chronic diseases.
Nurses are very important in handling GDM well because they teach pregnant women and get them to take part in looking after themselves. Nurses also assist women in managing the difficulties of gestational diabetes and enhancing their general health. Treatment options consist of cognitive-behavioral therapy, sex therapy, mindfulness and relaxation strategies, psycho-education, and couples counseling. Modifying one’s lifestyle is the best form of treatment. Treatment usually starts with medical nutrition therapy, exercise, and managing weight. Women experience more favorable results when they can control their diet (restricting carbohydrates and total calories), engage in consistent exercise (for at least 150 min per week), and monitor their glucose levels independently. 12 Given the significant role of nurses in Jordanian healthcare settings, empowering them with effective educational tools is vital to improve outcomes in women with GDM.
Significance of the research
Approximately 14% of pregnancies around the world are influenced by gestational diabetes; its recurrence changes depending on hazard components and screening and determination methods, and it is increasing at the same time as type 2 diabetes and weight. 13 Out of the 21,909 women who gave birth in the chosen hospitals, 1.2% of the women received a diagnosis of GDM. The incidence (3.5%) was significantly higher in women over 35 years of age compared to women under 20 years (0.4%) and women between 20 and 35 years (0.9%). The incidence did not vary across the three health sector regions and the regions of the country. The incidence was also significantly higher in women who were obese (3.4%) compared to both normal and overweight women (0.6%). 14
The fact that GDM has minimal symptoms and that a pregnant woman is typically unaware that she has it until it is identified during a normal prenatal screening is one of the main issues with the condition. Though almost symptomless, GDM is linked to serious pregnancy complications, such as respiratory distress syndrome, shoulder dystocia, macrocosmic, fetal death in the womb, hyperbilirubinemia, hypoglycemia, cardiomyopathy, and perinatal mortality due to unknown abnormalities. Furthermore, a mother may experience several symptoms like hypertension, an early birth, infection-related issues, pre-eclampsia, and an increased risk of type 2 diabetes during the postpartum period. 15
The quality of one’s sleep is a crucial sign of one’s overall quality of life, which influences one’s mental well-being and is intimately linked to the onset of numerous illnesses. Pregnancy-related sleep disturbances linked to diabetes pose a serious risk to the health of both moms and unborn children, and these risks are closely correlated with blood glucose levels. 16 Therefore, this study will be conducted.
Aim of the research
This research aimed to evaluate the effect of a nursing approach based on the ΡRECEDE-ΡROCEED model on health behaviors and sleep quality among women with gestational diabetes.
Research hypotheses
Subject and methods
Research design
A quasi-experimental design was used to accomplish this research. A typical design for a quasi-experimental study includes evaluating one participant group both before and after an independent variable is manipulated or treated. The independent variable can be blamed for any noteworthy variations in the pretest and posttest results. 17 The reporting of this study conforms to the TREND statement. 18
Setting
The study was conducted as a single-center controlled trial at the obstetric and gynecological outpatient clinic of Al Basheer Hospital, Jordan.
Sampling
Sample type: A purposive sample was used.
Sample size
The sample size in this study was estimated based on the mean difference in diabetes self-care activities reported in a previous study by Al-Hashmi et al. (2018), in which a 0.6-point improvement was observed (M1 = 3.1, M2 = 3.7) with a standard deviation of 1.2. This difference was considered clinically meaningful and achievable through the intervention. Using G*Power software with a two-sided α = 0.05 and power = 90%, which was selected to ensure a high probability of detecting a true effect, the required sample size was computed to include 45 participants per group, resulting in a total sample of 90 women. Recruitment persisted until the target sample size was achieved. In the case that a person withdrew or was lost during the study, efforts were taken to find substitute volunteers who met the inclusion criteria in order to maintain the sample size.
Non-random assignments were made to the participants due to the quasi-experimental nature of the study and practical considerations for planning the intervention sessions. The study group consisted of the first 45 eligible women recruited and received an educational program based on the PRECEDE-PROCEED model in addition to regular hospital care, and the following 45 eligible women were included in the control group and received conventional hospital treatment alone. Both groups were matched as closely as possible in terms of age, gestational age, and other baseline characteristics to minimize potential bias (see Figure 1).

CONSORT flow diagram for data collection.
Inclusion criteria
– Women with gestational diabetes.
– Women aged 18 years and older (mothers under 20 were included because gestational diabetes can occur in younger pregnancies, and including them helps represent the real population).
– Women with a gestational age of 24–28 weeks.
– Devoid of any health or pregnancy-related complications.
– Women who can read and write.
Exclusion criteria
– Preexisting sleep disorders or diagnosed sleep apnea.
– Other chronic medical conditions that could affect pregnancy outcomes.
– Multiple pregnancies (e.g., twins or more).
– Adherence to specific dietary regimens unrelated to GDM management.
– Participation in any other clinical trial or educational program related to GDM or pregnancy during the study period.
Data collection tools and outcomes
Primary outcomes (post-intervention, 4 weeks after program completion):
Health-promoting behaviors: Total score on the Health-Promoting Lifestyle Profile II (HPLP-II; 41-item version used in this study; higher scores = better lifestyle).
Sleep quality: Pittsburgh Sleep Quality Index (PSQI) global score (0–21; lower = better sleep).
Secondary outcomes
HPLP-II subscale scores: Nutrition, physical activity, stress management, health responsibility, and interpersonal relations.
PSQI component scores: Subjective sleep quality, latency, duration, efficiency, disturbance, medication use, and daytime dysfunction.
ΡRECEDE-ΡROCEED determinants: Knowledge, attitude, enabling, and reinforcing factor scores.
Assessment timing
All measures were collected at baseline (pre-intervention) and at follow-up 4 weeks after the intervention.
Tool I: – A structured interviewing questionnaire
Researchers created it after studying associated research.19–21 It incorporated:
– Part 1: General characteristics of the studied women (age, level of education, occupation, and residence).
– Pre-pregnancy body mass index (BMI): Pre-pregnancy BMI was collected through participant self-report and calculated as weight in kilograms divided by the square of height in meters (kg/m²). It was included in the descriptive analysis as a baseline characteristic to allow for group comparisons at the start of the study.
– Part 2: Past medical history related to gestational diabetes, including family history of the disease.
– Part 3: Obstetric history such as gestational age, parity, gravida, and abortion.
Tool II: the PRECEDE-PROCEED model construct
The questions are crafted to identify Predisposing, Enabling, and Reinforcing factors.
1. Predisposing factors, which included 2 sections:
A. Section (I) knowledge assessment sheet: The assessment comprised 11 questions aimed at determining the level of knowledge among women about gestational diabetes such as meaning of GDM, women at high risk for developing GDM, causes, risk factors, symptoms, effects on newborn, effects on mother, diagnosis, trimester of developing GDM, treatment methods, and ways to prevent GDM.
Scoring system: For each item, the accurate response obtained a rating of 2, whereas the wrong answer obtained a rating of 1. The total knowledge score was determined by adding up the scores of the correct answers. Higher scores suggested a deeper comprehension of GDM. The overall knowledge score was divided into the following categories:
– Satisfactory knowledge: overall knowledge score ⩾ 60%
– Unsatisfactory knowledge: overall knowledge score < 60%
B. Section (II) Attitude assessment sheet: It contained 13 items designed to measure women’s attitudes about gestational diabetes.
Scoring system: The three points on the Likert-type scale on the attitude assessment sheet were marked as follows: “(1) Disagree, (2) Neutral, and (3) Agree.” The overall attitude score of women was classified into the following categories:
– Low attitude when the overall score was less than 60%.
– Moderate attitude when the total score was between 60% and 75%.
– High attitude when the overall score exceeded 75%.
2. Enabling factors: It contained six assessment questions about women’s social activities related to gestational diabetes, like searching for an educational program about gestational diabetes, possessing the knowledge and expertise to manage complications related to gestational diabetes, utilizing various resources to acquire knowledge regarding gestational diabetes, have enough time to work out or read about gestational diabetes, consume foods rich in the essential nutrients daily and possess simple access to medical facilities.
Scoring system: On the enabling factor sheet, there were three Likert-type scale points: (1) No, (2) Sometimes, and (3) Yes. The categories detailed below reflected the overall enabling factors score for women:
– Low social activities when the overall score was less than 60%.
– Moderate social activities when the total score was between 60% and 75%.
– High social activities when the overall score exceeded 75%.
3. Reinforcing factors: It contained five questions designed to gauge women’s encouragement and support of family, friends, and medical professionals concerning gestational diabetes, including husband represents support for you and ensure that you get through this phase safely, the surroundings aid in modifying unhealthy behaviors, receive encouragement from loved ones and friends when you say you want to change your way of life, get a prize from your family for leading a healthy lifestyle, and medical authorities support and encourage by emphasizing the value of routine checkups.
Scoring system: The three-point Likert-type scale on the reinforcing factor sheet was as follows: No (1), Sometimes (2), and Yes (3). The following divisions reflected the overall reinforcing factors score for women:
– Low support and encouragement when the overall scores were less than 60%.
– Moderate support and encouragement when the total scores were 60% to 75%.
– High support and encouragement when the overall score exceeded 75%.
Tool III: health-promoting lifestyle profile-II
It was adapted from Walker et al. (1995) to assess the health-promoting practices of pregnant women. There were 41 items total, with 5 subscales: nutrition (11 items), interpersonal relationships (7 items), physical activity (7 items), health responsibility (8 items), and stress management (8 items).
Scoring system: The original 4-point Likert scale was adapted to a 3-point scale (Never = 1, Sometimes = 2, and Always = 3) to simplify the response format and enhance clarity. The overall score for each dimension was calculated by averaging the responses to the items within that dimension. A total score was determined by averaging the responses to all 41 items and varied from 41 to 123, with higher scores showing greater adoption of health-promoting behaviors. The total lifestyle score of women was categorized as follows:
– Poor lifestyle behaviors, when the overall score was less than 60%.
– Moderate lifestyle behaviors, when the total score was 60% to 75%.
– High lifestyle behaviors, when the overall score exceeded 75%.
Tool (IV): PSQI
In order to gauge the quality and patterns of sleep over the previous month, the PSQI was adapted from Symith. 22 There were 19 statements in total. Seven domains linked to sleeping habits were identified by PSQI, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medication, and daytime dysfunction.
Scoring system: A total score ranging from 0 to 21 was created by adding the 7 component scores, which ranged from 0 (no difficulty) to 3 (severe difficulty). Poorer sleep quality is indicated by higher scores. Sleep quality was divided into four categories.
■ (PSQI ⩽ 5): Sleep quality is considered good.
■ (PSQI: 6–10): Sleep quality indicates a Mild disturbance.
■ (PSQI: 11–15): Sleep quality is considered moderate disturbance.
■ (PSQI ⩾ 16): Sleep quality is considered poor.
In this study, we assumed that knowledge and attitudes (predisposing factors), enabling factors and reinforcing factors would influence women’s health-promoting lifestyle behaviors, which in turn would affect their sleep quality. We examined the relationships between these factors and outcomes using correlation, but no formal mediation analysis was performed.
Validity
Content validity was evaluated by 3 experts in obstetrics and gynecological nursing, each with more than 10 years of academic and clinical experience. Each item was assessed for clarity and relevance. The item-level CVI (I-CVI) ranged from 0.83 to 1.00, and the scale-level CVI (S-CVI/Ave) was 0.89. The tools were adjusted according to the experts’ suggestions to improve clarity and content relevance.
Reliability
The tools were evaluated for reliability by Cronbach’s alpha coefficient test, which indicated that the tools had consistent items with moderate to high reliability. The internal consistency of knowledge assessment sheet was α = 0.85, the attitude Likert scale was α = 0.82), the enabling factors sheet was α = 0.78, the reinforcing factors sheet was α = 0.75, the health-promoting lifestyle questionnaire was α = 0.84, and it was ranged from 0.79 to 0.87 for the six subscales and finally PSQI was α = 0.81.
Ethical considerations
This research received the green light from the Scientific and Ethical Research Committee at Philadelphia University’s Faculty of Nursing (as indicated by Approval No. [54/20/100/TK]). The research activities were carried out while adhering to the guidelines set forth in the Declaration of Helsinki. Furthermore, formal authorizations were secured from the necessary research environments.
A complete description of the study objectives and procedures was provided to each woman. Before any data were gathered, all participants gave their informed consent in writing. Privacy and anonymity were guaranteed to all participants, with participation being completely voluntary for all women. Women were assured that they could discontinue participation in the study at any time without any repercussions. Engagement in the study did not expose participants to any form of physical, social, or emotional risk. To ensure the confidentiality of personal information, data collection was securely disposed of following the completion of statistical analysis.
A pilot study
In order to confirm the tool’s sequence, clarity, and pertinence and to find any problems with the tool statements, a pilot study was conducted with nine women (10% of the total sample). The time needed to complete the questionnaire was another goal of the pilot study. The women who took part in the pilot study were then added to the sample without any changes.
Field work
After receiving formal approval from the director of Al Bashir Hospital, Jordan, information was gathered in five stages. The present study’s objectives were achieved through the adoption of the preparatory, interviewing, planning, implementation, and evaluation phases. The current study’s fieldwork was completed in a year, from the beginning of January 2024 to the end of December 2024. Two days a week, the researcher went to Al Bashir Hospital.
Educational content and delivery methods
Preparatory phase
The research process began with the preparatory phase. In order to conduct the research, books, articles, magazines, and networks about studies on the impact of the ΡRECEDE-ΡROCEED model on health behaviors among women with gestational diabetes were reviewed, covering both historical and contemporary literature on the subject. It enabled the researchers in creating the required data collection tools and comprehending the extent and criticality of the problem. During this stage, a formal letter was submitted to the director of Al Bashir Hospital, Jordan, requesting permission to conduct the research.
Interviewing and assessment phase
The researcher conducted visits to Al Bashir Hospital in Jordan twice a week. During these visits, the researcher personally conducted all interviews. The researcher started by presenting himself to the participants, followed by an explanation of the study’s purpose, then provided comprehensive information regarding the study, including goals, length, and tasks, and obtained consent from the participants to take part in the research.
The researchers employed the following instruments in each interview: instrument (I), “A structured interviewing questionnaire” was used to evaluate the study women’s overall characteristics. Tool II (the ΡRECEDE-ΡROCEED model construct) was used to identify the predisposing factors, which included knowledge and attitude about gestational diabetes, enabling factors, like having educational classes, having access to information sources, and having the ability to manage complexity, and reinforcing factors to assess the help and motivation provided by friends, family, and healthcare providers. Tool III Health-Promoting Lifestyle profile-II) was used to gauge the pregnant women’s health-promoting behaviors. Tool IV (PSQI) was utilized to measure sleep patterns and their quality. The average time needed to finish each woman’s interview was between 20 and 25 min. Two to three women were interviewed on average each day. All participants were followed to ensure they attended all sessions, and adherence to the educational material was monitored through attendance logs, discussion participation, and feedback during each session, as part of managing the study under the open-label design.
Planning phase
Based on the pre-program assessment baseline data and the available scientific literature, the researcher created an Arabic-language booklet with figures that addressed women’s knowledge gaps regarding GDM, healthy lifestyle choices, and gestational diabetes adaptive measures. The ΡRECEDE-ΡROCEED model was used as a guide when developing the educational program. Participants were divided in to small groups of 2 to 3 women to facilitate interaction, engagement, and monitoring adherence. Program objectives were created; they comprised the following:
General objective: After the nursing intervention sessions, each participant in the study group would exhibit high levels of lifestyle behaviors related to the six aspects of a healthy lifestyle.
Specific objectives: Upon completion the nursing intervention sessions, participants in the study group were anticipated to: – Obtain necessary information about GDM. – Adopt a positive outlook toward GDM. – Aware of factors that support and facilitate lifestyle changes. – Adopt health adaptive measures regarding GDM and sleep disturbances.
Implementation phase
The researcher applied an organized nursing program to help women manage gestational diabetes. The educational component was conducted over a period of 8 weeks and included four educational sessions scheduled biweekly (one session every 2 weeks). With each session ranging from 45 to 60 min in duration. Face-to-face sessions were held during antenatal clinics and scheduled in coordination with the availability of participating women. Participants received details about session timing during clinical visits, with additional reminder phone calls conducted a head of each session to enhance adherence.
Women assigned to control group was provided with the usual medical care offered by hospital, whereas subjects in the intervention group were administered routine care alongside educational intervention designed according to ΡRECEDE-ΡROCEED model.
The initial session focused on introducing women to the nursing intervention designed for gestational diabetes management which was developed based on ΡRECEDE-ΡROCEED model. Women were informed of the next session schedule at the end of the meeting. The next session started with a summary of the prior session and its goal, using simple Arabic language to match the women comprehension levels. Multiple teaching strategies were utilized, including interactive group discussion, role playing, demonstrations and visual materials such as educational videos, PowerPoint presentations, customized booklets, and posters. A specific amount of time was allotted at the end of each session to discuss participants questions and receive clarifications on any unclear issues.
The first session started on the woman’s initial visit after the interview stage and included definition, pathophysiology, risk factors, causes, symptoms, effect of GDM on mother and newborn, diagnosis of GDM, treatment methods, and effect of GDM on sexual function and health behaviors.
The second session started on the women’s second visit after the interview stage and included changing women’s outlook toward gestational diabetes to a positive one (diabetes mellitus is not a life-threatening condition; it can be avoided by adopting healthy lifestyle habits and getting regular blood glucose tests).
The third session began during the women’s third visit and followed the interview stage, and took into account how the ΡRECEDE-ΡROCEED model affects sleep quality and health behaviors among women with GDM. Encourage women to attend educational classes, have access to information resources, and have the ability to manage complications. Women should also have the encouragement and support of their families and medical professionals.
The fourth session included educating women on adopting health-adaptive measures related to gestational diabetes and sleep disturbances. Sessions were held in small groups of 2 to 3 women to facilitate interaction. For participants who missed any sessions, makeup sessions were offered when possible, and educational materials were provided via phone or email. Participants were encouraged to ask questions during sessions or contact the researcher by phone for additional support.
Evaluation phase
Data were gathered 4 weeks after the intervention and compared with pre-intervention data using the same pre-assessment instruments in order to evaluate the intervention of the PRECEDE-PROCEED model on health behaviors and sleep quality among women with gestational diabetes. Attendance, participation, and adherence to the educational content were considered in the evaluation. To prevent bias, the control group was evaluated before the study group in this open-label design. Women in the group are under control received the educational booklet so they could benefit from it in future pregnancies.
Statistical analysis
Information was checked before being entered into the computer system. The purpose was achieved using SPSS Version 0.22 for statistical analysis and data organization. Descriptive statistics, such as mean, standard deviation, frequency, and percentages, were utilized. Chi-square tests, independent t-test, and Pearson correlation coefficients were utilized. A p-value less than 0.05 was considered statistically significant, while a p-value less than or equal to 0.001 was considered highly significant.
Results
Table 1 summarizes sociodemographic characteristics of both groups. The table illustrates that there was not a statistically significant variance found between both groups in terms of age, residence, education, occupation, and BMI (p > 0.05). These findings indicate that both groups were comparable at baseline, ensuring a balanced starting point for the intervention.
Distribution of both groups according to sociodemographic characteristics (n = 90).

Note. No statistically significant difference (p > 0.05); t: independent t-test; €: Fisher’s exact test.
Table 2 summarizes obstetrics history of both groups. The table illustrates that there was not a statistically significant variance found between both groups in term of gestational age, gravidity, parity, history of abortion, or previous gestational diabetes (p > 0.05). These results confirm baseline comparability between groups.
Distribution of both groups according to obstetrical history (n = 90).
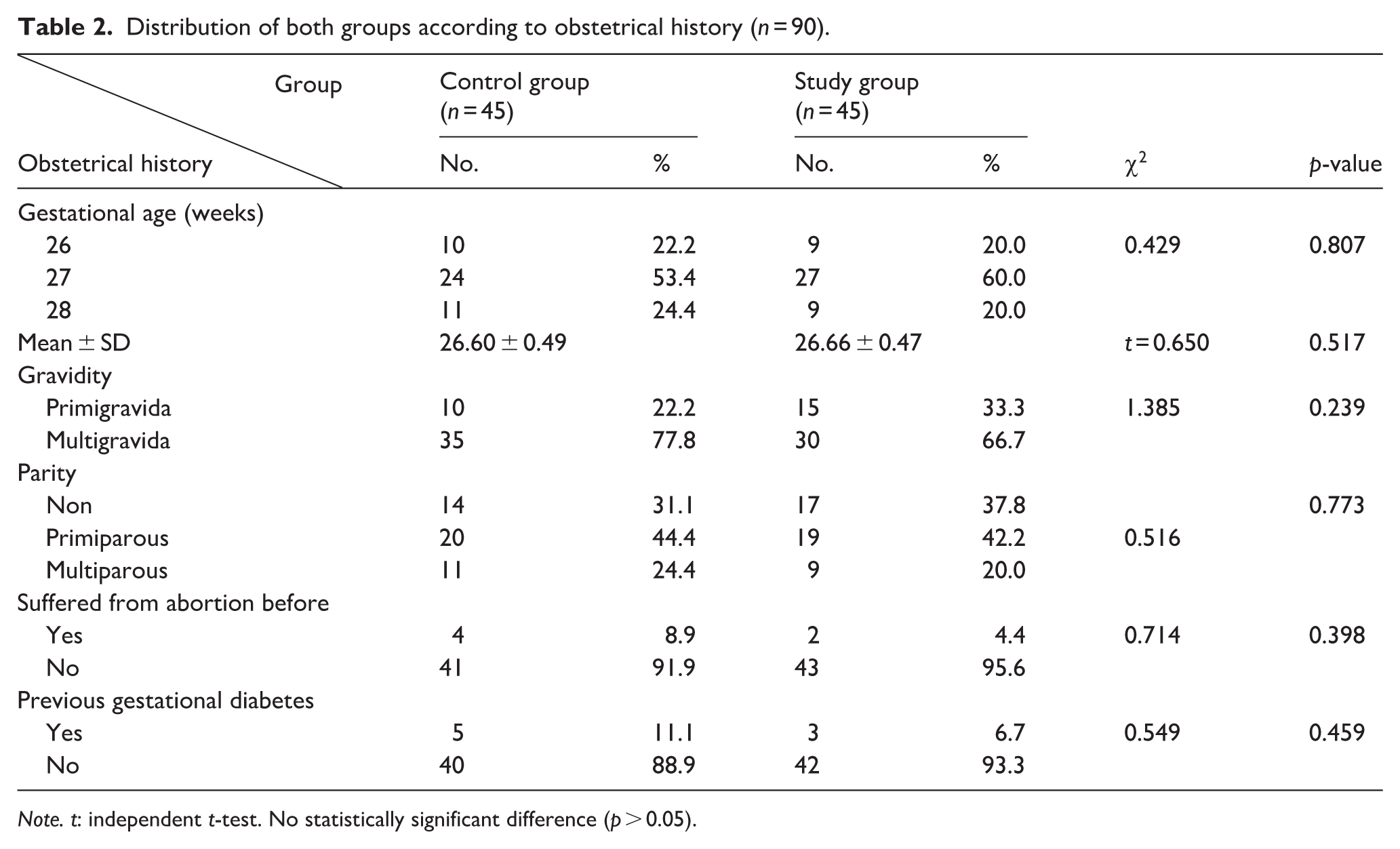
Note. t: independent t-test. No statistically significant difference (p > 0.05).
Table 3 shows no significant difference in pre-intervention knowledge, attitude, enabling, and reinforcing characteristics between the two groups (p > 0.05). Whenever there was a highly statistically significant difference between the mean ± SD of both the study and control group at the post-intervention phase (p < 0.001**). That means ±SD regarding predisposing factor (knowledge and attitude), enabling factor, and reinforcing factor of a study group during the post-intervention phase was 19.77 ± 3.97, 26.40 ± 3.79, 14.75 ± 2.20, and 11.11 ± 1.70 compared to 14.88 ± 4.97, 26.40 ± 3.79, 14.75 ± 2.20, and 9.35 ± 1.72 of control group, respectively.
Comparison of the mean scores of educational and ecological assessment phase structures of PRECEDE-PROCEED model among both groups at pre- and post-intervention phases (n = 90).

Note. No statistically significant difference (p > 0.05).
A high statistically significant difference (p ⩽ 0.001).
t: independent t-test; MDw: mean difference within groups; MDb: mean difference between groups.
ANCOVA adjusted for age, residence, occupation, and educational level.
Table 4 indicates that, in the pre-intervention phase, there was not a statistically significant variance found in the mean score of health-promoting lifestyle behaviors and their aspects between both groups (p > 0.05). After the intervention, the study group’s mean difference score for health-promoting lifestyle behaviors was higher than the control group’s (p < 0.001). It is evidenced that the total mean ± SD of the study group was raised in post-intervention than pre-intervention from 66.86 ± 6.78 to 97.02 ± 15.27 and for the control group from 66.95 ± 8.42 to 77.71 ± 11.55, respectively.
Comparison of the total mean scores of health-promoting lifestyle behaviors regarding gestational diabetes in both groups at pre- and post-intervention of the PRECEDE-PROCEED model (n = 90).

Note. ns: no statistically significant difference (p > 0.05).
A high statistically significant difference (p ⩽ 0.001).
t: independent t-test.
ANCOVA adjusted for age, residence, occupation, and educational level.
Figure 2 illustrates that 6.7% of the control group and 4.4% of the study group had high lifestyle behaviors regarding gestational diabetes in the pre-intervention phase. While, 8.9% of the control group and 57.8% of the study group had high lifestyle behaviors regarding gestational diabetes in the post-intervention phase.
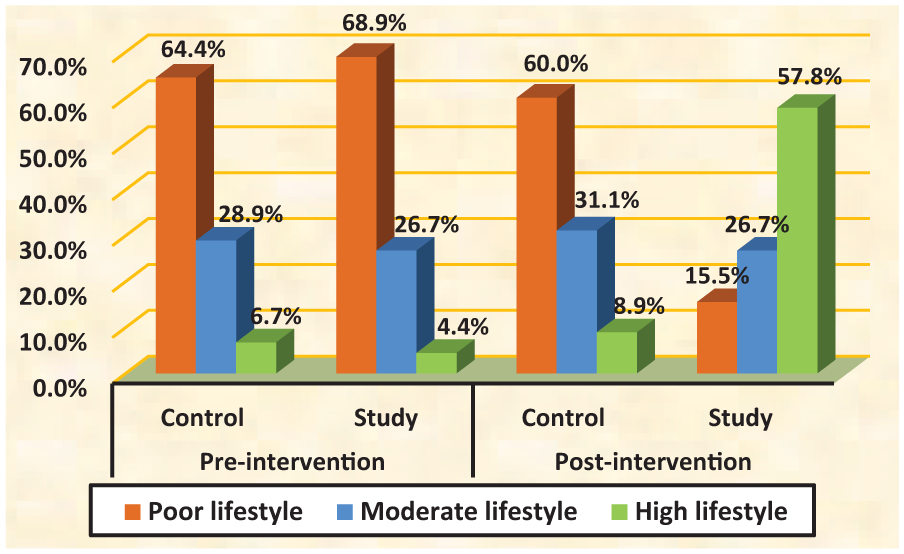
Distribution of studied women’s total lifestyle behavior scores at pre- and post-interventions of the PRECEDE-PROCEED model (n = 90).
Table 5 demonstrates that there was no notable statistical distinction between the two groups in terms of the overall average sleep quality score before the intervention (p > 0.05). Conversely, a highly significant statistical variance was observed between the study and control group in relation to the overall average sleep quality score after the intervention (p ⩽ 0.001). The total mean ± SD of the study group was lower in post-intervention than pre-intervention, from 11.91 ± 4.26 to 8.20 ± 2.65, and for the control group from 11.13 ± 5.68 to 11.24 ± 5.32, respectively.
Comparison of the mean scores of women’s quality and patterns of sleep in both groups at pre- and post-intervention of the PRECEDE-PROCEED model (n = 90).

Note. t: independent t-test; ns: no statistically significant difference (p > 0.05).
Statistically significant (p ⩽ 0.05).
Highly statistically significant (p ⩽ 0.001).
Figure 3 shows that 40.0% of participants in the control group and 33.3% of participants in the study group had severe sleep quality disturbance during the pre-intervention phase. Meanwhile, 31.1% of participants in the control group had severe sleep quality disturbance after the intervention, while there was no severe sleep quality disturbance among women in the study group after the intervention of the PRECEDE-PROCEED model.

Distribution of the studied sample (control and study groups) according to total quality and pattern of sleep at pre- and post-intervention of PRECEDE-PROCEED model (n = 90).
Table 6 illustrates a significant positive connection between lifestyle scores and sleep quality in both groups pre- and post-intervention, showing high statistical significance (p ⩽ 0.001).
Correlation between total lifestyle behaviors score and total quality and pattern of sleep score of both groups at pre- and post-intervention phases (n = 90).

Note. **A highly statistically significant difference (p ⩽ 0.001).
Discussion
Worldwide, gestational diabetes is commonly reported, making it a significant health issue. The condition of GDM significantly affects both lifestyle habits and sleep quality in pregnant women, which may be associated with the anticipated mortality risk among diabetic pregnancies. 23
This study evaluated how a nursing program guided by the ΡRECEDE-ΡROCEED model influenced sleep quality and health behaviors in pregnant women with gestational diabetes. Results revealed significant positive changes among the intervention group versus the control group, confirming the research hypothesis.
The current research indicated that the demographic profiles of both groups show no measurable differences. The table indicates that about two-fifths of both groups were aged 30 years or older, with a mean ± SD of 28.37 ± 5. 31 for the control group, and 28.08 ± 6.09 for the study group. Additionally, less than two-thirds of the control group and over half of the study group resided in rural regions. Furthermore, fewer than half of the control group and more than half of the study group had attained secondary education. In terms of occupation, over half of the participants in both groups were not employed. BMI was considered a baseline characteristic and showed no significant difference between groups. This suggests that the BMI did not confound the intervention’s effects on the outcomes measured.
The current results come about concurred with Eraky Mahmoud and Abdel Hakeem Hasneen, 24 who found that three-fifths of the studied participants were in the age group >30 years. More than half of the participants lived in rural areas, more than three-quarters were housewives, and more than half of them had secondary education. Also, this finding aligns with the research carried out by El-Ansary and Fouad, 25 indicating that slightly over two-thirds of pregnant women over the age of 30 had an average age of 27.6 ± 5.9 years. According to the researcher, the similarities in the data could be ascribed to the significantly higher incidence of GDM in women over the age of 30. This may also result from the connection between age and the likelihood of developing GDM.
Regarding the obstetric background of the females analyzed in the research cohorts, the findings showed no statistically notable distinction in obstetric history between both groups. In addition, the current results showed that over half of the women in both groups were at 27 weeks of gestation. Many had been pregnant multiple times, with fewer than half being first time mothers. Most participants in the study had no history of abortion and had not previously been diagnosed with GDM. The outcomes mirror the observations of Byakwaga et al., 26 which indicated that most participants had not previously diagnosed with gestational diabetes. Furthermore, the results support the findings of Mohamady et al., 27 which showed that most women in their study undergo more than one pregnancy and childbirth.
Poor knowledge of gestational diabetes can result in inadequate comprehension of medical recommendations, which can hinder adherence to recommended diet and lifestyle practices and place both the woman and her fetus at greater risk of complications. 25 The study showed that before the program, both groups knew about the same amount regarding diabetes during pregnancy, with no real differences seen. After the program, clear differences between the groups started to appear. Having correct knowledge is key to building a good mindset and improving health actions. The improvements that were seen are especially important, as they show we need to keep giving support and advice to help women change habits and choose wisely. These results could mean the PRECEDE model was used well, which worked in spreading knowledge about diabetes in pregnancy.
In line with the current findings, Ahmed Osman Mohamed et al. 28 noted a significant enhancement in knowledge, along with facilitating and reinforcing factors right after the ΡRECEDE-ΡROCEED intervention, with lasting improvements seen at the 1-month follow-up. This result is consistent with the work of Ugwu and Ene, 21 who explored how a diabetes education program affected the understanding of pregnant women. They discovered that more than three-quarters of the control group and over a quarter of the study group lacked adequate knowledge about gestational diabetes before joining the education program. By the conclusion of the diabetes education program, it was determined that more than a third of the control group participants and over three-quarters of the participants in the study group had gained adequate knowledge regarding gestational diabetes.
The attitudes and self-care practices of expectant mothers significantly influence the outcomes of gestational diabetes during their pregnancies. A pessimistic perspective on diabetes may hinder women from adhering to medical guidance, leading to poorer results for both the mother and the infant. 29 The present study revealed that prior to the educational intervention, both groups exhibited similar attitudes toward gestational diabetes without any notable differences. Following the intervention, a notable distinction appeared between the two groups. The results indicate that the intervention meaningfully influenced pregnant women’s views on gestational diabetes, as it offered vital information that informed their attitudes.
Consistent with previous research, Kanoori et al. 30 examined how educational sessions affected pregnant women’s understanding and perspectives on gestational diabetes, with results indicating notable advancements following the sessions. In line with El-Ansary and Fouad, 25 the results indicated that approximately 75.0% of participants began with a negative general attitude toward GD. After the intervention, most individuals showed a positive attitude, which helped enhance their skills and improve disease management effectively.
Facilitating elements were essential in transforming intentions into behaviors. The present study investigated the facilitating elements, including obtaining family support for insulin treatment and dietary modifications, gaining important knowledge and skills through educational programs for gestational care, and following the directives of health professionals. The results from the current study displayed a significant, statistically strong difference between the intervention and control groups following the intervention. This highlighted the effectiveness of the ΡRECEDE-ΡROCEED model in empowering expectant mothers by offering essential information that fosters beneficial beliefs and attitudes regarding gestational diabetes and its self-management practices. By deepening their comprehension of their partners’ subjective norms and utilizing the available enabling factors, they can increase their intention to engage in behaviors related to gestational diabetes. This confirmed the positive effects of applying the intervention based on the earlier model.
The outcomes aligned well with the discoveries by Ahmed Osman Mohamed et al., 28 who demonstrated a notable enhancement in enabling and reinforcing factors; this progress continued even after a month. Additionally, these findings correspond with the study by Lamadahet al. 31 conducted in Iran, which centered on analyzing self-care behaviors associated with gestational diabetes. The research executed an educational program for empowerment based on the BASNEF model. The results showed a significant enhancement in the average score of facilitating factors for the intervention group compared to the control group after the intervention. Three studies investigating educational programs based on the BASNEF model all yielded comparable findings, indicating a significant increase in the average score of enabling factors after implementation.
The positive outcomes of implementing the intervention based on the PRECEDE model are evident. In a comparable manner, El Ashery Askeret al. 32 investigated the outcome of an educational program grounded in the PRECEDE model on promoting preventive actions among subjects at elevated risk for type 2 diabetes. Their findings indicated a decrease in average scores regarding knowledge, enabling factors, and reinforcing factors associated with diabetes prior to the implementation of the educational intervention. A notable enhancement was noted, showing statistical significance right after the nursing intervention and once more 3 months later.
Comparison of average scores for lifestyle habits associated with gestational diabetes showed no significant differences between the study and control groups before the intervention, both in general health-promoting lifestyle behaviors and in their specific areas. After the intervention, the study group showed notably higher improvements in average scores for overall health and multiple aspects of health-enhancing lifestyle practices compared to the control group. These enhancements can be linked to the success of the educational program, which seems to have favorably impacted various aspects of health-promoting behaviors in the participants. These data are similar to those found by Zakaria et al., 33 who noted a significant rise in the uptake of healthy lifestyle habits among women with GDM following a lifestyle intervention when compared to the period before the intervention.
Examination of initial data revealed no statistically significant difference in overall sleep quality scores between the both groups prior the intervention. The evaluation conducted after the intervention indicated a highly significant difference in overall mean sleep quality scores, benefiting the study group. Enhancements in sleep quality might be linked to participants’ compliance with health advice given through the nursing program utilizing the PRECEDE-PROCEED model, especially recommendations concerning relaxation techniques. These results align with the research of Bay Ozcalik and Sogukpinar, 34 who found notably reduced average PSQI scores and enhanced sleep quality for participants in the intervention group versus the control group. Additionally, involvement in the educational program was significantly linked to sleep quality, representing about 6% of its variance.
The present findings indicate a strong statistical correlation between the total lifestyle behaviors score as well as total sleep quality and predisposing factors (total knowledge and attitude), enabling factors, and reinforcing factors. These findings could be attributed to the increased awareness of factors that contribute to gestational diabetes, which encourages the adoption of healthy preventive measures to prevent complications and ensure a healthy pregnancy. The discoveries were consistent with the research conducted by Zeinali et al., 35 revealing a noteworthy correlation between knowledge scores, enabling factors, and reinforcing factors with gestational diabetes, alongside lifestyle behavior practices scores among expecting mothers throughout the intervention stages.
Recommendations: Based on research findings, it was recommended that:
Implementing continuous educational programs utilizing the ΡRECEDE-ΡROCEED model for women with gestational diabetes to enhance their knowledge and awareness surrounding the condition.
Distribute brochures and posters on health behavior modification for gestational diabetes to outpatient clinics and maternal and child health centers.
Further research
For improved generalizability of the findings, it is advised to conduct the study again using a sizable and representative probability sample.
Nurses are encouraged to fulfill their role as educators by providing health education on topics such as gestational diabetes, health behaviors, and sleep quality.
Strengths of the research
The research utilized proven and trustworthy tools, including the Health-Promoting Lifestyle Profile-II and the PSQI, increasing the precision of the results.
A thorough approach was employed by evaluating several aspects, encompassing knowledge, attitudes, facilitating factors, and health behaviors.
Thorough monitoring and management of possible confounders enhanced the credibility of the findings.
Limitations of the research
One limitation of this study is the relatively small sample size of 90 participants from a single center, which may affect the generalizability of the findings to a broader population.
The reliance on self-reported data for some variables, such as pre-pregnancy BMI, may be subject to recall bias or inaccuracies.
Conclusion
Concurring with the findings of the recent study, it was determined that the study hypotheses were validated, and the utilization of the ΡRECEDE-ΡROCEED model proved to be successful in enhancing the knowledge, attitude, sleep quality, and health behaviors of pregnant women diagnosed with gestational diabetes. Furthermore, a strong and statistically significant correlation was observed between the total scores of lifestyle behaviors and sleep quality, and the predisposing factors (total knowledge and attitude), enabling factors, and reinforcing factors in both the study and control groups before and after the intervention phases. Furthermore, a strong and significant positive association was observed between the overall score for sleep quality and the overall score for lifestyle behaviors in both the study and control groups, concurring with the findings of the recent study.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Riyadh Elm University, College of Pharmacy, Nursing and Medical Sciences, for their support and assistance throughout this research. In addition, the researchers are grateful to the women who participated in the study for the advancement of nursing science.
Author’s Note
Fatima Kamal Ali and Amira Mohamed Abdelfatah are now affiliated with the Department of Obstetrics and Gynecological Nursing, Faculty of Nursing, Benha University, Banha, Egypt.
Ethical Considerations
This research received the permission from the Scientific and Ethical Research Committee at Philadelphia University’s Faculty of Nursing (as indicated by Approval No. 54/20/100/TK). The research activities were carried out while adhering to the guidelines set forth in the Declaration of Helsinki. Furthermore, formal authorizations were secured from the necessary research environments. A complete description of the study objectives and procedures was provided to each woman.
Consent to participate
Before any data were gathered, all participants gave their informed consent in writing. Privacy and anonymity were guaranteed to all participants, with participation being completely voluntary for all women.
Consent for publication
Not applicable.
Author Contributions
Fatima Kamal Ali: Conceptualization; Methodology; Supervision; Writing – original draft; Formal analysis.
Amira Mohamed Abdelfatah: Investigation; Validation; Writing – original draft; Formal analysis.
Rabia Hani Haddad: Conceptualization; Supervision; Data curation; Writing – review & editing; Methodology; Investigation.
Talal Bani Ahmad: Investigation; Writing – original draft; Data curation; Software.
Fathia Mahmoud AbdElmenim Sayed: Investigation; Validation; Visualization; Resources.
Nashwa Saber Atia: Resources; Visualization; Validation; Investigation.
Ashraf Jehad Abuejheisheh: Conceptualization; Methodology; Supervision; Project administration; Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.