
Abstract
Background:
Health workforce shortages are a serious impediment to the delivery of effective and person-centered care, particularly in conflict settings. Midwives are a critical cadre who can help avert maternal and child death, but face persistent barriers to education, employment, regulation, and professional development—challenges that are especially pronounced in conflict-affected areas. Few studies have systematically explored midwives’ experiences in these settings.
Objectives:
The EQUAL midwifery cohort study was established to systematically examine midwives’ educational and professional trajectories in Northeast Nigeria and in Central and Southeast Somalia, with the goal of identifying context-specific factors influencing retention, deployment and professional growth.
Design:
Multiple cohorts of students and recent graduates will be enrolled, complete an intake survey, and be followed with additional surveys approximately 6 months after enrollment and then annually. Focus group discussions and in-depth interviews with a sub-set of participants will follow each round of surveys to expand on survey findings.
Methods and Analysis:
Qualitative data analysis will focus on the lived experiences of participants, and how these experiences shape their professional identities and career trajectories. Survey analysis will assess levels of attrition, including withdrawal from training and exit from the profession post-graduation. Cox regression models will estimate hazard ratios and 95% confidence intervals for these outcomes, and median survival time in the profession will be calculated to determine when attrition is most likely. Risk factors for attrition during both training and professional practice will be examined.
Ethics:
Ethical approval was obtained from John Hopkins Bloomberg School of Public Health, the Somali Research and Development Institute, and Yobe State Health Ministry of Health Ethics Committee.
Discussion:
This research will offer insights into a critical yet under-explored segment of the global health workforce: early career midwives in conflict-affected settings. It serves as a proof-of-concept for the feasibility of longitudinal health workforce research in conflict-affected areas of Nigeria and Somalia, offering unprecedented evidence on the lived experiences and expressed needs of midwives to inform the improvement of midwifery education, working conditions, and support networks in these settings.
Plain language summary
• This will be the first study to follow midwives in humanitarian settings over time, filling a gap in knowledge about the experiences of this important group within the health workforce.
• The research is part of a multi-country research consortium and involves partnership with local researchers, including midwives, who contribute deep knowledge of the health systems and firsthand understanding of the realities of midwives in conflict settings.
• Following midwives over time enables the study to observe their professional journeys, measure how many leave the field, and capture changes in motivation in a way that a studies conducted at a single point in time cannot provide.
• The study focuses on conflict-affected areas of Nigeria and Somalia, so findings may not reflect the experiences of midwives in other areas within or outside of the two countries.
Introduction
The global health community is at a critical juncture. Despite significant progress in recent decades, reductions in maternal and newborn mortality have stagnated, with a large share of the global mortality burden in countries with appeals for international humanitarian assistance to address the impacts of armed conflict, climate emergencies, food insecurity, and disease outbreaks.1 –3 While most maternal and neonatal deaths and stillbirths can be prevented with timely access to high-quality care, myriad challenges to provision of safe, effective, timely and person-centered services exist, including health workforce shortages and persistent barriers to midwifery education, employment, regulation, and professional development.4 –6
The International Confederation of Midwives (ICM) defines a midwife as “a person who has successfully completed a midwifery education program based on the ICM Essential Competencies for Midwifery Practice and the framework of the ICM Global Standards for Midwifery Education, recognized in the country where it is located; who has acquired the requisite qualifications to be registered and/or legally licensed to practice midwifery and use the title ‘midwife,’ and who demonstrates competency in the practice of midwifery.” 7 In short, midwives are trained health professionals, qualified, and licensed to provide care to women throughout pregnancy, childbirth, and the postnatal period.
Across low, middle and high-income contexts, documented challenges to providing high-quality midwifery care include social factors (e.g., gender inequality), professional factors (e.g., absence of midwives in policy dialog, low recognition by other professions of midwifery skills, restrictions on roles, or scope of practice), and economic factors (e.g., comparatively low salaries, lack of transport, accommodation, or support structures for round-the-clock service provision).8,9 In some settings, the struggle of midwives for recognition as skilled, autonomous professionals is not only a barrier to establishing midwifery models of care 10 but also to individual midwives’ career progression and can be a disincentive for people considering a career as a midwife.11 –13 In conflict-affected settings, these issues may be exacerbated, and midwives may face additional challenges such as expanded job responsibilities, inconsistent salaries, threats to personal security, and secondary trauma (both physical and psychological).14 –18
Prospective nursing and midwifery cohort studies in high-income countries (e.g., United Kingdom, Australia, New Zealand, and Sweden) have provided valuable insights to strengthen both education and professional support and development efforts. 19 However, no studies to date have systematically explored how early career midwives navigate entry into the workforce in conflict-affected contexts. In fact, relatively few studies have set out to document personal and professional experiences of health workers in crisis-affected settings and, while often discussed as factors hindering quality health service delivery, efforts to measure or critically analyze drivers of workforce turnover and dropout in this group are relatively rare.20,21 Studies conducted by the ReBUILD consortium provide rich insights into the complexities of health worker experiences in crisis and post-crisis contexts.22,23 Qualitative studies conducted in Cameroon, Ethiopia, Mali, and Yemen highlight the coping mechanisms that healthcare workers employ to manage stressors faced due to armed conflict, insecurity, and disruption of basic health system functions.24 –27 Complementary studies in Syria explore the motivation of healthcare workers who remained in Syria through periods of extreme insecurity and health system collapse, as well as the professional and psychological struggles of those forced to flee, providing insights into the complexity of factors contributing to workforce dropout and migration during protracted conflicts.28,29 Most of these studies are cross-sectional or retrospective in nature, however, and do not focus on the lived experiences of midwives.
The few studies that do examine factors influencing retention of midwives in conflict-affected settings, namely Afghanistan and the Democratic Republic of Congo, emphasize the importance of context-adapted gender-sensitive strategies to prevent attrition of midwives working in resource-constrained, insecure environments.30,31 A deeper and more systematic exploration of midwives’ experiences is needed to understand the extent to which support needs vary across contexts and to improve responsiveness of current midwifery education, workforce development, and support systems.
Research aims
The aim of this study is twofold:
To generate evidence on factors affecting midwifery students’ and early career midwives’ aspirations, workforce participation, and retention by tracking a cohort of students and graduates over a multi-year period.
To document early career midwives’ experiences working in conflict-affected areas, including changes in responsibilities, personal and professional stressors, and support networks during periods of increased insecurity.
Methods
Study design
Longitudinal research is essential for understanding career trajectories. This prospective midwifery workforce cohort study employs a sequential, explanatory mixed-methods design, whereby qualitative methods are used to explain and expand quantitative survey findings. Multiple cohorts of students and recent graduates will be enrolled in the cohort study, complete a structured intake survey, and be invited to participate in an initial follow-up survey approximately 6 months after enrollment, and then subsequent surveys at approximately 1-year intervals. Following each round of surveys, focus group discussions and in-depth interviews will be conducted with a sub-set of cohort members to explore and expand upon survey findings. From a participant perspective, the current duration of the study is up to 2 years. Funding is secured through early 2026, ensuring a minimum of one round of post-graduation follow-up for all cohorts (Figure 1). Additional funding will be pursued in hopes of following participants for 5 years (or more) post-graduation.

Cohort study timeline.
Setting
In Nigeria, research is being conducted in Yobe State in the Northeast Zone of Nigeria. Yobe has been acutely affected by the decade-long armed conflict associated with Boko Haram insurgency. Across the state, a substantial proportion of the population resides in areas that are affected by armed conflict, population displacement, and disruption of livelihoods and social services. 32 Maternal and newborn health service delivery is hampered by a series of challenges which include inaccessibility of health facilities, maldistribution and shortages of health workers, and gaps in quality of care. 33 Yobe was one of the first states in Nigeria to be given national approval to train “community midwives,” a 2-year program to prepare midwives serving rural community settings to help mitigate high mortality rates and address health workforce gaps. There are currently two midwifery programs in Yobe: a 2-year community midwifery program and a 3-year basic midwifery program. Both are fully accredited professional midwife training programs registered with the Nursing and Midwifery Council of Nigeria. 34
In Somalia, research is being conducted in Benadir and Galgaduud regions. Benadir region (Mogadishu) in Southeast Somalia is the capital and largest city in the country; Benadir is host to the largest protracted internally displaced population in the country, nearly 400,000 internally displaced persons (IDPs), mainly living in informal settlements across the city. Galgaduud is an administrative region of Galmudug state in Central Somalia, near the border with Ethiopia. The security situation across Somalia is volatile which has presented challenges for maternal and newborn health service delivery in the country. The combination of civil unrest, shortage in skilled birth attendants and lack of supplies and equipment have made the situation dire for women and children. Over the past decade, the country has expanded its midwifery education efforts. Midwifery schools offer one of two midwifery professional training programs: either a direct entry-entry midwifery program or a post-education program for nurses. This study will focus on the direct-entry programs which include diploma programs (3-year, primarily public-sector programs developed by the Ministry of Health and UNFPA) and 4-year bachelor’s degree programs offered by private institutions.
These sites were selected as part of a broader program of research to generate evidence to improve the provision of maternal and newborn health services in low-income conflict-affected contexts in sub-Saharan Africa. Midwifery workforce development and support was prioritized by research teams in both Nigeria and Somalia, and study locations within each country purposively selected based on maternal and newborn health indicators, partner presence, and accessibility for research.
Study population and recruitment
To date, two cohorts of students in basic and community midwifery programs have been enrolled as study participants in each country (Table 1). Eligibility criteria differed slightly across countries, depending on timelines for pre-service education program enrollment and graduation, as well as health workforce education stakeholder interests.
Cohort study enrollment by country, degree program and education status.
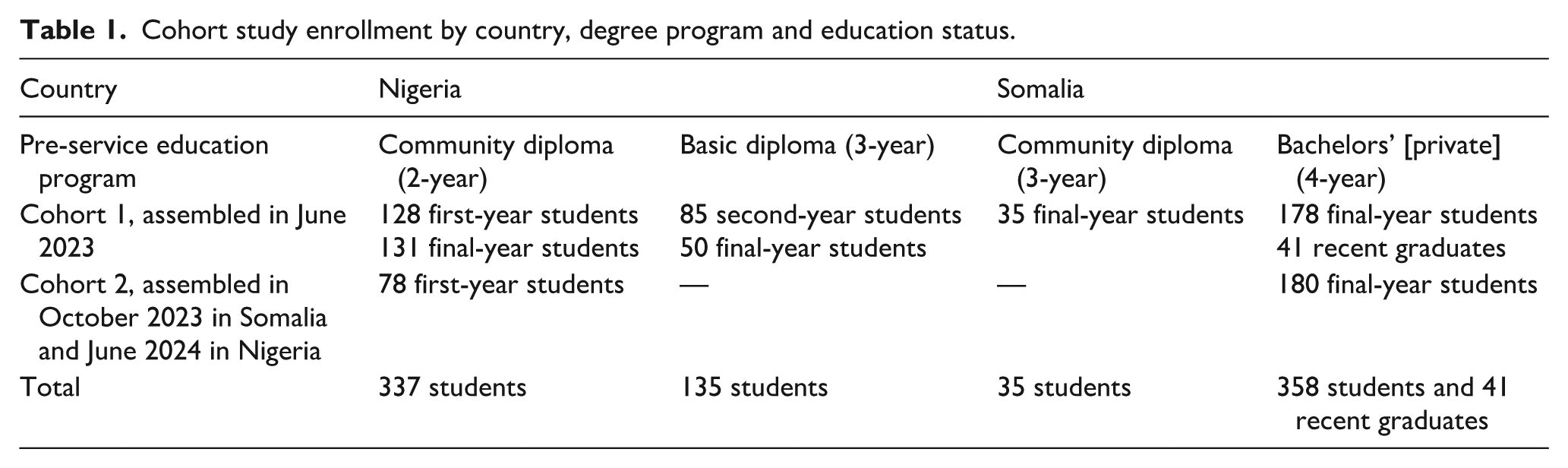
In Nigeria, the first cohort was assembled in June 2023 and the second cohort in June 2024. The study population comprises students recruited while studying in one of the two public direct-entry midwifery education programs in Yobe State at the time. To be eligible, students had to be enrolled in their first or second year in the 2-year community midwifery program or second or third year in the 3-year basic midwifery program at Shehu Sule College of Nursing and Midwifery in Yobe State. Students needed to have passed their first semester exam which signifies interest in continuation of the program. Those who had not passed the exam, those were not in the targeted year and those who declined to provide consent were not eligible to participate. Ultimately, 394 individuals enrolled in the first cohort and 78 in the second cohort for a total of 472 participants in Nigeria.
In Somalia, the first cohort was assembled in June 2023 and second in October 2023. The study population comprises students recruited while in their final year of study (or shortly following graduation, if the academic year was not in session) at one of eight purposively midwifery education programs in Benadir and Galgaduud. Of 16 private universities that provide direct entry midwifery education programs and 2 community midwifery education programs located in these 2 regions, we purposely selected 7 private degree programs in Mogadishu and the only public community midwifery diploma program in Galgaduud. We were unable to include the one community midwifery diploma program in Mogadishu as it did not have any students engaged in their last year of study. All students in the selected schools who were in their last year were invited to join the study.
The first cohort included students from both private and community midwifery programs, but the second cohort only had students from private schools. This was because community midwifery schools in Somalia recruit every 3 years, and during the second data collection period, their students were in their first year and thus were not eligible for recruitment into the study. Ultimately 254 individuals enrolled in the first cohort and 180 in the second cohort for a total of 434 participants in Somalia.
All cohort study participants in Nigeria and the vast majority of participants in Somalia were recruited in person on campus. For all schools, program directors were contacted in advance of the study team’s visit and asked to inform eligible student cohorts of the upcoming study enrollment visit. Students with interest in participating were asked to arrive at a designated location on campus and to sign up for a time slot to learn more about the study and, if interested, provide informed consent and complete the intake survey. All timeslots were scheduled during school breaks or outside of hours when class is in session to avoid disruptions.
The only exception to the process was enrollment of one batch of recent graduates enrolled in Somalia. In this case, because students were no longer on campus when recruitment was being scheduled, the program director emailed each graduate to inform them about the study, and their contact information would be shared with study recruiters unless they opted out within a designated time period. Study team members then contacted each graduate to invite them to a telephone interview.
All students and graduates enrolled in both countries were female, which is to be expected as midwifery is a predominantly female profession in both countries.
Data collection instruments and procedures
A summary of quantitative data collection procedures is presented in Table 2, and summary of qualitative data collection procedures is presented in Table 3. Data collection instruments are available in Supplemental Material.
Cohort size and number of follow-up surveys planned by country.

Qualitative data collection planned by country.

FDGs: focus group discussions; IDIs: in-depth interviews.
Cohort intake and follow-up (tools A and B)
Written informed consent was obtained prior to commencing in-person data collection, and oral informed consent was obtained prior to commencing telephone surveys.
Structured student intake surveys (tool A) capture participants’ demographic characteristics, experiences during pre-service education (including any impacts of conflict and insecurity on their academic experience), their excitement and fears about becoming a midwife, and plans after graduation, as well as perspectives on public opinion about midwifery. The survey additionally integrates validated scales, such as the Perceived Stress Scale (PSS-14), which assesses psychological stress and burnout. 35 For follow-up surveys with continuing students, the same tool is used, and static demographic questions skipped to avoid repetition.
Follow-up surveys post-graduation (tool B) document participants’ employment status and location, clinical and administrative responsibilities, working conditions, support structures, challenges faced, job satisfaction, and physical health. Questions were incorporated and adapted from existing scales and instruments. These include the Nursing Incivility which assesses exposure to disrespect in nursing professional contexts 36 ; the Copenhagen Burnout Inventory, 37 used to measure personal, work-related, and client-related burnout; the Nursing Workplace Satisfaction Questionnaire, 38 which explores job satisfaction in healthcare settings; and the Nordic Musculoskeletal Questionnaire, 39 a standardized tool for assessing musculoskeletal symptoms related to occupational health.
Surveys are designed to take no more than 90 min to complete.
Focus group discussions (tools C and D)
Following each round of surveys, focus group discussions are conducted with a randomly selected sub-sample of current midwifery students (tool C) in each country, and sub-sample of recently graduated midwives (tool D) in each location.
Focus group discussions with students explore participants’ career plans, experiences as a student (including impacts of conflict on their academic experience), and recommendations to improve midwifery education programs. Focus group discussions with graduates explore challenges identified through intake and follow-up surveys, experiences in seeking or waiting for employment and working as a midwife, how personal and professional experiences affect career goals, and recommendations for improvement of working conditions and experiences.
Each focus group discussion is anticipated to last no more than 1 h, and no individual will be invited to participate in more than one group discussion. Discussions will be conducted in English, or the predominant local language (i.e., Hausa in Nigeria, Somali in Somalia).
In-depth interviews (tools E and F)
In addition, after each round of follow-up survey, in-depth interviews are conducted with a random sample of up to 10 midwives in each country who reported in the survey that they have withdrawn from a midwifery pre-service education program (tool E) or stopped practicing midwifery (tool F). Interviews with students withdrawing from midwifery programs ask about reasons for dropping out, personal plans, recommendations to improve the program, and impacts of conflict on their academic experience. Similarly, interviews with graduates who report they have stopped working as a midwife will ask about reasons for leaving their job, experiences working as a midwife, and recommendations for improvement of midwifery working conditions and experiences, with the aim of understanding the underlying reasons behind attrition of midwives. If we are unable to identify students or graduates who dropped out/quit, no interviews will be conducted.
Each interview is anticipated to take no more than 1 h. Interviews will be conducted in person in English, or the predominant local language (i.e., Hausa in Nigeria, Somali in Somalia).
Data management and processing
Survey data is collected using Kobo Collect software on tablet computers or mobile telephones (KoBo Toolbox, Cambridge, USA). Routine data management and quality checks are done in Stata 16 (StataCorp LLC, College Station, USA).
Audio recordings of in-depth interviews and focus group discussions are transcribed into English. Personal identifying information used for recruitment purposes will be destroyed upon completion of data collection (after last round of follow-up). All other study data and documentation will be retained in each country according to institutional and donor data retention policies. De-identified quantitative datasets will be made available in an open-access repository within 6 months of the final data collection round.
Maintaining the cohort
At baseline, each cohort member provides their mobile numbers, so the study team can contact them by phone in subsequent rounds of data collection. At each of the follow-up surveys, participants will be asked to verify or update their contact information. Between data collection rounds, various strategies will be used to support participant retention in the cohort, including (1) calling participants every 6 months to confirm contact information and continued interest in study participation, (2) sending personalized reminder emails and WhatsApp messages to individuals who do not respond to phone calls, and (3) transferring a modest amount of mobile data credit as a token of appreciation to each individual completing a survey. Participants may withdraw from the cohort at any time.
Data analysis
Cross-sectional analysis
Cross-sectional analysis of the data will be performed after each round, to ensure timely dissemination of study results, since waiting for the conclusion of longitudinal data collection will delay sharing of critical study findings. Additionally, round-by-round analysis will allow the research team to modify and make necessary additions to the qualitative study instruments, such as adapting questions based on emerging findings and probes for deeper interrogation of quantitative findings. After each round, the team will use descriptive statistics, namely measures of central tendency such as means, medians, and standard deviations and inter-quartile ranges, for continuous variables and frequencies for categorical variables.
We will compare point estimates using t-tests for continuous variables and chi-square tests for categorical variables. Particular attention will be paid to understanding differences across study variables between basic and community midwifery participants in Yobe, Nigeria as well as students in private versus public programs in Somalia. While all participants are considered midwives under the ICM definition, we will disaggregate findings by training pathway within each country to explore how differences in training type, duration, and deployment processes shape workforce entry, placement, and retention.
Longitudinal analysis
A central objective of the longitudinal study will be to quantify rates of program withdrawal during midwifery training and rates of attrition from the midwifery profession after graduation. Given the substantial contextual differences between the two settings, analysis will be conducted separately by country and will not be pooled. Cox regression models will be used to estimate hazard ratios for both training program withdrawal and professional attrition, along with corresponding 95% confidence intervals. These models will allow us to analyze time-to-event for key outcomes such as withdrawal from the midwifery program and exit from the workforce. We will also calculate the median survival time in the profession to identify when attrition is most likely to occur.
In addition to quantifying attrition, we will investigate risk factors for attrition, both during training and post-graduation. Independent variables will include students’ experiences of the educational program, including exposure to bullying, perception of insecurity, faculty support, stress and burnout, and perceived respect for the profession within the community, as well as characteristics of the workplace and experience of the profession, including whether midwives are expected to perform tasks outside their scope of practice, their salary, working conditions, exposure to workplace violence, and access to professional support systems and mentorship. These variables will be modeled using multivariable Cox regressions, which will be tested for the proportional hazards assumption. We will additionally explore potential interaction effects between independent variables (e.g., working conditions such as salary and availability of medicines and supplies interactions with community violence).
To assess potential attrition bias, we will compare baseline characteristics of participants in the cohort with those who were lost to follow-up, including demographic variables (such as origin governorate, age, marital status), academic performance, withdrawal intention, and other variables at baseline. Sensitivity analyses will be conducted to examine the robustness of findings under alternative assumptions about missingness (e.g., list-wise deletion vs. imputation methods). Longitudinal statistical analyses will be conducted using Stata software, version 16 (StataCorp LLC, College Station, USA) or greater. Reporting on quantitative analyses will be guided by the STROBE checklist for cohort studies. 40
Qualitative analysis
Our qualitative analysis will aim to capture the experiences and realities of midwifery students, particularly how they navigate conflict and violent insecurity as they pursue their education in volatile contexts like Nigeria and Somalia. We will additionally seek to capture the experience of midwifery graduates during the job search process and as they enter the midwifery workforce. The analysis will be grounded in a phenomenological approach, with the aim of characterizing the lived experience of midwives in conflict as they navigate intense upheaval, insecurity, and uncertainty, and how these experiences shape their professional identities and career trajectories.
We will employ a combination of deductive and inductive approaches to qualitative data analysis. Deductive coding will be guided by the research study’s main objectives and research questions. A codebook based on these pre-identified themes and ideas will be created and expanded iteratively with deeper analysis of the data. Emerging insights and themes will be captured through inductive codes, to preserve participants’ narratives. We will use techniques such as open-coding, line-by-line coding, and in vivo coding to remain faithful to participants’ experiences, language, and meaning. We will use methods such as the constant comparison method and searching for negative cases to maintain rigor of the analysis and will engage in memo-writing and team discussions to make sense of the data. Qualitative data analysis will be conducted using Dedoose software, version 9 or greater (SocioCultural Research Consultants, LLC, Los Angeles, USA). Reporting on qualitative analyses will be guided by the COREQ checklist. 41
Ethical considerations
Ethical approval was obtained from John Hopkins Bloomberg School of Public Health (IRB00024146), the Somali Research and Development Institute (SORDI-EA02 52), and Yobe State Health Ministry of Health Ethics Committee (MOH/GEN/747/VOL.I). Data collector trainings cover standard operating procedures for in-person and telephonic data collection in conflict-affected settings, including context-specific measures to ensure safety of study team members and participants and referral pathways available in case participants disclose or experience distress during data collection.
Discussion
This research will offer insights into a critical yet under-explored segment of the global health workforce: early career midwives in conflict-affected settings. As one strategy for promoting a primary healthcare approach for women’s, children’s, and adolescent’s health and well-being, WHO recommends transitioning health systems “away from fragmented risk-oriented models of care to midwifery models in which women and newborn receive equitable, person-centered, respectful, integrated and high-quality care by midwives working within collaborative interdisciplinary teams from pre-pregnancy through the postnatal period.” 42 Stakeholders see this as a cost-effective and financially sustainable strategy for improving maternal and newborn health, 43 yet recognize the wide disparities in the availability of nurses and midwives across regions and stagnating progress toward sustainable development goals.44,45
Health workforce strengthening efforts often prioritize recruitment, training, and deployment strategies, with less attention to challenges of transition from education to practice, or the social and professional conditions that support or undermine midwives’ ability to remain and thrive in the profession.11,46 Evidence-based guidance on how to attract, retain, protect, and support a growing midwifery workforce is particularly crucial in fragile and conflict-affected settings characterized by high stress, trauma, workforce turnover, and migration.15,16,28
Only a few longitudinal health workforce studies have been conducted in sub-Saharan Africa, and none in conflict-affected health systems. 47 The Ethiopia Health Worker Cohort Study enrolled 90 medical students and 219 nursing students in 2004 and followed them over time to generate evidence on career preferences, satisfaction and motivation, with a particular focus on choices between urban and rural posting and decisions to migrate abroad. 48 Similarly, the Wits Longitudinal Study to Determine the Operation of the Labour Market (WiSDOM) in South Africa, launched in 2017, follows eight health professional groups to examine career choices and job location decisions of health professional graduates of Wits University. The study is still ongoing and includes nurses but not midwives. 49
Strengths and limitations
To the best of our knowledge, this will serve as the first multi-country health workforce cohort study focused specifically on midwives in low-and-middle income countries, and the first in conflict-affected contexts. 42 Prospective cohort studies require long-term investments in research staff, infrastructure, and funding, which are rare in humanitarian settings 50 ; greater risks of cohort attrition and non-response bias threatening the representativeness of the study population and conclusions drawn are reasonable concerns, albeit not reasons to avoid research when the needs for evidence to guide program planning and resource allocation are high. 51 This study will serve as a proof-of-concept, demonstrating the feasibility of longitudinal health workforce research in conflict-affected areas of Nigeria and Somalia and providing an unprecedented source of evidence on lived realities and expressed needs for improving midwifery education, working conditions, and support networks in these settings.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261438787 – Supplemental material for Learning from the experiences of midwifery students and recent graduates in humanitarian and conflict-affected settings: A prospective cohort study protocol
Supplemental material, sj-docx-1-whe-10.1177_17455057261438787 for Learning from the experiences of midwifery students and recent graduates in humanitarian and conflict-affected settings: A prospective cohort study protocol by Hannah Tappis, Emilia Iwu, Hawa Abdullahi, Charity Maina, Asia Mohammed and Shatha Elnakib in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057261438787 – Supplemental material for Learning from the experiences of midwifery students and recent graduates in humanitarian and conflict-affected settings: A prospective cohort study protocol
Supplemental material, sj-docx-2-whe-10.1177_17455057261438787 for Learning from the experiences of midwifery students and recent graduates in humanitarian and conflict-affected settings: A prospective cohort study protocol by Hannah Tappis, Emilia Iwu, Hawa Abdullahi, Charity Maina, Asia Mohammed and Shatha Elnakib in Women's Health
Footnotes
Acknowledgements
The authors acknowledge this study would not be possible without the contributions of time and interest from participating midwifery pre-service education program leadership, students, and graduates. We are also grateful for the dedication of EQUAL Research Programme Consortium members at the Institute for Human Virology, Nigeria (IHVN), Somalia Research and Development Institute (SORDI), Johns Hopkins Center for Humanitarian Health, as well as to Alicia Adler at the International Rescue Committee for graphic design support.
Ethical considerations
Ethical approval was obtained from John Hopkins Bloomberg School of Public Health (IRB00024146), the Somali Research and Development Institute (SORDI-EA02 52), and Yobe State Health Ministry of Health Ethics Committee (MOH/GEN/747/VOL.I).
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by UK International Development from the UK government (PO 8613) as part of the EQUAL Research Programme Consortium
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data underlying this analysis will be made available on Figshare.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.