
Abstract
Background:
Endometriosis is a chronic disease that impacts an estimated 10% of women. It is characterized by endometrial glands and stroma growing outside the uterus. Surgery is a mainstay of diagnosis and treatment. Infection is a leading complication following minimally invasive surgery (MIS) endometriosis excision. Currently, there are limited data on antibiotic prophylaxis for these cases.
Objectives:
To study the utility of prophylactic antibiotic administration in postoperative infection prevention among women undergoing MIS for endometriosis.
Design:
This retrospective cohort study included patients who had MIS for endometriosis at a quaternary academic medical center between January 2016 and May 2023. Patients who received antibiotic prophylaxis were compared to those who did not. The primary outcome was the rate of postoperative infections in each group. Secondary outcomes included rates of unscheduled postoperative visits, readmissions, and reoperations.
Results:
Of the 729 patients included, 595 (81.6%) patients received antibiotics, and 134 (18.4%) did not. Among women who received antibiotics, endometrioma excision (36.5% versus 23.1%, p = 0.003), ureterolysis (38.0% versus 25.4%, p = 0.007), and concomitant myomectomy (43.5% versus 11.9%, p < 0.001) were more common. The proportion of stage IV endometriosis was higher among women who received antibiotics (22.7% versus 11.9%, p = 0.005). Estimated blood loss, surgery length, and hospital admission times were lower in the no-antibiotics group. There were no infections in the no-antibiotics group and 7 (1.2%) in the antibiotics group.
Conclusion:
Infectious complications were rare among patients undergoing MIS for endometriosis. The higher prevalence of infection among patients who received antibiotics likely reflects more severe endometriosis and higher surgical complexity in these cases. No infections in the no-antibiotics group suggest that prophylaxis may be safely omitted in simpler cases. A larger, prospective study is needed to investigate further the potential benefit of antibiotic prophylaxis in more complex endometriosis surgeries.
Introduction
Endometriosis is a chronic disease characterized by endometrial glands and stroma outside the uterus. 1 It affects approximately 10% of the female population, most commonly of reproductive age. 2 The most common clinical presentations are dysmenorrhea, infertility, and adnexal masses.1,3,4 In many cases, the chronic inflammatory nature of endometriosis significantly decreases patients’ quality of life. 3 Treatment of endometriosis includes medical and surgical options, and treatment decisions are based on symptom severity, disease extent, reproductive desire, surgical history, patient age, and more.1,3 Surgery is the fundamental tool for diagnosis and treatment, as it allows direct visual identification of lesions, excision of affected tissue, and pathologic diagnosis.1,3,5,6
Several publications have found an association between endometriosis and pelvic infections, both before and after surgery.7–16 Minimally invasive surgery (MIS), both laparoscopic and robotic, is the standard-of-care surgical approach for endometriosis cases. 17 Infection is a leading complication following MIS endometriosis excision, particularly for deeply infiltrating disease and cases involving the bowel.18–21 The pathogenic mechanisms leading to pelvic infection in patients with endometriosis may be the result of an increased inflammatory state, alteration of the pelvic microbiome, impaired immune response, and anatomy distortion favorable to bacterial proliferation.22–24
Currently, the American College of Obstetrics and Gynecology (ACOG) does not recommend antibiotic prophylaxis for gynecologic laparoscopic procedures that do not include entry into the bowel or the vagina. 25 This recommendation is based on a Society for Gynecologic Surgeons (SGS) meta-analysis that found no benefit for routine use of prophylactic antibiotics in such cases. The authors of the meta-analysis acknowledge, however, that the evidence to support this recommendation was poor, as it is based on only two small trials that were imperfect in design. 26
In light of the limited data on the subject, we aimed to study the effect of prophylactic antibiotic administration on postoperative infection prevention among women undergoing MIS for endometriosis.
Materials and methods
In this retrospective cohort study, we followed the STROBE checklist for design. We included all patients who had MIS (laparoscopic or robotic) for endometriosis with surgeons in the Division of Minimally Invasive Gynecologic Surgery (MIGS) at Cedars-Sinai Medical Center in Los Angeles, California between January 2016 and May 2023 in a quaternary, urban, academic, community-based medical center. Patients of three different surgeons, all trained in various AAGL Fellowships for MIGS, were included. We excluded cases with concurrent hysterectomy, colpotomy, and bowel resection, including appendectomy. Patients with malignancy, preexisting pelvic infection, or those with incomplete records were also excluded.
Patients were selected for antibiotics solely at the discretion of the surgeon. Generally, antibiotics are administered in cases with known risk factors for infection, including suspected severe endometriosis. While this is the general practice, there is no standard guideline followed by the surgeons, and each surgeon varies in practice. Patients who received prophylaxis were administered intravenous antibiotics in the operating room prior to anesthesia induction or intraoperatively at the surgeon’s discretion, with a target for administration prior to skin incision. Antibiotic choice was largely based on current recommended regimens for hysterectomy, including cefazolin 2gm and appropriate alternatives for those allergic to it. In some cases where appendectomy was a possibility, cefoxitin was administered as an alternative to cefazolin or in addition to cefazolin, as it is recommended for prophylaxis in appendectomy. All patients underwent perineal-vaginal preparation with povidone-iodine solution (in rare cases of allergy, a dilute chlorhexidine preparation was used) and abdominal preparation with chlorhexidine gluconate and isopropyl alcohol.
Pre-, intra-, and post-operative characteristics were collected from the electronic medical record for all patients included. Pre-operative variables collected included basic demographic information: age, body mass index (BMI), drug use, smoking status, American College of Anesthesiologists classification, race, and ethnicity. Intra-operative characteristics included the type of prophylactic antibiotics used, surgical procedures performed, endometriosis stage, intra-operative complications, estimated blood loss (EBL), surgery length, and hospitalization length. Post-operative variables included any infectious or non-infectious complications, emergency room visits, readmissions, and reoperations within 30 days of the surgery. Individual chart review included the use of the “care everywhere” feature, allowing for the review of charts from outside facilities using the same electronic medical record, which includes many outside hospitals and urgent cares in the region.
We categorized surgical site infections according to the CDC/NHSN surveillance definitions, including the following: superficial incisional, deep incisional, and organ/space. 27 Superficial incisional infections are those that involve the skin and subcutaneous tissue at the incision. Deep incisional infections involve deeper layers, including the muscle and fascial layers. Organ/space infections included pelvic tissue infections, such as those of the uterus or adnexa, as well as pelvic abscesses. Urinary tract infections were reported separately. We further delineated major and minor post-operative complications based on the Clavien-Dindo classification system. 28 The endometriosis stage was classified using the revised American Society for Reproductive Medicine scoring system. 29
Study participants were divided into two cohorts according to receipt of prophylactic antibiotics. The primary outcome was the occurrence of any post-operative infection within 30 days of surgery. Secondary outcomes included rates of unscheduled postoperative visits, readmissions, and reoperations.
Statistics analysis
We compared patients who received prophylactic antibiotics to those who did not using chi-square test and Fisher’s exact test for categorical variables and Mann–Whitney U test for continuous variables, after normality was tested. Categorical variables were reported as proportions and continuous variables as medians and interquartile ranges. We performed a sub-analysis for cases of patients with stage IV endometriosis. A two-sided p-value of <0.05 was considered statistically significant. Statistical analyses were performed using Software Package for Statistics and Simulation (IBM SPSS version 27; IBM Corp, Armonk, NY, USA).
Ethical approval
This study was conducted according to good clinical practice guidelines and was approved by the Institutional Review Board (IRB #2382). Due to the retrospective nature of the study, a waiver for informed consent was accepted.
Results
A total of 729 patients were analyzed, 595 (81.6%) in the antibiotic group and 134 (18.4%) in the no-antibiotic group (Table 1). Baseline characteristics were comparable between groups except for age, smoking status, and race. Patients who did not receive antibiotics were younger, were more commonly smokers, and were more commonly of White race, compared with patients who did receive antibiotic prophylaxis.
Baseline and operative characteristics.

Data are n (%) or median [interquartile range]. ASA: American College of Anesthesiologists.
Antibiotic regimens used are summarized in Table 1. In 63/595 cases (10.6%), more than one agent was administered. Of these, 53 cases had cefoxitin added to cefazolin, and the rest were other combinations.
Among women who received antibiotics, endometrioma excision (36.5% versus 23.1%, p = 0.003), ureterolysis (38.0% versus 25.4%, p = 0.007), and concomitant myomectomy (43.5% versus 11.9%, p < 0.001) were more common. The proportion of stage IV endometriosis was higher among women who received antibiotics (22.7% versus 11.9%, p = 0.005). The no-antibiotics group had lower EBL, surgery length, and hospital admission times.
There were no infections in the no-antibiotics group and 7 (1.2%) in the antibiotics group (Table 2). Superficial incisional skin infections occurred in 3 (0.5%) cases, and organ/space infections occurred in 3 cases (0.5%) in the antibiotics group. There were no significant differences in other intraoperative or postoperative complications, including readmissions or reoperations. When comparing infection rates according to the type of antibiotics administered, comparable rates were found (p = 0.819).
Surgical outcomes and complications.

Data are n (%).
In a sub-analysis of cases of stage IV endometriosis only, 16 patients did not receive antibiotics, and 135 patients received antibiotics. Three (2.2%) infections occurred, all in the antibiotics group (Table 3).
Infections in patients with stage IV endometriosis undergoing minimally invasive surgery for endometriosis.
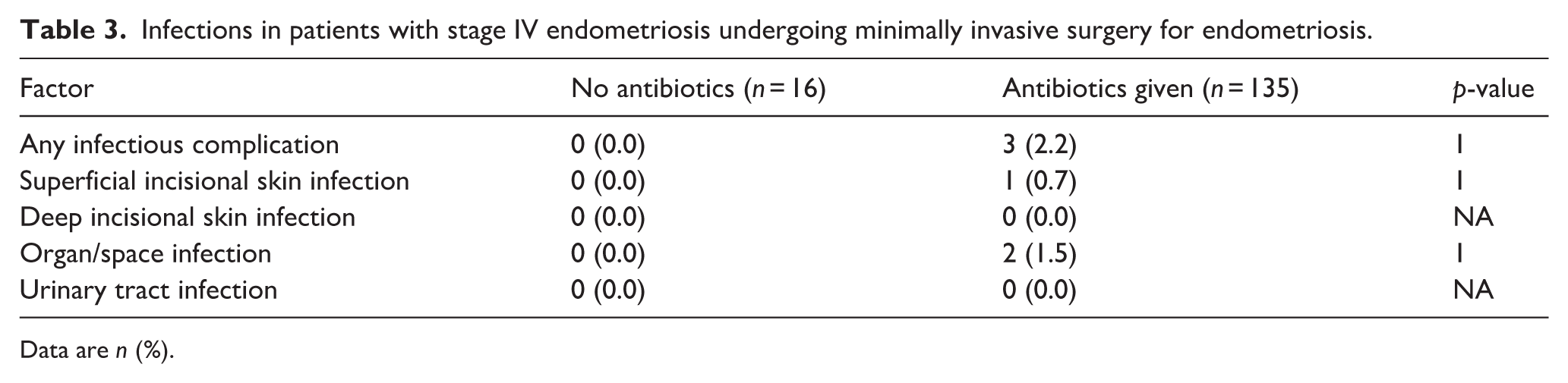
Data are n (%).
When comparing variables that differed between the two study groups, including patient age, race, laparoscopic myomectomy, EBL, surgery time, and total hospital time, none was associated with infection rates.
Discussion
The majority of patients undergoing laparoscopy for endometriosis received antibiotic prophylaxis. There were no infections in the no-antibiotics group and very few in the antibiotics group. Patients who underwent concomitant endometrioma excision, ureterolysis, and myomectomy received antibiotics more frequently. Patients who had more severe endometriosis were more prevalent in the antibiotics group. EBL, surgery length, and hospital admission length were lower in the no-antibiotics group, proxies for surgical complexity. Among patients with stage IV endometriosis, all infections occurred in the antibiotics group.
Antibiotic prophylaxis comprises a brief course of antimicrobials, usually initiated before the start of surgery. They are used to decrease intraoperative microbial contamination and ultimately reduce post-operative infections.6,25 Some infections, especially superficial surgical site infections, may be caused by postoperative contamination and are not addressed by prophylaxis. Although generally safe, physicians should avoid overuse of antibiotics given the risk of bacterial antibiotic resistance and other adverse reactions.6,25 Identifying cases with a genuine need for antibiotic prophylaxis is thus critical to perioperative care.
Patients with endometriosis have altered microbiomes, likely stemming from a chronic inflammatory state.23,30 Recent literature suggests microbiome variations, including certain bacterial mutations, may be associated with the development of endometriosis.31–34 Additionally, patients with endometriosis likely have impaired immune responses, potentially impacting their ability to fight infections. 22 Evidence continues to accumulate, noting an association between endometriosis and pelvic infections outside of surgery.7–10 This increase in infection risk outside of surgery, coupled with infection being reported as a leading complication of MIS for endometriosis, 18 further emphasizes the importance of studying the prevention of infection at the time of endometriosis surgery.
ACOG’s antibiotic prophylaxis recommendations for gynecologic laparoscopy are based almost solely on a 2013 SGS meta-analysis that includes only two non-hysterectomy randomized controlled trials.25,26,35,36 One found no differences in infections among 356 patients undergoing gynecologic laparoscopy with either amoxicillin–clavulanate or cefazolin pre-operative antibiotic prophylaxis. 35 The second randomized 450 women to pre-operative antibiotic prophylaxis with a first-generation cephalosporin or no antibiotics. 36 Both of these studies were noted to be of poor quality, with low infection rates at 0%–5.5%.35,36
The overall infection rate in our population was 1.2%, which is lower than most previous studies reporting rates ranging from 4.7% to 5%.18,19 Our infection rate for patients with stage IV endometriosis group was 2.2%, and only occurred in the antibiotic group. This is also lower than prior reports. An Italian study noted 52 infections among the 927 patients (5.6%) who underwent radical excision of stage IV endometriosis without concomitant bowel surgery. The authors did not comment on antibiotic usage. These differences may be explained by surgeons’ targeted use of antibiotics in this study, as surgeons likely preferentially chose to administer antibiotics in more severe cases of endometriosis.
The surgeons in the MIGS Division provide a benign gynecologic surgical consultation service in the region, including an endometriosis center. In our population, the severity of endometriosis and, therefore, surgical complexity tends to be high. This referral bias likely explains the relatively low proportion of patients not receiving antibiotics.
Our results indicate that surgeons tended to give antibiotics more frequently in more complex and severe cases. Patients who received antibiotics had more severe endometriosis and higher surgical complexity, likely causing a higher prevalence of infection despite antibiotic prophylaxis. Given that there were no infections in the no-antibiotics group, it may be that surgeons were accurately selecting appropriate antibiotic use based on complexity. We can’t be certain, however, since the rationale for using antibiotics or not wasn’t documented, and it may be reflective of surgeons’ general practice as well. The results suggest that antibiotic prophylaxis may be safely omitted in simpler cases. However, further prospective studies are needed to confirm these findings.
The more complex and severe cases that largely comprised the antibiotics group in this study may have had an even higher infection rate had they not received antibiotic prophylaxis. This hypothesis cannot be adequately addressed within the methods of the current study. Similarly, the association between concomitant procedures, including myomectomy, adenomyomectomy or bladder surgery and infection risk could not be accounted for in the present study. A more extensive, preferably multicenter, randomized study is needed to adequately power and further investigate the potential benefit of antibiotic prophylaxis in more complex endometriosis surgeries.
Following a meticulous literature review, we did not identify another study evaluating the impact of prophylactic antibiotics for endometriosis surgery. This constitutes the main strength of our research. The granularity of the collected data is another strength.
Limitations
Several limitations should be acknowledged. Every retrospective study introduces potential bias through missing data and not evaluating factors that may have affected the results despite meticulous electronic medical record review. Individual review included the use of the “care everywhere” feature in the electronic medical record to include patients who sought care at thousands of outside hospitals. So, while recall bias surely affects all retrospective studies reviewing complications to some degree, we believe the effect is minimal in this study.
Data were sourced from a single center in an urban area where patients tend to be of higher socioeconomic status, limiting the study’s generalizability. More specifically, our population had few smokers or patients with elevated BMI, both risk factors for infection. Thus, our infection rates may be lower than those in a more general population. 25 Additionally, the study was performed at an endometriosis referral center within a single tertiary/quaternary referral center with high-volume fellowship-trained endometriosis surgeons, reflecting a population with more complex disease, cared for by highly specialized surgeons, further limiting generalizability. Finally, the analysis was limited by a relatively small number of infections among both groups. The convenience-based sample size and the limited number of outcomes limit the statistical power to detect differences between groups and draw conclusions. Additionally, a multivariable regression analysis, to adjust for potential confounders, was not possible, as it would have resulted in overfitting. For patients with Stage IV endometriosis included in the sub-analysis, only a minimal number of women didn’t receive prophylactic antibiotics, limiting the strength and reliability of this sub-analysis. Therefore, the absence of infections in this subgroup is not sufficient to draw conclusions.
The lack of infection in patients in this study undergoing minor endometriosis surgery without antibiotic prophylaxis suggests this practice may be safely avoided in these cases, consistent with ACOG guidelines. However, a higher rate of infection among more advanced endometriosis cases in general and a lower infection rate in this cohort compared to previous reports of infection may indicate a potential benefit of antibiotic prophylaxis in this population. Given these findings and that data currently guiding recommendations on antibiotic prophylaxis for benign gynecologic surgery is based on two nearly 20-year-old RCTs that did not focus on any particular surgery or pathology, it is undoubtedly time this topic is readdressed in a more focused fashion. As the type and extent of laparoscopic surgeries for endometriosis evolve, so should our evidence. Acknowledging the limitations of our analysis, and in the absence of high-quality data to the contrary, we believe the benefits of prophylactic antibiotics outweigh the risks in surgery for complex endometriosis and that our data support recommending use in these cases.
Conclusions
Infectious complications were rare among patients undergoing laparoscopy for endometriosis. The higher prevalence of infection among patients who received antibiotics likely reflects more severe endometriosis and higher surgical complexity in these cases. The absence of infections in the no-antibiotics group suggests that current ACOG guidelines are likely appropriate in this population. However, this retrospective study highlights the need for more extensive prospective investigation of the potential benefit of antibiotic prophylaxis in endometriosis excision surgeries to better understand appropriate use.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261426914 – Supplemental material for The effect of prophylactic antibiotic administration for endometriosis surgery
Supplemental material, sj-docx-1-whe-10.1177_17455057261426914 for The effect of prophylactic antibiotic administration for endometriosis surgery by Kacey M. Hamilton, Raanan Meyer, Rebecca Schneyer, Kelly N. Wright and Matthew T. Siedhoff in Women's Health
Footnotes
Acknowledgements
We would like to thank the Cedars Sinai data specialists for their assistance in obtaining and matching data for this study.
Author note
Ethical Considerations
This study was conducted according to good clinical practice guidelines and was approved by the Institutional Review Board (IRB #2382).
Consent to participate
Due to the retrospective nature of the study, a waiver for informed consent was accepted.
Consent for Publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kacey Hamilton: Consultant for Intuitive.
Raanan Meyer: Consultant for Intuitive.
Rebecca Schneyer: Consultant for Ethicon and Intuitive.
Kelly N. Wright: Consultant for Aqua Therapeutics, Hologic, Ethicon, Karl Storz.
Matthew T. Siedhoff: Applied Medical Consultant.
The remaining authors report no conflict of interest.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.