
Abstract
Background:
Postpartum physical activity (PA) is crucial in supporting maternal health, contributing to mental health and well-being, weight management, and overall physical fitness. Although multiple health organizations have issued PA recommendations for postpartum women, the content and quality of these guidelines have not yet been systematically evaluated.
Objectives:
To evaluate the quality of published guidelines on PA for postpartum women and to summarize their recommendations to provide clearer guidance for healthcare providers and postpartum women.
Design:
Systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources and methods:
Six electronic databases were searched for guidelines related to PA for postpartum women. Gray literature was also reviewed. Guidelines were included if they were developed by recognized health organizations, provided PA (including structured supervised exercises) recommendations for postpartum women, and were published or updated within the last 10 years. Data extraction and quality appraisal were independently conducted by pairs of reviewers using the Appraisal of Guidelines Research and Evaluation Tool (AGREE II).
Results:
Eighteen guidelines were included, with AGREE II scores ranging from 50% to 92%. Seven guidelines (39%) met the criteria for satisfactory methodological quality. Most guidelines recommended that postpartum women engage in at least 150 min of moderate-intensity aerobic PA per week, while the 2025 Canadian guideline supports a minimum of 120 min based on meta-analytic evidence. Common recommendations included pelvic floor muscle training, strengthening exercises, and other exercises, with advice to seek healthcare guidance for women with special conditions.
Conclusion:
There is a universal agreement across guidelines that postpartum women should aim for at least 120–150 min of moderate-intensity PA weekly. Future research should strengthen the evidence for specific types of PA, delivery mode considerations, and implementation strategies.
Registration:
International Prospective Register of Systematic Reviews: PROSPERO (CRD42023447331).
Introduction
The promotion and successful implementation of maternity healthcare have significantly improved maternal and perinatal outcomes in recent decades.1,2 Traditionally, the focus has been on providing care for women during pregnancy, labor, and delivery, with comparatively less attention given to the postpartum period.3,4 Studies have shown that more than 50% of women experience diverse and impactful health problems following childbirth, ranging from physical complications such as urinary incontinence to mental health issues such as depression and fatigue. 5
The postpartum period begins immediately after the birth and extends from 6 weeks to 12 months.6,7 During this period, women face significant challenges related to hormonal and physiological changes, physical recovery from childbirth, and often disrupted sleep associated with caring for a newborn.8,9 These factors can collectively affect women’s physical and mental health during the postpartum period. Importantly, the postpartum period is associated with increased health risk, as more than 50% of maternal deaths occur after childbirth. 10 Insufficient postpartum care may lead to serious consequences, including postpartum depression, which is associated with a higher risk of hospitalization and death in the first year after delivery.10–12 Therefore, postnatal care plays a critical role in supporting women’s mental and physical health and promoting optimal postpartum recovery and well-being. 13
Physical activity (PA) is defined as any bodily movements produced by skeletal muscles that require energy expenditure, 14 while exercise refers to activities requiring physical effort to improve or maintain physical fitness. 15 In this review, we used the term PA in line with how most guidelines apply it, which primarily referred to structured or planned exercise rather than general lifestyle activity. The benefits of PA during pregnancy are well established and include reduced risks of gestational diabetes, excessive gestational weight gain, hypertension, pre-eclampsia, depression, and anxiety.16,17 Evidence also suggests that PA during the postpartum period can reduce postpartum depression, promote weight control, and improve emotional and physical well-being.18–20
Guidelines for pregnancy and the postpartum period play a critical role in promoting the health and well-being of both mothers and babies. The World Health Organization (WHO) and country-specific guidelines, such as the USA, the UK, Brazil, and Australia, have issued recommendations for PA during pregnancy and highlighted the importance of PA for women during the pregnancy and postpartum period.18–21 These guidelines commonly promoted activities such as walking, yoga, swimming, and strength training, and generally recommended 150–300 min of moderate-intensity aerobic PA per week.18–21 However, studies have indicated that most postpartum women do not meet the recommended PA levels.22,23 Contributing factors include limited time, lack of social support, and insufficient clarity regarding safe and practical postpartum programs.24,25 Integrating guidelines for postpartum PA recommendations is crucial to ensure comprehensive care and promote holistic healthcare throughout the reproductive journey. Inconsistent guidance across guidelines may also contribute to confusion among postpartum women and healthcare professionals.26,27
Previous reviews conducted by Evenson et al.25,28 have synthesized international postpartum PA guidelines summarizing the content of recommendations. However, these reviews did not systematically appraise the methodological quality of the guidelines. This review extended this work by comprehensively evaluating both the content and quality of postpartum PA guidelines by using the Appraisal of Guidelines Research and Evaluation Tool (AGREE II). Therefore, this review aimed to clarify current PA recommendations and highlight differences in rigor, provide guidance for clinicians, researchers, and policymakers to strengthen evidence-based support for postpartum women.
Methods
This systematic review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 29 The protocol for this systematic review was registered in PROSPERO (CRD42023447331) and is available at http://www.crd.york.ac.uk/prospero. No institutional ethics approval was required.
Data sources and searches
Six electronic databases were searched using keywords related to “PA” or “exercise,” “postpartum” and “guideline.” Searches were conducted on Medline via Ovid (1946–present), Embase, Maternity and Infant Care, Web of Science, Scopus, and Cinahl Complete from their inception to August 15th, 2023, and updated on June 24th, 2025 (see Supplemental File 4 for details). Gray literature was searched with Google Scholar, including the first 250 articles. Database searches were supplemented by manual searches of reference lists of included studies and published systematic reviews relevant to this study. No language restrictions were applied. The full search strategy is presented in Supplemental File 1.
Guideline selection
Two reviewers (QL and JC) independently screened titles, abstracts, and full texts to identify potential studies based on predefined inclusion and exclusion criteria using the Covidence software (Veritas Health Innovation, Melbourne, VIC, Australia). Any disagreements were resolved through consensus or by consulting a third reviewer (YT). Authors were contacted for additional information when necessary. For guidelines published in languages other than English, we sought an official English version. If none was available, we used Google Translate or artificial intelligence as an initial tool and then consulted health professionals fluent in the relevant languages to ensure accuracy.
Guidelines were included if they satisfied all the following criteria:
Produced under the auspices of a health professional association or society, a public or private organization, a healthcare organization or plan, or a government agency.
Contained systematically developed statements including recommendations, strategies, or information to guide decisions about PA for women during the postpartum period in both postpartum-specific guidelines and guidelines for the general population.
Published or updated within the previous 10 years (including the year of 2014).
Provided PA recommendations for women during their postpartum period.
Guidelines were excluded if they:
Were not evidence-based clinical practice guidelines, such as guidelines based solely on consensus without an explicit literature search.
Did not provide PA recommendations for postpartum women.
Data extraction
Pairs of reviewers (QL and JC, QL and YT) independently extracted all available data using tables that captured the general guideline information (title, country, organization or society, publication year, methods for guideline development, assessment of the strength of evidence, and conflict of interest). They also extracted details on the benefits of PA for postpartum women, and PA recommendations, including types of PA, timeframe for initiating PA, and recommended duration and intensity of PA (see Supplemental Files 2.1–2.4 for details). Any disagreements were resolved through consensus or consulting a third reviewer (YT or JC).
Quality appraisal
The quality appraisal for included guidelines was conducted by pairs of reviewers (QL and JC, QL and YT) independently using the AGREE II instrument. 30 Any disagreements were resolved by consensus or a third reviewer (YT or JC). All the reviewers need to complete the AGREE II Online Training (http://www.agreetrust.org/resource-center/agree-ii-training-tools/) before conducting the quality assessment. The AGREE II instrument consists of 23 items categorized into six domains, including (1) scope and purpose; (2) stakeholder involvement; (3) rigor of development; (4) clarity of presentation; (5) applicability, and (6) editorial independence, followed by two global rating items (“Overall Assessment”). Each item is scored on a 7-point scale (1 = strongly disagree to 7 = strongly agree). Domain scores are automatically calculated by summing up the scores of the individual items in a domain and by scaling the total as a percentage of the maximum possible score for the domain (obtained score − minimum possible score)/(maximum possible score − minimum possible score). 31 Following the scoring recommendations on the AGREE II instrument, there has not set minimum domain scores or patterns of scores across domains to differentiate between high quality and poor quality. 31 Thus, in this study, to achieve a “satisfactory” quality guideline had to score at least 50% on all 6 domains, and an average score of more than 60% in each domain was considered as a good score.32–34
Results
Characteristics of guidelines
A total of 11,921 articles were identified from the electronic database search, and additional sources (e.g., reference lists and Google Scholar). After excluding duplicates and screening titles, abstracts, and full texts, 18 guidelines were retrieved in this review (Figure 1).

The PRISMA flow diagram for databases, registers, and gray literature.
For the included guidelines, two were conducted by the WHO7,18; two were from Australia35,36; one each was from Austria 37 , Brazil 19 ; Brunei 38 ; Canada 39 ; Qatar 40 ; the Republic of Kenya 41 ; Singapore 42 ; Sri Lanka 43 ; Sweden 44 ; Switzerland 45 , and the UK 46 ; and three were from the USA.20,47,48 Among the 18 guidelines, 16 were published in English, one in Swedish, and one in German. Thirteen guidelines (73%) focused on PA for the general population, including both pregnant and postpartum women as special populations within these guidelines. A total of five guidelines (27%) were specific to PA for pregnant and postpartum women. The main characteristics of the included guidelines are shown in Table 1.
Main characteristics.

NR: not reported; COI: conflict of interest.
The USA, 2018* guideline is: 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, 2018.
Quality appraisal of guidelines
The results of the guideline appraisal based on the AGREE II tool assessment are provided in Table 2. The guideline developed by WHO scored the highest with 92%. 7 The overall quality of the 18 guidelines ranged from 50% to 92%. Quality was also assessed through the six domains: scope and purpose ranged from 69% to 100% (average 83%), stakeholder involvement ranged from 42% to 100% (average 74%), rigor of development ranged from 23% to 94% (average 59%), clarity of presentation ranged from 56% to 90% (average 69%), applicability ranged from 21% to 85% (average 50%), and editorial independence ranged from 25% to 100% (average 55%). Seven of the 18 guidelines (39%) were of satisfactory methodological quality,7,18,36,39,46,47,49 based on the criteria set out in the AGREE II tool.
AGREE II assessment results.
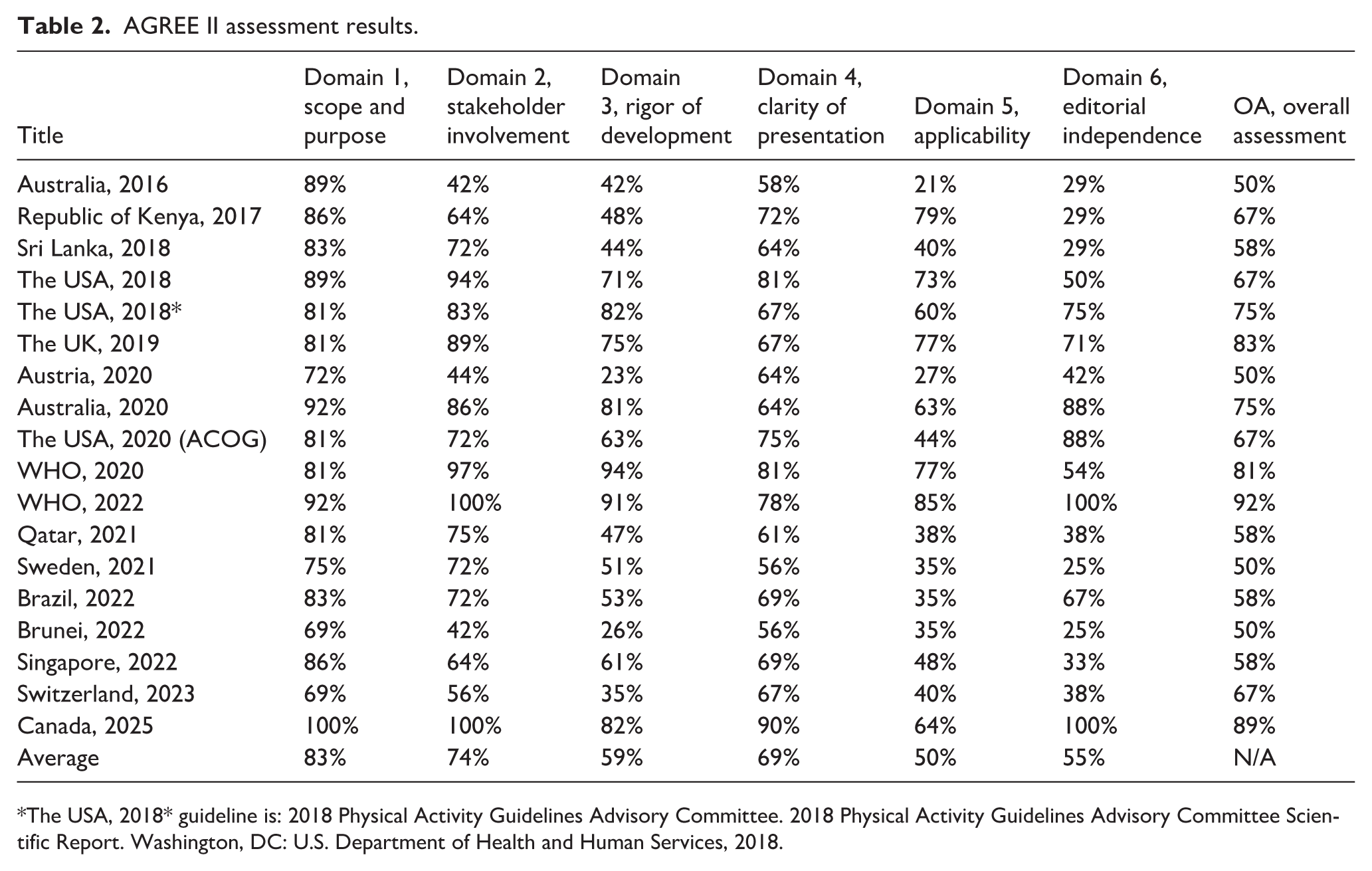
The USA, 2018* guideline is: 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, 2018.
Recommendations for PA
Most guidelines (88%) recommended that healthy women should engage in at least 150 min of moderate-intensity aerobic PA per week during the postpartum period. Furthermore, 15 guidelines (83%) suggested that postpartum women should engage in a variety of different PA (e.g., pelvic floor muscle exercise, strengthening exercise, or stretching exercises) as part of their PA program.7,18–20,35–42,44–46 Additionally, nine guidelines (53%) proposed that any amount of PA is better than none for postpartum women, particularly for those unable to meet the recommended 150 min/week.7,18,19,35,37,40,42,45,46 Additional details are provided in Supplemental File 2.2.
Safety and contraindications
Although all included guidelines recommended that postpartum women without contraindications should engage in at least some level of PA, most guidelines did not provide a comprehensive list of contraindications. Instead, most guidelines advised postpartum women to seek guidance from healthcare professionals before resuming PA.7,18,35,36,38–43,48–50 Notably, the 2025 Canadian guideline uniquely provided a structured list of contraindications and precautions to guide safe postpartum PA engagement. 39
Frequency, duration, and intensity of PA
Most of the guidelines (82%) suggested that PA should be performed throughout the week and could be divided into 2–3 times per week. Nearly all guidelines endorsed the goal of accumulating at least 150 min of moderate-intensity PA weekly. Nine guidelines (69%) suggested that light-intensity PA or some amount of PA is better than none.7,18,19,35,37,40,42,45,46
Type of PA
Most of the guidelines recommended that aerobic (94%),7,18–20,35,37–46,48,49 and pelvic floor muscle exercises (67%) should be performed.18–20,35–37,39,40,42,44–46 Strengthening (56%)7,18,37–40,42,44–46 and stretching exercises (41%)7,18–20,38,41,42 were identified as a general recommendation for postpartum women, followed by other exercises such as Yoga or Pilates (24%).7,19,42,45 Additional details are provided in Supplemental File 2.3.
Delivery type and PA
Less than 35% of guidelines indicated that return to PA should differ according to delivery mode. Guidelines from Australia and the USA suggested that the mode of delivery should be considered when resuming PA postpartum.20,21,35 The Austrian guideline recommended gradual resumption of PA from 4 to 6 weeks after vaginal delivery, while the Qatar guideline suggested that PA should gradually resume from 4 to 8 weeks after vaginal delivery, and 8 to 12 weeks after cesarean delivery.37,40
PA in previously active women
More than 50% of the guidelines suggested that women who were active before pregnancy and who engaged in vigorous-intensity aerobic activity before and during pregnancy could continue with their activity level postpartum. 47 Some guidelines (35%) suggested that women who were physically inactive before birth should gradually increase their level of PA postpartum. Almost 50% of guidelines recommended that postpartum women should seek advice from healthcare providers if they are unsure about which type of PA they should engage or if they have any special conditions.7,35,36,38,39,41,47
Initiation of PA
Pelvic floor muscle exercises were recommended to be performed immediately after birth by four guidelines.19,20,37,44 Three guidelines suggested that postpartum women should resume moderate-intensity PA gradually after 4–8 weeks postpartum.37,40,46 Although the 2025 Canadian guideline did not specify a start time for pelvic floor muscle training, it recommended performing pelvic floor muscle exercises daily during the first year postpartum. 39
Proposed therapeutic effects of PA
The most frequently reported benefits for postpartum women included alleviation of postpartum depression (61%),19,21,35,36,38–40,42,45–47 weight management (47%),19,35,40–42,44,46,47 enhancement of emotional well-being (24%),19,35,40,46 and improvements in physical fitness (39%).19,20,35,39,41,42,46 Reduced risk of urinary incontinence (17%).18,21,39 Additional details are provided in Supplemental File 2.4.
Discussion
This review identified 18 guidelines, consensus statements, and position papers published between 2016 and 2025 that provide recommendations on PA for postpartum women. Across all guidelines, there was a consistent agreement that women without contraindications should engage in regular PA during the postpartum period. Nearly half of the guidelines advised seeking healthcare consultation before resuming PA in the presence of special conditions.
Although previous systematic reviews of PA guidelines for postpartum women have summarized general recommendations on PA,25,28 this is the first systematic review that comprehensively applied a methodologically rigorous analysis of the 18 guidelines across six domains. Although most guidelines performed well in terms of scope and clarity, methodological rigor, applicability, and editorial independence were frequently weaker. These findings align with previous evaluations of clinical practice guidelines in other health domains.51–53
Only 7 of the 18 guidelines (39%) achieved satisfactory methodological quality.7,18,36,39,46,47,49 Many guidelines lacked practical details on implementation (e.g., facilitators, barriers, or resource implications). This limitation may contribute to the persistent gap between guideline recommendations and real-world uptake by healthcare providers.54–56 While low AGREE II scores may affect guideline usability, challenges in implementation are also influenced by broader contextual factors such as limited time, competing clinical priorities, and variability in postpartum women’s individual needs. 39
With respect to delivery mode, less than 30% of guidelines provided delivery-specific guidance for postpartum PA. This limited coverage likely reflects gaps in the available evidence regarding mode-specific PA safety and progression, rather than shortcomings in guideline development itself. Similarly, although aerobic activity was consistently recommended, fewer guidelines provided specific direction regarding strengthening, stretching, and pelvic floor muscle training progression.
Most guidelines conceptualized PA primarily as structured or planned exercise, with limited inclusion of lifestyle or household activities. Our review adopted this definition to remain consistent with the included guidelines. However, this narrow focus may limit the applicability of recommendations to the lived realities of postpartum women. Future guidelines should consider incorporating broader domains of PA and provide more practical, individualized recommendations.
Implications for future research
Clinical guidelines consistently recommend that healthy postpartum women engage in at least 120–150 min of moderate-intensity PA per week, with benefits including improvements in mental and physical health, weight management, and urinary incontinence.18,36,39,46 However, translating these recommendations from guidelines into the real world remains challenging. Most guidelines provide only general recommendations on duration and intensity, with limited attention to the impact of mode of delivery, pelvic floor health, or the optimal timing for initiating PA postpartum. While aerobic activity is relatively well studied, evidence on other modalities, such as strengthening and stretching, remains scarce, and few guidelines address lifestyle or household activity.
Future research should therefore evaluate the safety and effectiveness of different PA modalities, determine optimal frequency, intensity, and progression, and compare supervised versus unsupervised programs. More tailored recommendations based on delivery mode, pelvic floor status, recovery trajectory, and women’s individual circumstances should be investigated. In addition, implementation research is urgently needed to address the persistent gap between guidelines and real-world uptake by identifying barriers and facilitators from both healthcare professionals’ and postpartum women’s perspectives. Developing practical supports such as counseling resources, referral pathways, or digital tools will be critical to enhancing the applicability and usability of future guidelines.
Strengths and limitations
We applied comprehensive methods in conducting searches, screening, selection, and quality appraisal to ensure the representativeness and scientific rigor of our results. However, several limitations should be acknowledged. First, we only searched for several databases and Google Scholar; some recommendations from resource-limited countries may not be included due to the inability to access their databases. Second, although the AGREE II tool has been widely used, it has its own limitations, such as the fact that the instrument does not set criteria for domain scores to distinguish high, moderate, or low-quality, and it only focuses on the methodological quality of guidelines rather than clinical appropriateness and feasibility. 57 As this review focused on guidelines rather than primary studies, traditional risk of bias assessments were not applicable. Nonetheless, we addressed potential sources of bias by using AGREE II to systematically appraise methodological quality. Third, by including both postpartum-specific guidelines and general population guidelines that include postpartum, we may have diluted specificity; however, this approach was necessary to avoid excluding widely used sources if advice. Finally, publication bias may also be present, as guidelines that are unpublished or informally distributed may not have been missed.
Conclusion
PA during the postpartum period is associated with a wide range of health benefits for women. Most high-quality guidelines recommend that postpartum women without contraindications engage in regular moderate-intensity aerobic PA each week, with minimum recommended volumes ranging from 120 to 150 min. Commonly recommended activities include aerobic exercise, pelvic floor muscle training, strengthening training, and stretching. However, detailed guidance regarding the optimal timing for initiating different types of PA, progression strategies, and delivery mode-specific recommendations remains limited. Future research should focus on strengthening the evidence base for these aspects and on developing more implementation-focused guidance to support healthcare professionals and postpartum women in safely and effectively engaging in PA.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261421734 – Supplemental material for Physical activity postpartum: A systematic review and quality appraisal of clinical guidelines
Supplemental material, sj-docx-1-whe-10.1177_17455057261421734 for Physical activity postpartum: A systematic review and quality appraisal of clinical guidelines by Qianwen Lan, Allan Chak Lun Fu, Marnee J. McKay, Milena Simic, Josielli Comachio, Ye Tian and Paulo Ferreira in Women's Health
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Kanchana Ekanayake, the academic liaison librarian at the Medicine and Health University Library, for her invaluable guidance in developing the search strategy for this research.
Ethical considerations
There is no need for ethical approval and consent to participate as this is a systematic review.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.