
Abstract
Background:
Due to minimal effects, new directions for behavioral (non-pharmacologic/non-surgical) obesity interventions are required. Previous research suggests that physical activity and exercise (PA/exercise) might have considerable merit for weight reduction via impacts on mood and other psychosocial correlates of controlled eating. Although as few as 3 bouts/week of low-moderate intensity PA/exercise are associated with improved mood—with no dose–response effect beyond that frequency—it is unknown if mood improvements may be leveraged when participants already complete ⩾3 bouts/week by treatment start.
Objectives:
The present research addressed gaps in the available PA/exercise–psychosocial change–weight management research.
Design:
This study combined group contrasts with mediation analyses.
Methods:
Women participating in a community-based cognitive-behavioral obesity treatment emphasizing the increase of PA/exercise and exercise-related self-regulation and self-efficacy (N = 99) were divided for separate analyses into groupings of <3 bouts/week, and ⩾3 bouts/week, of light (e.g., easy walking) and moderate (e.g., fast walking) PA/exercise regularly completed prior to treatment start. The participants were assessed on psychosocial and PA/exercise changes from baseline to month 3.
Results:
Reductions in total mood disturbance (TMD), depression, and anxiety scores were overall significant, with no significant difference by exercise-frequency grouping. PA/exercise increases were significantly greater in the <3 bouts/week groupings. Change in self-regulatory skills usage mediated relations between groupings and changes in TMD, depression, and anxiety. In subsequent serial mediation models, significant paths from grouping → self-regulation change → self-efficacy change → TMD and depression changes were found.
Conclusion:
Whether or not ⩾3 bouts/week of PA/exercise are completed at intervention start, TMD, depression, and anxiety may be reduced through treatment foci on increasing PA/exercise, self-regulation, and self-efficacy. Findings might be useful for informing scalable obesity treatments.
Introduction
Approximately 42% of adults in the United States have a weight-to-height ratio that classifies them as having obesity (i.e., body mass index (BMI) ⩾30 kg/m2). 1 That medical issue, which is associated with numerous health risks, 2 has been consistently increasing over many decades in wealthy nations. 3 Although controlled eating and increased physical activity/exercise (PA/exercise) will reliably reduce weight in almost all adults with obesity, those behaviors have consistently been resistant to change—especially beyond the initial weeks after their initiation.4,5 First-line approaches aiming to simply inform affected individuals on methods to improve their diet and increase PA/exercise 6 have been particularly unsuccessful.7,8
Adjusting behavioral obesity-treatment contents
More recent theory- and evidence-grounded approaches have incorporated weight loss behavior-change methods based on their verified psychosocial correlates. 9 Those include participants’ use of self-regulatory methods (e.g., goal-setting, cognitive restructuring/productive self-talk) and their development of more favorable mood (e.g., reduced anxiety and feelings of depression) and self-efficacy (i.e., feelings of ability/mastery). Treatment foci on such psychological constructs (and their interactions) is consistent with social cognitive theory10,11 and theories that support more granular aspects of that broad-reaching paradigm such as self-regulation theory, 12 self-efficacy theory, 13 and the mood-behavior model. 14 Although some improvements were found via earlier cognitive-behavioral approaches, their overall modest outcomes15,16 stimulated increased use of more invasive processes such as weight loss (bariatric) surgery 17 and anti-obesity medications. 18 Although those medical interventions are often promoted as remedies for obesity requiring minimal effort on the part of patients,19,20 each has notable health risks 21 and can also be expensive and difficult to disseminate in a scalable manner. 22 Even given clear challenges, 23 some researchers have persisted at seeking innovative methods to address the obesity problem through behavioral/psychosocial means in a large-scale and cost-effective manner.24,25
An extended role for physical activity/exercise
In reviews of over 100 related studies, the use of PA/exercise was considered uniquely important for weight loss attainment.26–29 Increased PA/exercise might be a vehicle for improvements in psychosocial correlates of improved eating behaviors such as mood, 30 self-regulation, and self-efficacy.26,28,29 However, even theory-driven cognitive-behavioral weight loss treatments have often addressed PA/exercise as merely an optional adjunct to eating changes because of its minimal (direct) contribution to energy deficits.15,30 Research indicates that improvements in both PA/exercise and the aforementioned psychological constructs are most pronounced in the initial 3 months of treatment, but they reliably carry-over to later and longer-term changes. 29 Both theory10,12–14,31 and research26,28,3233,34 suggest that (1) early changes in mood facilitate increases in both self-regulation and self-efficacy, (2) exercise-focused self-regulation and self-efficacy generalize to eating-related self-regulation and self-efficacy (and sustained weight loss via more controlled eating), and (3) use of newly learned self-regulation skills facilitate increased self-efficacy via feelings of mastery over goal-directed behaviors that are considered challenging (e.g., maintaining regular exercise).
Implications for physical activity/exercise amounts
Although less clear for those with a mental health disorder, 35 it was further indicated that ⩾3 light-moderate bouts of PA/exercise per week induce significant improvements in mood in sedentary and low-active adults, with no further improvements associated with more frequent bouts and greater intensities. 25 A synthesis of 30 related studies also called into question a PA/exercise dose–mood change relationship. 36 This favors the “psychological hypothesis” of the physical activity–mood change relationship over biochemically based hypotheses (e.g., “serotonin hypothesis,” “norepinephrine hypothesis” 30 ), which would require the presence of a dose–response relationship. 37 Rather, the psychological hypothesis suggests that factors such as self-efficacy and its interrelation with self-regulation mediate the PA/exercise–mood improvement relationship (i.e., feelings of ability and accomplishment are associated with a positive psychological/emotional/mental outlook30,38,39).
Thus, evaluating the lower end of PA/exercise outputs for mood improvement is important because greater amounts, possibly impelled by physiologically driven guidelines for high energy expenditures for weight loss, 40 are associated with reduced adherence—a considerable problem most prevalent in women with obesity.25,41 Based on the aforementioned and other findings, 42 it is presently unclear whether increased PA/exercise can be leveraged for mood and other relevant psychosocial improvements when program participants regularly complete ⩾3 bouts/week of PA/exercise prior to starting their treatment program. It is possible that associated reductions in negative mood had already been maximized (i.e., floor effect), and thus, treatments might not be able to depend on the valuable mood improvements derived from increased PA/exercise in those already moderately (or greater) active. Such a finding would inform behavioral treatment content.
Research questions/hypotheses
In consideration of the aforementioned theories and studies, a research question was whether reduction in negative mood over 3 months would significantly differ among participant groupings where (the equivalent of) ⩾3 bouts/week of PA/exercise were/were not already regularly completed at treatment start (i.e., baseline). It was expected that PA/exercise would significantly increase across participants, and those changes would be significantly greater in groupings where <3 bouts/week were completed at baseline (as that group would have more available room for improvements). Additionally, it was expected that the 3-month increase in self-regulation skills usage would significantly mediate relations between participant groupings of completing/not completing 3 PA/exercise bouts at baseline and reduction in negative mood. Given expected relationships between changes in self-regulation and self-efficacy,25,26,28 it was also posited that paths from grouping → change in self-regulation → change in self-efficacy → mood changes would be significant.
Women with obesity were incorporated because research suggests that females are more affected by mood in weight-management contexts than males. 43 Also, women are the more frequent enrollees in obesity treatments. 44 Thus, findings with them could be the most relevant. However, it was also previously indicated that outcomes in the present area of inquiry will likely generalize to men. 9 It was hoped that the present field-based research of 3 months would help clarify appropriate usages and mechanisms of the exercise–mood improvement relationship, and help determine how they could best be leveraged within efficiently disseminated behavioral obesity treatments.
Materials and methods
Participants
Data were from a continuing research program in the United States focused primarily on behavioral obesity treatment outcomes (e.g., weight and body composition changes). Because the present aims and analyses were unique to this research, the reuse of participant data was justified. Women participants of ⩾21 years of age with obesity at baseline (confirmed by study staff measurement of their BMI at that time) were included. Each had a goal of weight loss. Additional inclusion criteria were: (1) no known contraindication for safe and complete participation within a local community-based health promotion center-based program, (2) no participation in another weight-management program within the previous 12 months, (3) no change in a psychotropic medication (including dosage) within the previous 6 months, and (4) no current/soon-planned pregnancy. Data were collected prior to restrictions associated with the COVID-19 pandemic. Demographic data on the participants are given in Table 1. For the current study, each participant was grouped, post hoc, based on whether she reported completing the equivalent of <3 light PA/exercise bouts/week at baseline (n = 53) or ⩾3 light PA/exercise bouts/week (n = 46), and (separately) the same for moderate PA/exercise bouts/week at baseline (i.e., n = 73 and n = 26, respectively). To facilitate the dichotomization of groupings, each participant’s Leisure-Time Physical Activity Questionnaire score 45 (described in the “Measures” section below) at baseline was used to separately assess the equivalent of 3 light bouts of PA/exercise/week (i.e., a score of 9) and the equivalent of 3 moderate bouts of PA/exercise/week (i.e., a score of 15) as cut points.
Demographic characteristic of the study sample (N = 99).

GED: general education degree; BMI: body mass index; SD: standard deviation.
Ethical requirements of the World Medical Association Helsinki Declaration and the American Psychological Association were maintained. The Kennesaw State University Institutional Review Board approved the protocol (study 17173) and the informed consent form signed by each participant prior to their start of any study process.
Measures
Brief measures possessing adequate validity were sought and incorporated to minimize inaccuracies due to participant burden associated with completing multiple lengthier inventories. 46
PA/exercise was measured using the Leisure-Time Physical Activity Questionnaire. 45 Bouts of ⩾15 min completed during the “previous 7 days” (one word was altered from the original “typical 47 7 days” for purposes of this study) were recalled. Response options were “mild exercise (minimal effort; e.g., easy walking),” “moderate exercise (heartbeat faster than resting, but not exhausting; e.g., fast walking),” and “strenuous exercise (heart beats rapidly; e.g., running).” Those responses were assigned scores of 3, 5, and 9, respectively, based on their associated metabolic equivalent of task (MET; a measure of physical intensity). That score was multiplied by the corresponding number of bouts of that intensity completed within the previous 7 days, then summed. As examples: 3 bouts of mild exercise (3 × 3 METs) = 9; and 3 bouts of moderate exercise (3 × 5 METs) = 15. Concurrent validity of the Leisure-Time Physical Activity Questionnaire was indicated in previous research through its score correspondences with accelerometry and treadmill stress-test scores with test–retest reliability over 2 weeks at 0.74.48–52 A recent review also deemed the Leisure-Time Physical Activity Questionnaire sensitive to cases where adverse physical conditions foster minimal levels of PA/exercise. 53
Total mood disturbance (TMD) was measured through use of the 30-item Profile of Mood States-B (brief form). 54 Reflecting over the previous 7 days, response options for each item ranged from 0 (not at all) to 4 (extremely) for each of its one- to three-word items (e.g., “dejected,” “anxious,” “vigorous”), which centered around dimensions of depression, anxiety, fatigue, anger, confusion, and vigor. Those were equally weighted, with the total of vigor item response scores subtracted from the sum of the other five proposed dimensions of overall negative mood. Thus, the possible score range for TMD was −20 to 100. Scores for the depression and anxiety scales of five items each were also separately calculated. Their possible score ranges were both 0–20. For each of the Profile of Mood States-B scores used in this research, a higher score indicated more negative mood. In women, earlier research indicated acceptable internal validity (mean Cronbach’s α = 0.90), with test–retest reliabilities over 3 weeks averaging 0.70. 54 Previous research also supported concurrent validity through Profile of Mood States score correspondences with well-validated, but lengthier, mood measures such as the Beck Depression Inventory (for depression), the Manifest Anxiety Scale (for anxiety), and the Minnesota Multiphasic Personality Inventory-2. 55 Associations between scores from the present brief form B and full 65-item Profile of Mood States were strong at β = 0.93–0.98. 56 Within the present sample, the mean Cronbach’s α = 0.83. A review indicated that Profile of Mood States score changes are sensitive to exercise stimuli across sample types. 57
Exercise-related self-regulatory skill usage was measured using the 10-item Exercise-Related Self-Regulation Scale (e.g., “I make formal agreements with myself to be physically active”).21,58 Items reflected self-regulatory skills proposed by Michie et al. 59 as being consistent with social cognitive theory. Response options for each item ranged from 1 (never) to 4 (often), and were summed. The possible score range was 10–40, with a higher respondent score indicating their more frequent use of self-regulatory skills. Previous research reported an acceptable internal validity (Cronbach’s α = 0.81), with test–retest reliability over 2 weeks at 0.74. 58 Predictive validity was supported by associations between score increases and increased exercise. 58 Within the present sample, Cronbach’s α = 0.74.
Exercise-related self-efficacy was measured using the five-item Exercise Self-Efficacy Scale. 60 It measured confidence at persisting with PA/exercise under challenging conditions (e.g., “I feel I don’t have the time,” “I am tired”). Response options for each item ranged from 1 (not at all confident) to 11 (very confident) and were summed. The possible score range was 5–55, with a higher score indicating more self-efficacy in the respondent. Previous research reported acceptable internal consistencies of Cronbach’s α = 0.76–0.82, and test–retest reliabilities over 2 weeks at 0.74–0.78. 60 For the present sample, Cronbach’s α = 0.76.
Procedure
The present cognitive-behavioral obesity treatment consisted of components of PA/exercise support (baseline to month 6), and support of controlled eating (months 3–12). Because the focus of this investigation was baseline to month 3, the period where most PA/exercise gains are typically made, 30 the PA/exercise support processes within that time frame are given. Subsequent procedures not accounted for in this report are described elsewhere. 61 The treatment content was based on tenets of social cognitive theory,10,62 but the supporting paradigms of self-regulation theory 12 and self-efficacy theory 13 additionally informed the treatment content.
After obtaining training in administration of the study treatment by research staff, sessions were administered by existing staff members of the community health promotion facilities agreeing to participate in the present research. There were four 50-min meetings (one instructor/one participant) conducted over the initial 3 months (weeks 1, 3, 7, and 11) held in private office settings. Although safe and acceptable PA/exercise was discussed, most session time was spent on the development of each participant’s self-regulatory skills, which included relapse prevention, cognitive restructuring, dissociation from discomfort, stimulus control, behavioral contracting, and short-term goal progress monitoring. There was instructor–participant collaboration on PA/exercise goal tracking during each session, and even small amounts of progress were highlighted there. The relationship between increased perceptions of competence toward adhering to regular exercise (i.e., increased self-efficacy) through regular usage of newly developed self-regulatory skills was a consistent treatment focus. Regarding PA/exercise amounts, although the governmental recommendation of at least 150 min/week of moderate or higher intensity bouts for health promotion was mentioned, it was suggested that any increase that was maintained could be productive. Thus, no specific exercise amount was assigned. The need for consistent PA/exercise was emphasized because its adherence, especially for women with obesity, has been challenging.41,63
Non-instructional research staff conducted structured protocol fidelity checks on 15% of instructor-administered treatment sessions. Compliance was strong, and only minor adjustments were required to be presented to the instructors. Non-instructional study staff also administered the study measures to participants in a private area. Based on the ratio of intervention sessions attended/total number of possible sessions, participants’ mean adherence was 82%.
Data analyses
Based on established criteria, 64 there was no systematic bias in participants with versus without missing data (i.e., missing-at-random in the 9% of overall missing values that were each beyond baseline). That satisfied the established criterion for imputation using the expectation–maximization algorithm,65,66 and facilitated an intention-to-treat format.67,68 Variance inflation factor scores of <2.0 indicated acceptable multicollinearity,69,70 and neither floor nor ceiling effects were observed prior to the analyses.
Mixed-model repeated measures analysis of variance (ANOVA) first assessed significance in mood changes from baseline to month 3 (separately for TMD, depression, and anxiety) and then evaluated whether those changes significantly differed by grouping (i.e., time × grouping effects). Separate analyses were conducted for groupings based on whether light PA/exercise at baseline or moderate PA/exercise at baseline was being considered. Coding for each was no = 0 (at least three sessions/week of PA/exercise was not completed at baseline), yes = 1 (at least three sessions/week of PA/exercise was completed at baseline). A similar analysis assessed PA/exercise change from baseline to month 3. Supplementary within-group (dependent) t tests were also calculated.
Using aggregated data, separate models that accounted for each mood measure and both PA/exercise intensity level grouping were fit. Specifically, significance of mediation of the association between the dichotomously coded PA/exercise groupings and the mood changes, by changes in exercise-related self-regulation, was assessed. Finally, change in exercise self-efficacy was added to the previous models as a second mediator in serial multiple mediation analyses. Based on recent suggestions, 71 a significant relationship between the independent variable (grouping) and the dependent variable (mood change) was not first required to conduct those regression analyses.
Sensitivity analyses assessed the relationship of baseline PA/exercise and baseline moods, and the prediction of mood changes by initial moods, also accounting for light and moderate PA/exercise groupings. SPSS Statistics version 28.0.1.0 (IBM, Armonk, NY, USA) was used for statistical testing, incorporating the PROCESS 4.2 macroinstruction mediation models 4 and 6, with 10,000 percentile-based bootstrap resamples of the data. 71 Statistical significance was set at α ⩽ 0.05 (two-tailed), and one-tailed where relationships had previously been established between PA/exercise and the tested psychosocial variables in similar contexts. 72 Where bootstrapping was employed, a 95% confidence interval (95% CI) was used to assess significance. The Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines 73 informed the reporting format.
Results
Contrasting baseline physical activity/exercise frequency-based groupings on changes in mood and physical activity/exercise
Table 2 provides descriptive statistics and ANOVA results for each mood and PA/exercise measure change from baseline to month 3 within the groupings, and for aggregated data. There was no significant difference in any mood measure at baseline, by PA/exercise intensity/frequency grouping. For TMD, depression, and anxiety, improvements from baseline to month 3 were significant overall, with large effect sizes in both the light and moderate PA/exercise groupings. None of the associated time × grouping effects were significant. For PA/exercise, improvements were also significant overall, with large effect sizes for both groupings. There was a significant time × grouping effect for only the moderate PA/exercise groupings, with greater increase found in the grouping reporting completion of <3 PA/exercise bouts/week at baseline. In supplementary within-grouping analyses, dependent t tests yielded significant improvements throughout (ps <0.001, except p = 0.011 on depression change and p = 0.020 on anxiety change for the PA/exercise grouping participants who reported ⩾3 moderate-intensity PA/exercise bouts/week at baseline). Effect sizes were large for all changes in TMD and PA/exercise (Cohen’s ds = 0.99–1.66) and moderate for depression and anxiety changes (Cohen’s ds = 0.49–0.76).
Mixed-model repeated measures analysis of variance results.

Light exercise (LTex) <3 = baseline physical activity/exercise of less than three light-intensity sessions/week (a baseline score of <9 on the LTPAQ), n = 53. Light exercise (LTex) ⩾3 = baseline physical activity/exercise of at least three light-intensity sessions/week (a baseline score of ⩾9 on the LTPAQ), n = 46. Moderate exercise (MODex) <3 = baseline physical activity/exercise of less than three moderate-intensity sessions/week (a baseline score of <15 on the LTPAQ), n = 73. Moderate exercise (MODex) ⩾3 = baseline physical activity/exercise of at least three moderate-intensity sessions/week (a baseline score of ⩾15 on the LTPAQ), n = 26. Aggregated data, N = 99. Δ = change in score during the designated period. η2 p = partial eta-squared (SSEffect/[SSEffect + SSError]), where 0.01, 0.06, and 0.14 represent small, medium, and large effects, respectively. TMD: total mood disturbance; PA/ex: physical activity/exercise; LTPAQ: Leisure-Time Physical Activity Questionnaire; SD: standard deviation.
Mediations of relations between baseline physical activity/exercise frequency grouping and mood changes through changes in self-regulation
For the light PA/exercise groupings, 3-month change in (Δ) exercise-related self-regulation significantly mediated relations between grouping and ΔTMD, B = 2.56, SE B = 1.64, 95% CI [0.025, 5.413]; Δdepression, B = 0.37, SE B = 0.25, 95% CI [0.008, 0.807]; and Δanxiety, B = 0.32, SE B = 0.26, 95% CI [0.000, 0.765]. Each of those overall predictive models was significant, R2 = 0.27, p < 0.001; R2 = 0.18, p < 0.001; and R2 = 0.08, p = 0.018, respectively (see Figure 1(a)–(c) for relationship data within the embedded paths).

Mediation of self-regulation change in predictions of changes in (A) total mood disturbance, (B) depression, and (C) anxiety by light physical activity/exercise grouping (N = 99).
For the moderate PA/exercise groupings, Δexercise-related self-regulation significantly mediated relations between grouping and ΔTMD, B = 4.31, SE B = 1.99, 95% CI [1.167, 7.781]; Δdepression, B = 0.61, SE B = 0.32, 95% CI [0.127, 1.173]; and Δanxiety, B = 0.52, SE B = 0.37, 95% CI [0.076, 1.184]. Each of those predictive models was significant, R2 = 0.27, p < 0.001; R2 = 0.18, p < 0.001; and R2 = 0.08, p = 0.016, respectively (see Figure 2(a)–(c) for embedded path data).

Mediation of self-regulation change in predictions of changes in (A) total mood disturbance, (B) depression, and (C) anxiety by moderate physical activity/exercise grouping (N = 99).
Within each model (Figures 1 and 2), the relationship between Δself-regulation and Δmood was significant (after controlling for each of the other relationships across the included variables).
Serial mediation analyses of relations between baseline physical activity/exercise frequency grouping and mood changes through changes in self-regulation and self-efficacy
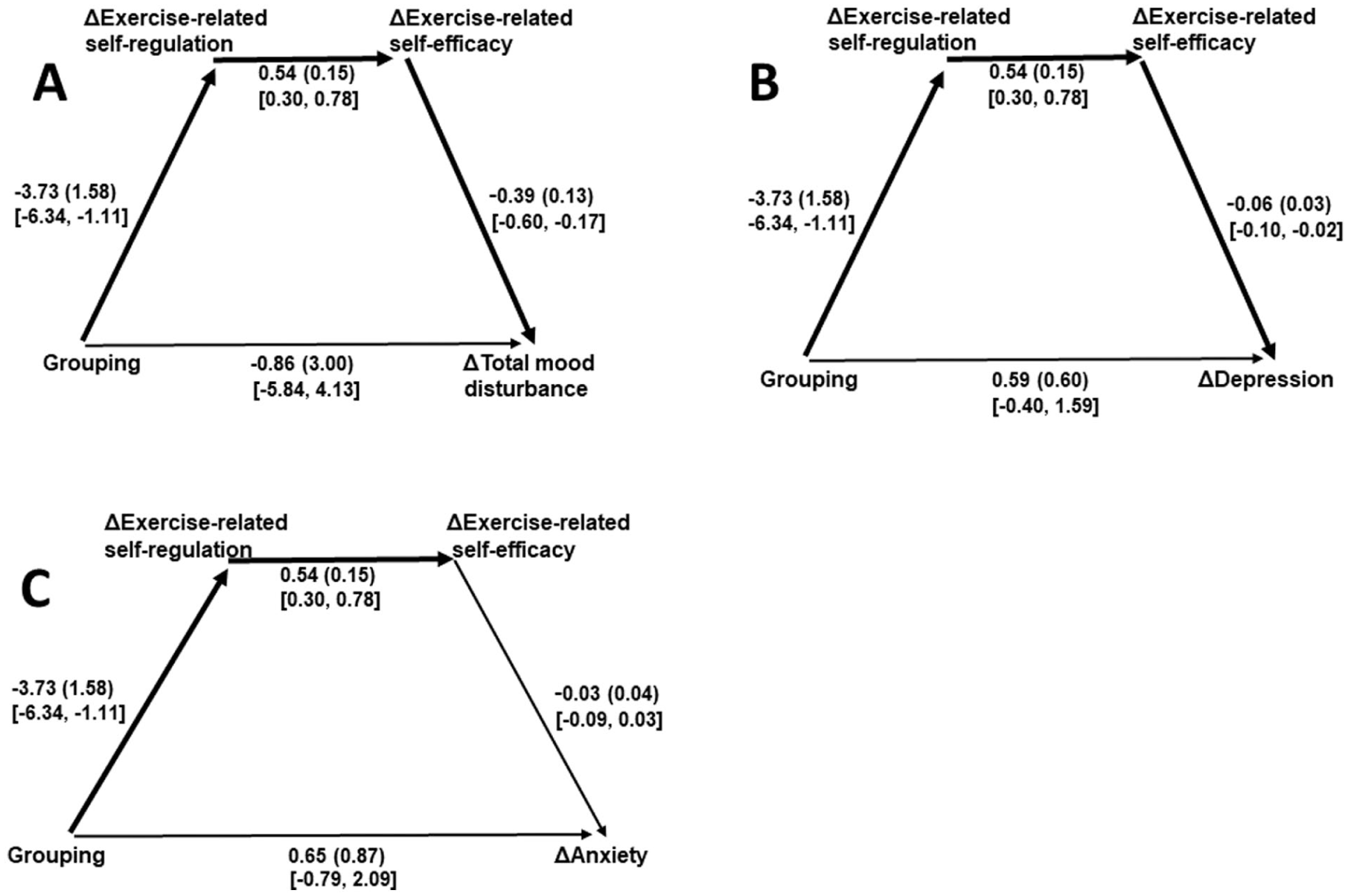
For the light PA/exercise groupings, the following paths were significant: grouping → Δexercise-related self-regulation → Δexercise self-efficacy → ΔTMD, B = 0.46, SE B = 0.36, 95% CI [0.016, 1.153]; and grouping → Δexercise-related self-regulation → Δexercise self-efficacy → Δdepression, B = 0.07, SE B = 0.06, 95% CI [0.000, 0.187]. The following path was not significant: grouping → Δexercise-related self-regulation → Δexercise self-efficacy → Δanxiety, B = 0.03, SE B = 0.06, 95% CI [−0.037, 0.138]. Each of those overall predictive models was significant, R2 = 0.34, p < 0.001; R2 = 0.22, p < 0.001; and R2 = .09, p = 0.036, respectively (see Figure 3(a)–(c) for embedded path data).

Serial mediation analyses of paths from light physical activity/exercise grouping to changes in (A) total mood disturbance, (B) depression, and (C) anxiety through changes in self-regulation and self-efficacy (N = 99).
For the moderate PA/exercise groupings, the following paths were significant: grouping → Δexercise-related self-regulation → Δexercise self-efficacy → ΔTMD, B = 0.79, SE B = 0.45, 95% CI [0.161, 1.591]; and grouping → Δexercise-related self-regulation → Δexercise self-efficacy → Δdepression, B = 0.12, SEB = 0.09, 95% CI [0.016, 0.309]. The following path was not significant: grouping → Δexercise-related self-regulation → Δexercise self-efficacy → Δanxiety, B = 0.06, SE B = 0.09, 95% CI [−0.055, 0.219]. Each of those overall predictive models was significant, R2 = 0.34, p < 0.001; R2 = 0.23, p < 0.001; and R2 = 0.09, p = 0.032, respectively (see Figure 4(a)–(c) for embedded path data).
Serial mediation analyses of paths from moderate physical activity/exercise grouping to changes in (A) total mood disturbance, (B) depression, and (C) anxiety through changes in self-regulation and self-efficacy (N = 99).
Within each model (Figures 3 and 4), the relationship between Δexercise-related self-regulation and Δexercise self-efficacy was significant (after controlling for each of the other relationships across the included variables).
Sensitivity analyses
There was no significant relationship between PA/exercise at baseline and baseline TMD, β = −0.16, p = 0.124; baseline depression, β = −0.18, p = 0.079; or baseline anxiety, β = −0.10, p = 0.352. There were significant relationships between TMD at baseline and ΔTMD, β = −0.66; baseline depression and Δdepression, β = −0.69; and anxiety at baseline and Δanxiety, β = −0.71, ps < 0.001. The addition of grouping into step 2 of the above equations did not significantly contribute to the explained variance in ΔTMD, ps >0.300; Δdepression, ps >0.200; or Δanxiety, ps >0.070.
Discussion
The present results informed behavioral obesity treatments on their usage of PA/exercise-associated mood improvements. Because intensities of completed PA/exercise were sometimes unclear in previous related research, analyses separately accounted for both light and moderate intensities. Supporting the corresponding hypothesis, PA/exercise of a moderate intensity increased more in the grouping that started initially lowest on that measure. That result is consistent with a key target of the present cognitive-behavioral treatment, which was increasing PA/exercise in sedentary and low-active adults. 72 In evaluating the primary research question, it was found that the significant baseline to month 3 score reductions in TMD, depression, and anxiety did not significantly differ by grouping (nor did they significantly differ at baseline). This suggests that, although attaining three bouts/week of PA/exercise appeared to demonstrate a floor effect in regard to reducing negative mood in some previous research, 25 meaningful mood improvements still were observed across both tested groupings. Findings also indicated that those significant mood improvements might similarly occur whether the initial PA/exercise amounts are of a light or moderate intensity. Although exercise amounts of up to 420 min/week have been suggested within the scientific literature in the hopes of expediting weight loss via associated energy expenditures, 74 those directives might challenge adherence, especially in adults with obesity.41,75 Thus, if PA/exercise is incorporated to foster improvements in psychosocial correlates of controlled eating—as has been indicated as advantageous 76 —lesser amounts might also be valuable. This is consistent with suggestions that the greatest value of PA/exercise for weight loss is in its ability to induce psychosocial changes that are predictive of controlled eating.9,25 Because the PA/exercise amount–mood change association was indirectly negated here, the psychological hypothesis of the effects of exercise on mood was supported.30,37
Based on social cognitive theory,10,62 and more specifically self-regulation theory 12 and associated research,25,26,28 the hypothesis that changes in exercise-related self-regulation would mediate the exercise frequency-based grouping-mood change relationships was supported. This further bolstered the present treatment’s focus on building an array of self-regulatory skills across participants. Although requiring distinct testing, based on coaction theory 31 and previous research,33,77,78 those self-regulatory skills might also transfer (i.e., generalize) to supporting the eating behavior changes that are essential for weight loss and reductions in obesity. Also, both improved mood and increased self-regulation have been shown to be favorably associated with emotional eating reduction and overall control over eating during the long-term. 79
The final hypothesis was partially supported in that the significant prediction of heightened self-efficacy by increased self-regulation mediated the grouping → ΔTMD, and grouping → Δdepression, relationships. However, the path from grouping → Δself-regulation → Δself-efficacy → Δanxiety was not significant. Although each of the overall predictive models were significant, it is unclear why anxiety had effects that differed somewhat from those of TMD and depression. It is possible that for anxiety change, a longer period is required to observe a significant path, as the present data indicated that directionality was consistent with the models incorporating TMD and depression changes. That finding should be further-explored in extensions of this research because anxiety is an important psychological predictor of controlled eating and sustained weight loss. 80 Notwithstanding that, findings of the significant paths support self-regulation theory, 13 and how self-efficacy may be increased via participants’ enhanced mastery over their personal environmental challenges through usage of newly learned self-management skills.
Although various psychosocial constructs have been associated with adherence to PA/exercise and controlled eating, and their interrelations; improvements in mood, self-regulation, and self-efficacy have been primary.9,81 They each, individually, have significantly contributed to the explained variance in both of those behavioral changes. Although it is presently unclear what psychological factor(s) holds the most value within behavioral obesity treatments, the present focus on self-regulatory skills development appeared to possess considerable merit for improving mood and increasing exercise-related self-efficacy. The findings also indicated prospects for further research regarding their carry over for sustaining improvements in eating behaviors.25,31,78 Further research should aim to clarify precisely what self-regulation skill or skills are the most salient so that treatment time might be most efficiently allocated. It should be noted, however, that attention to any of the considered psychological variables assessed within this report could represent an advancement over the continued atheoretical reliance on providing suggestions to eat in a controlled manner (or maintain a specific “diet”), to exercise at as high a level as possible, and expect meaningful improvements to emerge from solely those directives. 82
Limitations
Although contributions were made within this study related to the development and improvement of the treatment of obesity through behavioral means, limitations should also be acknowledged. For example, given that the present study partitioned the full sample for some analyses and incorporated assessments of both group equivalence and mediation of effects, extensions/replications using similar analytic formats should better-account for sample size and power to increase confidence in the findings. Also, although exercise-related psychological changes over the short term have carried over to longer-term changes in eating behaviors and weight loss,33,78,83 that was not directly tested within the confines of the present investigation. Thus, related studies of lengthier durations, that adequately address dietary changes via exercise-associated mood improvement, are required. Furthermore, the measurement of PA/exercise was reliant on participants’ recall and self-report and lacked a specific assessment of duration. More objective measurement, such as through accelerometry, might enhance accuracy in extensions of this research. Additionally, analyses of generalizations of findings to men—and across ages, ethnic/racial groups, socioeconomic strata, and medical issues (e.g., diabetes, reduced mobility)—are needed. Moreover, because groupings were established post hoc, this research was essentially a single-group design with all participants receiving the same standardized cognitive-behavioral treatment. In consideration of that, control conditions are needed to account for expectation, social support effects, and other possible experimental confounds associated with an interpersonally administered treatment, 84 and analyses should separately consider both the earlier stages where weight loss is expected, and beyond 6–9 months where regain of weight is projected.4,5 Such longitudinal analyses conducted within field environments would also increase relevance regarding the role of PA/exercise in the psychological aspects of obesity treatment and serve to further inform scalable referral possibilities for the medical community.
Conclusion
Given the presently high prevalence of obesity, 1 and that the typical informational approaches (possibly lasting only several minutes once or twice a year in a medical professional’s office) fail,7,8 health behavior-change researchers should seek to “package” protocols for their widespread application. As in this investigation, community health centers, YMCAs, and fitness/wellness centers provide an opportunity for that. Thus, although staffing has become minimal in such settings, we advocate for further research within those and similar environments. Possibly, referrals by physicians, nurse practitioners, and other medical professionals to such longitudinal programs will allow the present findings to help better address needed mechanisms for large-scale change. Based on the extant results, even manageable amounts of PA/exercise can become a basis for psychosocial changes that help to foster success with weight loss. Findings here also provide a rationale for why PA/exercise is one of the strongest predictors of sustained weight loss,85,86 but this typically cannot be reconciled by its associated energy expenditures.
Footnotes
Acknowledgements
The authors acknowledge the participants and instructors involved in the present research.
Ethical considerations
The Kennesaw State University Institutional Review Board approved the protocol (study 13173).
Consent to participate
The informed consent process required a signature from each participant prior to any study activity on their part.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset analyzed during the current study will be made available from the corresponding author upon reasonable request.