
Abstract
Background:
Addressing preconception health through targeted interventions, as advocated by the WHO, can greatly improve maternal and child outcomes.
Objectives:
The study explores community perceptions, preparedness, and expectations regarding preconception care (PCC). It evaluates the acceptance of nurses delivering PCC services, the efficiency of a community-based PCC package, and community readiness for village-level PCC services, aiming to co-develop a tailored PCC package.
Design and methods:
This formative research, conducted from March to September 2024, used a qualitative approach comprising focus group discussions, in-depth interviews, and free listing with ranking exercises across 96 villages under four primary health centers (PHCs) in rural Maharashtra, India with population of around 120,000, was carried out across four PHCs: PHC An (28 villages), PHC Kh (G) (25 villages), PHC Ta (Wa) (25 villages), and PHC Wa (26 villages). The study involved diverse participants, including eligible couples, village representatives, and community health workers. Data were analyzed using thematic content analysis, employing both deductive and inductive methods to identify themes related to perceptions, contributions, and expectations for PCC.
Results:
The study revealed limited community awareness of PCC, especially regarding genetic screening and early detection. Despite this, participants recognized PCC’s benefits for maternal health and safer deliveries, strongly supporting locally accessible clinics. Community priorities such as health screening, family well-being, and lifestyle changes reflected a holistic view of PCC. Communities proposed low-cost services, local clinic management, and promotion via self-help groups and village platforms. Expectations included diagnostics, infertility treatment, nutrition support, and counseling, with calls for both doctors and nurses to deliver services effectively.
Conclusion:
The findings highlight the community’s readiness to adopt PCC services, provided they are affordable, accessible, and tailored to local needs. The study underscores the importance of culturally sensitive approaches and leveraging community networks to promote PCC. Integrating locally prioritized areas into PCC frameworks can enhance maternal and child health outcomes and ensure effective implementation in resource-limited settings.
Plain Language Summary
This study explores how communities understand and prepare for preconception care (PCC), which is healthcare provided to individuals before pregnancy to ensure healthier mothers and babies. Preconception care focuses on promoting health and addressing risks before pregnancy, such as proper nutrition, early detection of health issues, and family planning. We conducted the study in rural areas of Wardha, Maharashtra, where many families face challenges accessing healthcare. Through interviews and group discussions with community members, including women, men, and healthcare workers, we learned about their views on PCC, their expectations for services, and the barriers they face. The study found that while many people were not aware of specific PCC services like genetic testing or disease prevention, they understood the importance of planning for a healthy pregnancy. They emphasized the need for local PCC clinics to provide services like blood tests, vaccinations, and counseling on family planning and healthy lifestyles. Community members also highlighted the importance of educating young women and families about health before pregnancy. The research revealed strong community support for introducing PCC services at the village level, provided they are affordable and accessible. People were willing to contribute to and manage these services through local leaders and healthcare workers. These findings show the need for healthcare programs that focus on preconception care, tailored to local needs and supported by the community. By addressing gaps in awareness and providing culturally appropriate services, PCC can help improve the health of mothers and babies in rural areas.
Keywords
Introduction
Over the years, advancements in antenatal care have significantly reduced maternal and neonatal mortality. Yet, despite these improvements, an estimated 800 women and 6700 newborns continue to die daily from preventable complications related to pregnancy and childbirth. The burden of these deaths is disproportionately high in low- and middle-income countries, where unplanned pregnancies, preterm births, birth defects, complications during labor, and infections are the primary contributing factors. 1 Globally, half of maternal deaths are attributed to just three causes: hemorrhage, hypertensive disorders, and sepsis. 2 Relying solely on antenatal care has proven to be insufficient, as it fails to address health issues that emerge before or in the early weeks of pregnancy. In low-resource settings, the first antenatal visit often occurs too late to detect and manage problems that contribute to maternal and neonatal mortality and morbidity. This highlights the need for earlier interventions and comprehensive care strategies to improve outcomes. 3
Role of preconception care in improving health outcomes
Much of the maternal and neonatal mortality and morbidity has its roots in the preconception period. Therefore, providing care before pregnancy, known as preconception care (PCC), is crucial in preventing maternal and child mortality and morbidity. PCC involves a set of interventions offered to women and couples before conception, aiming to improve and promote favorable neonatal and birth outcomes. By identifying and addressing modifiable risks to maternal and fetal health, it leverages social, behavioral, and medical interventions to optimize health before pregnancy.4–6 PCC has the potential to significantly improve maternal and child health outcomes. Recognizing this, the WHO has developed a comprehensive PCC package that covers 13 key areas. The WHO strongly recommends its global implementation to address critical health needs before pregnancy.7,8
Challenges and opportunities for PCC in India
Currently, India lacks a dedicated public health program for providing regular PCC services, with existing interventions scattered across various policies. The delivery of PCC interventions faces challenges due to the absence of specific sociocultural guidelines, limited understanding of community needs, lack of awareness, and resource constraints among healthcare providers. A qualitative study by Chutke et al. 9 revealed that women in rural areas had a meager understanding of PCC, often perceiving it as unnecessary or unfamiliar, despite expressing a willingness to adopt healthier practices if adequately informed. This gap in awareness significantly limits the uptake of early interventions aimed at improving maternal and child health outcomes. Furthermore, Chandhiok et al. 10 explored task-shifting in maternal health services and emphasized the operational difficulties in implementing decentralized care models, such as those involving community-level workers. Their findings underline the need for supportive infrastructure, clear role definitions, and adequate training when expanding health services like PCC at the grassroots level.
This formative research aims to address these gaps by enhancing the understanding of these factors. It forms part of a stepped-wedge cluster randomized implementation trial 11 titled as “Evaluating the effects of a community-based Pre-Conception Care package through trained nurses on Pre-conception Health, Maternal and Child Health Outcomes” that will assess the impact of a community-based PCC package, delivered by trained nurses, on preconception health, maternal health, and child health outcomes. It is recognized that government healthcare facility doctors will have limited involvement in delivering PCC to the community, as they are already burdened with providing curative and preventive services. To address this, a task-shifting strategy has been implemented, where trained nurses take on the responsibility of delivering PCC services.9,11,12 Thus, study aims to explore the community’s acceptance of nurses in delivering PCC services, assess the efficiency of nurses in providing the PCC package, and understand community perceptions, preparedness, and expectations regarding PCC. Additionally, it will determine the community’s readiness to engage with PCC services if made available at the village level. A key focus of the study is to co-develop a comprehensive PCC package in consultation with the community, ensuring it addresses their specific needs and encourages active contribution toward improving maternal and child health outcomes.
Methods
Study design and methods
This formative research was conducted using a qualitative approach to assess community perceptions, preparedness, and expectations regarding PCC. It was conducted as part of a stepped-wedge cluster randomized implementation trial, with the goal of co-developing a community-based PCC package delivered by trained nurses. The research adhered to the Consolidated criteria for reporting Qualitative Research (COREQ) guidelines, 13 ensuring transparency, rigor, and a systematic approach throughout the study (Supplemental Annexure 1). The qualitative methods employed included focus group discussions (FGDs), in-depth interviews (IDIs), and free listing and ranking exercises. The fieldwork for this research was conducted between March and September 2024. The proposed project was an attempt to implement PCC interventions at the village level in real-life settings and will help to develop a community-based PCC package that could be delivered through a task-sharing approach by trained auxiliary nurse midwives.
Study settings
The study was conducted in 96 villages across 4 primary health centers (PHCs) located in the Wardha Community Development Block of Maharashtra, India. These villages ranged in size, with populations between 300 and 10,000, covering a total population of approximately 120,000 people. Peri-urban villages within a 5-km radius of Wardha town were excluded from the study to focus on rural community. The PHCs involved were:
PHC An: 28 villages
PHC Kh (G): 25 villages
PHC Ta (Wa): 25 villages
PHC Wa: 26 villages
Sample size, participants, and sampling method
The sample size for this formative research was determined based on the need to gather diverse and comprehensive perspectives from different community members regarding PCC. As the study utilized qualitative methods, it adhered to the principle of data saturation. Saturation was reached when no new information or themes emerged from the data collection, ensuring that the sample was sufficient to meet the study’s objectives. Supplemental Table S1 provides a matrix outlining the data collection methods, their objectives, and the associated sample sizes. Participants were selected using purposive sampling based on the following eligibility criteria:
● Inclusion Criteria:
● Eligible couples: Newly married couples planning for a baby or couples who already had one or more children and were planning for another child.
Key informants: Village representative like: ○ Sarpanch (village head), ○ Gram Sabha members (village council members), ○ Accredited social health activist (ASHA) workers (community health workers) ○ Anganwadi Sevika (village childcare workers) ○ Police Patil (village police representatives) ○ Other community members like male and female community resource person, Panchayat resource person, and Bachatgut members (women self-help group members)
Exclusion criteria: Couples with either partner using permanent contraception (male or female sterilization procedures like tubal ligation or vasectomy) were excluded from the study.
Data collection process
To ensure ethical participation, all eligible participants were informed about the purpose, procedures, voluntary nature of participation, and their right to withdraw at any time. Given the low literacy levels in the study area, verbal informed consent was obtained instead of written consent. The consent process was conducted in the local language, and participants’ verbal consent was audio-recorded prior to initiating any interview or FGD. This approach was approved by the Institutional Ethics Committee (IEC) for Research on Human Subjects at Mahatma Gandhi Institute of Medical Sciences (IEC/406/2023) dated 30 December 2023. Field techniques included establishing rapport with villagers through prior meetings, where the concept of PCC was thoroughly explained. It was also ensured that the village head was informed in advance about the purpose of the study to gain their support and involvement. Following these initial engagements, eligible couples were informed about the study and approached through their respective village representatives to encourage participation. Data collection methods were planned based on the population of the villages. In more densely populated villages with group gram panchayats, separate FGDs were conducted for men and women. In smaller villages, a combination of qualitative methods was used, but all key informants across the study area were approached for IDI. The complete interview tool guide used in this study is provided in the Supplemental Annexure 2. The initial step of the fieldwork involved conducting IDIs, which helped the team to understand the overall status of the village. This included gathering information on the number of eligible couples and the community’s views on healthcare services, such as antenatal and postnatal care (ANC and PNC). The insights gained from these IDIs also helped in organizing participants for subsequent FGDs and Free Listing and Ranking exercises. The project team received training on qualitative data collection methods, and all data collection activities were conducted under the supervision of an anthropologist to ensure methodological rigor. The primary method of engagement with villagers and higher village authorities was face-to-face interaction, which allowed the team to build rapport. In some cases, telephonic conversations were used to facilitate further communication and coordination with village representatives. The profiles for male FGDs, female FGDs, and IDIs are detailed in the Supplemental Tables S2–S4.
Voice recordings of the interviews, lasting 30–40 min, were taken, while sociograms and detailed field notes captured participant interactions and key observations during the sessions. Female FGDs were conducted during the day, with ASHA informing participants in advance. Data collection methods were held in various village locations, including Anganwadi centers (village-level childcare and maternal health center under the Integrated Child Development Services scheme in India), schools, temples, or participants’ homes. Male FGDs, conducted in the evening, posed challenges due to the availability of participants, with frequent off-topic queries and cross-questions directed at female facilitators, making each session unique. For free listing and ranking, participants listed their expectations for the village PCC clinic on chart paper, with individual scores assigned based on the total number of expectations.
Data analysis
The data collected from the FGDs, IDIs, and free listing and ranking exercises were analyzed using thematic content analysis following established qualitative research standards ensuring credibility, dependability, and confirmability.14–16 All FGDs and IDIs conducted in Marathi language were transcribed verbatim by trained researchers followed by translation into English for analysis. The translated transcripts, along with detailed field notes and sociograms, were reviewed by two independent researchers to ensure accuracy and contextual consistency. A mixed approach was used for data analysis. Initially, a deductive approach was applied, using predefined themes based on the research objectives, while remaining open to new themes that emerged inductively from the data. This combination allowed for structured analysis while accommodating the discovery of unexpected insights. The analysis followed a systematic approach to identify recurring themes and patterns in community perceptions, preparedness, and expectations regarding PCC.
Familiarization with the data was achieved through repeated reading of the transcripts, which allowed the researchers to immerse themselves in the content. For the coding of the qualitative data, a manual approach was used with three coders to ensure consistency, accuracy, and inter-coder reliability throughout the analysis. Initial coding was conducted by two independent researchers, who reviewed the transcripts line by line, identifying key phrases, ideas, and recurring thoughts shared by the participants. The coding process involved identifying first-order codes, which were based on direct responses from participants. The codes represented recurring topics such as PCC Perceptions, PCC Contribution, and PCC Expectation. After the first-order codes were identified, the researchers grouped similar codes into second-order sub-themes. These sub-themes captured more specific aspects of the participants’ views and experiences. The sub-themes were further consolidated into higher-order themes based on their conceptual similarity.
To ensure the reliability of the themes and sub-themes, the coding and thematic structure were discussed among the research team, including the Principal Investigator. Discrepancies in coding and theme identification were resolved through discussion until consensus was reached. In addition to thematic analysis, a quantitative aspect was incorporated by calculating respondent frequency for each first-order code, indicating how many participants shared a specific view. This helped prioritize the most frequently mentioned and important themes. The final themes were refined and reviewed in collaboration with the Principal Investigator. This ensured that the themes accurately captured the key insights related to community readiness for PCC and addressed the study objectives. The finalized themes provided a comprehensive understanding of community perspectives, including their expectations from PCC services and the challenges they faced in accessing care. The final themes were validated through consensus and triangulated across multiple data sources and researchers to ensure credibility and trustworthiness, as recommended in qualitative research standards.
Triangulation
Triangulation was employed in this study to enhance the validity and reliability of the findings by incorporating data from multiple qualitative methods—FGDs, IDIs, and free listing and ranking exercises. Methodological triangulation ensured that data collected through FGDs, which captured group perceptions, were cross-validated with insights from IDIs, providing detailed individual perspectives, and free listing and ranking, which highlighted specific community expectations regarding PCC. Data source triangulation involved gathering information from diverse participants, including newly married couples, key informants like Sarpanch, ASHA workers, and Anganwadi Sevikas, and couples planning for another child, ensuring a comprehensive understanding of community views. Additionally, investigator triangulation was applied, with two independent researchers conducting the initial coding and thematic analysis, and any discrepancies being resolved through discussions with the Principal Investigator. This triangulation approach strengthened the study’s conclusions by ensuring consistency and depth across multiple data sources and methods.
Results
The results of this formative research provide valuable insights into the community’s understanding and engagement with PCC. Emerged themes reflect the community’s perceptions of PCC, their contributions toward implementing PCC practices, and their expectations of such services. The findings are organized into distinct thematic categories, each illustrated with direct quotes from participants to highlight the perspectives shared. The analysis is presented in the following sections, detailing the core themes that have emerged from the data.
Community perceptions of PCC: Thematic insights from FGDs and IDIs
Contributions to PCC: A thematic review from FGDs and IDIs
Expectations for PCC services: Thematic findings from FGDs and IDIs
Expectations for PCC: Insights from free listing and ranking analysis
Figure 1 outlines the barriers, perceptions, and benefits of PCC using a community-based mind map. The higher-order theme in Table 1 is community perceptions of PCC. The table reveals that, while the community recognizes the advantages of PCC, there is still a significant lack of awareness, particularly regarding early disease detection, genetic screening, and preparing for a healthy pregnancy. Cultural norms, such as the strong preference for male children, persist and often influence reproductive decisions. Respondents emphasized the importance of inter-conception care, particularly the need for proper spacing between children to ensure adequate nutrition for both mother and child. They highlighted the benefits of PCC, including improved maternal and child health, safer deliveries, and the convenience of having a PCC clinic in the village, which would save time and money by providing timely care.
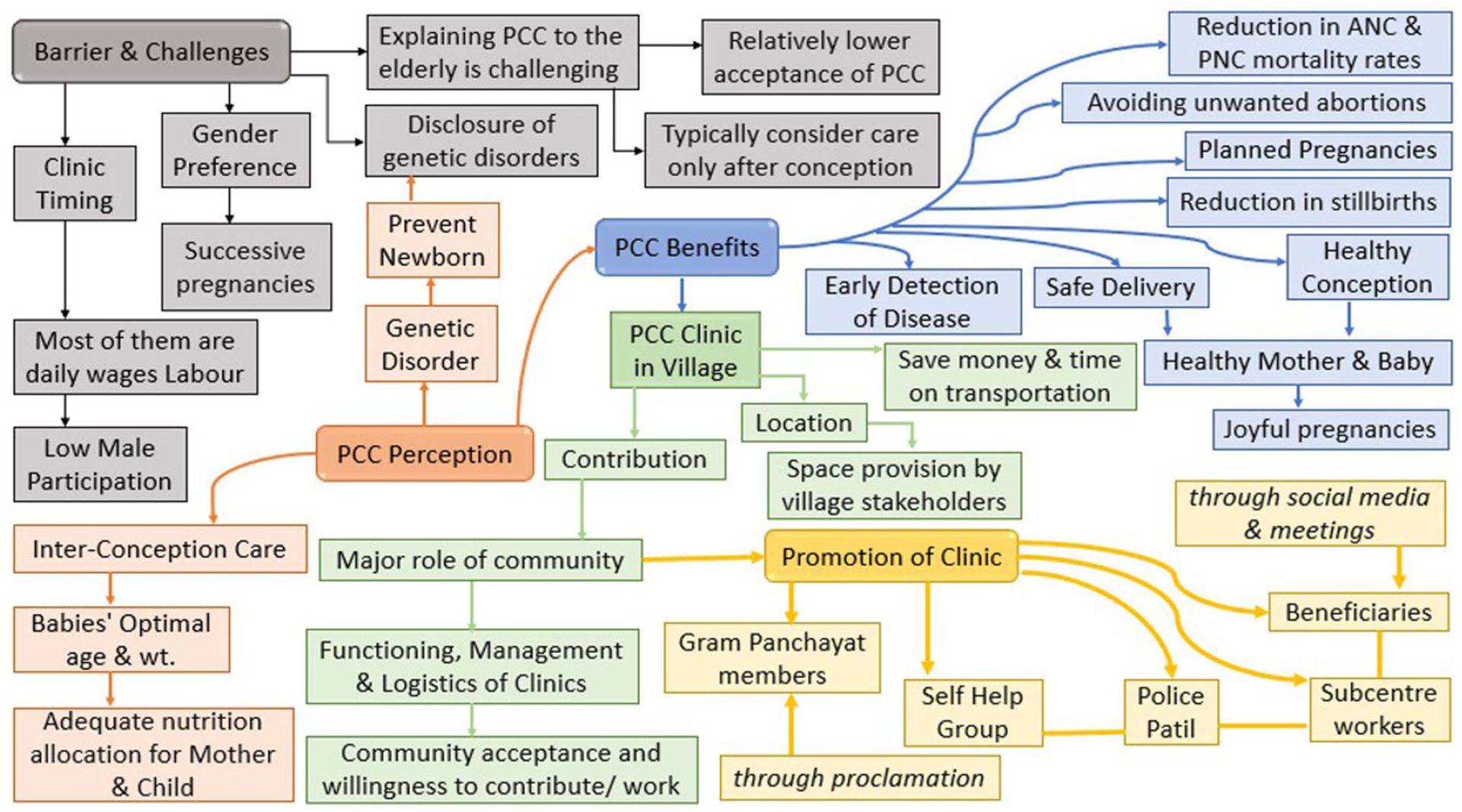
Barrier, perceptions, and benefits of PCC: A community-based mind map.
Community perceptions of PCC: Thematic insights from FGDs and IDIs.
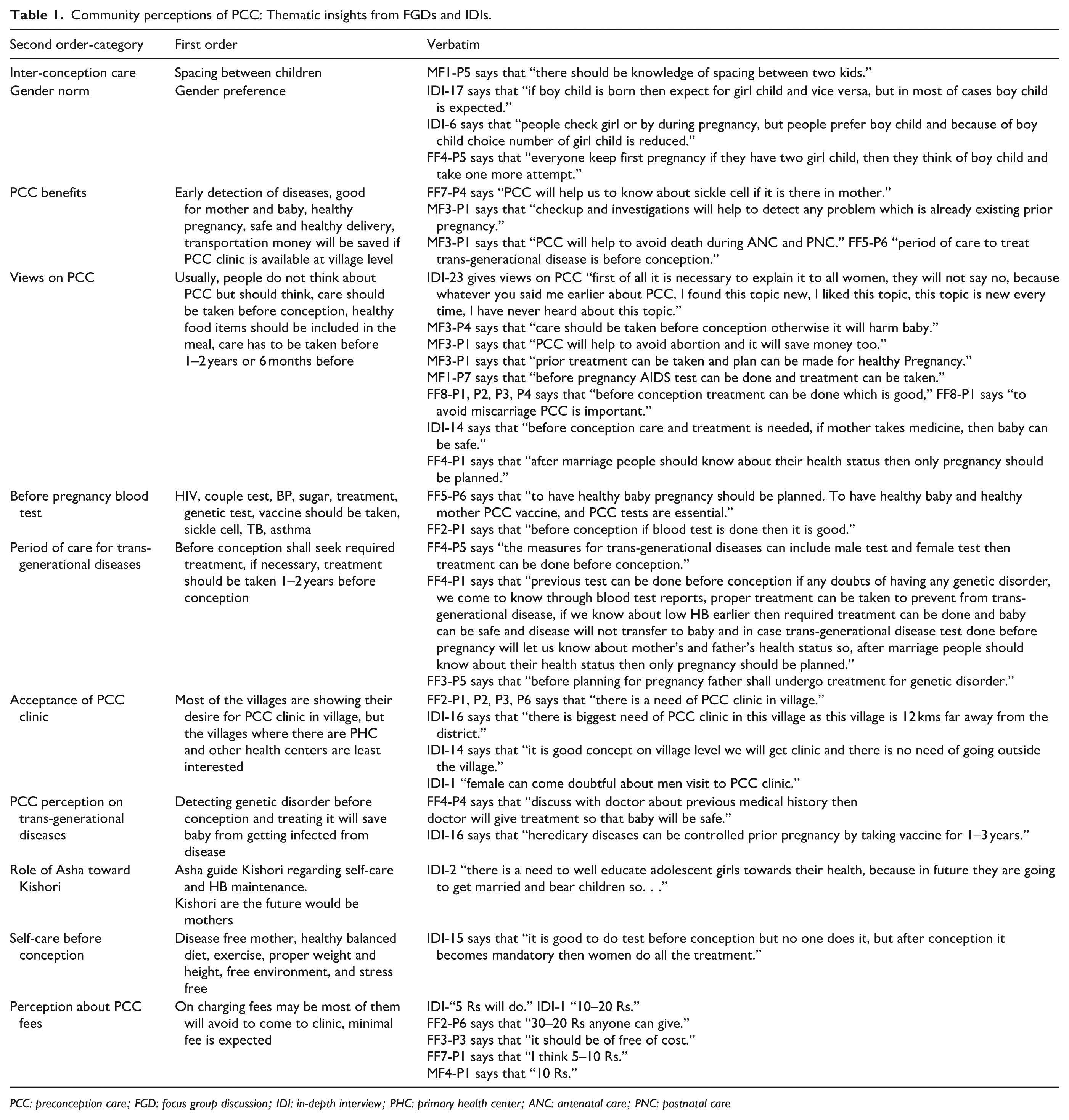
PCC: preconception care; FGD: focus group discussion; IDI: in-depth interview; PHC: primary health center; ANC: antenatal care; PNC: postnatal care
Additionally, respondents stressed the importance of blood tests before conception, mentioning tests for HIV, blood pressure, sugar levels, genetic disorders, and vaccines like tetanus. There was also a focus on the period of care for trans-generational diseases, with many agreeing that treatment for genetic disorders should begin 1–2 years or at least 6 months before conception to ensure a healthy baby. Commonly discussed trans-generational diseases included blood pressure, diabetes, thyroid issues, and genetic conditions, all of which respondents believed should be treated before pregnancy.
While the community expressed a desire for PCC clinics, particularly in remote areas, concerns about affordability and accessibility were raised. Some participants suggested that fees should be minimal, as many struggle with paying taxes and may avoid attending the clinic if the costs are too high. In contrast, villages with existing healthcare centers showed less interest in new PCC services. The role of ASHA workers in educating adolescent girls (Kishori) was also emphasized, as they are the future mothers and often suffer from anemia. Finally, respondents highlighted the importance of self-care before conception, including regular health monitoring, genetic testing, a nutritious diet, and taking the necessary PCC vaccines. Couples should be aware of their own and their partner’s health status before planning a pregnancy. Overall, the community showed a readiness to adopt PCC but needs increased education, financial support, and accessible services to ensure successful implementation.
The higher-order theme in Table 2 is contributions to PCC, which encompasses the community’s role in managing, promoting, and supporting the PCC clinic. The table reveals that management responsibility could be shared among various local figures, such as ASHA workers, self-help groups, Bachatgut members, and even educated youth, demonstrating flexibility and inclusivity in leadership. Promotion of the PCC clinic is expected to rely heavily on grassroots efforts, including discussions during local meetings, women’s groups, ASHA workers, and informal platforms like WhatsApp groups. The community showed readiness to contribute financially, with suggested amounts ranging from INR 50/- to INR 1000/-, depending on individual economic capacity. This indicates a general willingness to support the clinic despite varying financial capabilities. Additionally, several potential locations for the clinic were identified, including Gram Panchayat offices, Anganwadi centers, schools, and even available rooms in PHCs or government hospitals. The need for coordination with local authorities, like the Sarpanch, was also emphasized. Overall, the analysis reflects strong community support for the PCC clinic, relying on local resources, networks, and leadership to ensure its success.
Contributions to preconception care: A thematic review from FGDs and IDIs.

PCC: preconception care; FGD: focus group discussion; IDI: in-depth interview; PHC: primary health center; ASHA: accredited social health activist.
The higher-order theme in Table 3 is expectations for PCC services, which captures the community’s anticipated services and support from PCC clinics. The community expressed the need for a broad range of healthcare facilities, including essential tests like blood tests, sonography, vaccines, and emergency care, particularly for conditions like infertility, asthma, and chronic diseases. Additionally, there is a strong demand for counseling services, covering areas such as family planning, safe pregnancy practices, hygiene, spacing between children, and counseling for newlyweds and in-laws. Affordability is a crucial factor, with many participants advocating for low or no fees, particularly for those living below the poverty line. The community also highlighted the importance of providing targeted health education for adolescent girls (Kishori) to prepare them for future motherhood. Respondents emphasized the need for both male and female doctors, gynecologists, and nurses, especially during emergencies, with nurses managing ongoing care after the first visit. Overall, the community’s expectations reflect a desire for comprehensive, affordable, and accessible PCC services, emphasizing the importance of education, counseling, and full medical support.
Expectations for PCC services: Thematic findings from FGDs and IDIs.

PCC: preconception care; FGD: focus group discussion; IDI: in-depth interview.
The Table 4 presents the ranking exercise analysis of facility expectations for PCC across various villages serviced by different PHCs in the region. This free listing and ranking exercise provide insights into the relative prioritization of different PCC packages based on the needs and preferences expressed by the communities. Nutritional conditions (NC) and health screening (HS) consistently rank high across most villages, indicating a widespread emphasis on basic health and nutrition as foundational to PCC. Anji PHC and Khrangana PHC show NC and HS frequently ranked in the top 3, suggesting strong community interest in nutrition-related interventions and regular health check-ups as priorities. Environmental health (EH) and addiction (Add) are generally ranked lower, particularly in villages like Bogaon Nandora and Dorali, where EH appears among the last three rankings. This might reflect either a lower perceived immediacy of environmental factors in preconception health or limited community awareness of how environmental issues impact maternal and child health. Similarly, addiction receives varied attention, with certain villages like Mandavgad ranking it as low as 9th or 10th, highlighting differing community attitudes or levels of concern toward substance use in the preconception phase. Genetic conditions (GC) and mental health (MH) rank in mid-level positions in several villages, indicating moderate awareness and concern. Karanji Kaji ranks GC and MH as fourth and fifth, respectively, showing some prioritization. This positioning could imply an understanding of genetic and mental health’s roles in family health but perhaps less urgency compared to other categories.
Expectations for PCC: Insights from free listing and ranking analysis.

NC: nutritional conditions, VPDs: vaccine preventable disease, GC: genetic conditions, EH: environmental health, Inf: infertility/subfertility, MH: mental health, FW: family well-being, IV: interpersonal violence, Add: addiction, HS: health screening, Cont: family welfare, Lm: lifestyle modification; PCC: preconception care; PHC: primary health center.
The comparison to the WHO-recommended PCC packages with our study reveals additional locally prioritized areas that enrich the traditional scope of PCC, reflecting specific community needs. HS emerged as a unique package, encompassing checks for conditions such as diabetes, hypertension, thyroid disorders, and general blood testing, beyond the WHO’s focus on preventing disease transmission. This inclusion highlights the community’s proactive stance on identifying and managing non-communicable diseases (NCDs) before pregnancy, a perspective aligned with the growing importance of NCD prevention in maternal and child health. Family well-being emphasizes family dynamics, social support, and education for young women (Kishori), touching on family planning education, child spacing, and reducing stigma around reproductive health. This package reflects the role of extended family in health decisions and the community’s cultural understanding that reproductive health involves family and societal structures. The community’s emphasis on family well-being suggests a culturally sensitive approach that values collective support as integral to a woman’s health journey. While lifestyle modification package marks a proactive approach to physical wellness, with a focus on exercise promotion, community-based physical activity programs, and overall quality of life enhancement. Unlike WHO’s emphasis on the cessation of harmful substances, this package underscores the community’s belief in positive lifestyle changes, recognizing exercise as a preventive measure that prepares individuals for a healthy pregnancy. The attention to physical well-being highlights the importance of quality of life in the preconception phase, resonating with an evolving understanding of holistic health. In our study, we integrated tobacco use and psychoactive substance use from the WHO package into a cohesive Add package, which incorporate the comprehensive approach to addiction prevention and treatment. This reflects a nuanced understanding of addiction, advocating for both health education and rehabilitation resources at the community level. The presence of this package signifies an awareness of addiction as a condition that requires support rather than solely a behavior to avoid. The final consensus on retaining specific PCC packages as shown in Figure 2 was achieved through collaborative decision-making involving the Technical Advisory Group (senior public health professionals, health administration members, obstetricians, gynecologists, and researchers with experience in PCC).
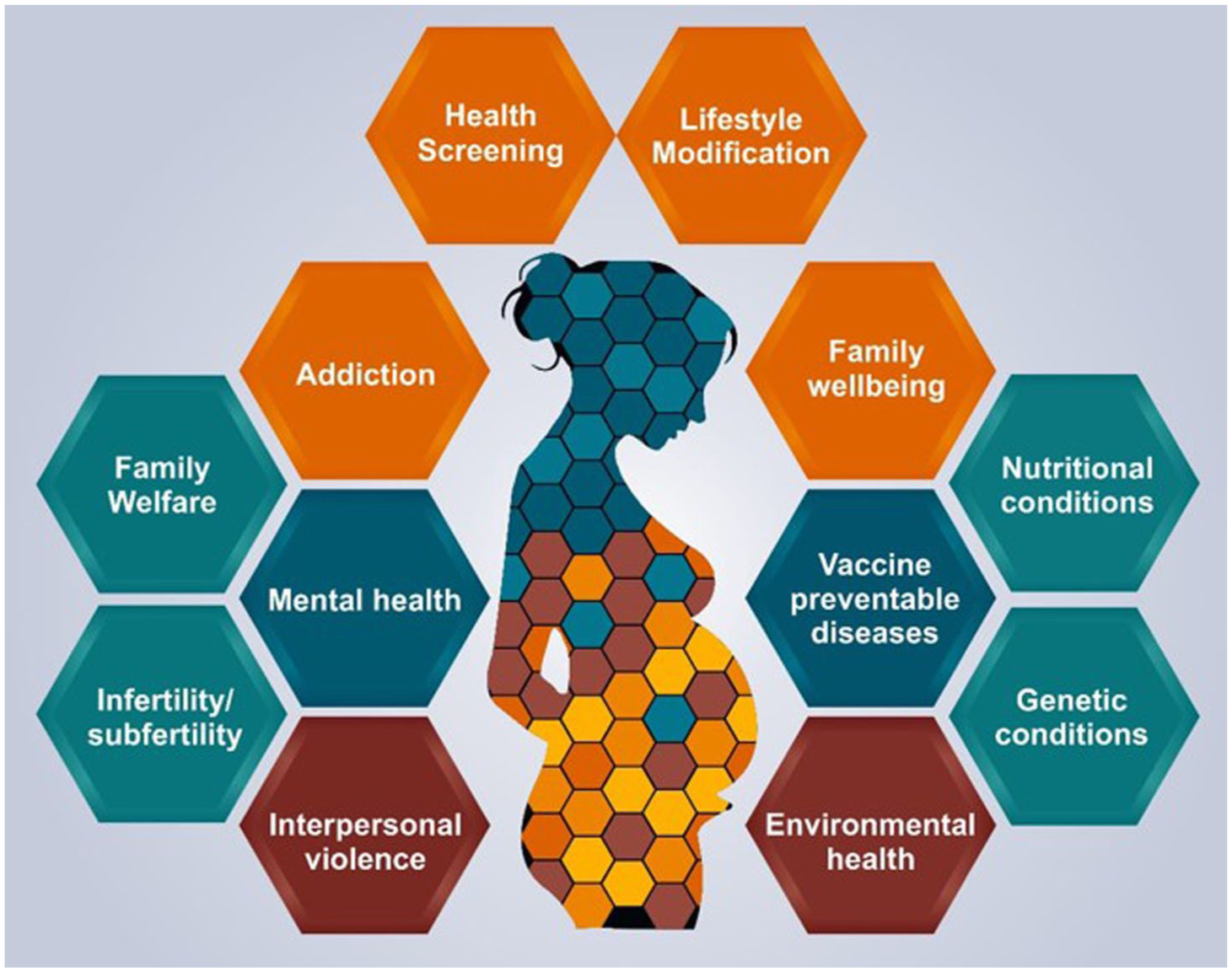
Research-based comprehensive preconception care packages.
Discussion
The community in this study showed a basic understanding of the benefits of PCC, such as better maternal and child health, safer deliveries, and the importance of pre-pregnancy care. However, many participants lacked awareness of specific services like genetic screening or early disease detection. For example, the limited understanding of genetic screening and early disease detection aligns with observations by Singh et al. 17 who noted that a lack of knowledge about genetic risks is a barrier to PCC adoption. Cultural factors, such as the preference for male children, continue to influence reproductive decisions, a pattern similarly reported in the Indian context, where gender norms often shape healthcare-seeking behaviors.10,11,12 Similar findings were reported by Doke et al., 18 who noted that rural populations often struggle with misconceptions and limited knowledge about PCC. These findings suggest the need for targeted educational interventions to address these knowledge gaps, as noted in educational initiatives about PCC awareness that emphasize community-tailored strategies to foster understanding and uptake.18–21
The community demonstrated a willingness to contribute to PCC, both financially and through active participation in clinic management. This finding resonates with the task-shifting approaches described by Deller et al., 22 where community health workers and other local actors played pivotal roles in promoting maternal and newborn health services in resource-limited settings. These findings echo recommendations by Chutke et al. 19 and Nomita Chandhiok et al., 10 who emphasized using local networks and health workers to deliver PCC in rural areas. However, the varying levels of financial contributions reported in this study suggest the need for flexible and inclusive funding mechanisms to ensure equitable access. This aligns with previous findings that emphasize the need for sustainable models combining community involvement with external support.17,21 This resonates with findings from Ojifinni et al., 23 where high costs and logistical issues were major barriers to PCC adoption in low-resource settings. Current study underscores the gaps in awareness and access to PCC services, pointing to the need for better integration of PCC within existing healthcare frameworks, similar findings are shown by Annadurai et al. 24 and Kolhe et al. 12
The community expressed a strong need for comprehensive PCC services, including essential health tests (e.g., blood tests, genetic screening), counseling on family planning, and education on healthy pregnancies. There was a particular focus on addressing NCDs like diabetes and hypertension, which reflects the growing recognition of their impact on maternal health. This aligns with Ebrahim et al., 25 who highlighted the importance of integrating preventive care, such as NCD management, into PCC programs. Additionally, the emphasis on family well-being and targeted education for adolescent girls (Kishori) underscores the need for culturally sensitive interventions that prepare young women for healthy motherhood.
Our findings align with many of the PCC elements recommended by WHO, but they also reveal additional priorities specific to the local context. For example, while WHO emphasizes preventing disease transmission, the community in this study prioritized HS and family well-being as critical components of PCC. HS emerged as a key package, addressing conditions like diabetes, hypertension, and thyroid disorders, which are not prominently highlighted in WHO’s guidelines. Similarly, the focus on family well-being, covering family dynamics, child spacing, and reducing stigma around reproductive health, adds a unique cultural dimension to PCC implementation.26,27 These locally enriched priorities highlight the importance of adapting global recommendations to meet the specific needs of the community.
One of the significant challenges identified in this study was the heavy workload on healthcare providers, which limits their ability to deliver PCC effectively. To address this, the study suggests task-shifting strategies, such as involving trained nurses to manage PCC clinics, which align with the findings by Chandhiok et al. 10 and Deller et al. 22 Similar approaches have been successful in other countries like Hong Kong and South Korea, where nurses and midwives play a central role in delivering PCC.21,23 However, for such strategies to succeed, there must be adequate training, supportive policies, and consistent resources to sustain these initiatives over time. According to few studies Daly et al., 28 Pimple et al., 29 and Narendra et al., 30 challenges such as poor compliance, low awareness, and weak program monitoring must be tackled to integrate PCC into India’s healthcare system, particularly to achieve Sustainable Development Goals by 2030, which aligns with the finding of the current study. The findings of study by Fussi et al. 31 and Phalke et al. 32 highlight a need for structured training programs to enhance awareness and practice among healthcare workers.
Limitations and recommendations of the study
While the study’s qualitative approach provides in-depth insights, its findings may have limited generalizability to other regions due to contextual variations. Differences in awareness and priority-setting across villages suggest heterogeneity in community perspectives, which may not capture the full spectrum of opinions. Additionally, economic concerns raised by participants point to potential challenges in implementing proposed PCC services, particularly with regard to affordability and access among underprivileged groups. Nevertheless, the inclusion of direct participant quotes enhances the richness of the findings and offers a nuanced understanding of community needs. The comparison with WHO-recommended PCC packages underscores the importance of locally prioritized areas such as HS, family well-being, and lifestyle modification. The community’s focus on trans-generational health issues and their expressed readiness to offer financial and logistical support highlight strong engagement and cultural adaptability. These findings make the study both practical and actionable for designing context-specific interventions.
Conclusion
This formative research provides valuable insights into the community’s understanding, contributions, and expectations regarding PCC. While the community recognizes the benefits of PCC, such as improved maternal and child health, safer deliveries, and inter-conception care, there remain significant gaps in awareness of key aspects like genetic screening, early disease detection, and self-care practices. The community demonstrated strong support for PCC clinics, with a willingness to contribute financially and manage clinics through local figures like ASHA workers, self-help groups, and educated youth. Preferred locations for clinics included Gram Panchayat offices, Anganwadi centers, and primary healthcare facilities, reflecting the community’s emphasis on accessibility and convenience. The comparison with WHO-recommended PCC packages reveals additional locally prioritized areas that address specific community needs. HS emerged as a key package, and Family Well-being package highlights the importance of family dynamics, social support, and education for young women, reflecting the cultural significance of collective decision-making in reproductive health. lifestyle modification and addiction package, these community-driven priorities enrich the traditional scope of PCC, emphasizing holistic, culturally sensitive strategies for maternal and child health. The current study highlights the community’s readiness to adopt PCC, provided services are affordable, accessible, and aligned with local priorities. By leveraging existing community networks and addressing gaps in awareness and healthcare delivery, PCC can be effectively integrated into existing healthcare frameworks to ensure better maternal and child health outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251400073 – Supplemental material for Understanding community perceptions, preparedness, and expectations of preconception care: A formative research approach
Supplemental material, sj-docx-1-whe-10.1177_17455057251400073 for Understanding community perceptions, preparedness, and expectations of preconception care: A formative research approach by Swati Misra, Kamlesh Mahajan, Mohini Gawai, Abhishek V. Raut, Poonam Varma, Rameshwar J. Paradkar, Shuchi Jain, Subodh S. Gupta and Bishan S. Garg in Women's Health
Footnotes
Acknowledgements
Our heartfelt gratitude to all the participants who generously shared their valuable time, insights, and experiences, enabling us to delve deeper into the community’s perceptions, preparedness, and expectations regarding preconception care (PCC). We are especially thankful to the community health workers—accredited social health activist, auxiliary nurse midwife, and local governing bodies for their support and collaboration during the study. Our sincere appreciation goes to the research team for their unwavering dedication and efforts in conducting this formative research. We also extend our gratitude to Mr. Dinesh for his invaluable assistance in creating our research-based comprehensive PCC package.
ORCID iDs
Ethics approval
Ethical approval for the research was obtained from the Institutional Ethics Committee (IEC) for Research on Human Subjects at Mahatma Gandhi Institute of Medical Sciences (IEC Approval No. IEC/406/2023, dated 30 December 2023). Verbal consent was then audio-recorded before beginning each interview or group discussion, in alignment with IEC-approved procedures.
Consent to participate
Verbal consent was audio-recorded before beginning each interview or group discussion, in alignment with IEC approved procedures.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study (Proposal ID: IIRP-2023-7250) and (File No: EMTR/SG/DEL/03/5 dated 21 December 2023) is being by funded the Indian Council of Medical Research (ICMR).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.