
Abstract
Background:
Caesarean section (C-section) rates in Mexico have risen dramatically over the past decade, reaching 55% by 2023. While life-saving when correctly indicated, excessive use may alter the natural timing of childbirth and shift population-level birth outcomes.
Objectives:
To examine national trends in gestational age, birth weight and birth length from 2010 to 2023, and evaluate their association with mode of delivery.
Design:
Population-based repeated cross-sectional analysis using national birth certificate data.
Methods:
We analysed a 1-in-1000 random sample of birth certificates from Mexico’s national registry (n = 27,435) for 2010–2023. Fractional polynomial models assessed national trends in birth outcomes by delivery type. Multivariable linear regressions adjusted for maternal age, parity, schooling and year of birth. Marginal effects were used to examine changes in C-section rates by maternal age.
Results:
The C-section rate rose from 45% in 2010 to 55% in 2023. Over the same period, full-term births (⩾39 weeks) declined from 66.5% to 57.7%, while early-term births (37–38 weeks) rose from 26.6% to 34.2%. Gestational age declined over time for both vaginal and C-section deliveries. A sharp rise in C-section rates beginning around 2015 coincided with abrupt downward trends in gestational age, birth weight, and length across delivery modes. In adjusted models, birth by C-section was associated with a reduction of 0.5 weeks in gestational age at birth (p < 0.001), increased risk of prematurity (β = 0.053, p < 0.001), and reductions in birth weight (β = −21.04 g, p = 0.001) and length (β = −0.41 cm, p < 0.001), compared to vaginal delivery.
Conclusion:
The rising prevalence of C-sections in Mexico aligns with a broader shift towards earlier deliveries, driven primarily by an increase in early-term births. This shift affects both surgical and spontaneous deliveries and may have long-term implications for children health.
Plain Language Summary
This study looked at changes in how and when babies are born in Mexico. In particular, we wanted to know whether the increase in caesarean section (C-section) births over the past decade has affected the timing of childbirth and newborn health. C-sections can save lives when medically needed, but they have become much more common in Mexico. In 2010, about 45% of all births were by C-section. By 2023, that number had risen to 55%. We wanted to understand how this trend might be influencing when pregnancies end and what that means for babies. To study this, we analysed a random sample of over 27,000 official birth records from across the country, covering the years 2010 to 2023. We looked at how the length of pregnancy (gestational age), baby’s weight and length at birth, and the type of delivery (C-section or vaginal birth) changed over time. We found that, as C-sections became more common, fewer babies were born at or after 39 weeks of pregnancy (which is considered full-term). Instead, more babies were being born at 37–38 weeks, which is called early-term. This shift happened not only for C-section deliveries but also for vaginal births, suggesting that hospital practices and scheduling may be affecting all deliveries. We also saw small but noticeable drops in average birth weight and length during the same period. These findings raise concerns that babies are being born earlier than necessary. While many early-term babies are healthy, being born even slightly early can increase the risk of breathing problems, time in intensive care, and long-term health issues. This study suggests that efforts to reduce unnecessary C-sections and encourage full-term births could benefit both mothers and babies.
Introduction
Caesarean sections (C-sections) are a critical medical intervention that can save the lives of mothers and newborns when medically necessary. 1 However, excessive use of C-sections without medical indications has been associated with negative health outcomes for both mothers and infants. 2 According to WHO’s most recent statement (2015), population-level C-section rates higher than 10% are not associated with further reductions in maternal or neonatal mortality. 3 In recent years, Mexico has experienced a dramatic increase in C-section rates, with nearly 55% of births occurring via this method by 2023. 4 This places Mexico among the countries with the highest C-section rates globally, far exceeding the WHO recommendations and comparable to levels observed in countries with the highest rates of medicalized births, such as Brazil and the Dominican Republic. 5
Despite advances in maternal and neonatal care, Mexico’s maternal mortality rate (MMR) and neonatal mortality rate (NMR) have shown stagnation in recent years, even as C-section rates have continued to climb. According to the Global Burden of Disease Study 2023, the MMR in Mexico decreased by 20% from 1990 to 2000 (74.8–59.6 deaths per 100,000 live births), by 23% from 2000 to 2010 (59.1–45.4), but only by 3% from 2010 to 2023 (45.4–44.1). 6 Similarly, the NMR dropped from 18.6 deaths per 1000 live births in 1990, to 7.8 deaths per 1000 live births in 2020, with a projected estimate of 7.3 neonatal deaths per 1000 live births in 2025, suggesting that further reductions are increasingly difficult to achieve. 7 These trends align with WHO reports indicating that exceeding an optimal C-section threshold does not necessarily yield further improvements in maternal or neonatal outcomes and may divert resources from cases where surgical intervention is truly needed. 3
A closer examination of the leading causes of neonatal mortality reveals a concerning association between rising C-section rates and an increasing burden of preterm and early-term births. Prematurity is the leading cause of neonatal mortality in Mexico, accounting for approximately 28% of neonatal deaths, followed by congenital anomalies (21%), neonatal infections, and birth asphyxia. 8 Many of these conditions are linked to shortened gestational duration, which can be influenced by elective or non-medically indicated C-sections. A rise in unnecessary C-sections has significant implications for maternal and neonatal health. When performed without medical necessity, C-sections can deprive foetuses of the chance to complete gestational development and be delivered naturally when due. 9 The interruption of this natural process has been associated with unintended negative consequences, including increased risks of respiratory distress syndrome,10–13 alteration of the microbiota,14,15 feeding difficulties,16–18 impaired immune development in newborns, 19 and increased risk of infection-related hospitalization in childhood.20,21
Emerging research also suggests that being born at early-term gestations (37–38 weeks) rather than full-term (39–40 weeks) may have lasting consequences on metabolic and cognitive development, potentially predisposing individuals to chronic diseases later in life.22–24
The increasing incidence of C-sections in Mexico raises important concerns regarding its impact on neonatal health. While the country has achieved substantial reductions in neonatal mortality, the decline in gestational age at birth due to the overuse of C-sections may be introducing new risks that were previously less prevalent. Understanding how this trend is affecting newborn outcomes is crucial for informing public health strategies aimed at optimizing birth practices and improving neonatal health.
This study aims to analyse national-level trends in gestational age, birth weight, and birth length in Mexico over the past decade, investigating the role of increasing C-section rates in shaping these outcomes. By evaluating changes in these indicators across different delivery modes, we seek to better understand how the growing prevalence of C-sections is influencing birth timing and neonatal health in Mexico.
Methods
Study design and population
This study employed a retrospective observational repeated cross-sectional design using publicly available birth certificate data from Mexico’s National Birth Registry (Subsistema de Información sobre Nacimientos (SINAC), for its acronym in Spanish) for the years 2010 to 2023, covering over 27 million births. According to a report issued by the Mexican Government in 2022, based on a nationally representative survey, approximately 97.5% of births occurring in the year prior to data collection had an official birth certificate issued by the Ministry of Health, which feeds into SINAC. 25 The SINAC database has been widely used for epidemiologic research on perinatal outcomes and is considered the primary source of national birth statistics in Mexico.4,26–29
Given the extremely large size of the national birth registry (over 27 million records for the period 2010–2023), we analysed a 1-in-1000 simple random sample (n ≈ 27,000) of birth certificates. This sampling strategy was selected for two main reasons. First, advanced modelling techniques such as fractional polynomial regression are computationally intensive, and fitting such models to the full dataset would require prohibitively large computing resources and could lead to convergence issues. Second, as is well recognized in statistical practice, very large sample sizes cause standard errors to shrink, leading to highly significant p-values even for associations of negligible practical importance. Using a large, random and nationally representative sample allows for robust inference while ensuring that hypothesis tests retain their intended interpretive value (i.e. distinguishing meaningful associations from trivial ones). To confirm representativeness, descriptive statistics for gestational age at birth, birth weight and length, and mode of delivery were compared between the analytical sample and the full registry, showing negligible differences (Supplemental Table 1).
To further document analytic precision, we estimated minimum detectable effect sizes under conventional assumptions (α = 0.05, two-sided; 80% power). Given the observed group sizes of 14,496 (vaginal) and 12,939 (caesarean), the design can detect between-group differences as small as 0.06 weeks in gestational age (SD = 1.76 weeks), 16 g in birth weight (SD = 479.96 g), and 0.10 cm in birth length (SD = 2.81 cm). For prematurity, using the overall prevalence (7.12%), the minimum detectable absolute risk difference is 0.87 percentage points. These calculations indicate high statistical sensitivity at the chosen sampling fraction.
Inclusion and exclusion criteria
The analytic sample comprised all birth records between 2010 and 2023 with valid information on the study variables (gestational age, birth weight, birth length, mode of delivery, maternal age, number of pregnancies, schooling, and year of birth). Observations with gestational age values <23 completed weeks were excluded from the analysis (representing 0.03% of all births). This threshold was selected because births occurring below 23 weeks are considered extremely preterm and generally regarded as non-viable in clinical practice, with very limited chances of survival outside highly specialized settings. Furthermore, gestational age values as low as 13 weeks were present in the registry, and their inclusion would have unduly influenced the results and potentially introduced significant bias. The 23-week threshold is supported by contemporary clinical guidelines and practice.30,31 The dataset was merged across multiple years and harmonized to ensure consistency in coding schemes and variable definitions.
Variables
The primary outcome variables were: gestational age (weeks), birth weight (g), birth length (cm). Births were categorized according to standardized gestational age definitions recommended by the American College of Obstetricians and Gynecologists (ACOG Committee Opinion No. 579, 2013) as follows: preterm (<37 weeks), early-term (37 weeks 0 days to 38 weeks 6 days), and full-term (⩾39 weeks 0 days). 32 A category corresponding to late-term or post-term pregnancies (⩾41 weeks) was not generated, as the analysis of this group was beyond the specific scope of this study. The main exposure variable was mode of delivery, categorized as C-section or vaginal birth. Covariates included: number of pregnancies, maternal age (years), schooling (in categories: less than primary, complete primary education, and complete secondary education), and year of birth.
We assessed the completeness of all analytic variables. Missingness for gestational age was (n = 71, 0.26%), birth weight (n = 1305, 4.8%), birth length (n = 456, 1.7%), maternal age (n = 45, 0.16%), number of pregnancies (n = 8, 0.03%) and schooling (n = 287, 1.1%). All records included information on mode of delivery and date of birth.
Statistical analysis
To assess temporal trends in gestational age, birth weight and birth length, fractional polynomial regression models were applied to capture potential nonlinear patterns over time. Fractional polynomial models were estimated with the maximum polynomial degree set to 2. The best-fitting model was selected according to the default criterion of minimum deviance (i.e. lowest Akaike Information Criterion). These models allow for flexible trend estimation without imposing restrictive assumptions of linearity. 33 Since our objective was to assess national trends and not to produce state- or municipality-level estimates, no stratification was required. To explore differences in birth outcomes by delivery type, separate regression models were estimated for C-section and vaginal births. Additionally, marginal effects and predictive margins were computed to illustrate how gestational age, birth weight and birth length varied across different delivery modes over time.
To evaluate the association between delivery mode (C-section versus vaginal) and birth outcomes, linear regression models were fitted, adjusting for maternal age, year of birth, number of pregnancies and schooling. Prematurity was analysed as a binary variable (<37 weeks versus ⩾37 weeks) in regression models. Interaction terms were included where relevant to assess modifying effects, particularly interactions between gestational age and maternal age in determining the occurrence of a C-section. Robust standard errors were used to account for heteroskedasticity in linear probability models (for C-section and prematurity). 34 Temporal trends in birth outcomes were evaluated by including ‘year’ as a continuous predictor in the regression models. A statistically significant trend was defined as a p-value <0.05 for the year coefficient. All models were estimated using a complete case approach, meaning that only records with valid (non-missing) values for the outcome, exposure and covariates were included in each analysis.
Data cleaning and preparation, and all statistical analyses, were conducted using Stata v18 (StataCorp. 2023. Stata Statistical Software: Release 18; StataCorp LLC, College Station, TX, USA). The reporting of this study conforms to the STROBE guidelines for cross-sectional studies. 35
Ethics and consent
This study used publicly available, de-identified birth registry data. Because the dataset contained no personal identifiers, neither ethics approval nor informed consent was required, in accordance with guidelines for secondary data analysis of anonymized data.
Results
The sample included 27,435 births (representing over 27 million births during the study period), with 47% delivered via C-section. The mean gestational age at birth was 38.5 weeks (SD = 1.7 weeks). Average birth weight and length were 3200 g (SD = 478 g) and 49.8 cm (SD = 2.8 cm), respectively. Mothers in the sample ranged in age from 15 to 45 years, with a mean age of 27.6 years. Full descriptive statistics by mode of birth are displayed in Table 1.
Descriptive characteristics of the study population by mode of birth, Mexico, 2010–2023. The table presents counts and percentages for categorical variables, and means with standard deviations in brackets for continuous variables. Differences by mode of delivery are shown for infant sex, gestational age at birth (weeks), birth weight (g), birth length (cm), maternal age (years), number of pregnancies and preterm birth (<37 weeks). All estimates are based on a 1-in-1000 simple random sample of national birth certificates.

SD: standard deviation.
The proportion of births delivered by C-section remained relatively stable from 2010 to 2014, fluctuating between 44% and 46% (p-for-trend = 0.112). Beginning in 2015, the trend shifted, and C-section rates began to increase steadily (p-for-trend <0.001). By 2023, more than 55% of births were delivered via C-section, representing an absolute increase of over 10 percentage points in less than a decade. This upward trend was consistent across the latter half of the period and is depicted in Figure 1. Interaction models indicated that this rise was more pronounced among older mothers. Marginal effects analysis demonstrated that the annual increase in the percentage of C-sections was 0.4 percentage points for 15-year-old mothers but rose to 0.8 percentage points for 45-year-old mothers.

Temporal trend in the proportion of births delivered by caesarean section in Mexico, 2010–2023. Estimated using fractional polynomial regression. The solid line represents the predicted proportion of C-sections, and the shaded area indicates the 95% confidence interval of the prediction.
The distribution of gestational age at birth shifted notably between 2010 and 2023. The proportion of full-term births (⩾39 weeks) decreased from 66.5% in 2010 to 57.7% in 2023, while early-term births (37–38 weeks) increased from 26.6% to 34.2%. The share of preterm births (<37 weeks) fluctuated between 5.7% and 8.4%, without a clear upward trend. These changes reflect a gradual leftward shift in gestational age distribution, with a growing concentration of births occurring before 39 weeks (Figure 2 and Supplemental Table 2).
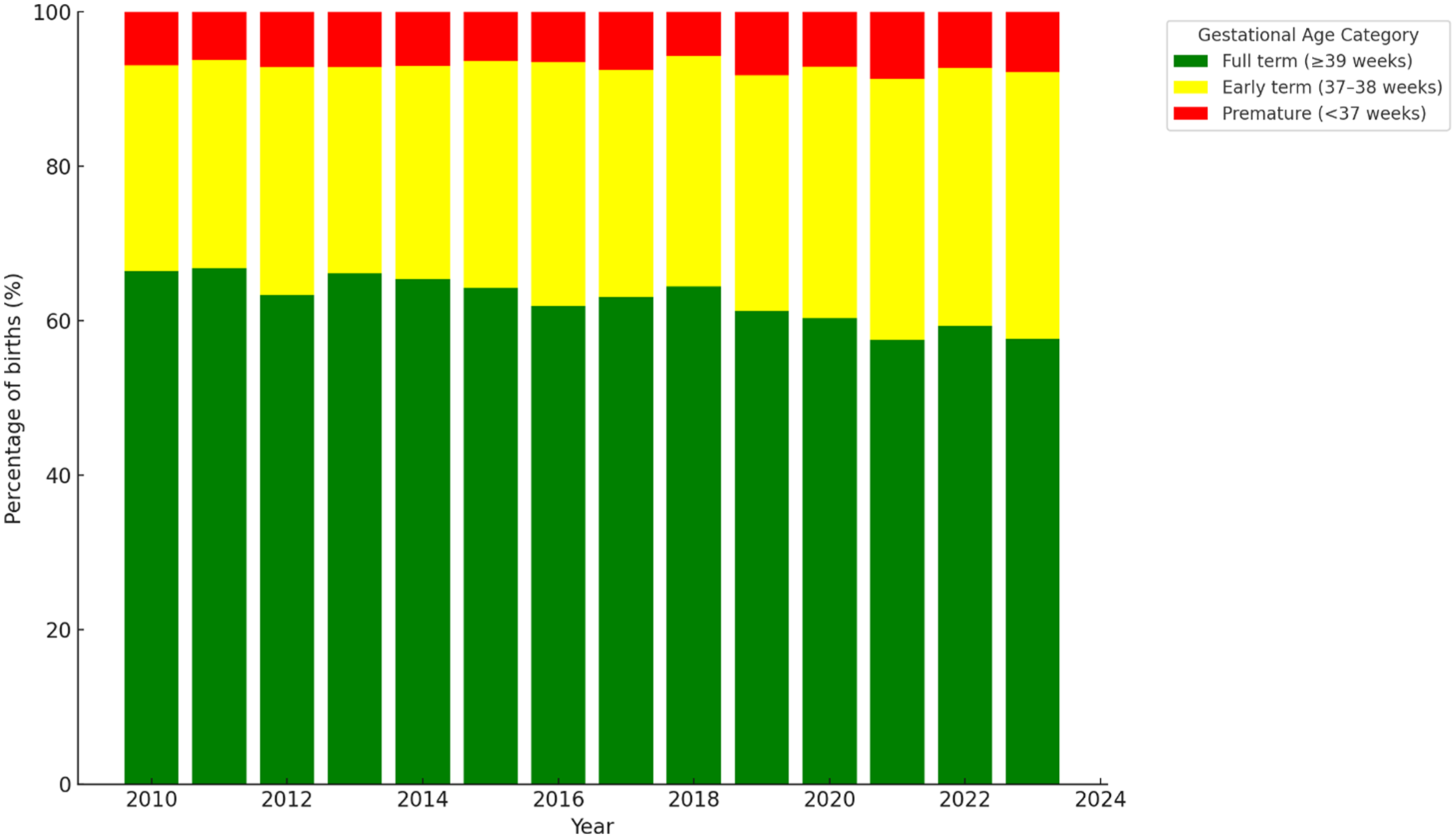
Distribution of gestational age at birth in Mexico, 2010–2023. The figure shows the annual percentage of births classified as preterm (<37 weeks), early-term (37–38 weeks) and full-term (⩾39 weeks).
Analysis revealed a statistically significant decline in gestational age over the study period. This downward trend occurred for both delivery modes, as shown in Figure 3. The trend was significant for both delivery modes (change for vaginal births: β = −0.011 weeks/year, p = 0.004; for caesarean births: β = −0.021 weeks/year, p < 0.001). Across the entire study period, births delivered by C-section occurred on average 0.5 weeks earlier than those delivered vaginally (β = −0.500, 95% CI: −0.54 to −0.46, p < 0.001), after adjustment for year, maternal age, number of pregnancies and schooling (Table 2). This reflects an overall difference attributable to mode of delivery, irrespective of the year of birth. Prematurity increased modestly at a rate of approximately 0.1 percentage points per year (β = 0.001, p = 0.008), representing an absolute yearly increase in the proportion of preterm births, although the trend was less pronounced than for gestational age.
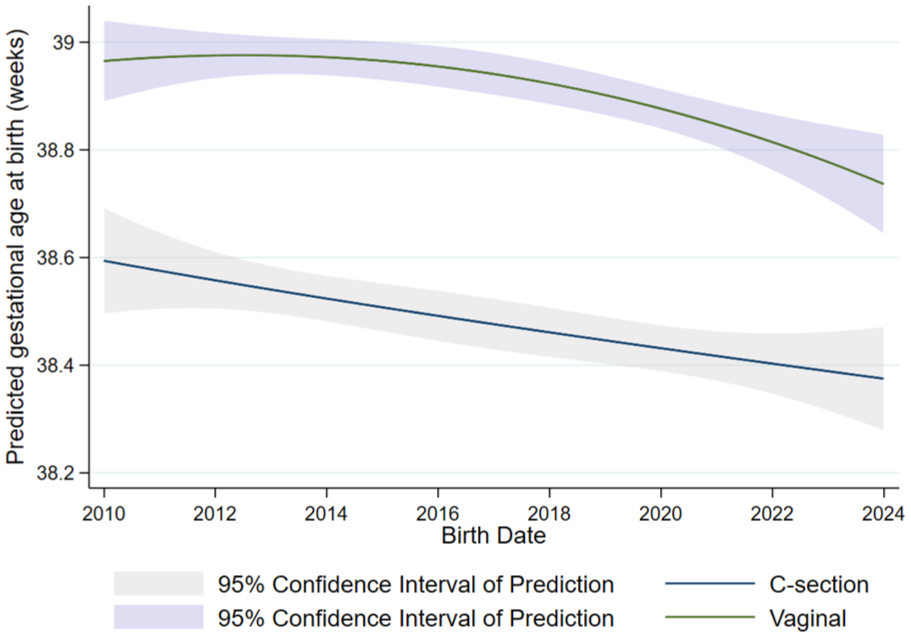
Fractional polynomial regression of gestational age at birth by mode of delivery, Mexico, 2010–2023. Estimated predicted mean gestational age is plotted separately for caesarean and vaginal deliveries. Shaded areas represent 95% confidence intervals of the prediction.
Estimates from multivariable linear regression models predicting gestational age, prematurity, birth weight and birth length. Each column represents a separate model. All models adjusted for delivery mode, year of birth, maternal age and number of pregnancies.

p-value in brackets. C-section: caesarean section.
Robust standard errors.
p < 0.1. **p < 0.05. ***p < 0.01.
Birth weight and length both displayed a convex pattern over time, with clear peaks in the mid-2010s followed by sustained declines (Figure 4). For birth length, vaginal deliveries rose to just above 50.2 cm around 2014–2015 before entering a gradual decline, while C-section deliveries peaked slightly lower in the same period and then decreased more steeply, reaching ~49.3 cm by 2023. A similar trajectory was observed for birth weight: vaginal deliveries increased to nearly 3170 g in 2014–2015 and then declined sharply after 2016, while C-section deliveries followed the same pattern but remained consistently lower, ending near 3090 g in 2023. Over the whole period, babies delivered via C-section weighed on average, 21 g less than those delivered vaginally (p = 0.001) and length showed a mean reduction of 0.41 cm associated with C-section deliveries (p < 0.001).

Fractional polynomial regressions of birth length (left) and birth weight (right) by mode of delivery, Mexico, 2010–2023. Estimated means for birth length (cm) and weight (g) are plotted separately for caesarean and vaginal deliveries. Shaded areas represent 95% confidence intervals of the prediction.
Maternal age was positively associated with birth weight (β = 1.63 g/year of age, p = 0.004), birth length (β = 0.006 cm/year of age, p = 0.021) and prematurity (β × 100 = 0.01 percentage points per year of age, p = 0.008), while showing a weak negative association with gestational age (−0.010 weeks/year of age, p < 0.001). The number of pregnancies was positively associated with birth weight (β = 16.87 g per pregnancy, p < 0.001) but only marginally with birth length (β = 0.027 cm per pregnancy, p = 0.085), and was also linked to a modest increase in the probability of prematurity (β × 100 = 0.3 percentage points per pregnancy, p = 0.021). Conversely, the number of pregnancies was not significantly associated with gestational age. Finally, schooling, particularly having at least completed secondary school, was associated significantly to a decrease in gestational age at birth, and an increase in birth length and weight, but not with prematurity. Complete model estimates are shown in Table 2.
Discussion
Our findings provide evidence that the increasing prevalence of C-sections in Mexico, rising from 45% in 2010 to 55% in 2023, has significantly contributed to the decline in gestational age at birth. This reduction in gestational age is not primarily driven by an increase in premature births, but likely by a systemic shift in obstetric practice, where deliveries – particularly those via C-section – are occurring earlier than in previous years.
The precise drivers of Mexico’s rising C-section rates are an active area of research and debate.35–39 In the analysed data, while the likelihood of undergoing a C-section increases with maternal age, the annual increase is relatively modest for younger mothers (0.3 percentage points per year for 15-year-olds) but more pronounced for older mothers (1.0 percentage point per year for 45-year-olds). This suggests that while rising maternal age contributes to the overall increase in C-section rates, it does not fully account for the observed trends in gestational age decline. Instead, it is likely that shifting obstetric practices, rather than demographic changes alone, are the primary drivers of this trend. Potential explanations brought forward include economic and institutional factors, such as insurance payment structures that incentivize surgical over vaginal deliveries, hospital specialization in surgical obstetrics (partly in response to higher obesity prevalence) and socio-economic disparities associated with urban settings, higher maternal education and private healthcare use.36–40
A particularly striking observation is that gestational age has declined not only for births via C-section but also for vaginal deliveries. This decline began around 2015 and mirrors the inflection point in the upward trend of C-sections. This synchronicity suggests that the rising prevalence of scheduled C-sections is not merely affecting the surgical subset of births but is subtly reshaping the broader distribution of gestational age across all deliveries. From the gestational age by delivery type plot, vaginal births appear remarkably stable in gestational timing up to ~2015. The post-2015 decline suggests a spillover effect of elective early C-sections onto the residual pool of vaginal deliveries – possibly due to less tolerance for postdates or hospital routines nudging towards earlier admission or intervention. This reflects a cultural or systemic shift in obstetric decision-making, not just clinical indication. As a growing proportion of pregnancies are electively ended before full-term via C-section, spontaneous vaginal births increasingly represent those that happen to occur earlier by chance. In this context, later-onset spontaneous labours (e.g. after 39–40 weeks) are effectively being ‘selected against’, not through direct intervention in vaginal deliveries, but because those pregnancies are no longer reaching full-term to begin with. This indirect selection effect alters the natural curve of gestational age among vaginal births, producing a leftward shift in the entire population’s distribution. The net result is a systemic shortening of pregnancy duration across delivery modes, even in the absence of direct obstetric action on vaginal births, reshaping the broader distribution of gestational age across all deliveries.
Consistent with this, the proportion of full-term births (⩾39 weeks) has dropped from over two-thirds in 2010 to under 58% by 2023, while early-term births (37–38 weeks) have risen nearly 8 percentage points. The proportion of preterm births has fluctuated from 5.7% to 8.4% over the study period, with no consistent directional trend. These figures underscore a sustained and measurable compression of gestational length, predominantly affecting term births.
Regression models confirm these trends. After adjustment for covariates, the negative coefficient for year (−0.016 weeks/year, p < 0.001) indicates a steady temporal decline in gestational age, even after adjusting for delivery type, maternal age, parity and schooling. C-sections are indeed associated with an increased likelihood of premature birth, and although there was a significant upward trend in prematurity, this was comparatively less pronounced that that for gestational age in general. This supports the interpretation that most of the observed shift is occurring within the term range rather than due to rising preterm deliveries.
Visual trends in birth weight and length further support the interpretation of an accelerated shift towards earlier deliveries (Figure 1). From 2010 to approximately 2015, both parameters exhibited a rising trend, consistent with more pregnancies reaching full-term. However, this upward trajectory halts and reverses precisely when the proportion of C-sections begins to increase more steeply. From that point forward, both birth weight and length decline sharply across delivery modes. This synchronicity strengthens the argument that the increasing medicalization of delivery timing – particularly through elective C-sections – is compressing gestational age at the population level. Although the average cross-sectional differences between modes of delivery are on the order of 21 g and 0.4 cm, the longitudinal pattern shows a cumulative erosion of foetal growth potential over time, particularly after 2015. This pattern suggests that growing numbers of infants are being delivered before they reach their maximal in utero growth trajectory, possibly missing a critical window for maturation. Given the well-established associations between early-term birth and long-term health outcomes, this emerging trend merits attention not only for its epidemiological coherence but also for its potential clinical consequences.
Recent population-level studies from a variety of countries demonstrate that rising C-section rates are consistently associated with modest but measurable reductions in average birth weight and length at the population level. Analyses of national datasets, such as the U.S. cohort of over 23 million births (1990–2013), show that as C-section and elective induction rates have increased, the mean length of gestation has shortened by nearly a week, resulting in a significant downward shift in mean birth weight (e.g. ~67–79 g lower than would be expected if intervention rates had remained stable). 41 Our findings in Mexico align closely with these trends: as C-section rates rose from 45% to 55% between 2010 and 2023, there was a clear redistribution of births towards earlier gestational ages (from ⩾39 to 37–38 weeks), with corresponding declines in both birth weight and length. International studies, have similarly found that infants delivered by C-section are more likely to be of lower birth weight and shorter length compared to those born vaginally, particularly when C-sections are performed electively at early-term.42–45 The shift is consistent and appears to be driven by the truncation of gestation that occurs when deliveries are scheduled before 39–40 weeks.
High C-section rates have been associated with a downward shift in gestational age at birth in many populations. In Brazil, for example, the rise of elective C-sections has coincided with a marked increase in early-term births (37–38 weeks): in one city, the proportion of babies born by C-section at 37–38 weeks jumped from 28% in 1978–79 to 68% by 2010. 46 National analyses show a similar pattern – municipalities with extremely high C-section usage have far more babies born early-term. In this study, it was found that in Brazilian towns where >80% of deliveries were by C-section, the rate of 37–38 week births was 62% higher than in towns where C-sections were <30%. These high-C-section locales also saw a 22% higher risk of babies being born preterm (<37 weeks), suggesting that non-medically indicated C-sections are often performed earlier than necessary. 46 A study in rural China likewise reported that medically unnecessary C-sections tend to occur at lower gestational ages within the term period. 47 In that study, over 40% of C-sections were clearly elective, and C-section delivery was significantly associated with a shorter full-term gestation. Similar trends have been observed in other highly medicalized settings – for instance, in the United States the mean gestational age at birth fell by more than half a week (from ~39.1 to 38.5 weeks) between 1990 and 2020, largely attributed to increases in scheduled early deliveries. 48 These data illustrate that as C-section rates climb, a growing fraction of births are shifted into the early-term period (and even late preterm range), rather than the natural 39–40+ week timeframe.
The proliferation of early-term births (37–38 weeks) driven by elective C-sections has raised concerns because babies delivered even slightly early can face higher risks at birth and beyond. Neonatal outcomes are noticeably poorer on average for early-term infants compared to full-term (39–40 weeks) infants. A population study in Turkey reported that early-term deliveries comprised about 26% of all births and were far more likely to require neonatal intensive care – the neonatal intensive care unit (NICU) admission rate among 37–38 week infants was 7.5%, with significantly higher incidence of respiratory distress (38% versus lower in full-term), jaundice, hypoglycaemia, feeding difficulties and other morbidities. 49 Notably, the vast majority of these early-term babies were delivered by C-section, underlining the role of elective delivery timing. Findings from other settings echo these concerns. An Iranian cohort study found that scheduling a C-section at 38 weeks instead of waiting until ⩾39 weeks led to a marked increase in transient tachypnoea of the newborn and NICU admissions for breathing problems. 50 In short, infants born even a week or two early (often due to planned C-sections) face heightened risks of immediate respiratory complications, longer hospital stays and readmissions in the first days of life. These avoidable neonatal risks have prompted experts to recommend against elective deliveries before 39 weeks in healthy pregnancies.
Beyond the neonatal period, research suggests that early-term birth can have long-term implications for child health and development. Although early-term infants are officially ‘term’, their last few weeks in utero are a critical period for organ maturation (brain, lungs, metabolic systems, etc.), and shortening this period may subtly affect developmental outcomes. Large population studies in Scandinavia and elsewhere have linked 37–38 week births to slightly poorer neurodevelopmental outcomes compared to 39–40 week births. 51 For instance, a Scottish study 400,000+ children found that babies born at 37–39 weeks were significantly more likely to need special education that those born at 40 weeks or more. 52 Likewise, a systematic review reported that children born early-term have higher rates of mild cognitive deficits, poorer school performance, and behavioural problems relative to full-term peers. 53 These effects, while modest on an individual level, appear consistently in large samples. In rural China, a study of over 2700 infants observed a clear gradient in developmental scores by gestational age – every additional week of gestation up to 40 weeks was associated with higher cognitive, language and motor development scores in infancy. 47 Importantly, that study implicated unnecessary C-sections in potentially stunting this late-gestation developmental boost, since elective C-sections cut short otherwise healthy pregnancies.
Respiratory and immune outcomes in the longer term have also been linked to early-term birth. Epidemiological research shows that infants born at 37–38 weeks have a modestly higher risk of childhood asthma and wheezing disorders compared to those born at 39–40 weeks. A recent national cohort study in Sweden (which controlled for confounders and even compared siblings) found that early-term birth was associated with about a 13% increase in asthma risk through childhood into mid-adulthood. 54 This suggests that even a slight curtailment of gestation can leave lasting effects on pulmonary development or immune programming. There is also emerging evidence of metabolic consequences. Early-term birth has been associated with higher rates of childhood overweight and possibly other metabolic issues. An Israeli population study reported that children delivered at 37–38 weeks showed elevated rates of obesity and even early-life type 1 diabetes by adolescence. 23 Researchers speculate that early-term infants miss out on final weeks of in utero metabolic conditioning and may experience altered gut microbiota (especially since many are C-section delivered), which could predispose them to metabolic dysregulation later.
Limitations
Our study has several limitations. Most notably, the birth certificate dataset does neither provide information on the clinical indications for C-section, nor does it capture obstetric complications such as pre-eclampsia or chorioamnionitis. This limits our ability to address confounding by indication and to adjust for other relevant pregnancy factors. Additionally, the recording of gestational age is not standardized and may be subject to misclassification. While we adjusted for available maternal characteristics, residual confounding from unmeasured variables remains possible. Moreover, residual confounding by unmeasured social determinants cannot be excluded, as we were unable to adjust for socio-economic status as a potential confounder, due to the absence of detailed individual-level socio-economic data in the national birth registry. However, information on maternal education (a usual proxy of socio-economic status) was indeed available, and the estimates reported here account for it. We acknowledge these constraints and recommend that future studies incorporating more granular clinical data are needed to further elucidate the mechanisms underlying the trends we observed. Lastly, although no formal a priori power analysis was conducted, minimum detectable effect size calculations based on the overall variability and sample sizes indicate ample statistical power for the intended national-level analyses.
Conclusions
In summary, rising C-section rates in several Latin American and other highly medicalized countries have led to more births occurring at 37–38 weeks, shifting the gestational age distribution earlier. These early-term, often elective, births carry incrementally higher risks for neonatal respiratory complications and NICU admission and have been associated with subtle but measurable long-term disadvantages in cognitive development, respiratory conditions (such as asthma) and metabolic outcomes. These findings underscore the importance of avoiding non-essential C-sections and of carefully considering the timing of planned deliveries. Policies that promote delivery closer to 39–40 weeks –when medically appropriate – may help improve newborn and child health outcomes. Each additional week of gestation up to full-term confers developmental and physiological benefits that should be weighed against the perceived convenience of early elective delivery.
Moreover, the rise in C-sections over the past decade has coincided with a stagnation in progress towards reducing maternal and neonatal mortality. Excessive use of C-sections may divert resources away from high-risk pregnancies, potentially increasing overall maternal risk without offering clear survival benefits.
Our findings highlight the urgent need for policy interventions to reduce non-medically indicated C-sections and promote evidence-based, physiologically respectful obstetric care. Strategies may include stricter guidelines for scheduling elective C-sections and public health campaigns emphasizing the benefits of full-term gestation. In Mexico, an important step in this direction is the recent publication of an Official Mexican Norm on Midwifery, which calls for the integration of all forms of professional midwifery into hospitals and birth centres. 55 This initiative aims to support normal deliveries and foster collaborative care models alongside medical personnel. Additionally, further research is needed to explore the institutional and economic drivers of early deliveries, including physician incentives, hospital policies, and maternal preferences.
In conclusion, the increasing rate of C-sections in Mexico is not only altering gestational age distributions but may also have far-reaching consequences for neonatal and maternal health. As the likelihood of full-term vaginal births declines, efforts should be directed towards ensuring that obstetric care prioritizes evidence-based decision-making to optimize maternal and neonatal outcomes. Addressing the over-medicalization of childbirth requires a coordinated effort involving policymakers, healthcare providers, and public health initiatives to safeguard the health of future generations.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251399895 – Supplemental material for The impact of excessive caesarean deliveries on gestational age at birth in Mexico: National-level trends, 2010–2023
Supplemental material, sj-docx-1-whe-10.1177_17455057251399895 for The impact of excessive caesarean deliveries on gestational age at birth in Mexico: National-level trends, 2010–2023 by Héctor Lamadrid-Figueroa and Jimena Fritz in Women's Health
Footnotes
Acknowledgements
None.
Ethical considerations
This study used publicly available, anonymized administrative birth registry data. Because the dataset contains no personal identifiers, ethics approval was not sought or required.
Consent to participate
Not applicable. The study relied exclusively on anonymized administrative data, so individual informed consent was not sought or required.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.