
Abstract
Background:
While diet and activity interventions are modestly effective, sufficient sleep is crucial to weight loss success but is often not a focus in postpartum programs.
Objectives:
To identify (1) perceived factors affecting sleep, diet, and physical activity of postpartum individuals, (2) how these behaviors influence one another, and (3) how interventions can be designed to address them.
Design:
Qualitative study using individual semi-structured interviews with postpartum individuals.
Methods:
Fourteen postpartum individuals were interviewed to explore their experiences, perspectives, and needs regarding sleep, diet, and physical activity. They were also asked to share thoughts and suggestions regarding potential interventions. All interviews were transcribed verbatim, and transcriptions were double-coded using an inductive approach. Coded transcripts were examined for patterns, categories, and themes.
Results:
Four themes were identified: (1) participants identified modifiable cognitive factors (e.g., sleep-related worry) and behavioral factors (e.g., social media use) impacting sleep after childbirth. (2) They noted that fatigue from poor sleep hindered postpartum exercise, yet exercise improved both mood and sleep quality. (3) While wanting to maintain a healthy diet, fatigue from inadequate sleep influenced their food choices. (4) Participants suggested flexible interventions—including online resources and support during well-child visits—that provide sleep education, tailored nutritional guidance for breastfeeding, structured exercise programs, and peer support.
Conclusion:
Postpartum individuals perceive an interconnectedness among sleep, diet, and physical activity and are interested in flexible interventions that address all three behaviors simultaneously.
Plain language summary
Many people experience changes to their sleep, eating habits, and physical activity after having a baby. These changes can affect their ability to lose weight and stay healthy after childbirth. While past programs have tried to help with diet and exercise, they often don’t focus on sleep, even though poor sleep can make it harder to eat well and stay active. We interviewed 14 postpartum individuals to learn more about how sleep, diet, and physical activity affect each other, and how future programs could support these behaviors in a more connected way. Participants described feeling too tired to cook or exercise, often turning to quick snacks and skipping movement. Many also said stress, worry, and screen time made it hard to fall asleep. At the same time, some people found that when they were able to be active, it helped them sleep better and feel more in control of their eating. Participants said they would like flexible, practical support that fits into their daily routines. They wanted guidance on sleep, tailored nutrition advice, structured but simple movement options, and opportunities to connect with other new parents. They also suggested that online tools and pediatric visits could be good times to offer this help. This study shows that sleep, diet, and activity are deeply connected in the postpartum period. By designing programs that address all three together, and that work within the realities of new parenthood, we may be better able to support long-term health after childbirth.
Introduction
Postpartum weight retention increases the risk of adverse maternal outcomes (e.g., pre-eclampsia, gestational diabetes)1,2 in subsequent pregnancies, as well as obesity and cardiovascular disease development later in life.3 –10 In addition to its physical health consequences, postpartum weight retention is associated with more severe experiences of postpartum depression and anxiety. 11 Given the growing recognition that pregnancy and the postpartum period represent critical windows for long-term health promotion, 12 identifying effective, acceptable strategies to reduce postpartum weight retention is a public health priority.
While numerous interventions have addressed postpartum weight retention through strategies emphasizing calorie restriction and physical activity promotion,13 –30 the effectiveness of these postpartum interventions remain modest at best.31 –33 The modest success of postpartum interventions points to a complex interplay of weight-affecting factors (e.g., sleep) beyond diet and exercise. Emerging evidence suggests that sleep disturbances, highly prevalent among postpartum individuals,34 –36 may play a pivotal role in postpartum weight retention. Sleep is independently associated with obesity through its effects on energy-regulating hormones, energy metabolism, energy expenditure, and increased eating opportunities.37,38 Data from randomized controlled trials suggest that poor sleep quality at the study baseline lowers the odds of successful weight loss in diet and physical activity interventions.39,40 Moreover, data from randomized controlled trials in general adult populations suggest that addressing sleep, diet, and physical activity together is more effective than intervening on diet and physical activity alone. 41 Diet, sleep, and physical activity are interrelated, circadian-regulated behaviors that influence one another biologically and behaviorally. Reflecting this interconnection, the American Heart Association recently added sleep to its cardiovascular health framework (Life’s Essential 8), recognizing it as a core health behavior, alongside diet and physical activity, that supports cardiovascular health across the lifespan. 42
Despite this growing evidence, the development of multi-behavior change interventions that incorporate sleep in the postpartum period remains limited, partly due to a lack of foundational data on how postpartum individuals experience and manage these interconnected behaviors. To design effective and acceptable interventions, it is essential to understand the lived experiences, behavioral drivers, and support needs of individuals in the postpartum period. Qualitative research is uniquely suited to generate these insights, especially in early-phase intervention development, by uncovering context-specific challenges and preferences that may not be captured through quantitative methods alone.43,44 This study aimed to fill the knowledge gap by conducting semi-structured interviews with postpartum individuals to gain insights into (1) the perceived factors that impact the sleep patterns, diet, and physical activity of postpartum individuals, (2) perspectives on how these behaviors influence each other, and (3) perspectives on how interventions could address the three behaviors together. The data generated from this study are significant because they provide important insights into how future interventions can be designed to support multiple interrelated health behaviors in a holistic and practical way.
Methods
Study overview
This study uses a Qualitative Description approach, a common method for qualitative studies in health sciences contexts. As Sandelowski describes, the goal of qualitative description is to provide a comprehensive description of the individual’s experiences in a way, that is, both accessible and reflective of their lived experiences without imposing complex theoretical interpretations. 45 By focusing on describing the participants’ experiences, we aim to gain insights that can inform the development of interventions. This method is particularly well-suited for exploring the interconnection of sleep, diet, and physical activity postpartum and how participants believe these behaviors can be supported through holistic interventions. The reporting of this study conforms to the Consolidated Criteria for Reporting Qualitative Research checklist (Supplemental Appendix 1). 46
Participants
This study used a purposive, heterogeneous sampling approach to enroll postpartum individuals who could provide insight relevant to the study’s aims. The sampling approach was designed to ensure diversity in race, with the goal of exploring cross-cutting themes and patterns. Inclusion criteria were: (1) age 18 years or older, (2) gave birth within the past 12 months, (3) not currently pregnant at the time of the interview, and (4) the ability to complete the interview in English. There were no specific exclusion criteria. Participants were recruited from Allegheny County, PA, USA, using Pitt+Me, an extensive clinical research registry maintained by the University of Pittsburgh’s Clinical and Translational Science Institute 47 and Pittsburgh Brown Mamas, 48 a local pregnancy and postpartum advocacy group. Interested individuals were contacted by research team members who assessed eligibility and collected general demographic information (i.e., participants’ age, infant age, current pregnancy status). To support the consent process, participants were emailed a digital copy of the consent form in advance of scheduling the interview, giving them time to review the study details, and ask questions. Verbal informed consent was obtained immediately before the interview, after eligibility screening, and before data collection began. Interviews were conducted in-person and virtually (following COVID-19 safety protocols) between March and November 2020. The University of Pittsburgh’s Institutional Review Board approved the use of verbal consent as this was deemed a minimal-risk study (protocol #19110195).
Interview guide development
The study team collaboratively developed the interview guide to capture the participants’ lived experiences after childbirth in their own words (Supplemental Appendix 2). The core questions, “Tell me about your diet,” “Tell me about your sleep,” and “Tell me about your physical activity,” were chosen to allow participants to provide broad, open-ended descriptions of their everyday experiences. Another core question, “How do these behaviors impact each other?” was intended to explore the interconnectedness of sleep, diet, and physical activity, which is a central focus of this study. By prompting participants to describe how these behaviors influence one another, the aim was to capture how changes in one behavior (e.g., disrupted sleep) might affect another (e.g., poor diet or lack of physical activity). Follow-up prompts, such as “What have you tried to do to address those behaviors?” and “What does your nighttime routine look like?” were asked to obtain descriptions of specific actions or interventions they have tried to improve each behavior. Finally, participants were asked, “What would you like to see in an intervention that addresses these behaviors?” to gather participants’ ideas for designing a potential intervention.
Data collection
After obtaining verbal consent and before beginning the interview, participants were asked to complete a brief demographic survey to characterize the study sample; the survey included standard items such as age, education, employment, infant age, and feeding method (Supplemental Appendix 3). Later, the principal investigator (M.S.H., a male, PhD-trained behavioral specialist) and a research assistant (S.S., a female, graduate student in clinical psychology), both trained in qualitative interviewing, conducted individual semi-structured interviews that lasted between 30 and 60 min. Neither interviewer had any pre-existing relationship or role with any of the participants. Participants were given the option to choose the interview times and modality (in-person or virtual). The first four interviews were conducted in person, based on the participants’ preference. However, the remaining 10 interviews were conducted remotely (via video or phone) to comply with COVID-19 safety protocols. All participants received $50 (plus $7 for parking for in-person interviews) immediately following the interview.
The principal investigator and the research assistant debriefed after each interview to reflect on the content and assess whether new information was being uncovered. Recruitment was halted once we observed that participants consistently reported similar experiences, and no new data were emerging, indicating theme saturation. 49 All interviews were audio-recorded and transcribed verbatim by TranscribeMe for analysis.
Analysis
The codebook was inductively developed from the interviews using NVivo software (QSR International Pty Ltd., Burlington, MA, USA). 50 Two trained qualitative analysts independently co-coded 10 transcripts to establish intercoder reliability, which was assessed using Cohen’s kappa statistics. 51 The average Cohen kappa score was 0.67, indicating substantial agreement. Coding differences were discussed among the coders until full agreement on coding was reached. The primary coder then coded the remaining transcripts independently.
Once data collection was complete, the primary coder conducted a thematic analysis to systematically describe the participants’ experiences. 52 The data were organized into categories and themes that captured the critical aspects of participants’ descriptions related to sleep, diet, and physical activity. This process involved grouping similar codes to form broader categories while remaining closely aligned with the participants’ original language and the practical details of their experiences. The goal was to ensure that the final themes provided a comprehensive yet straightforward reflection of the participants’ experiences, suitable for informing the development of a holistic intervention.
Results
A total of ~93 individuals expressed interest in participating through the Pitt+Me research registry (N = 53) and the Pittsburgh Brown Mamas (N = 40). A team member attempted to contact all interested individuals; however, they were not able to reach or schedule many individuals due to limited availability. No individuals who were contacted declined participation, and there were no withdrawals. Thematic saturation was reached after ~10 interviews; however, we continued interviewing until 14 participants were enrolled to ensure a diverse range of perspectives. The final sample consisted of 14 postpartum individuals with a median age of 33 years [Interquartile range (IQR) 32–36]and a median age for their last child of 6 months (IQR 3–7). Five participants identified as Black or African American, three as White, one as Asian Indian, and five did not disclose their race. Eight participants lived with and shared a bed with a partner. Three participants shared a bed with their child. Half of the participants were currently breastfeeding (Table 1).
Sample characteristics.

Median (Q1–Q3); n (%).
We identified four themes describing participants’ current experiences with sleep, physical activity, and diet and recommendations for future interventions (Table 2).
Summary of key themes with illustrative subpoints and quotes.
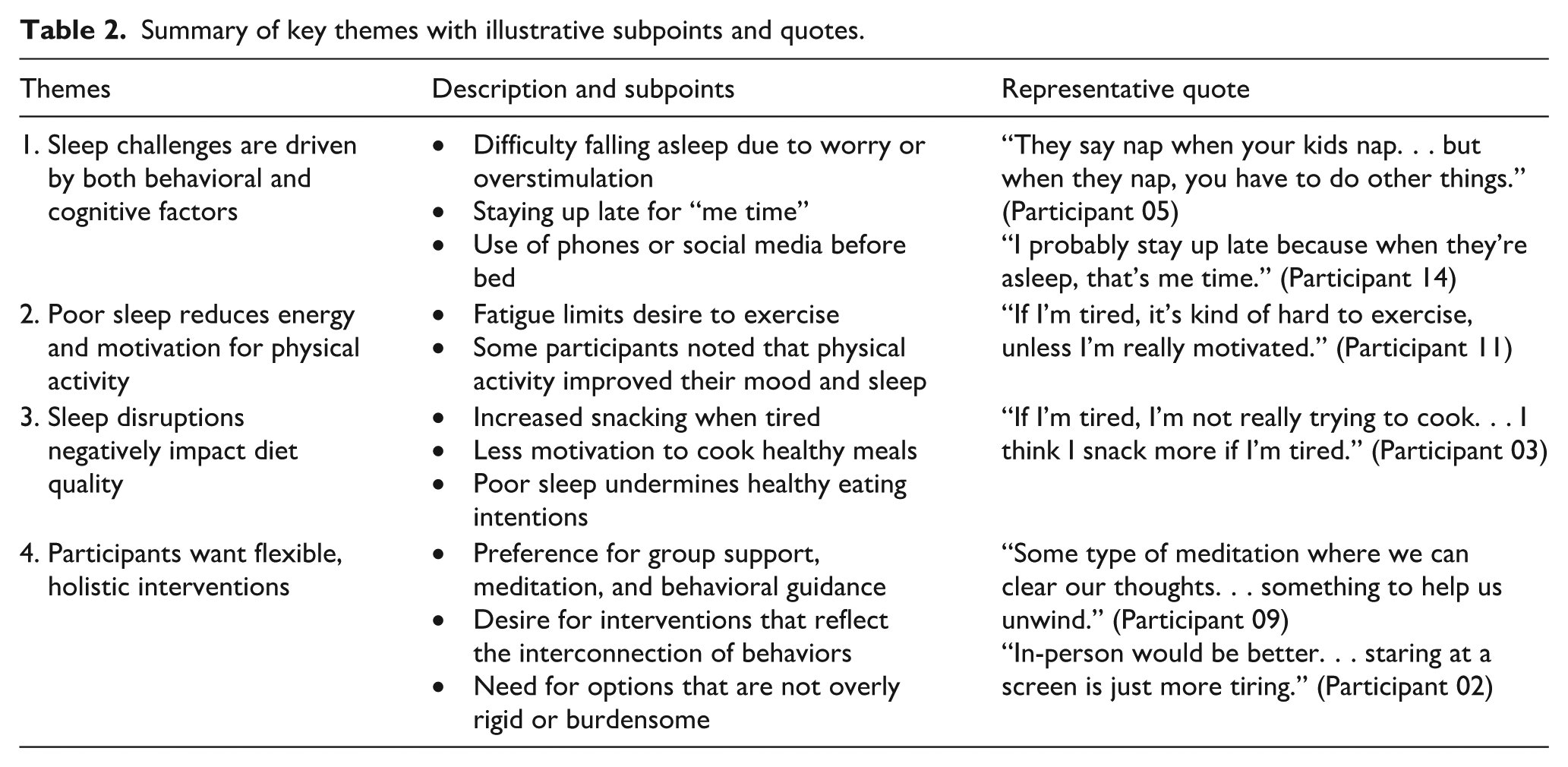
Theme 1: Sleep challenges are driven by both behavioral and cognitive factors
Participants described various cognitive and behavioral factors that they felt impacted their sleep. Many expressed difficulty “shutting off” their minds, with anxiety or worries about their infant keeping them awake. A participant (Study ID: 19) explained, “Everyone tells me, ‘Oh, sleep when the baby sleeps.’ That is a lie, that is a myth, and it is impossible. . .for a mom. [. . .] We’re constantly worried, is he okay? Is he sleeping okay? Is he breathing?” Likewise, another participant noted:
It’s inconsistent. Sometimes I have trouble falling asleep while the baby is asleep just with all the things on my mind just that mind racing and thinking about all the things that I have to do or that I didn’t get to think about during the day because I’m tending to everyone else so. But sometimes it’s my own mind that keeps me from sleeping. (Study ID: 21)
Participants also noted that several behavioral factors affected their sleep. For example, some participants noted that using electronic devices, such as phones or social media, made it difficult to fall asleep. A participant shared, “One thing I’ve tried to do is do less electronics before bed, kind of put a cap on when I stop looking at my phone” (Study ID: 33).
To cope with sleep disturbances and their daytime effects, participants described various strategies, including melatonin and essential oils, increased caffeine use, meditation, and exercise. One participant described their relaxation routine, “I do this mind game where you start at your toes and you tell your toes that you’re asleep and you kind of work your way up your body [. . .] it kind of just relaxes me to a point where I can kind of drift off” (Study ID 28). The same participant also described identified physical activity and diet as a behavior that affects sleep.
I find that having that exercise [. . .] having the ability to let go of everything that’s happening during the day through exercise just sweating it out really helps me throughout the rest of the day. [. . .] I also noticed that when I eat certain things, it affects how I sleep.
Theme 2: Poor sleep reduces energy and motivation for physical activity
Participants frequently mentioned that poor sleep impacted their energy levels and limited their ability to engage in physical activity. A participant shared, “Once I’m able to go to sleep, I’m exhausted. [. . .] And exercise is hard to fit in.” Another shared a similar experience: “If I don’t get good sleep, I feel more tired and sluggish. Exercise can be hard to fit in” (Study ID: 21).
However, some participants spoke about the mental health benefits they experienced when they did manage to exercise. For example, one participant (Study ID: 27) stated, “Actually, exercise has been a big one for me, not just for physical health but for mental clarity. I find that I can handle my day better and even sleep better if I’ve done something active.” Similarly, another participant (Study ID: 28) echoed this experience: “Honestly, exercise has been a big one. Just making sure that I am in the best place possible mentally, and one way I do that is through exercise.”
Participants also described their experience of a cyclical relationship between sleep and exercise, where poor sleep made exercising more challenging, but exercise sometimes improved their sleep and mood. For example, a participant (Study ID: 28) said, “I find that I can handle my day better and even sleep better if I’ve done something active.” Another mother of a 5-month-old (Study ID: 27) added, “Exercise can be hard to fit in, but when I do, it helps my mood and just makes it easier to manage everything.”
Theme 3: Sleep disruptions negatively impact diet quality
Participants described how fatigue resulting from poor sleep impacted their ability to prioritize healthy eating. Although many participants expressed a strong intention to maintain healthy diets, they frequently reached for convenient, low-effort foods when energy levels were low. One participant explained: “If I just feel like I’m trying to muddle through a day, I’ll grab whatever’s around instead of stopping to think about what I’m putting into my body. So I think sleep probably does have an impact on diet to a degree” (Study ID: 10).
Despite their intentions, many participants struggled to prepare meals that aligned with their health goals. As one participant shared: “I’m just so tired, and I don’t feel like I have enough time. . . I do a lot of shortcuts. . . I might eat TV dinners or chips just to keep me going.” (Study ID: 5) Another participant echoed this sentiment, highlighting the difficulty in preparing meals amidst fatigue: “I like to eat a lot of vegetables. . .but now it takes too much time. I do shortcuts, like granola bars or TV dinners” (Study ID: 18).
Several participants expressed frustration with not being able to maintain their pre-pregnancy or pregnancy healthy eating habits. One participant noted, “Before I got pregnant, I used to be more mindful about including vegetables, but now it’s just whatever is easiest to grab. It’s hard to make the choices I used to” (Study ID: 9).
Another participant shared a similar comment: “I’m trying to get back to how I was eating when I had gestational diabetes because it was just so much healthier for me. . . [but] it’s hard to keep that up now” (Study ID: 4).
While fatigue and time constraints led participants to prioritize convenience, many recognized the long-term benefits of healthy eating and expressed a desire to return to more nutritious eating patterns when possible. For example, one participant mentioned:
If I had the energy, I would go back to meal prepping like I did before. I just don’t have the mental space to do it right now. (Study ID: 36)
Theme 4: Participants want flexible, holistic interventions
Participants shared recommendations for their preferred intervention content and format. The content would cover sleep education, tailored nutrition guidance, structured physical activity, and peer support.
Some participants described sleep education as a valuable component. A 32-year-old mother of three expressed, “Education around sleep could be useful. [. . .] I have that insight to know some things that maybe I could do differently to help myself [. . .] but I know not everyone necessarily knows all that information about sleep” (Study ID: 04). Similarly, another participant stated, “I didn’t know enough about sleep before I had my baby. It would have been so helpful to have someone explain it to me before. I think sleep education could really make a difference” (Study ID: 36).
Participants also identified nutrition guidance tailored to postpartum needs as necessary, especially for breastfeeding mothers. A 37-year-old mother of an 11-month-old suggested, “I think it might be good for them to have [information] on hand to share [. . .] so that parents have the support for making healthy food choices from the start” (Study ID: 5). Someone else said, “Getting information on how to make healthier choices postpartum would have been so helpful. It’s hard to know what you should be eating when you’re breastfeeding and sleep-deprived” (Study ID: 4).
Several participants recommended structured programs for physical activity. Structured programs would provide informational support, accountability, and help building a healthy routine. A 40-year-old mother of two noted, “More regular walks would be great [. . .] just something to keep myself from hurting and feeling stiff” (Study ID: 4). Another participant shared their thoughts, stating, “Having some kind of structured physical activity program would be so helpful. . . I think I’d feel better just walking or doing some stretching every day, even if it’s brief” (Study ID: 37).
Peer support was highly valued by participants, who expressed a desire for opportunities to connect with others who shared similar experiences. One participant explained,
Me, personally, I love being around people, so the group is– I would prefer that group one. Because that way you bond with other people, you meet other people, you share experiences, you learn, you encourage, you– it’s smooth. (Study ID: 18)
This sentiment highlights the importance of peer connections in providing emotional reassurance and fostering a sense of community during the postpartum period.
Participants preferred flexible intervention formats that would accommodate the demands of postpartum life. Many felt that online resources would allow them to participate on their own schedules. A 40-year-old mother of three shared, “I would probably be more likely to use something web-based, online because it’s more accessible. [. . .] I don’t know if I can take the hour out of my day to drive there and have that meeting and come back” (Study ID: 9).
In addition to online options, some participants saw pediatric visits as a potential moment to deliver postpartum support, as they involved regular, trusted interactions with healthcare providers. One mother noted, “I think the pediatrician, that is a place where– them having information to help us [. . .] That, I think, is a good time for that” (Study ID: 5).
Discussion
Through semi-structured interviews, we probed factors that impact the sleep patterns, diet, and physical activity after childbirth, perspectives on how these behaviors influence each other, as well as ideas on interventions that might address the three behaviors together. First, participants identified a range of modifiable cognitive and behavioral factors affecting sleep, such as worry, caffeine intake, nocturnal social media use, exercise, and over-the-counter sleep aids. Second, while participants acknowledged the importance of exercise for their mental health, they also reported significant barriers, including sleep-related fatigue, childcare responsibilities, and time constraints. Third, participants highlighted the challenges in maintaining a healthy diet due to time limitations and lack of energy from disrupted sleep. Fourth, participants underscored the interconnected nature of these behaviors, describing how changes in one behavior (e.g., sleep) influenced others (e.g., diet and activity). Lastly, participants offered recommendations for supportive postpartum interventions, emphasizing the need for flexible interventions that address the three behaviors together. These findings have important implications for designing perinatal weight management interventions to more align with the preferences of postpartum individuals.
This study’s findings on factors affecting postpartum sleep, diet, and physical activity not only are consistent with prior research but also offer unique contributions.53 –65 Specifically, while previous studies have identified postpartum barriers and facilitators to individual behaviors—such as sleep disruptions, dietary challenges, and physical activity barriers—our study is among a few studies to explicitly explore how these behaviors interact in the lived experiences of postpartum individuals. For example, Badon et al. identified similar barriers to postpartum exercise, including fatigue, mood, and childcare responsibility in a sample of individuals with perinatal depression. 66 Our findings highlight a reciprocal relationship between sleep and exercise—individuals struggle to engage in physical activity due to fatigue, yet those who are active report improved sleep quality and mood. This paradox suggests a need for tailored approaches that acknowledge postpartum exhaustion while promoting movement in practical, low-effort ways. Structured exercise may feel overwhelming in the early postpartum period, especially for sleep-deprived individuals balancing infant care and recovery. Future interventions could focus first on reducing sedentary behavior before introducing formal exercise recommendations. Public health guidelines suggest breaking up prolonged sitting with light movement, such as standing while feeding, taking short walks during childcare routines, or engaging in gentle stretching while playing with an infant. 67 These strategies may feel more feasible than dedicated workout sessions, allowing postpartum individuals to gradually incorporate physical activity without exacerbating exhaustion.
Interventions may need to consider psychological beliefs about rest versus movement to cope with fatigue. Our findings suggest that postpartum individuals may perceive rest as more beneficial than physical activity when fatigued, which aligns with prior research showing that postpartum fatigue is a key barrier to exercise participation.53,66 Interventions should address these perceptions by framing movement as a means of improving energy levels rather than depleting them. Additionally, integrating participant-driven strategies—such as incorporating movement into existing caregiving tasks—may improve adherence and sustainability.
Prior research has also identified the challenges to consuming a healthy diet due to time constraints and the dual responsibilities of caring for an infant and managing personal health often. 68 However, our study more explicitly highlights how sleep deprivation exacerbates fatigue and alters food choices, leading to a preference for quick, high-energy foods. Our findings suggest that postpartum dietary interventions incorporate strategies to counteract the effects of sleep deprivation on food choices and decision-making. Given that poor sleep exacerbates cravings for high-energy, processed foods, 69 interventions that include examples of nutrient-dense and quick-to-prepare meal options may promote both energy stability and sleep quality.
Another important implication of our study is that it highlights the behavioral strategies that postpartum individuals actively use to navigate these challenges—an aspect frequently overlooked in existing research. For example, participants noted that meditation or breathing exercises before bedtime served as a strategy to calm racing thoughts and aid sleep. This finding aligns with evidence from non-postpartum populations. A growing body of literature demonstrates that mindfulness-based practices, including body scans, breathing exercises, and guided meditation, can improve sleep quality, particularly by reducing pre-sleep cognitive arousal.70,71 For instance, a meta-analysis by Rusch et al. found that mindfulness meditation significantly improved sleep quality in adults with moderate effect sizes. 72 Others indicated that limiting caffeine intake in the afternoon helped reduce sleep disruptions and enhance overall restfulness. Additionally, several women deliberately restricted evening social media use to avoid overstimulation and anxiety, describing this as a significant change that allowed them to transition to sleep more effectively. These strategies reflect established components of cognitive and behavioral approaches to insomnia, including stimulus control and mindfulness techniques. 73 Our findings also emphasize the bidirectional nature of these behaviors, with participants illustrating how changes in diet and physical activity directly impacted sleep quality. To our knowledge, few studies have documented the use of mindfulness-based sleep strategies in postpartum individuals, suggesting that our study contributes new insight into how this population naturally adopts such techniques. Women who practiced mindful relaxation techniques before bedtime reported experiencing more restful sleep.
Research, clinical, and policy implications
Prior lifestyle interventions targeting postpartum weight retention have produced modest weight loss, typically around 1.7–2.5 kg, with large variability (ranging from −13 to +0.75 kg) and limited evidence on which components are most effective.32,74,75 While interventions that incorporate self-monitoring, goal setting, and behavior change theory tend to be more effective, implementation of these components has varied widely, limiting generalizability, and impact. 32 Most prior studies did not include sleep as a targeted behavior, despite its strong link to dietary choices, physical activity, and weight regulation and the growing evidence that sleep may enhance weight loss outcomes. For example, Thomson et al. found that among adults participating in a weight loss intervention, those who reported more consistent sleep and fewer sleep disturbances were significantly more likely to achieve clinically meaningful weight loss. 40 Similarly, Elder et al. showed that participants who slept at least 7 h/night during a behavioral weight loss trial lost more weight than those with shorter sleep duration, independent of intervention adherence. 39
The current study helps fill an important knowledge gap by providing qualitative insight into how postpartum individuals experience these three behaviors as interrelated and mutually reinforcing. Participants also provided direct suggestions on how perinatal weight management interventions could address sleep, diet, and physical activity together. Given the circadian regulation of sleep, diet, and physical activity, interventions should be designed to account for the biological interconnectedness of these behaviors and their collective influence on metabolic health.76,77 Sleep, meal timing, and exercise are all entrained by the body’s master clock in the suprachiasmatic nucleus, and disruptions in one domain can dysregulate others.76 –78 By educating participants on circadian alignment strategies, such as maintaining consistent sleep–wake times, eating meals within an optimal window for metabolic efficiency, and engaging in physical activity during biologically appropriate times of the day. Emerging evidence suggests that such strategies may influence metabolic outcomes, 79 but their effectiveness in postpartum populations remains to be tested.
Building on this foundation, the intervention content within each behavioral domain should provide targeted strategies to optimize health outcomes. Sleep education content could focus on environmental and behavioral strategies to improve sleep quality. This might include guidance on managing sleep-related anxiety or worry and appropriate wind-down routines before bed (e.g., limiting screen time). The diet-related content could provide consultations with health coaches who understand the unique dietary needs of postpartum women. The physical activity content should provide accessible, low-impact exercise options tailored for postpartum individuals. Structuring these elements within a flexible, online format could enhance accessibility and engagement, allowing participants to incorporate these strategies into their daily lives.
In addition, the increasing availability and use of wearable devices and fitness trackers presents an opportunity to support behavior change in a scalable and low-burden way.80,81 These tools can facilitate self-monitoring of sleep and physical activity, reinforce engagement through real-time feedback, and provide valuable data to inform personalized coaching. Incorporating wearable technology into postpartum interventions could help bridge the gap between daily routines and health goals, particularly for individuals balancing caregiving demands.
Furthermore, creating peer support groups as part of the intervention could foster a sense of community and shared experience among postpartum individuals. These groups could provide emotional support, practical advice, and motivation to maintain healthy behaviors. Engaging healthcare providers, particularly pediatricians who frequently interact with new mothers, could also enhance the intervention’s reach and effectiveness.
Healthcare providers can provide crucial support to postpartum individuals by incorporating brief, structured discussions about maternal sleep, diet, and physical activity during child wellness visits. A model for integrating maternal health into pediatric care already exists in the treatment of postpartum mood and anxiety disorders, where pediatricians are uniquely positioned to screen, educate, and connect mothers to appropriate mental health resources within primary care settings. 82 For example, pediatricians could screen for sleep disruptions, assess fatigue-related dietary habits, and provide guidance on integrating low-barrier physical activity into daily routines. Additionally, they could offer referrals to postpartum support services and deliver brief behavioral counseling to encourage sustainable health behaviors. By embedding these discussions into routine pediatric care, healthcare providers can help bridge the gap between postpartum health interventions and real-world accessibility, ensuring that sleep, diet, and physical activity remain prioritized within the broader maternal and child healthcare system.
Limitations
Considering these findings, several limitations should be noted. First, while we identified cross-cutting themes, we did not have an adequate sample size to identify subgroup differences (e.g., race, ethnicity, socioeconomic status, parity, relationship status). Likewise, we did not assess for or diagnose postpartum mental health disorders as part of this study, and mental health status was not used as an inclusion or exclusion criterion. As such, we do not include participants’ formal diagnoses or psychiatric histories, which could reveal unique barriers, facilitators, or preferences for intervention content and format. However, some participants did voluntarily mention mental health challenges (e.g., anxiety or stress) in the context of their experiences, and these insights are reflected in the themes where relevant. Second, our study primarily focused on individual and interpersonal-level factors without explicitly assessing environmental or societal influences, such as economic stability, workplace policies, or access to nutrition assistance programs (e.g., Special Supplemental Nutrition Program for Women, Infants, and Children). Future research should use multilevel frameworks to understand these broader determinants better. Finally, while we interviewed participants across a postpartum range (2–12 months), future research should examine time-varying influences by conducting multiple interviews across the perinatal period. Given that factors influencing sleep, diet, and physical activity most likely change throughout the postpartum period, such as changes in work schedules, childcare responsibilities, and breastfeeding status, repeated interviews at key transition points (e.g., early postpartum, return-to-work period, etc.) could help tailor the intervention content and/or delivery.
Conclusion
In conclusion, this study highlights the need for holistic interventions to support sleep, diet, and physical activity needs of mothers. By identifying key internal and external factors affecting these behaviors and gathering detailed participant recommendations, we can develop comprehensive programs tailored to the unique needs of postpartum women. Such interventions should provide strategies to improve sleep, provide nutritional guidance, and offer accessible physical activity options while fostering community support and involving healthcare providers. Implementing these strategies can significantly enhance the overall health and well-being of postpartum women, ultimately reducing the risk of long-term adverse health outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251384412 – Supplemental material for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention
Supplemental material, sj-docx-1-whe-10.1177_17455057251384412 for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention by Marquis S. Hawkins, Michele D. Levine, Maya I. Ragavan, Daniel J. Buysse, Esa M. Davis, Megan E. Hamm, Kathleen M. McTigue, Swathi Srinivasan, Rachel Wasilko and Judy C. Chang in Women’s Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057251384412 – Supplemental material for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention
Supplemental material, sj-pdf-2-whe-10.1177_17455057251384412 for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention by Marquis S. Hawkins, Michele D. Levine, Maya I. Ragavan, Daniel J. Buysse, Esa M. Davis, Megan E. Hamm, Kathleen M. McTigue, Swathi Srinivasan, Rachel Wasilko and Judy C. Chang in Women’s Health
Supplemental Material
sj-pdf-3-whe-10.1177_17455057251384412 – Supplemental material for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention
Supplemental material, sj-pdf-3-whe-10.1177_17455057251384412 for Postpartum dietary, sleep, and physical activity behaviors: A qualitative study to inform efforts to address postpartum weight retention by Marquis S. Hawkins, Michele D. Levine, Maya I. Ragavan, Daniel J. Buysse, Esa M. Davis, Megan E. Hamm, Kathleen M. McTigue, Swathi Srinivasan, Rachel Wasilko and Judy C. Chang in Women’s Health
Footnotes
Ethical considerations
The University of Pittsburgh Institutional Review Board approved the protocol for this study on January 1, 2020 (protocol #19110195).
Consent to participate
All participants will be required to provide consent (including verbal) prior to enrollment and baseline assessments.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Heart, Lung, and Blood Institute (1K01 HL161439-01) and the University of Pittsburgh’s Clinical and Translational Science Scholars Program (KL2 TR001856-03).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Over the past 3 years, Dr. Daniel Buysse has been a paid or unpaid consultant to Sleep Number, Idorsia, and Eisai. All consulting agreements have been for <$5000/year from any single entity. Dr. Daniel Buysse is an author of the Pittsburgh Sleep Quality Index, Pittsburgh Sleep Quality Index Addendum for PTSD (PSQI-A), Brief Pittsburgh Sleep Quality Index (B-PSQI), Daytime Insomnia Symptoms Scale, Pittsburgh Sleep Diary, Insomnia Symptom Questionnaire, and RU_SATED (copyrights held by the University of Pittsburgh). These instruments have been licensed to commercial entities for fees. He is also co-author of the Consensus Sleep Diary (copyright held by Ryerson University), which is licensed to commercial entities for a fee. He has received grant support from NIH, PCORI, AHRQ, and the VA. Dr. Esa Davis is a member of the United States Preventive Services Task Force (USPSTF). Dr. Judy Chang is a member of the National Academies of Science, Engineering, and Medicine (NASEM) standing committee on Reproductive Health, Equity, and Society. This article does not necessarily represent the views and policies of the USPSTF or NASEM.
Data availability statement
De-identified interviews can be made available with a data use agreement.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.