
Abstract
Background:
There is a lack of data regarding the current state of lactation accommodations at continuing medical education (CME) events to guide best practice recommendations.
Objective:
To evaluate CME attendee attitudes, experiences, and preferences as it pertains to lactation support accommodations at CME events.
Design:
A cross-sectional study utilizing an electronic-based survey.
Methods:
Surveys were administered electronically to attendees of seven CME courses from August 2022 to October 2023, and de-identified data were collected to a secure database. Attitudes regarding lactation accommodations, personal preferences for lactation accommodations, and experiences with lactation at CME events were analyzed.
Results:
Of the 337 survey respondents, 169 had personal experience with lactation and 47 had experience with lactation at a CME course within the past 10 years. The majority of respondents agreed that lactation accommodations should be a priority (n = 264, 83%) and are a medical need (n = 285, 89%). Of those with recent experience lactating at a CME course, only 19% (n = 9) indicated adequate lactation accommodations were provided. Due to inadequate accommodations, 77% (n = 36) of respondents experienced decreased participation in the CME course content, 70% (n = 33) claimed fewer hours of CME credit, and 74% (n = 35) experienced decreased satisfaction in the CME course. Preferences for lactation accommodations included proximity to the meeting, audio–visual streaming of content, privacy, security, and signage supporting lactation in addition to an adequate designated space with access to an electrical plug and water supply.
Conclusions:
The current state of lactation accommodations at CME courses is inadequate and contributes to inequitable experiences for lactating participants. Course participants are supportive of lactating healthcare professionals at CME courses and recognize lactation accommodations as a priority. Further work is needed to inform and institute changes to lactation accommodations for healthcare professionals.
Keywords
Introduction
Over the past several decades, there have been increasing numbers of women graduating from medical schools and other professional schools, with women representing over 50% of medical school matriculants.1,2 Despite the evolving landscape of the medical field and the desire for greater gender workforce diversity, access to lactation accommodations continues to be significantly lacking.3 –8 Lactation has many proven health benefits and is recommended by several national and international organizations.9 –11 Despite recommendations strongly encouraging lactation and the associated legal requirements for lactation support, 12 there remain both structural and cultural barriers for lactating physicians.4 –8,13,14 This lack of support for lactating physicians is associated with premature termination of lactation and various negative health, social, and emotional ramifications.3 –5,7
Continuing medical education (CME) courses are attended by physicians and other healthcare professionals (HCPs) to remain up to date on medical knowledge, skills, and professional performance.15,16 Systematic reviews have demonstrated that CME courses are effective in disseminating knowledge and can improve performance across a range of skill sets. 16 In addition to demonstrating significant efficacy in enhancing medical knowledge, skills, and clinical outcomes,15,16 CME events provide additional benefits such as networking and exposure to further career opportunities. 17
Prior best practice recommendations for lactation accommodations at CME events highlighted the current challenges, gaps, and barriers for lactating individuals who attend CME events for professional purposes. 18 The outlined recommendations were based on expert opinion of the authors. 18 There remains a considerable lack of data regarding the current state of lactation accommodations and the needs and preferences of lactating individuals at CME events.
We aimed to evaluate CME attendee attitudes, experiences, and preferences as it pertains to lactation support accommodations at CME events. By doing so, the study data will help provide an evidence base to guide future lactation accommodation recommendations during CME courses.
Methods
The present study was designed as a mixed method cross-sectional electronic-based survey study, intended to directly assess CME course attendee attitudes, experiences, and preferences regarding lactation accommodations at CME events. The survey was voluntary, anonymous, and sent electronically using REDCap19,20 after completion of CME courses. The study survey was entirely separate from official course evaluations. In accordance with the Declaration of Helsinki, the study was reviewed by expedited review procedures and was approved by Mayo Clinic Institutional Review Board (ID: 22-006975). The application involved quality improvement and quality assurance and was determined that the application did not constitute as research as defined under 45 CFR 46.10. Protocol-approved passive consent was obtained from all study participants prior to study initiation. Passive consent occurred in that the consent to participate was embedded in the email sent to all course attendees. Participation in completing the survey and data collection was completely voluntary and separate from course evaluations. Guidelines for reporting this study followed the Consensus-Based Checklist for Reporting of Survey Studies and are outlined in the Supplemental Material. 21
Instrument
The voluntary, de-identified, electronic survey consisted of demographic (age, sex, professional role, etc.) information, questions concerning attitudes on lactation accommodations, preferences, and lactation accommodation experiences at CME events. Approval from the CME course directors was the determining factors for CME course inclusion. Through the study timeline, conferences with varying geographic location, subspecialty conferences, and time throughout the year were asked to participate to attempt to increase generalizability.
Due to the absence of a validated instrument that adequately addressed our study objectives, a novel survey was developed to assess barriers to lactation and perceptions of lactation support. The development process followed a structured, iterative methodology grounded in existing literature and expert consensus. A comprehensive review of peer-reviewed literature was conducted to identify commonly reported barriers to lactation, recommendations for lactation support, and relevant demographic variables. Survey items were drafted to reflect key domains identified in the literature, including structural, interpersonal, and individual-level barriers, as well as facilitators of lactation support. Gender neutral language related to lactating persons was intentionally used to improve generalizability.
The initial pool of items was reviewed and refined through a collaborative, consensus-driven process involving the study’s multidisciplinary author team, which included clinicians, researchers, and education coordinators. Through iterative discussions, each item was evaluated for clarity, relevance, and comprehensiveness. Items were revised, added, or removed based on group feedback to ensure alignment with the study’s aims and to enhance content validity. Survey items were formatted using a combination of Likert-type scales, multiple-choice questions, and a single open-ended response. This approach was intended to balance quantitative rigor with opportunities for qualitative insight.
All survey respondents answered demographic information, questions about attitudes regarding lactation accommodations, and information about personal lactation experience. The survey utilized branching logic to gain relevant information from individuals, when applicable. Survey respondents who indicated personal experience with lactation answered additional questions regarding anticipated lactation needs and accommodation preferences during CME events. Survey respondents who indicated experience lactating at a CME event within the prior 10 years answered a subset of questions regarding the current state of lactation accommodations at CME events, based on their recent experiences. Questions were focused on prior experiences at any CME event, and not specifically the course in which the survey list was obtained from. The majority of survey questions were posed on a Likert-based scale, with answers ranging from strongly disagree to strongly agree, not important to extremely important, and never to very often. Participants with personal lactation experience were asked a single open-ended question regarding the most important factor to improve lactation support at CME events.
Data collection
Data were collected using an electronic REDCap survey.19,20 The survey was not linked to any identifiable registration information for CME participants. Electronic surveys were sent as a secure web link to the email address provided during conference registration for conferences occurring between August 2022 and October 2023. Reminder emails for survey completion were sent to study participants in accordance with institutional guidelines. All participants of CME courses were eligible to participate regardless of profession, self-identified gender, or prior lactation experience. Participants were excluded if the survey was not completed.
CME participants were provided with the electronic survey within 2 days following the end of the CME course, with 2 weeks to complete the voluntary survey. A total of one original email and two reminder email notices were sent over a period of 6 weeks before all contact was terminated. After 8 weeks from course completion, the de-identified survey was closed, and no other responses were allowed. After all courses were completed and the final survey was closed, the data collection phase of the study was completed, and data were incorporated into a secure database for subsequent statistical analysis.
Statistical analysis
Data were analyzed using SAS statistical software, Version 9.4 (SAS Institute Inc., Cary, NC, USA). Respondent characteristics are summarized for each of the three cohorts of interest (all respondents, respondents with personal lactation experience, and respondents with experience lactating at a CME course) using frequency counts and percentages. Analyses assessing the association of age and sex with CME lactation attitudes was performed using data from all respondents who indicated their sex was either female or male. Respondents were grouped according to age (⩽50 years versus ⩾51 years) and self-reported sex (female versus male). Attitude responses were dichotomized and the number (%) of respondents who reported favorable attitudes was summarized for each of seven attitude questions. For each question, a multivariable logistic regression analysis was performed with age and sex as explanatory variables. Initial analyses were performed with the age-by-sex interaction term included in the model to assess whether the effect of age was dependent on sex. If the interaction term was not significant, the logistic regression model was fit with only main effect terms for age and sex. For these analyses, p-values <0.05 were considered statistically significant and results are summarized by presenting the odds ratio and 95% confidence interval for age (⩽50 years versus ⩾51 years) and sex (female versus male) with odds ratios greater than 1 indicating higher odds of a favorable attitude for the given lactation question.
Qualitative responses from a single, open-ended question were collected in Microsoft Excel for thematic analysis. Open coding was performed on free text responses from 66 respondents independently, in duplicate by two authors. These initial codes were inductively analyzed and separated into themes. Through inductive, iterative exploration and discussion, consensus was reached regarding the most important themes.
Results
The survey was delivered to attendees of seven CME courses occurring between August 2022 and October 2023. Course locations included Minnesota (2), West Virginia, Florida (2), Illinois, and California. Course attendees came from 49 states and the District of Columbia; individual respondent practice location was not collected. A total of 2,019 attendees were sent surveys at the end of their CME course; at the end of data collection, 337 participants (16.7%) had completed the survey. Among the 337 participants, 169 indicated they had personal experience with lactation and 47 indicated experience lactating at a CME course in the last 10 years. Of all respondents, 74% identified as female and 25% as male. Responses to the demographic information are outlined in Table 1.
Baseline survey respondent characteristics.

CME: continuing medical education.
CME participant attitudes toward lactation accommodations
The majority (n = 264, 83%) of respondents agreed or strongly agreed that it should be a priority to provide lactation accommodations and support, and 66% (n = 210) personally knew someone who would benefit from improved lactation support. The majority (n = 239, 75%) agreed or strongly agreed they would be comfortable with individuals expressing or pumping in shared educational or event spaces. The majority (n = 218, 69%) disagreed or strongly disagreed that lactation is shared spaces would distract from their educational experience, while an additional 17% (n = 54) were neutral regarding this issue. Overall, 89% (n = 285) of respondents were supportive of lactation accommodations as a medical need.
When analyzed by sex (male or female) and age (<50 years or >51 years), there were several notable differences (Table 2). Compared to those 51 years of age or older, those 50 years of age or under were more likely to agree that it should be a priority to provide lactation accommodations (OR = 1.86, 95% CI: 1.02, 3.39; p = 0.044), that they know people who would benefit from improved lactation support (OR = 2.94, 95% CI: 1.79, 4.84; p < 0.001), and they support women breastfeeding in public (OR = 3.08, 95% CI: 1.57, 6.03; p = 0.001; Table 2). Those 50 years of age and under were also more likely to disagree to statements indicating that lactation should only be done in private (OR = 1.83, 95% CI: 1.10, 3.02; p = 0.019), and lactation in shared spaces would distract from educational experiences (OR = 2.05 95% CI: 1.25, 3.68; p = 0.004). Compared to males, females were more likely to know people who would benefit from improved lactation support (OR = 2.26, 95% CI: 1.31, 3.90; p = 0.003), and support lactation accommodations as a medical need (OR = 2.31, 95% CI: 1.11, 4.82; p = 0.025).
Association of age and sex with attitudes.

OR: odds ratio; CI: confidence interval.
Analyses were performed using multivariable logistic regression. For these analyses, the explanatory variables are age and sex. Initial analyses included the age-by-sex interaction effect to assess whether the effect of age was dependent on sex. If the interaction term was not significant, a logistic regression was performed using only main effect terms, with the results summarized by presenting the OR and 95% confidence interval for age (⩽50 years compared to ⩾51 years) and sex (female compared to male).
Not all respondents answered each question. Across all questions, the minimum sample size was 40, 38, 150, and 81 for males ⩽50 years, males ⩾51 years, females ⩽50 years, and females ⩾51 years, respectively.
The age-by-sex interaction was statistically significant indicating that the effect of age differs between males and females. Among females, those 50 years of age or under were more likely to agree with this statement compared to those 51 years of age or older (OR = 3.20, 95% CI: 1.73, 5.93; p < 0.001). Among males, there was no significant difference between age groups (p = 0.469).
For these analyses, respondents were grouped according to age (⩽50 years versus ⩾51 years) and sex (female versus male). For questions 1, 2, 3, 4, and 7, the number (%) of respondents who agreed or strongly agreed is summarized for each group. For questions 5 and 6, the number (%) of respondents who disagreed or strongly disagreed is summarized.
For the statement “If a course attendee chose, I would be comfortable with them pumping/expressing milk in the shared educational event spaces,” a significant age-by-sex interaction was detected (p = 0.012), indicating that the effect of age was dependent on sex. Among females, those 50 years of age or under were more likely to agree with this statement compared to those 51 years of age or older (OR = 3.20, 95% CI: 1.73, 5.93; p < 0.001); and among males, there was no significant difference between age groups (p = 0.469).
Current state of lactation accommodations at CME events
Survey data from respondents with lactation experience at a CME course in the prior 10 years was collected. Of the 47 respondents, only 19% (n = 9) indicated that adequate lactation support accommodations were provided. The remaining 81% (n = 38) reported, overall, adequate lactation support was not provided in their experience. The current state of specific accommodations is outlined in Table 3.
Lactation accommodations at CME events.

Answered by respondents with experience lactating at a CME course in the prior 10 years. CME: continuing medical education.
The majority (62%) reported that they have expressed in public or shared spaces due to inadequate private accommodations. Additionally, 81% had pumped or expressed milk in a makeshift area, such as a bathroom, closet, or storeroom because of inadequate lactation accommodations at CME events.
As a result of inadequate lactation accommodations, many respondents highlighted direct negative impact on their educational experience. The majority (n = 36, 77%) reported experiencing decreased CME engagement and participation in valuable course content due to lack of adequate lactation support. The lack of adequate lactation support space led 70% (n = 33) of individuals to claim fewer hours of CME credit. Additionally, 74% (n = 35) reported experiencing decreased satisfaction in a CME course due to lack of adequate lactation accommodations.
Of the respondents with experience lactating at a recent CME event, 55% indicated that the lack of adequate lactation accommodation at a CME course created personal negative feelings such as anxiety, fear, resentment, and alienation.
Preferences of respondents with personal lactation experience
Of the 169 survey respondents with personal lactation experience, 152 (90%) participated in further questions regarding accommodation needs and preferences. Important priorities included access to an electrical plug and water, private and locked room, proximity to the meeting space, audio and video streaming of the course content, and signage supporting lactation in public spaces (Table 4).
Preferences for CME lactation accommodations.

Answered by respondents with personal lactation experience. CME: continuing medical education.
Respondents noted they would expect to express milk two (n = 79, 59%) or three (n = 42, 31%) times during an 8-h conference. Only 24% (35/148) of respondents in this sample had utilized wireless wearable breast pumps to express milk. Of the individuals who had utilized wearable pumps, 43% would feel comfortable pumping or expressing in common areas if supportive signage was posted. The remaining 57% of respondents were unsure or would not prefer to express in common areas.
When asked to rank their preferences for various lactation accommodation settings, the most preferred option was a private space with audio–visual (AV) streaming of course content. The next preferred option was a private space without AV capabilities followed closely by a dedicated, shared lactation space with AV streamed content.
Notably, 21% (33/157) of respondents reported that insufficient lactation accommodations led to not registering for a CME conference, and 53% (82/154) would be more likely to register for a CME course if lactation accommodations were known at time of registration.
Qualitative results
Respondents with personal lactation experience were asked to provide the single most important factor to improve the lactation experience at CME events. Thematic analysis of 66 responses was performed and 6 important themes were identified (Table 5). The most impactful factor was the need for a designated space that had been considered and designed specifically for the purpose of lactation with learner safety, comfort, and learning in mind.
Themes for improving lactation experience at CME events.
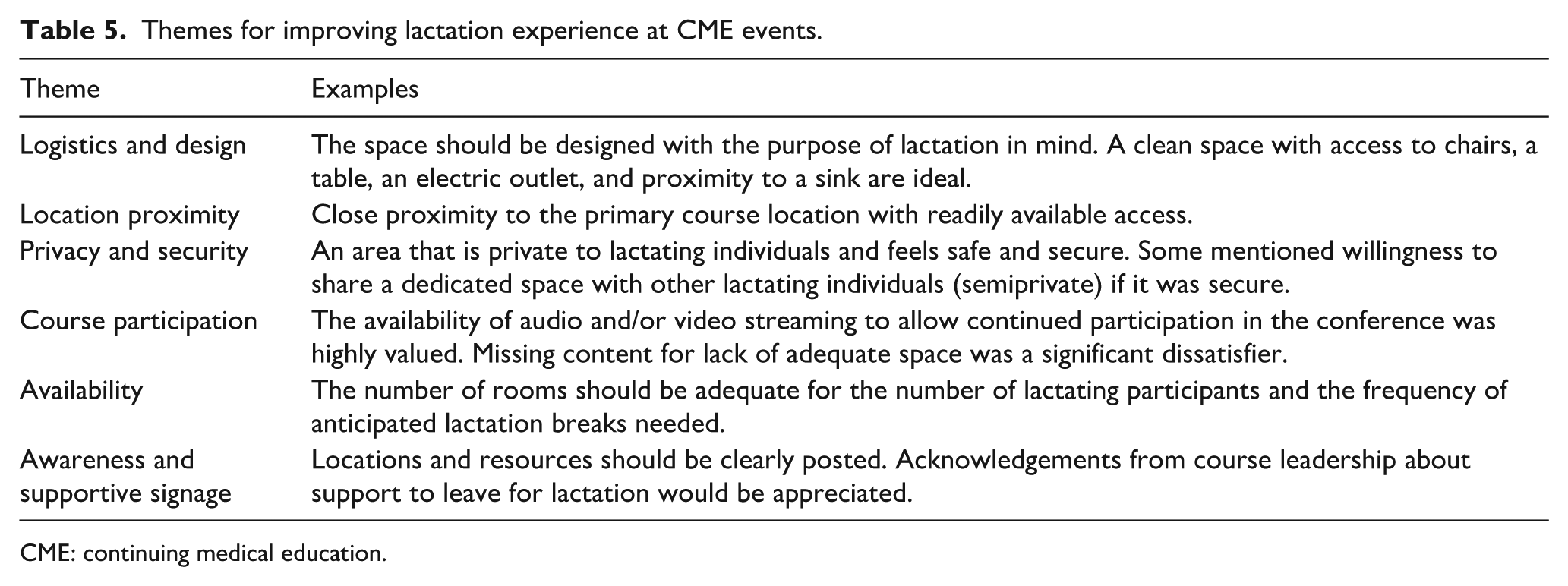
CME: continuing medical education.
Discussion
This study was designed to assess the attitudes of CME attendees regarding lactation accommodations, to clarify the current state of accommodations, and to capture data regarding lactation needs and preferences at CME events. This study demonstrated an ongoing, general lack of systemic design and structure to support lactating attendees at CME events over the past decade. The identified gaps in adequate lactation accommodations included insufficient space, space design, proximity to the space, and inability to participate in course content. These gaps have led to lower satisfaction and participation in CME events. This lack of support led to claiming fewer credit hours for lactating HCPs and continues to contribute to inequities in medical education. The data demonstrate the significant lack of support and the need for immediate action to be taken.
It should be noted that while these results were focused on CME courses, the findings are consistent with literature regarding lactation support for HCPs in general. Despite the benefits of lactation being well documented and supported by medical societies, there remains significant barriers to HCP lactation in the workplace.3 –8,13,14 In a survey regarding hospital support of lactation, 97% of female faculty physicians, fellows, and residents identified at least one occupation-related barrier to lactation. 13 In previous studies of physician lactation, common barriers included lack of appropriate space, difficulty with scheduling, work–life balance, and lack of colleague support.5,8,13 Additionally, many individuals reported stopping lactation early due to these barriers.4,5,7
Notably, the vast majority of CME attendees, regardless of their gender or prior lactation experience, felt lactation accommodations should be a priority. There was strong support from all participants for public breastfeeding and for lactation as a medical need. However, when analyzed per age group, there was a statistically higher amount of support for public lactation and prioritizing lactation support in those ages 50 and under. This generational shift toward supporting public lactation has been demonstrated in other studies regarding breastfeeding 22 and is representative of the changing norms of attitudes regarding lactation. This study demonstrates there is an overall positive view of public lactation, designating lactation as a medical need, and providing better lactation support. These results should be interpreted with caution due to potential bias from self-selection in those who responded to the survey.
In recent years wireless, wearable pumps have become more common and have been identified as a way to optimize lactation goals for physicians. 23 However, our study revealed that the majority of respondents who had utilized wearable pumps still prefer private lactation spaces be provided. While wearable pumps may be an option for HCPs going forward, this should not replace adequate lactation accommodations.
Our study demonstrates that despite the strong support from CME attendees surveyed for ensuring appropriate lactation accommodations, there remains a lack of systematic implementation to support lactating attendees. Of note, 21% of participants reported that lack of lactation accommodations previously led to not registering for a CME course; future areas of study include the impact of training and education and the need for further representation among medical professional societies. Lack of appropriate accommodations at events is a significant barrier to the equitable accessibility of education at CME courses. Providing appropriate lactation support and accommodations has lasting implications for both the professional and personal development of lactating HCPs.
Our quantitative and qualitative data outline specific areas that lactating attendees at CME conferences wish to be implemented and can provide guidance for future conferences. Establishing private and designated spaces for lactation was the most pressing need identified. An adequate number of rooms to lactate with attention to learner needs was another important factor. Conference course directors or other organizers of CME events should also take note that for a proper lactation space, having the designated space near the educational events, having proper facilities (i.e., sanitization available), and having AV streaming should be incorporated. Recommendations for consideration include working with event space staff to intentionally add appropriate lactation accommodations. Additionally, adding a question regarding need for lactation accommodations on registration forms prior to the event may assist in needs assessment and course planning. Future incorporation and further guidance regarding logistic recommendations for course directors should be explored in future research.
Limitations
Limitations to our study are similar to other survey-based studies, particularly with survey response rates. The sample-size for this study was not based on a formal statistical power analysis. Qualitative analysis may not be comprehensive as analysis was limited by sample size rather than thematic saturation. As CME course data and participant characteristics were kept separate from this survey, it is unclear how representative the sample is of the study population. Due to potential biases in response rate, interpretation of the results should be done with caution. In this study, the strong support for public breastfeeding could be influenced by selection bias. Furthermore, if respondents attended more than one CME conference, this may lead to over-representation of a single respondent’s opinion. Additionally, this study was administered to attendees at CME courses operated by our institution; there may be variations in responses and attitudes not identified by our population. This may affect the generalizability to other institutions and international conferences. However, the questions asked were general, about any recent CME course attended, and not specific to the lactation support at current courses. Prior research suggests that barriers to lactation are pervasive, so these themes are likely generalizable. Additionally, attendees were from across the nation and multiple subspecialty CME events were included, enhancing the generalizability of the study results.
Next, while all conference attendees were invited to respond to the survey, the majority of all survey respondents identified as female (74%). The survey used gender neutral terminology for lactating individuals regarding personal experience; while the survey asked for self-identified sex as a demographic, this likely does not fully describe any gendered differences in respondent attitudes. Additionally, the majority of survey respondents were physicians in non-surgical subspecialties. Experiences of other medical specialties or HCP roles may differ, and future research should expand generalizability. Future studies will need to be performed to address these issues. Additionally, no currently validated study met our needs. The survey utilized is not validated but was developed from common themes presented in prior literature regarding lactation accommodations for physicians.
Conclusion
The current state of lactation accommodations at CME courses is inadequate and contributes to inequitable educational experiences for lactating participants. The impact of inadequate lactation accommodations and support may have long-lasting implications for the professional and personal development of lactating HCPs. Overall, course participants recognize the importance of and support lactation accommodations at CME events. Specific needs outlined by this study include having private and designated spaces for lactation, appropriate signage, sanitization, easy access, and the ability to continue participating in the course. While refrigeration was not consistently provided based on our survey analysis, thematic analysis of respondent preferences did not identify refrigeration as an important theme for improvement. Future studies should further evaluate what components of accommodations define adequate lactation support in various settings. Until changes are made to address these barriers, there will continue to be inequity facing lactating HCPs at CME courses.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251375704 – Supplemental material for Lactation accommodations at continuing medical education courses: Attendee attitudes, needs, preferences, and experiences
Supplemental material, sj-docx-1-whe-10.1177_17455057251375704 for Lactation accommodations at continuing medical education courses: Attendee attitudes, needs, preferences, and experiences by Patricia Carey, Arya B. Mohabbat, Elizabeth Wight, Sanjeev Nanda, Sara Bonnes, Debra Blomberg, Ivana T. Croghan, Darrell Schroeder and Hannah Nordhues in Women's Health
Footnotes
Acknowledgements
The authors would like to thank the CME course directors for allowing them to distribute the survey to their course participants, and without whom this project would not have been possible.
Authors’ note
All authors have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline.
Ethical considerations
This project was approved by Mayo Clinic Institutional Review Board (22-006975) and was exempt from continued review.
Consent to participate
The survey was voluntary and all information was de-identified. Survey respondents consented to participate in the survey.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: REDCap was the data entry system for this trial. This project was supported in part by the Center for Clinical and Translational Science Grant Number UL1TR002377 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. This study was also supported in part by the Division of General Internal Medicine which supported time and effort for the regulatory support, REDCap build and electronic survey management (ITC) and funding for the statistical support (DRS).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.