
Abstract
Background:
Socio-economic disparities in stillbirth persist in Australia and other high-income countries. Despite increased attention to disparities in perinatal outcomes, including stillbirth, very little is known about the way conversations about stillbirth prevention are occurring within pregnancy care.
Objectives:
Understand how conversations about stillbirth prevention are experienced by parents of refugee and migrant backgrounds, interpreters, and healthcare professionals within public maternity services in Victoria and South Australia.
Design:
An interpretive qualitative design was used.
Methods:
Semi-structured interviews with 62 participants: 47 parents of refugee and migrant backgrounds, six midwives, five medical doctors, and four interpreters. Data were analysed using reflexive thematic analysis.
Results:
Analysis produced three themes: (1) searching for the right balance, reflecting health professionals’ hesitation to provide direct information if it might promote unnecessary distress or fear, or result in parents’ feeling coerced into medical intervention; (2) patterns and consequences of culturally unsafe care, situating conversations about stillbirth prevention within complex interpersonal and systemic contexts; and (3) safety within relationships built with time, illustrating time and trusting relationships as integral to culturally safe care. Health professionals’ hesitation to discuss stillbirth prevention directly with families restricts access to important health information for a population already facing numerous, longstanding barriers to high-quality maternity care. Distrust between parents, health professionals, and interpreters, fuelled by fragmented and time-poor maternity service design and delivery, can undermine the possibility of culturally safe conversations about stillbirth prevention.
Conclusion:
Investment to make culturally safe pregnancy care possible for women and families of refugee and migrant backgrounds is integral to reducing preventable stillbirths.
Keywords
Introduction
In Australia and other high-income countries socio-economic disparities in stillbirth persist.1–7 Australian population-based studies have consistently identified that women of refugee and migrant backgrounds are more likely to experience stillbirth than non-Indigenous Australian-born women.7–9 Despite efforts to address perinatal inequities, many women and families of refugee and migrant backgrounds continue to experience culturally unsafe or discriminatory care, poorer access to models of maternity care offering continuity of caregiver, and difficulties accessing quality interpreter services.3,10–14
Access to health information in women’s preferred language is an established foundation of quality maternity care,15,16 and the Australian Stillbirth Clinical Care Standard establishes that all women should receive information about the possibility of stillbirth early in pregnancy and be supported to adopt strategies that may reduce their risk. 17 However, sharing health information relating to stillbirth prevention within pregnancy care can be complex, particularly when conversations are occurring across languages and cultural contexts. This can place women and families of refugee and migrant backgrounds at risk of missing critical stillbirth prevention information.3,10,18,19 Compounding the challenge for health professionals, very little is known about refugee and migrant background parents’ experiences and preferences regarding having conversations about stillbirth prevention during pregnancy care. Nor is there a robust literature on the experiences of health professionals and interpreters in sharing stillbirth prevention information with women and families.
We report two qualitative studies conducted in Australia which aimed to support efforts to address stillbirth disparities by seeking to understand experiences of having conversations about stillbirth prevention during pregnancy from the perspectives of recent parents of refugee and migrant backgrounds, interpreters, and health professionals providing pregnancy care in Australia. The research was undertaken in partnership with two specialist refugee health agencies: The Refugee Health Service in Adelaide, South Australia, and the Victorian Foundation for Survivors of Torture (Foundation House) in Melbourne, Victoria.
Study context
Australian states and territories provide publicly funded maternity care to Australian citizens and others eligible for Medicare, 20 with a majority of families receiving public care (~75% in both Victoria and South Australia). 21 Women and families may be offered a choice regarding what model of maternity care they receive, though the specifics of these models and access to them can vary significantly between different maternity services. Public hospital maternity care is the most common model in both states, which usually involves women and families being cared for by different midwives and obstetricians across pregnancy, intrapartum, and postnatal care. The individual health needs of the woman and baby will influence how care is collaboratively organised between midwives and obstetricians, with other specialist medical, allied health, and language professionals (interpreters) included as necessary. The current strategy underpinning Australian maternity services emphasises the importance of continuity of care and caregiver; however access to models which enable continuity remains inconsistent.22,23
Methodology
Data were generated in two qualitative studies undertaken in South Australia and Victoria in 2020 (study 1), and in Victoria in 2021–2022 (study 2). Both studies sought to understand how conversations about stillbirth prevention during pregnancy care are experienced by recent parents of refugee and migrant backgrounds, with consistent approaches to recruitment, consent, and data generation and analysis. Study 1 also sought the perspectives of health professionals providing pregnancy care, and study 2 explored the experiences of interpreters working in pregnancy care settings. A qualitative design adopting a constructionist paradigm was used to facilitate interpretation of how conversations about stillbirth prevention are experienced, with sensitivity to the influences of culture, language, power, and worldview.24–26
Community involvement
Community members of refugee and migrant backgrounds, including parents, were involved in the research through partnerships with two specialist refugee health agencies, and the inclusion of community researchers within the study team. Community researchers have diverse cultural and linguistic backgrounds and are employed to work within their own communities.27,28 With established community networks and critical insights into ways to ensure research is culturally safe, community researchers were instrumental to the conduct of both studies. Nine community researchers who identified as belonging to study cultural and language groups (Table 1) were employed to inform approaches to recruitment, data generation and analysis, and community dissemination. In Victoria, community researchers conducted interviews in participants’ preferred language and facilitated translation and transcription of interviews to English. In South Australia, data generation was completed by another member of the research team with the assistance of an interpreter where necessary.
Participant characteristics (parents).
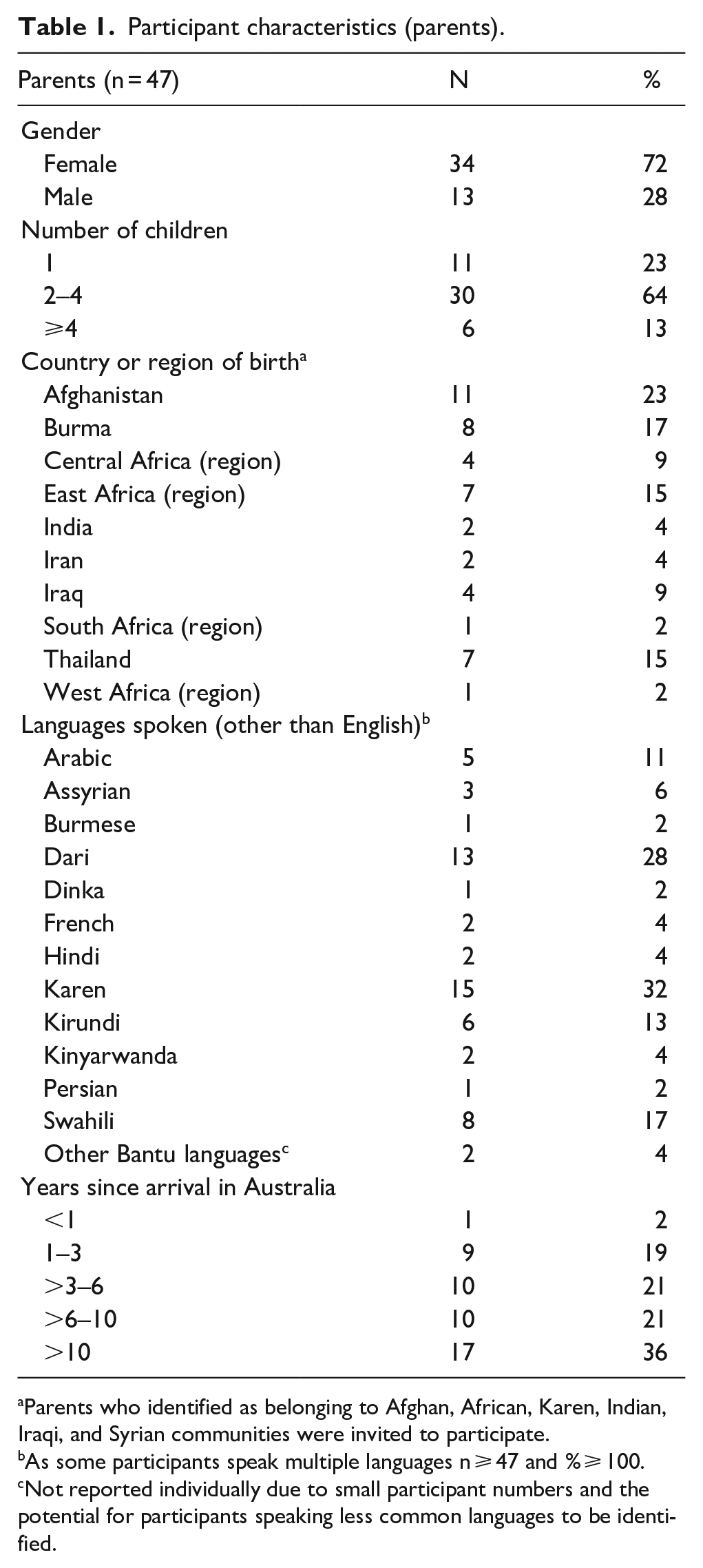
Parents who identified as belonging to Afghan, African, Karen, Indian, Iraqi, and Syrian communities were invited to participate.
As some participants speak multiple languages n ⩾ 47 and % ⩾ 100.
Not reported individually due to small participant numbers and the potential for participants speaking less common languages to be identified.
Recruitment and consent
Recent parents
Purposive sampling was used to recruit women and men who were aged 18 years or older; born in a low- or middle-income country and identified as belonging to the communities outlined in Table 1; and had a liveborn baby in the previous 12 months. Participants were recruited via the networks of community researchers, community organisations, and partner refugee health agencies. Potential participants were approached by a member of the research team in their preferred language and provided with opportunities to ask questions about the research or their participation. Consent was undertaken in participants’ preferred language, with both written and verbal consent options offered to enhance safety and ensure participants not literate in their preferred language were not prevented from participating. Snowball sampling was also used, whereby participants could let others within their networks know about the opportunity to participate in the study. We adopted a pragmatic and situated approach to recruitment; we aimed to recruit a total of 20–30 women and 10–20 men, as our previous research experiences suggested that this number of participants would produce data rich and complex enough to address our research aims without overwhelming the capacity of the team to undertake the work with integrity. 29
Health professionals and interpreters
Purposive and snowball sampling were used to recruit health professionals and interpreters who regularly work in public maternity services via the professional networks of the study team. Potential participants were sent a participant information sheet and invited to ask questions about the study or their participation prior to completing a consent form. Similar to our approach with parents, we aimed to recruit a total of 10–15 health professionals and 5–10 interpreters, as we understood from previous work that participant groups of this size were likely to generate complex datasets. Our pragmatic approach to recruitment was particularly appropriate, given the pandemic-related stressors health professionals and interpreters were navigating at the time of the study. We did not adopt data saturation concepts, as their use has been strongly discouraged as methodologically incoherent in studies utilising reflexive thematic analysis.29,30
Data generation and analysis
Data were generated via semi-structured interviews conducted via telephone or video platforms. Interview theme guides were developed by the research team and applied flexibly; interviewers were encouraged to identify and follow leads within the views and experiences participants shared (Supplementary File 1). Interviews were audio recorded with participant consent and transcribed. Interviews undertaken in languages other than English were translated to English during the transcription process by the member of the research team who undertook the interview.
The dataset comprised audio recordings, transcripts with associated language/translation notes where relevant, and fieldnotes. Data were analysed by the first author using reflexive thematic analysis as developed by Braun and Clarke.24,30,31 Reflexive thematic analysis is subjective and artfully interpretive, 32 with themes generated to explain patterns of shared meaning in the data. In accord with recently published best practice approaches for methodologically coherent reporting of studies using reflexive thematic analysis, 30 additional information regarding our analytic process is provided in Supplementary File 2, including our analytic use of the concept of “cultural safety.” Reporting has been informed by the Reflexive Thematic Analysis Reporting Guidelines (Supplementary File 3), 30 which can be accessed via the EQUATOR website. 33
Results
A total of 62 people participated (Tables 1 and 2).
Participant characteristics (health professionals and interpreters).
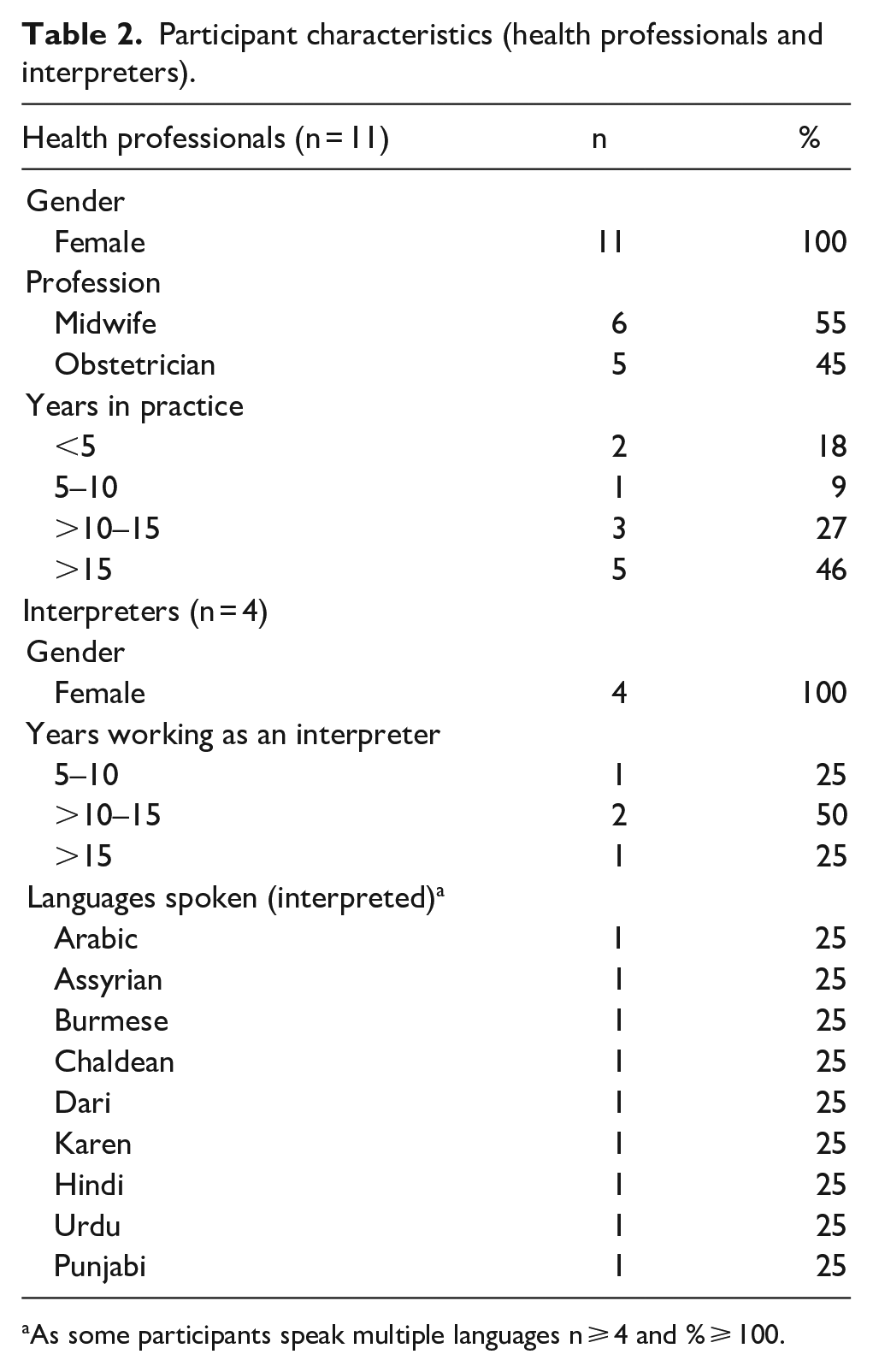
As some participants speak multiple languages n ⩾ 4 and % ⩾ 100.
Analysis produced three themes: searching for the right balance; patterns and consequences of culturally unsafe care; and safety within relationships built with time (Table 3). Direct participant quotes are presented as is appropriate when using reflexive thematic analysis.
Theme summary.

Searching for the right balance
This theme reflects the way participants (parents, health professionals, and interpreters alike) understood the need for approaches to stillbirth prevention in pregnancy care to incorporate a deliberate balance between sharing transparent and direct information with parents without promoting unnecessary distress, fear, or coercion.
Parents were clear in their desire to access thoughtful and direct information regarding stillbirth prevention, and felt that this is something that all parents should have access to: Yeah we can talk about [stillbirth]. . . I would like to know. It would be good because then we can know about how to prepare and take care so that that doesn’t happen to our baby. (Recent mother) I think it is very important that health care professional provide a clear verbal explanation about stillbirth and about the preventative factor. This is because if a woman is informed about potential risks factor during their pregnancy then they can prepare or do the right thing to reduce their risk. (Recent mother)
Although health professionals understood stillbirth prevention as an important element of high-quality pregnancy care, they hesitated to link conversations about topics such as fetal movements directly to stillbirth prevention, feeling they were “not good at telling it like it is.” This hesitation rested on a strong desire not to cause distress or fear for women and families, an understanding that discussions about stillbirth prevention can be “a bit anxiety-provoking,” a feeling that women would not want to speak directly about stillbirth at every pregnancy appointment, and a desire to avoid the topic of stillbirth being used to coerce women and families into making particular decisions, for example, regarding induction of labour: I think we are not good in linking [fetal movements and stillbirth] together. We just say, “It’s very important that you look at the movements of the baby. If it changes in any way you need to let us know”. . . but to say then in that sentence, “Because we don’t want your baby to be stillborn?” No. I don’t even think I say that, no. (Obstetrician) You don’t want to scare people into making decisions, you don’t want to coerce them into making decisions, you don’t want to hang this stillbirth threat over their neck. But you do want to give them the information because if you don’t give it to them, that’s wrong too. . . it’s a very difficult line to walk. (Obstetrician)
Both parents and interpreters were aware of this hesitation, reflecting that stillbirth prevention messages were often discussed during care without direct reference to stillbirth. For a number of parents, participating in the study interview was the first direct conversation they had about stillbirth, despite recently receiving pregnancy care: . . .The doctor didn’t speak about [stillbirth], they mostly just do check-ups on health and measure my stomach. It’s because I didn’t have any problems, so the doctor doesn’t speak to me much, they just check to see if everything is normal. . . I feel that they were avoiding that topic (stillbirth), [avoiding] telling us about it. They don’t speak about it. (Recent mother)
Health professionals’ fears about causing distress were not unfounded. Parents recalled times when repeated discussions during care, particularly regarding risk, could make them feel scared: . . . sometimes too much information is a problem, and this is what happened to me. . . they keep on telling me “don’t eat this don’t eat that because you are a diabetic, if you eat your baby becomes big”. . . so I stopped eating. I got so scared of a caesarean that I stopped eating food. (Recent mother)
Aware that discussions of risk can prompt fear and worry for parents, interpreters worked hard to adopt approaches that supported cultural safety and clear understanding between care providers and families. The cultural, linguistic, and emotional work interpreters undertook commonly occurred “behind the scenes,” beyond the awareness or appreciation of health professionals. Interpreters were clearly integral to the cultural safety of complex conversations within pregnancy care: In English they call it “stillbirth,” but it is difficult to say it in Karen. . . in Karen we will say the baby is ဟါဂီၤ (broken/ruined). . .“[when interpreting the English word “risk”] I have to interpret it as being “with worries/concerns” or “with challenges/complications” that might happen. . . But in Karen we don’t have much word for it. (Interpreter)
Patterns and consequences of culturally unsafe care
By illustrating experiences and consequences of culturally unsafe care, this theme situates conversations about stillbirth prevention as occurring within a complex interplay of interpersonal and systemic factors.
Parents, interpreters, and health professionals’ stories powerfully illustrated that maternity care systems are not well designed to meet the needs of families of refugee or migrant backgrounds. Time-pressured and fragmented pregnancy care due to short appointment blocks, delays and logistical challenges accessing (often ideally female) interpreters, and chronic and broad ranging workforce and systems pressures can compromise experiences of care. All participant groups noted that these issues left families feeling unimportant and uncared for: The problem is their antenatal care is so fragmented, their appointments are so short and so rushed. . . how can you ever possibly go over everything people need to know in maybe nine 15 minute appointments, over a space of 9 months? Can’t really, can you? The time that is given to those women is so minimal, they must feel that they’re a nuisance sometimes. (Midwife) We were comfortable with one of the senior midwives during the pregnancy check-up and we used to share anything with her but not with others because we felt that they did not take the time to really care for us. They just did their routine check and said “everything is ok bye.” (Recent father)
It was rare for parents to have access to appropriate health information in their preferred language during pregnancy, including information about stillbirth prevention. In the absence of appropriately translated health information, health professionals would sometimes provide factsheets or brochures in English and ask the woman to find someone at home who could read it for them. In the context of stillbirth prevention, this could lead to a situation where a woman’s school-age children were asked to read written information about stillbirth prevention as it relates to their own sibling in utero: They gave me a bunch of papers, I think [information about stillbirth prevention] was in there among the pile. They were in English so I couldn’t read it, I just left it. . . they told me to read it, but I can’t read it. . . They said ask someone at home to help you read it. My children can read a little bit but not much. But even if they can read, they don’t know how to interpret [the information] to you. (Recent mother)
Parents recounted experiences of perceived discrimination including racism within maternity care. This included being treated differently by health professionals due to their religion, ethnicity, refugee or migrant backgrounds, or because they did not speak English: Even during my appointments, she [obstetrician] used to go out of the consultation room a lot while I was sitting there, and she was taking a long time to come back to the room. I am not sure why she was doing that, maybe she didn’t like being with me because I was wearing a scarf. (Recent mother) With my third child. . . [the midwife said] “why you guys having another baby anyway? African people love having babies. . . Is it Centrelink? Do you guys get paid or something?” (Recent mother)
Ultimately, experiences of culturally unsafe care, including discrimination and dehumanising care, were distressing, eroded trust, and discouraged parents from seeking help when concerned about their or their baby’s wellbeing: As human beings we should be equal, isn’t that right?. . . We have human rights, and we all are equal, but I want to say that if you don’t treat people right then no one wants to go to you. (Recent father) I want to quote an example here of a midwife who was rude to me. She said “why did you come to hospital when you have just bleeding? Why did you call an ambulance when you don’t require an ambulance?” Maybe it’s a small thing for midwives but not for a would-be mother. So, these kinds of behaviours are really discouraging and make a person hesitant to ask, they make you scared to go again to hospital. (Recent mother)
Safety within relationships built with time
This theme illustrates the ways participants understood time and trusting relationships as interconnected and integral to culturally safe approaches to stillbirth prevention. The centrality of time was discussed as both practical and relational. In practical terms, parents, health professionals, and interpreters all stressed that more time is needed during pregnancy appointments to respond to emotional and cultural needs in addition to biomedical care. This may be especially true for care facilitated with the assistance of an interpreter where adequate time is necessary to ensure information is accurately moved between language and cultural contexts: We’re not given any extra time for appointments or anything, if a woman requires [an interpreter]. So I think that’s just appalling, that we don’t have any extra time to explain things to these women. (Midwife)
Time was discussed as also having important relational impacts. As demonstrated in the previous theme (patterns and consequences of culturally unsafe care), parents can feel unimportant and lose trust in care if they sense that a health professional is rushed or does not have time for them. Professional relationships can also suffer in time-poor and fragmented service systems. Interpreters reflected that when they were able to work consistently within a health service and build relationships with health service staff, they were able to do more to support culturally safe conversations during pregnancy: This is the difference. . . when you freelance and when you are actually part of a hospital setting, I think it makes a big difference, because my responsibility is not only as an interpreter, my responsibility is also as a [health service name] staff member. (Interpreter) . . .when I am not available, we organise interpreters through other agencies. [Agency interpreters] will not have seen [the woman] before and will only speak to them this one time and [then] leave. The interpreter will not know about the patient’s past history or future histories, so it will be more difficult for them to speak for [the woman]. . . So, [women] don’t feel entirely comfortable/satisfied speaking with external interpreters compared with us because they can ask us about everything. (Interpreter)
Health professionals often expressed a strong preference for working alongside interpreters they had an opportunity to get to know over time and therefore felt they could trust. In the absence of these trusting relationships, health professionals could worry that what they were saying was not being interpreted accurately or in full: . . .I have the feeling that interpreters don’t always help. . . sometimes I feel like what I’m saying is not being interpreted. . . but I don’t know how you can get that better unless you have someone that you really trust that speaks their [language], sometimes even their dialect, because you can have someone in the room that speaks the language but not their dialect, and then you’re still talking about oranges and apples; no one understands. (Obstetrician)
Interpreters’ reflections also demonstrate what can happen in the absence of trusting professional relationships. Health and social care professionals involved in the delivery of maternity care could lack experience or confidence working with interpreters, or could treat interpreters very poorly, ultimately compromising the quality of interpretation and therefore quality of care: . . .if the [health professional] have got experience, or has worked with interpreters, so then it will be a very easy going conversation. But some of them you come across, like oh my god. . . they treat you like you’re absolutely nothing. Well, you’re just an interpreter, I am the [health professional], I’m more important part of this conversation. . . [those are the] biggest barrier for you to break, to earn their respect and for them to understand that actually you’re the means of communication between [them] and the client. (Interpreter)
For some parents, opportunities to build relationships with the same health professionals and interpreters over time (continuity of care provider) was critical to their experiences of safety. Other parents, however, did not mind seeing different providers and interpreters so long as they practised with kindness and respect. Regardless of the availability or individual desirability of continuity of care provider, relational care that prioritises and enables compassionate and culturally safe approaches to care was viewed as essential by parents, health professionals, and interpreters alike: They spoke to us with friendliness and smiles and love. They measured us and measured our blood pressure and everything, they did it all with kindness, so I was happy about that. (Recent mother) I think that women are very open and happy to share their experiences with you if give them the time to listen to them. (Obstetrician) I think it’s more about body language, it’s not about not discussing [stillbirth], because if you talk about stillbirth, then they would appreciate the fact that you are helping them, the clinician is helping them to have a healthy and successful pregnancy. . . So, when you talk about it as information, so it is culturally safe. . . [families] will be more careful. (Interpreter)
Discussion
As identified in past research,3,19,34,35 health professionals in our study acknowledged that they often hesitated to speak directly with women and families about stillbirth due to fears they could cause unnecessary distress or worry. Conversations about elements of care such as monitoring fetal movements were common, but rarely directly linked to the prevention of stillbirth. Although health professionals may find it challenging to speak directly about stillbirth prevention with women and families during pregnancy, there are added complexities that are likely to make it even more challenging for health professionals having these conversations with women and families of refugee and migrant backgrounds. This may include uncertainty about how to approach conversations about stillbirth in culturally safe ways, confidence working alongside interpreters, and concerns regarding their ability to assess if information shared has been understood by women and families.12,36–38 Notwithstanding the challenges that health professionals experience in facilitating these conversations, recent parents and interpreters both felt that direct, thoughtful, and culturally safe conversations about stillbirth prevention ought to be part of pregnancy care for families of refugee and migrant backgrounds.
Despite shared ambitions amongst health professionals, interpreters, and recent parents for culturally safe approaches to stillbirth prevention to be embedded within pregnancy care, our study has identified a range of interpersonal and systemic factors that pose significant barriers to these ambitions being realised. Barriers include distrust in maternity care providers and services as a consequence of culturally unsafe care, fragmented and inflexible maternity service design and delivery, and inconsistent opportunities for parents, health professionals, and interpreters to build trusting relationships over time.
This study supports previous research identifying barriers to direct conversations about stillbirth prevention during pregnancy care and reinforces the importance of culturally safe maternity care.3,17,19,34,35 Importantly, the study offers new insights about the role of interpreters, rarely included within stillbirth research, with implications for maternity policy and practice in Australia and other high-income country contexts (Figure 1).
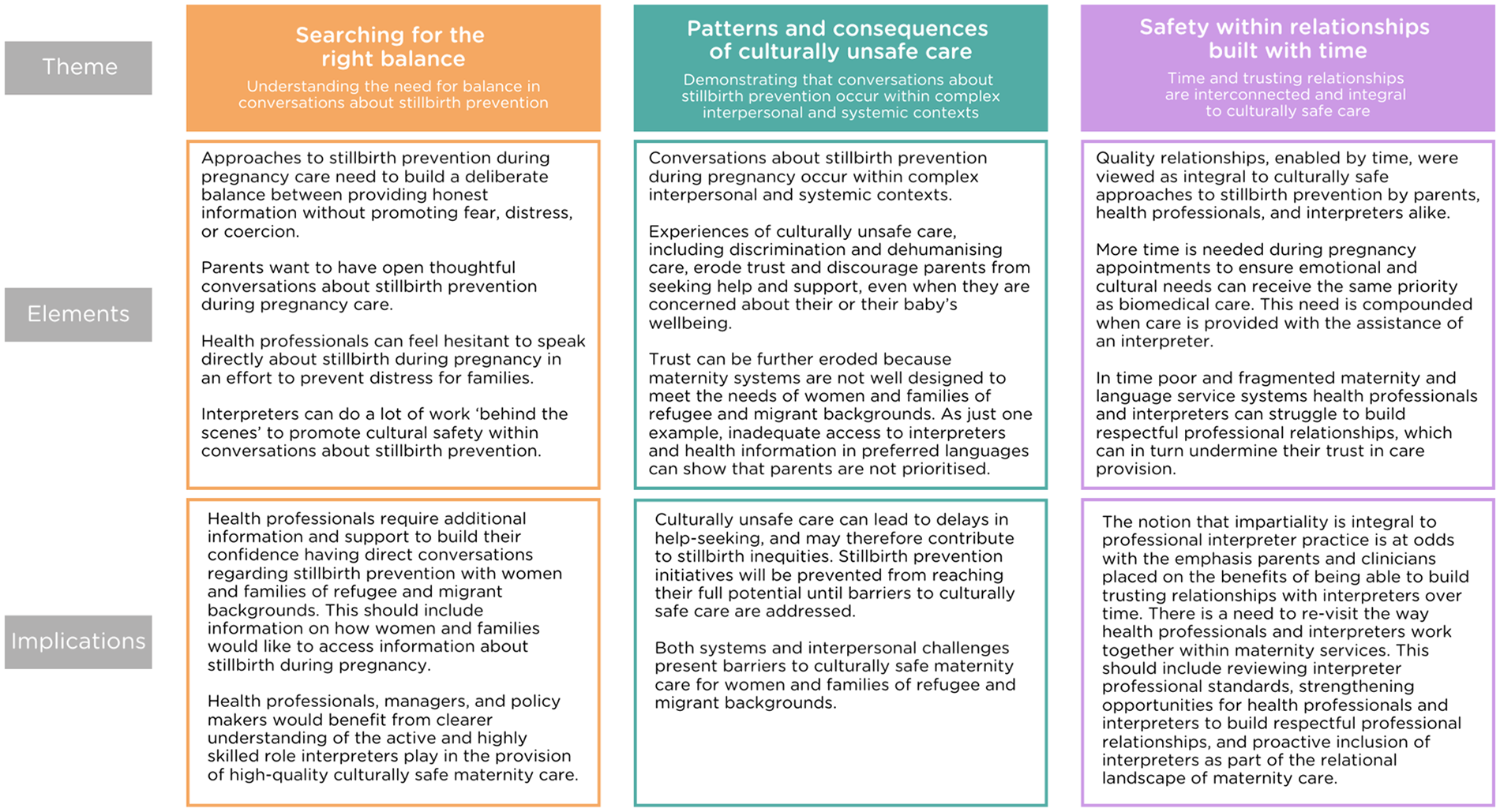
Results and implications.
Relational care is consistently identified as an important foundation of quality maternity care, including maternity care for women and families of refugee and migrant backgrounds.13,22,39–41 Relational qualities of care have also been highlighted as having the potential to help address perinatal disparities. For example, there is evidence that midwifery continuity of care, and the inclusion of bicultural workforces, is associated with improved experiences of and access to care.14,42,43 However, interpreters are rarely identified within the literature as part of this relational landscape. Indeed, the professional code of ethics for interpreters practising in Australia states that “professional detachment is required for interpreting and translation assignments in all situations,” and “where impartiality may be difficult to maintain because of personal beliefs or other circumstances, interpreters and translators do not accept assignments, or they offer to withdraw from the assignment.” 44 This presents a critical paradox, whereby parents, health professionals, and interpreters have emphasised the positive impact of being able to build meaningful relationships over time on experiences and perceptions of safety and quality in maternity care, but formal professional codes proactively discourage interpreters from practising in this manner. The argument that it is desirable or even possible for interpreters to remain impartial has faced strenuous criticism within the literature as utopian and unrealistic.12,38,45–49 Despite this, debate continues in interpreting and translating fields, and the concept of impartiality remains central to interpreter professional codes and standards in Australia 44 and the United Kingdom. 50
This study and past research have demonstrated that the highly skilled role interpreters can play in supporting cultural safety and understanding between health professionals and families can be underestimated or even mistrusted by health professionals.36,45,51 There is an opportunity for health professionals and interpreters, and maternity and language services, to re-evaluate their ways of working together. New approaches which better acknowledge and support the role interpreters can play in high-quality culturally safe maternity care, and promote opportunities for health professionals and interpreters to build meaningful professional relationships over time, could help to address some of the stubborn and in some cases worsening perinatal disparities evident in Australia and other high-income countries.3,6,52,53
Culturally unsafe experiences of care are an established barrier to maternity care for women and families of refugee and migrant backgrounds, including bereavement care, and a factor known to contribute to perinatal disparities.3,13,40,41,54 Parents clearly articulated changing their behaviours in response to experiences of unsafe care, including not discussing concerns or questions during antenatal appointments if they saw a clinician they did not trust. Until recently, efforts to address stillbirth disparities in Australia have largely focussed on the provision of clinical care, such as the identification and appropriate management of fetal growth restriction. 55 While the importance and clinical responses to factors relevant to stillbirth prevention like fetal growth restriction are well-defined, our study clearly demonstrates that culturally unsafe care can prevent families of refugee and migrant backgrounds from accessing appropriate information and clinical management. Therefore, well-designed evidence-based approaches to stillbirth prevention will not reach their full potential unless coupled with comparable investment to ensure care is culturally safe. As articulated in the Stillbirth Clinical Care Standard, 17 services need to take concerted action to ensure cultural safety and equity, which may include structural change and professional development to strengthen cultural safety, address structural racism, and enhance multidisciplinary team work.
Strengths and limitations
Strengths of this article include participation of parents (women and men) from a range of cultural backgrounds, including those not able to participate in English, facilitated by community researchers and refugee agency partnerships; and the involvement of interpreters who are rarely included in perinatal research. Results present an important opportunity to ensure maternity practice and policy is informed by the lived realities of parents, interpreters, and health professionals.
Recruitment of study participants via trusted specialist organisations and community and professional networks can help to enhance participant safety, especially for communities of refugee background who may be less familiar with research practices. 27 Interviews were undertaken via phone or video platform (e.g. Zoom) due to COVID-19 restrictions in place during the study period. While research using virtual methods during the pandemic could present challenges, a number of recent publications have identified potential benefits of engaging with research participants virtually, including when undertaking research with marginalised communities.56,57 The option for participants to engage via telephone ensured reliable Internet access was not required in order to participate.
Data generation was undertaken during the initial period of implementation of the Safer Baby Bundle in Victoria. 55 The Bundle, an Australian initiative led by the Stillbirth Centre of Research Excellence, includes five evidence-based elements which aim to improve key areas of practice known to influence stillbirth. The Bundle was not in use in South Australia at the time of data generation. We were sensitive to this contextual factor during analysis. Some Victorian parents received maternity care at a health service utilising the Bundle, which did include resources for parents (though at that time not available in a range of languages). In addition, a number of health professional and interpreter participants were providing care in a service that was implementing the Bundle. Importantly, all study results (themes) were generated from participants at both Bundle and non-Bundle sites, suggesting our results remain relevant for maternity services regardless of the implementation of the Safer Baby Bundle. One specific example of this is the reluctance of health professionals to directly discuss stillbirth during pregnancy care. The availability of Bundle resources which health professionals could share with families did not in isolation make health professionals more confident to link health information directly with prevention of stillbirth. Indirect conversations about individual health behaviours (e.g. monitoring fetal movements, smoking cessation) were common practice for participants at Bundle and non-Bundle sites.
Conclusion
This article provides rare insights into the realities of conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, interpreters, and health professionals. Health professionals’ hesitation to discuss stillbirth prevention directly with women and families restricts access to important health information for populations already facing numerous and longstanding barriers to high-quality maternity care. Distrust between parents, health professionals, and interpreters, fuelled by fragmented and time-poor maternity service design and delivery, can undermine the possibility of culturally safe conversations about stillbirth prevention. Ultimately, efforts to address preventable stillbirths require significant investment to address well-documented barriers to culturally safe maternity care. Future work should seek to understand how these interpersonal and systemic barriers can be addressed with professional, service, and system reform.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251365726 – Supplemental material for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study
Supplemental material, sj-docx-1-whe-10.1177_17455057251365726 for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study by Laura J. Biggs, Jane Yelland, Clemence Due, Elisha Riggs, Anna Ziersch, Erin Green, Shadow Toke, Shogoufa Hydari, TaMwePaw Noe, Josephine Sheriff, Maryaan Essa, May Alqas Alias, Ashay Baguet, Sana Zia, Josef Szwarc, Joanne M. Said, Philippa Middleton and Stephanie J. Brown in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251365726 – Supplemental material for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study
Supplemental material, sj-docx-2-whe-10.1177_17455057251365726 for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study by Laura J. Biggs, Jane Yelland, Clemence Due, Elisha Riggs, Anna Ziersch, Erin Green, Shadow Toke, Shogoufa Hydari, TaMwePaw Noe, Josephine Sheriff, Maryaan Essa, May Alqas Alias, Ashay Baguet, Sana Zia, Josef Szwarc, Joanne M. Said, Philippa Middleton and Stephanie J. Brown in Women's Health
Supplemental Material
sj-pdf-3-whe-10.1177_17455057251365726 – Supplemental material for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study
Supplemental material, sj-pdf-3-whe-10.1177_17455057251365726 for Conversations about stillbirth prevention during pregnancy care from the perspectives of recent parents of refugee and migrant backgrounds, health professionals, and interpreters: A qualitative study by Laura J. Biggs, Jane Yelland, Clemence Due, Elisha Riggs, Anna Ziersch, Erin Green, Shadow Toke, Shogoufa Hydari, TaMwePaw Noe, Josephine Sheriff, Maryaan Essa, May Alqas Alias, Ashay Baguet, Sana Zia, Josef Szwarc, Joanne M. Said, Philippa Middleton and Stephanie J. Brown in Women's Health
Footnotes
Acknowledgements
We would like to thank all study participants who shared their experiences and perspectives with us, and Fran Hearn, member of the Intergenerational Health Group at the Murdoch Children’s Research Institute, who supported community researchers undertaking interviews with recent parents.
Ethical considerations
Ethics approval was obtained from the Royal Children’s Hospital Human Research Ethics Committee (54826 and 66188) and the University of Adelaide Human Research Ethics Committee (54826).
Consent to participate
Consent was undertaken in participants’ preferred language, with both written and verbal consent options offered to enhance safety and ensure participants not literate in their preferred language were not prevented from participating.
Consent for publication
Consent to draw on participant experiences for publication, including anonymised quotations, was obtained prior to participation in the study.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Stillbirth Foundation Australia, and Commonwealth Department of Health 4-D1ON89X. Laura J. Biggs was supported by an early career fellowship from the NHMRC Stronger Futures Centre of Research Excellence (#1198270) while undertaking this project; Stephanie Brown is supported by an NHMRC Leadership Grant (L2)#2018144. Research at the Murdoch Children’s Research Institute is supported by the Victorian Government’s Operational Infrastructure Support Programme.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Due to the highly sensitive and identifying nature of interview data it is not possible for study data to be shared.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.