
Abstract
Background:
Cesarean section delivery is a surgical way to safeguard maternal and neonatal health when medical risk is associated with delivering babies. Its rates have been increasing globally over the past few decades, with a significant rise recorded in low- and middle-income countries, which leads cesarean section to crucial public health concerns due to unnecessary surgical interventions and associated risks for maternal and neonatal.
Objectives:
This study aims to identify the socioeconomic and demographic determinants contributing to the higher likelihood of cesarean section deliveries among Bangladeshi mothers residing in urban areas.
Design:
The initial survey employed a cross-sectional design to collect data.
Methods:
This research examined the Bangladesh Demographic and Health Survey (BDHS) dataset to identify the cesarean section among urban mothers. It utilized the chi-square test to measure associations, the Boruta algorithm, and a multivariable logistic regression model with a forest plot.
Results:
The study pointed out that urban mothers belonging in richer and richest families (adjusted odds ratio: 2.83, 95% confidence interval: 1.88–4.26 and adjusted odds ratio: 4.79, 95% confidence interval: 3.13–7.34) and higher educational attainment (adjusted odds ratio: 1.89, 95% confidence interval: 1.20–2.99) are significantly correlated with cesarean section. Divisional differences are also robust with the significance of Sylhet (adjusted odds ratio: 0.23, 95% confidence interval: 0.12–0.47) and Chottogram (adjusted odds ratio: 0.50, 95% confidence interval: 0.30–0.83) divisions. Media exposure (adjusted odds ratio: 1.54, 95% confidence interval: 1.27–1.87) and mothers gave birth at the age 20–24 and 25–34 (adjusted odds ratio: 1.67, 95% confidence interval: 1.31–2.14 and adjusted odds ratio: 3.15, 95% confidence interval: 2.03–4.89) are also highly significantly associated with the likelihood of cesarean section. Moreover, mothers working status (adjusted odds ratio: 0.53, 95% confidence interval: 0.43–0.65) and religion (adjusted odds ratio: 2.33, 95% confidence interval: 1.60–3.38) are also correlated with cesarean section.
Conclusion:
The study reveals socioeconomic and sociodemographic reasons associated with the increase in cesarean section rates among urban mothers in Bangladesh, highlighting the need for targeted interventions to mitigate cesarean section rates and improve maternal and neonatal health.
Introduction
Cesarean section (CS), often referred to as C-section, is a crucial surgical procedure introduced in the late 19th century to prevent life-threatening medical conditions for mothers and newborns.1 –5 However, both maternal and child health and well-being can be negatively impacted by medically unnecessary CS deliveries. As with any major surgery, CS is associated with both short- and long-term risks,6,7 including increased hazards of preterm or early-term 8 births and, in some cases, neonatal 9 deaths. A study found that CS delivery can cause two to four times higher maternal deaths than normal deliveries. 10 The increase in the global CS delivery rate has resulted in considerable clinical and economic challenges for the healthcare system, causing harm to maternal and infant health.11 –14 Even then, a steadily rising trend has been observed over the past 20 years in CS delivery globally. 14 The CS rate has increased from 7% to 21% from 1990 to 2024 globally, accounting for one CS in every five deliveries. The World Health Organization (WHO) projects that this rate is going to be 29% by 2030 globally and likely to be 63% in Eastern Asia, 50% in Western Asia, 54% in Latin America and the Caribbean, 48% in Northern Africa, and 47% in Southern Europe, 15 whereas it is necessary to limit CS to only those cases where it is clinically necessary, the 10%–15% threshold by WHO for CS has since been challenged.16 –18 A study conducted in 2024 showed that CS rates vary in sub-Saharan Africa; few countries experience low rates due to limited access to health facilities, and few countries experience increases. 19 Another study revealed that the weighted average CS rate in sub-Saharan Africa is 3.5%, but in Northern Africa, it is 27%. 20 Research conducted using Demographic and Health Survey data from nine South and Southeast Asian countries, including Bangladesh, showed a significant trend toward surgical deliveries. 21 Asia recorded the highest average annual rate of CS increase, whereas the global average CS rate increased by 12.4% between 1990 and 2014. 20 In Bangladesh, the overall CS rate has increased significantly from 2.7% to 24% between 2000 and 2014.21,22
The global rise in CS deliveries has become a great public health concern, mostly driven by socioeconomic and sociodemographic conditions rather than medical indications. 23 Studies suggest that CS is more likely among those mothers carrying babies smaller or larger than average, 21 younger mothers with a small pelvis, 24 and shorter mothers. 25 However, South Asian countries, including Bangladesh and India, experience high CS rates in low-risk women, particularly in urban areas with private healthcare settings, largely driven by the mother’s age and education, family wealth, and greater access to healthcare. 26 Studies have revealed that CS are high even among the poor when they are delivered in private facilities. 27 Moreover, a prior study reported that sometimes doctors suggest CS for financial gains without any medical indications. 28 Multiple studies have reported that increased CS rates in low- and middle-income countries are significantly associated with increased utilization among affluent urban mothers.20,29 A recent study conducted on 26 sub-Saharan African and South Asian countries found that the rate of CS was greater among urban populations. 4 Furthermore, it was found that the urban wealthier women were 15% more likely to use the CS delivery option than the poorer. 29 This trend is similar in Bangladesh as well. 30 From 1996 to 2018, CS delivery increased gradually from 0% to ~43% among urban mothers. 30
Although many studies have investigated population-based datasets to identify the reason behind rocketing CS rates,21,29,31 in Bangladesh, previous studies shows inconsistencies related to the use of data sources, limiting or varying sample size, and selection criteria, differences in methodological approaches such as descriptive versus multivariate analysis and variation in study aims with some focusing primarily on clinical indication, 4 whereas some are emphasizing broader sociodemographic and socioeconomic influencers.32 –34 However, a few studies have examined the demographic and socioeconomic determinants of Bangladeshi urban women. To promote medically justifiable CS deliveries, it is crucial to understand these determinants in formulating policies. 35 The study focuses on urban women since CS rates in urban areas are noticeably greater than in rural ones. 30 Greater access to private healthcare facilities, better socioeconomic levels, and variations in giving birth preferences affect this as well. 29 Particularly private ones, urban hospitals can actively encourage CS.36,37 Therefore, this study aims to explore socioeconomic and demographic risk factors that are correlated with CS among urban mothers in Bangladesh. These findings might help policymakers and governments make plans based on evidence to lower the adverse effects on both maternal and neonatal health while maintaining CS rates within the WHO’s recommended range.
Materials and methods
Data source and study design
This is a cross-sectional study that utilizes a secondary database extracted from the latest national survey (Bangladesh Demographic and Health Survey (BDHS)-2022) to investigate the risk factors influencing CS delivery in urban regions. This survey applied a two-stage stratified sampling method, selecting 675 listing units in the first stage using the probability proportional to size (PPS) sampling method. Of the 675 units, 438 are in rural areas, whereas 237 are situated in urban areas. A comprehensive family list was compiled in all enumeration units chosen in the first stage to function as a sampling framework in the second stage for household selection. In the second stage, 30 households were selected for each listing unit using a systematic sampling procedure. The survey was conducted with a total of 73,239 pregnancy records, comprising 24,355 from urban areas and 48,884 from rural areas, across 674 clusters following the exclusion of one rural cluster in Cox’s Bazar, Chittagong, due to security issues. The study included 11,562 women who responded to the question “Was the baby delivered by a CS?” and excluded women who resided in rural areas. The final sample comprised 3628 records following the removal of missing values. A weighted sample is employed in the analysis to validate the representativeness of the country’s sample. The weighted sample size amounts to 2969. The sampling procedure and guidelines for weight usage are outlined in the BDHS-2022 report. 38 The initial countrywide cross-sectional survey was conducted in four phases (each about 4 weeks in duration) beginning on June 27, 2022, and ending on December 12, 2022. Moreover, the reporting of this study conforms to the STROBE statement. 39
Target variable
The target variable in this study was coded as a dichotomous variable indicating CS delivery among women residing in the urban area in response to the question asked “Was the baby delivered by a CS?,” categorized as (i) no and (ii) yes and assigned values “0” and “1,” respectively.
Control variables
This study takes into account sociodemographic and socioeconomic variables as covariates, including maternal age (15–19, 20–24, 25–34, and 35–49 years), age at marriage (15–17, 18–24, and 25–34 years), age at first birth (15–19, 20–24, 25–34, and 35–49 years), educational attainment (none, primary, secondary, and higher), current working status (no and yes), wealth index (poorest, poorer, middle, richer, and richest), preceding pregnancy interval (<24, 24–48, and ⩾48), pregnancy order (1, 2, 3, and 4 or more), history of terminated pregnancies (no and yes), multiple delivery (no and yes), media exposure (no and yes), religious affiliation (Muslim and others), husband’s education level (none, primary, secondary, and higher), husband’s occupation (not working, worker, business, and service), and divisions (Barishal, Chattogram, Dhaka, Khulna, Mymensingh, Rajshahi, Rangpur, and Sylhet). The selection of variables was determined by their availability in the BDHS-2022 dataset, self-efficacy, and available literature.4,21,30,40,41
Statistical methods
This study considered the chi-square test to examine associations between the type of delivery and specific sociodemographic factors. Moreover, the Boruta algorithm was deployed for feature selection, which identified the most influential factors for CS deliveries. In this algorithm, the feature importance is estimated numerically. The “importance” measure of an attribute is determined as the loss of accuracy of classification based on the random permutation of attribute values between objects. Following that, the average and standard deviation of the accuracy loss are calculated. As a measure of importance, the Z score can be calculated by dividing the average loss by its standard deviation.42,43 The multivariable logistic regression model was used to identify the most significant factors for CS deliveries. Survey weight (V005: women’s individual sample weight) provided in the BDHS-2022 dataset was applied to account for the hierarchical survey design to ensure a population representative estimate. Forest plots were employed to illustrate the 95% confidence intervals (CIs) of the odds ratios (ORs) for covariates. All the analyses were conducted using STATA 17 (StataCorp LLC, College Station, TX, USA) and RStudio (Posit PBC, Boston, MA, USA), and a p < 0.05 was considered significant.
Ethical approval and consent to participate
In this study, a publicly available BDHS dataset was used, which was controlled by the Ministry of Health and Family Welfare of the Bangladesh Government. As the data are anonymized and publicly available to use, so no ethical approval was needed for this research. However, the original BDHS was reviewed and approved by the Institutional Review Board of ICF Macro in Calverton, United States, and the Bangladesh Medical Research Council, the national ethical committee in Bangladesh. Consent to participate is not applicable.
Results
It is observed that in 2022, 52.37% of urban women and 35.7% of rural women underwent the surgical delivery process; however, the CS rate was reported at 43% among urban women in 2018, which indicates a substantial rise over the past few years. In 2018, the division-wise prevalence of CS was Barishal (24.5%), Chattogram (26.0%), Dhaka (42.7%), Khulna (42.7%), Mymensingh (26.1%), Rajshahi (35.6%), Rangpur (27.8%), and Sylhet (22.6%). However, in 2022, the prevalence of CS in different divisions was Barishal (35.0%), Chattogram (31.0%), Dhaka (53.1%), Khulna (66.0%), Mymensingh (38.9%), Rajshahi (53.5%), Rangpur (43.1%), and Sylhet (25.7%). The bivariate analysis was conducted to investigate the association between the sociodemographic characteristics of Bangladeshi mothers residing in urban areas and the type of delivery. To evaluate these associations, the chi-square test was implemented, and the results are reported in Table 1. The results indicated a substantial association between the mother’s age and cesarean deliveries. The most common demographic for cesarean deliveries was mothers between the ages of 25 and 34 (57.4%). Cesarean deliveries are significantly correlated with the age of the mothers at their marriage (p < 0.001). The results of the analysis indicate that women who marry at an advanced age (25–34 years) are more likely to have CS deliveries than other married women (83.8%). CS rates are also highly significant (p < 0.001) when age at first birth is considered. A significant association exists (p < 0.001) between the education of the mother and the CS deliveries. Specifically, mothers with higher levels of education (76.3%) are more likely to undergo CS deliveries than illiterate women (29.0%). CS deliveries were substantially affected by the Wealth Quintile in urban areas. Wealthier women had significantly higher chances of opting for surgical deliveries when compared to the poorest (73.7%, p < 0.001). CS rates are considerably higher among mothers who have been exposed to media (60.2%, p < 0.001). The CS rates are greater among mothers with husbands who work as service holders (65.3%) and those with secondary or higher (73.6%), as evidenced by the significant associations (p < 0.001). Khulna division is the location where nearly three-quarters (71.8%) of the deliveries are CS. CS are prevalent in the urban areas of Bangladesh, specifically in the Barisal, Dhaka, Mymensingh, and Rajshahi divisions.
Association between type of birth and sociodemographic characteristics of Bangladeshi urban mothers, using the chi-square test.

The important covariates of CS in urban mothers were extracted using the Boruta algorithm from the set of significant explanatory variables. This approach gradually identifies the important and unimportant factors through statistical tests. 42 The green bars represent the confirmed factors, whereas the red bars indicate the rejected covariates of the target variable examined in the study (Figure 1).
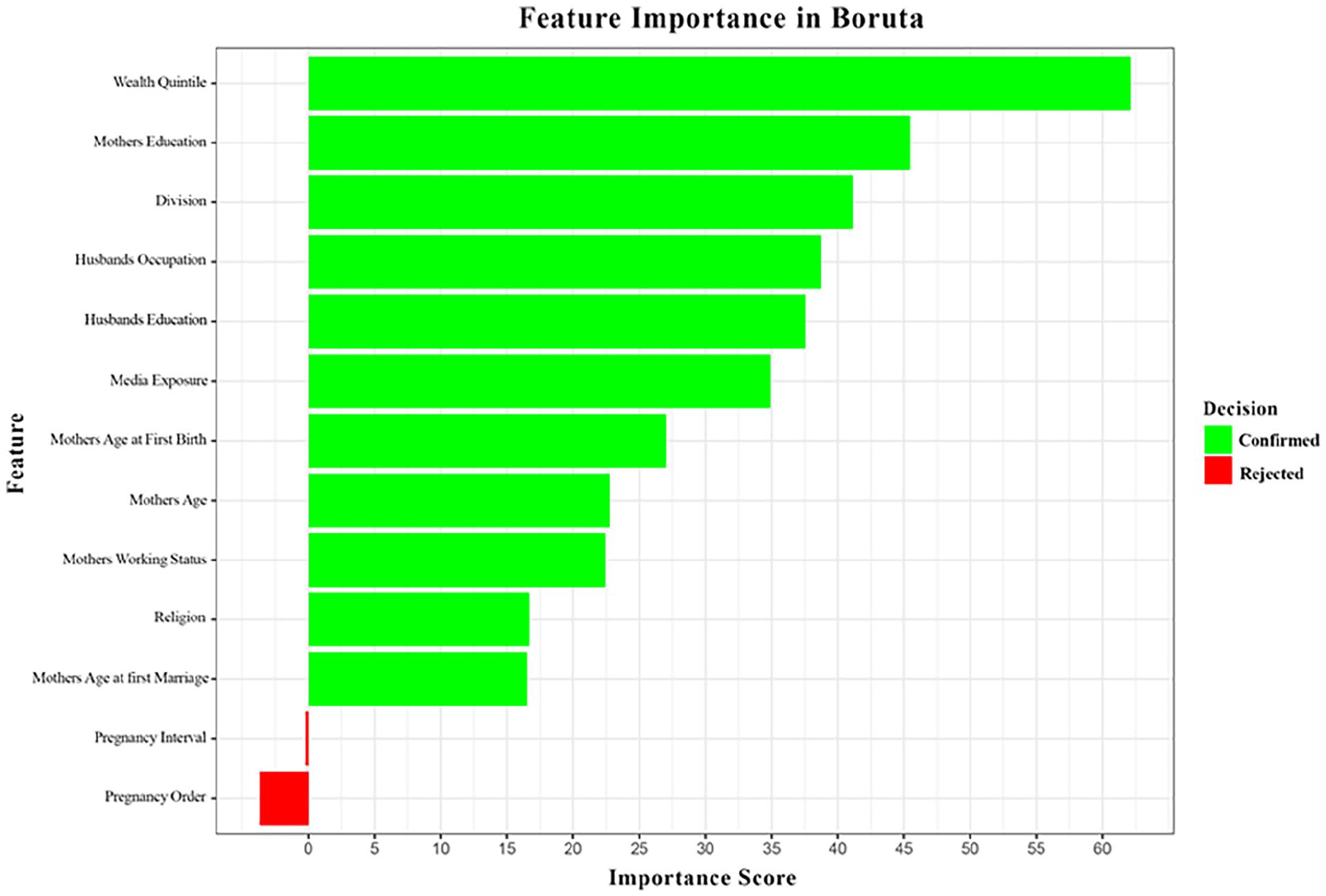
Covariate selection using the Boruta algorithm.
The Boruta algorithm identifies important features by evaluating their importance scores against randomly permuted shadow features using a Random Forest model. Features that consistently outperform the shadow features are ranked as important, whereas weaker ones are eliminated. The Boruta algorithm indicated that wealth quintile, mother’s education, division, husband’s occupation, husband’s education, media exposure, mother’s age at first birth, mother’s age, mother’s working status, religion, and mother’s age at first marriage are the important determinants, whereas preceding pregnancy interval and pregnancy order may be considered unimportant covariates of CS in urban mothers in this study (Figure 1).
The forest plot presented in Figure 2 visualizes ORs with a 95% CI for sociodemographic factors related to CS in urban mothers. As can be observed in the forest plot above, the higher odds of CS deliveries as the mother’s age at first birth increased, except for findings exhibited for ages between 35 and 49 years. Also, the odds of CS deliveries are lower for mothers aged 20–24 and 35–49 compared to mothers aged 15–19, with exceptional findings exhibited for ages between 25 and 34 years. This indicates that older mothers are less likely to have CS deliveries. Mother’s educational attainment is positively correlated; higher education shows an increase in odds compared to none. Wealth and CS delivery are significantly positively correlated; the OR is significantly increased for the richer and richest compared to the poorest. Media exposure and religions other than Islam are correlated with moderately higher odds, although CIs indicate more variability for the religion. Husband’s educational attainment indicated a moderate negative association, whereas working status exhibited higher odds, especially among business persons and service holders. A significant variation in ORs was observed in different divisions of Bangladesh. Findings depict that Dhaka, Mymensingh, and Sylhet have a higher deviation in odds, which suggests that the likelihood of CS delivery in Bangladesh urban areas is substantially influenced by the divisions when tested.

Forest plot of odds ratios and 95% confidence intervals for selected variables.
The factors that have a highly significant influence on delivery by CS in Bangladeshi urban mothers are identified through the use of binary logistic regression as a multivariate analysis and presented in Table 2. CS delivery is significantly impacted by the age at first birth, working status, wealth quintile, media exposure, religion, division, and husband’s education. Findings revealed that the CS delivery is considerably affected by the mother’s current age. Women aged 35–49 years had a 41% decreased chance of CS birth compared to those aged 15–19 years (adjusted OR (AOR): 0.59, 95% CI: 0.40–0.87). The odds of undergoing CS were 67% and 215% higher for the age group 20–24 years (AOR: 1.67, 95% CI: 1.31–2.14) and 25–34 years (AOR: 3.15, 95% CI: 2.03–4.89), respectively, than the age group 15–19 years, who gave birth for the first time. Employed mothers are nearly half as likely to undergo CS delivery as their unemployed counterparts (AOR: 0.53, 95% CI: 0.43–0.65).
ORs of cesarean delivery by selected covariates among Bangladeshi urban mothers: results from multivariable logistic regression analysis.

AOR: adjusted odds ratio; CI: confidence interval; Ref.: reference category.
Higher-educated respondents were almost twice as likely to undergo a cesarean birth as illiterate respondents, according to the study (AOR: 1.89, 95% CI: 1.20–2.99). Moreover, family wealth is significantly associated with CS; families with the richer and richest quintile had 183% (AOR: 2.83, 95% CI: 1.88–4.26) and 379% (AOR: 4.79, 95% CI: 3.13–7.34) higher chances of undergo CS delivery over vaginal delivery, respectively, compared to their poorest counterparts. Mothers who are exposed to media were 54% (AOR: 1.54, 95% CI: 1.27–1.87) more likely to go for the surgical delivery option compared to those who were not. From the variable religion, it is determined that individuals who identify with other religions are nearly 2.5 times more likely to have a CS than Muslim women (AOR: 2.33, 95% CI: 1.60–3.38). Additionally, the education of husbands had a significant impact on the delivery of a child by CS. The findings indicated that husbands working as service holders had nearly twice the likelihood of delivering via CS than those who were not working (AOR: 1.89, 95% CI: 1.18–3.02). Furthermore, women residing in Sylhet and Chattogram have considerably lower odds of cesarean delivery (AOR of 0.23 and 0.50, respectively) than those in Barishal (Table 2).
Discussion
The WHO recommended in 2015 that 10%–15% is the ideal rate of CS deliveries; however, the 10%–15% threshold for CS has since been challenged.5,16 Surprisingly, as per this study, 52.37% of urban women undergo to go under the surgical delivery process, which was significantly higher than the WHO’s recommendation. The CS rate was reported at 43% among Bangladeshi urban women in 2018, 30 meaning an increase of more than 10% over the past few years. Among the division-based urban CS rates, Khulna (71.8%) was topping the list. Several maternal health programs are running in Bangladesh, which might be contributing to the rising population-based CS rates. 44 In this study, it is revealed that various sociodemographic factors, such as the mother’s age at first birth, both husband and mother’s educational attainment and employment status, wealth quintile, media exposure (newspaper, radio, TV), etc., were significant contributors to the prevalence of CS in urban areas. Surprisingly, the important clinical factors, such as preceding birth interval, multiple deliveries, or history of terminated pregnancy, did not show significance with CS and were rejected in the covariate selection using the Boruta algorithm. Moreover, wealth quintile outstripped other socioeconomic predictors; a similar pattern has been observed in a cross-sectional study conducted on six developing countries. 45
This study revealed that the rate of CS in urban areas increases significantly with the advancement of age in the mother’s first birth. Women aged between 20–24 and 25–34 years were 67% and 215% more likely to undergo CS delivery. Previous studies conducted on CS deliveries also support these findings.46 –50 This trend may indicate that health considerations for slightly older mothers have increased, potentially as a result of the higher risk factors associated with maternal age. It may also reflect the mother’s preferences, as well as, biological challenges associated with delayed childbearing, such as the position of the child (position and presentation of the fetus in the womb, head-down position is ideal for vaginal delivery, whereas feet or buttocks first often require CS), diabetes, hypertension, and pre-eclampsia. 47 However, mothers whose current age was more than 35 years had 41% lower odds of CS, which contrasts with a previous study. 48 This contrast might be explained by factors such as prior childbearing experience or providers’ cautions about the surgical risks at older ages. However, these are possible explanations, and further study might be necessary to establish this association. Interestingly, highly educated mothers were more likely to undergo CS delivery. This trend might be due to educated mothers’ socioeconomic status, greater access to healthcare, and increased urbanization. This is aligned with a previous investigation in Turkey, 51 where the mother’s education level affected the prevalence of CS delivery. Also, in past years, Bangladesh has significantly improved the facilities of female education. 51 Opposite trends were observed in Brazil 51 and Scandinavia. 50 Surprisingly, mothers whose husbands were educated to the secondary level or higher were less likely to undergo the CS delivery option. One possible explanation for this is that educated husbands are more concerned about childbirth options and risks of undergoing surgical procedures, which discourages their wives from pursuing CS deliveries by emphasizing medical necessity. However, a previous study contrasts this finding 30 and might require more investigation.
Regarding the working status of mothers, working women had lower chances of using CS delivery. This might be because working women get less time to get institutional suggestions, health-seeking behaviors, and less antenatal care visits.52,53 Previous studies supported this finding.54,55 The wealth quintile was found to be another significant socioeconomic factor for CS delivery in this study. The prevalence of CS delivery rises with the rise of family wealth; richer and richest families appear to be highly significant. Better financial stability supports the expenses during CS delivery and wealthier families can access healthcare facilities like antenatal visits, and health checkups more frequently than poor families. 40 Previous studies reported similar findings.56,57 Like some previous studies, this study also found that mothers who were exposed to media such as newspapers, radio, and television were 54% more likely to use the surgical method of delivering babies. 55 This association could be due to the influence of media to increase health awareness and delivery options.32,45 This study also revealed that a mother’s religion had a huge impact on the CS delivery option; religions other than Muslim had shown a 133% higher prevalence of CS. This is also aligned with previous research conducted in Nigeria 58 and Tanzania. 59 This might have occurred due to different cultural norms and beliefs across the religious groups. Moreover, women’s husbands who were working as service providers are 89% more likely to suggest their wives undergo surgical delivery options compared to those whose husbands were not working. A prior study conducted on Bangladeshi urban and rural women supported this finding. 30 This might be due to the higher financial stability and greater access to the healthcare facility compared to the others. Mothers residing in the urban were of Chattogram and Sylhet divisions are significantly associated with and less likely to undergo the CS delivery option compared to the Barishal division, but Khulna, Rajshahi, and Rangpur divisions exhibited a greater likelihood of undergo CS delivery over normal delivery. This might be because of the heterogeneity of sociodemographic status and educational attainment in these regions. This is also in line with a prior study. 60
Strength, limitations, and further study
The key strength of this study is using the freshly cooked and nationally representative BDHS-2022 dataset. It is notable that determinants of CS delivery in urban areas had not been investigated using the BDHS-2022 dataset prior to this study. This study also encountered limitations due to some missing values in the dataset, which sometimes reduced the sample size and restricted the consideration of variables that might contribute to CS. Also, as there are differences in predictive factors between this and prior studies conducted on CS, there might be a few inconsistencies with this analysis. In a future study, a comparison between rural and urban areas may be explored.
Conclusion
The prevalence of CS delivery is 52.37%, which is way more than the ideal rate of 15% recommended by the WHO. Sociodemographic factors like wealth quintile, age, mother’s education and working status, husband’s education and working status, media exposure, religion, and division play a significant role in CS delivery in urban areas. Among them, wealth quintile, age at first birth, working status, and media exposure were the top risk factors. Pregnancy interval and pregnancy order were identified as unimportant variables by the Boruta algorithm. To keep the CS delivery within the recommended rate by WHO, a national-level comprehensive guideline should be developed by the policymakers to ensure CS is performed only when medically needed. To increase awareness and knowledge among educated and financially stable urban women, particularly first time and older mothers, on the pros and cons of CS delivery versus vaginal delivery. Newspapers, radio, and television can play a vital role in increasing awareness, health programs should be organized to promote vaginal delivery and to countering the perception of CS. Disparities in regions and socioeconomic status must be addressed by expanding maternal healthcare services and ensuring CS deliveries are completely medically necessary and not financially driven. Involving mothers and their partners in decision-making can reduce the need for CS, whereas antenatal services must be strengthened to reduce medical complications leading to CS delivery. The authors believe that, implementation of comprehensive and evidence-based strategies by the government from these key findings along with monitoring and hospital accountability can mitigate CS and increasing natural vaginal deliveries.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251356806 – Supplemental material for Determinants of cesarean section in urban areas of Bangladesh: Insights from the Bangladesh Demographic and Health Survey-2022
Supplemental material, sj-docx-1-whe-10.1177_17455057251356806 for Determinants of cesarean section in urban areas of Bangladesh: Insights from the Bangladesh Demographic and Health Survey-2022 by Md. Sazzad Hossan Sujon, Imran Hossain Sumon, Junayed Ahmmad, Md. Shahanewaj Asif and Md. Moyazzem Hossain in Women’s Health
Footnotes
Acknowledgements
We acknowledge ICF International, Rockville, MD, United States, for equipping us with the Bangladesh DHS dataset for this study. We are thankful to the editor and anonymous reviewers for providing insightful comments and feedback that helped to improve the quality and readability of the article.
Ethical considerations
In this study, a publicly available BDHS dataset was used, which was controlled by the Ministry of Health and Family Welfare of the Bangladesh Government. As the data are anonymized and publicly available to use, so no ethical approval was needed for this research. However, the original BDHS was reviewed and approved by the Institutional Review Board (IRB) of ICF Macro in Calverton, United States, and the Bangladesh Medical Research Council (BMRC), the national ethical committee in Bangladesh.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.