
Abstract
Background:
In Rwanda, legally induced termination of pregnancy (ToP) is permitted under specific conditions such as cases of rape, incest, being a minor, forced marriage or health-related issues.
Objectives:
To explore post-ToP mental health outcomes, the circumstances under which women seek ToP services and investigates their relationship with the presence or absence of psychological support.
Design:
A quantitative approach using a cross-sectional design was used for this study.
Methods:
Data collection recruited 305 women and girls who sought ToP services at eleven selected health facilities in Rwanda from June to August 2022. Life satisfaction, self-esteem, anxiety, and depression/grief were the outcome measures and were measured using the standardized tools. Binary logistic regression (adjusted odds ratios) was used to assess how the circumstances of seeking ToP and the presence or the absence of psychological support predicted mental health outcomes.
Results:
The findings indicate that the primary reasons for seeking ToP services include rape, pressure from a partner and fear of missing educational opportunities. There was a strong association between circumstances such as rape and partner pressure with negative mental health outcomes. The study also revealed that only a small proportion of women who received post-ToP psychological support from family, community or healthcare providers, while the majority did not. The absence of psychological support was significantly linked to an increased likelihood of low self-esteem, anxiety, depression, and dissatisfaction with life.
Conclusion:
The circumstances under which women seek ToP services significantly impact their mental health post service provision. The findings underscore the critical role of post-ToP support in mitigating negative psychological outcomes. Hospitals should screen depression/grief and offer psychological care support for women undergoing ToP.
Keywords
Introduction
Abortion is defined as termination of pregnancy (ToP) by removal or expulsion of an embryo or fetus prior to 20 weeks. 1 Above these weeks, normally known as the second trimester of the pregnancy, a ToP is generally performed for fetal anomaly. 2 When deliberate steps are taken to end a pregnancy, it is called an induced abortion, which may be safe or unsafe. Abortion is safe when carried out using a method recommended by the World Health Organization (WHO), appropriate to the pregnancy duration, and by someone with the necessary skills and this is legally induced abortion. 3 ToP or illegally induced abortion is defined as a procedure to terminate an unintended pregnancy that is performed by an individual lacking the necessary skills and/or in an environment that does not conform to the minimum medical standards or both, which has adverse outcomes. 4 Worldwide, around 56 million abortions are performed each year and about 45% of these abortions are illegal, which are likely to result in higher rates of adverse outcomes.
Lack of access to ToP has high impacts on health: Women with unwanted pregnancies who have limited access to ToP services opt for illegal ToP, which require medical attention. Unsafe abortion can contribute to 4.7%–13.3% of maternal deaths each year all over the world. 5 Further, of the many unsafe abortions that take place worldwide each year, almost all those recorded in developing countries resulted from unintended pregnancies. 6 Countries that restrict abortion record a high number of unsafe abortions, with developing countries bearing a disproportionate burden of 97% of the total cases. 6 Asia, Latin America, and Africa have 3/4 of the total unsafe abortions (3 out of 4 abortions). Africa alone accounts for almost half of all abortions necessitating medical attention. 1 Unsafe or ToP have an impact on women’s psychology.
The WHO 3 list of essential health care services includes ToP or comprehensive abortion treatment. Despite this publication, some countries still consider ToP to be an abnormal and criminal act. This stigma towards abortion services is associated with a lack of access to safe, affordable, timely, and respectful abortion treatment. Moreover, a lack of access to services affects women’s physical and mental health throughout their lives. 7 Mental health problems are notified in some women since their conception and may present different behaviors in both prenatal and postnatal periods. In prenatal depression, women present behaviors such as low mood, loss of interest, or pleasure in previously enjoyed activities, fatigue, hopelessness, restlessness, changes in appetite, alterations in sleep habits, difficulty concentrating, and thoughts of self-harm, social isolation, and fear of attachment issues. 8 Factors underlying antenatal depression, include lack of support from society and family, past history or family history of mental illnesses, lack of employment, childhood abuse, adverse life events, and intimate partner violence. Literature reveals that the majority of postnatal depression cases are preceded by antenatal depression and those who suffer from depression experience persistent feelings of despair and hopelessness and lose interest in activities that they once enjoyed; thus, reducing quality of life and overall well-being among women. 9 Maternal, prenatal, and postnatal psychological distress, such as anxiety and depression, can negatively affect mother–infant interactions. Since anxiety and depression are the common symptoms for women who have had an abortion, the emotional burden of an abortion decision can contribute to increased anxiety and depression, which in turn, can affect maternal well-being during pregnancy and after childbirth. 10 Feeling guilt and grief, stigma and judgement, mental health struggle, and lack of support are also commonly noted in both cases, that is, abortion and antenatal and postnatal mental health condition.11 –13
Additionally, literature stipulates controversies regarding an association between abortion and mental health. The first school of thought suggests that abortion contributes to mental health risks, while the second holds that the correlation between mental health and abortion is due to preexisting risk factors. 14 Abortion and mental health proponents who promote access to ToP and mental health services believe in the mental health risks from abortion, whereas abortion and mental health minimalists insist on preexisting risks as the primary cause for the association with more negative outcomes. Nevertheless, both groups agree on the fact that abortion, including ToP, is associated with increased rates of mental health outcomes and, relatedly, the WHO 2022 list of essential health care services during ToP service provision suggests that mental health increases after an abortion 15 for women in reproductive age. The psychological health of women after an abortion is one of the important components to consider when it comes to evaluating whether they are mentally healthy or not. The psychological effects of abortion among female clients have been the subject of scientific inquiry and public debate. 16 Conditions leading to abortion are, in turn, affected by numerous factors, that is, the socioeconomic conditions, the availability of ToP services, and the stigma surrounding abortion among women and girls seeking services. 17 Consequently, stigma related to seeking or provision of abortion is increasingly being recognized as having a negative impact on the physical and psychological health of female clients who seek abortion services. 18 As noted in the Reardon review, 19 the APA, 20 Task Force on Mental Health and Abortion report, both identified numerous risk factors, such as ambivalence, attachment to the pregnancy and feeling pressured to choose abortion. Further, the same report revealed a number of behaviors that women often present after an abortion which have roots from how pregnancy was perceived. Systemic, social, and personal factors are the precursors to unintended pregnancy and hence, place women at risk for having abortions and/or predispose them to experience mental health problems, regardless of pregnancy and its resolutions. The common behaviors after an abortion include low perceived ability to cope with the abortion prior to its occurrence, low perceived social support and low self-esteem which predicted more negative postabortion responses 20 whether is legal or illegal.
The impact of these factors to women are discussed in the literature. For example, a study conducted in the United States of America about the effects of pressure to abort on women’s emotional responses and mental health notes that this pressure caused more disruption of daily life, more frequent feelings of loss, grief or sadness about the abortion, and so much more. 21 Pressure from family or community members to abort can lead to increased levels of anxiety, depression, and emotional distress, significantly impacting women’s mental health and overall well-being.
Different authors have reported that ToP while legally permitted and individually requested, does not eliminate the possibility of postabortion grief.15,17,18,22,23 Moreover, the presence or the absence of grief may differ from country to country depending on various factors, including psychological support (social, family, partner, and healthcare provider (HCP)). Psychological support among women and girls is still limited, and this may lead to negative mental health outcomes. 24 Most women report having an abortion because they are not ready to care for a child (or another child), they have financial constraints, they have a responsibility to others (especially concerns related to caring for other children), a desire to avoid single parenthood, relationship problems, and they feel too young or immature to raise a child 25 ; while other pregnancies are terminated because they are a consequence of rape or incest. In another study, 60% of women with a history of abortion reported high degrees of pressure to abort and stated that they would have preferred to give birth if they had received more support from others or had more financial security. 24
However, women’s psychological experience of abortion is not uniform; rather, it varies as a function of their personal characteristics, events that led up to the pregnancy, and the circumstances of their lives and relationships at the time that a decision to terminate the pregnancy is made. 26 A teenager who terminates her first pregnancy may experience psychological effects different from those of an adult woman who terminates a pregnancy after giving birth to several children. 27 This difference is an important factor to keep in mind when considering how best to study and explain associations between abortion and mental health problems. This study examined postabortion mental health outcomes of life satisfaction, self-esteem, anxiety, and depression/grief and explores their relationship with the presence or absence of postabortion support. It also examined circumstances under which women and girls seek abortion services.
Literature reviews note the importance of including psychological support in the legally induced abortion service provision to women and girls, encouraging healthcare professionals to be ready to serve the purpose. 4 However, more is needed to be known regarding psychological support in women receiving ToP, as well as the relationship between psychological care and mental health post service provision in Rwanda. While it is of paramount to include psychological support to promote mental health outcomes after the service provision for women who have had ToP, this study provides the roadmap, on how to test the association between psychological support and mental health outcomes on women post ToP service provision to improve their mental health outcomes. This study has the potential to show the importance of improving mental health outcomes, inform policy, raise public awareness, and enhance the overall care provided to women seeking ToP services in Rwanda.
Materials and methods
The study design
This study used a descriptive cross-section study design to describe demographic characteristics, psychological attributes related to ToP, and mental health outcomes (life satisfaction, self-esteem, grief/depression, and anxiety) among women and young girls who had received ToP services.
Study setting and population
Rwanda is divided into four provinces, and Kigali City can be considered as the fifth. The study randomly selected two district hospitals from each province (Nyagatare, Nyamata, Nyabihu, Rubavu, Musanze, Shyira, Nyanza, and Kabutare Hospitals) and three district hospitals from Kigali city (Muhima, Kacyiru, and Kibagabaga Hospitals), totaling 11 district hospitals. The study population consisted of women and girls who received ToP services from these selected hospitals. In Rwanda, abortion is still illegal unless is secured under five criteria: (1) a pregnant person is pregnant as a result from rape, (2) when the pregnant person is pregnant as a result from incest up to the second degree, (3) the pregnant person is a child (less than 16 years old), (4) the person having abortion had become pregnant after being subjected to a forced marriage, and (5) the pregnancy puts at risk the health of the pregnant person or of the foetus. 28 In addition, the law allows abortions for the foregoing reasons up to 13 weeks gestation. However, abortion through 22 weeks gestation is also allowed for therapeutic purposes by which the pregnancy is seen to harm the life of the mother and/or of the fetus.
Sample size
The sample size for this study was calculated using OpenEpi software, version 3.03. It was developed by AG Dean KM Sullivan and MM Soe. It was estimated that 7020 females had received the service of ToP since 2018. As the hypothesized percentage frequency of the outcome in the population (p) was unknown, a value of 50% ± 5% was used. The study employed confidence limits of 5% and a design effect of 0.7. Based on these parameters, the total calculated sample size was 255 as the minimum required. As the minimum sample size was 255, we aimed at including all women provided with the ToP services from the hospital registry, responded positively, and the total participants were 305.
Inclusion and exclusion criteria
Women at any age who sought ToP services from 2018 in the public health facilities were included in this study, if responded to the call and will to participate and signed consent (both on paper and from google link). Exclusion was the one who cannot be reached due to not registering her contact in the medical register, did not respond to the phone call three times of trial, and refused to participate.
Recruitment and data collection
The recruitment process took place from June to July 2022. At each study site (district hospitals), we requested the hospital administration to identify a gatekeeper. The gatekeeper was any staff member involved in providing ToP services at the facility. The study team met with each identified gatekeeper to explain the study’s purpose and procedures. Following this, we asked the gatekeepers to contact potential participants using existing hospital records. These records included contact information for women and girls who had received ToP services and data collection occurred from August 9 to 26, 2022, at the selected health facilities.
A total of 678 women and girls were listed in the hospitals’ registers. Initially, the aim was to contact approximately 255 participants. However, due to challenges such as unreachable phone numbers and refusal to participate, gatekeepers eventually attempted to contact all 678 individuals. Of these, 305 responded to the call, agreed to participate, and scheduled a meeting with the researchers. Twelve had incomplete phone numbers and could not be reached. A further of 275, did not answer after 3 call attempts, and 86 declined participations, with no appointments made.
On the day of data collection, the gatekeeper introduced the researcher to the participant in a private setting and then left them alone. The researcher explained the study procedures, including the use of Google Forms and confidentiality measures. After providing informed consent, both via a signed form and digitally through the Google Form, participants completed a self-administered survey using a tablet with a pregenerated link. A data collector was present nearby to assist with any questions. The data collection team consisted of MS, who had extensive experience interviewing women in this research area and was knowledgeable in gender issues, legal aspects, and mental health; GN, with a background in quantitative data collection and mental health; and PU, a mental health nurse and university educator with experience in both qualitative and quantitative data collection, including interviews.
Tools for data collection
The survey used for data collection was developed based on the existing validated tools to measure four mental health outcomes: life satisfaction, 29 self-esteem, 30 anxiety, 31 and depression/grief. 32 The internal consistency of the instruments was assessed using Cronbach’s Alpha. The overall Cronbach’s Alpha value for the scale of life satisfaction (α = 0.87), self-efficacy (α = 0.71), anxiety (α = 0.95), and depression/grief (α = 0.92) indicating good internal reliability. Table 1 provides an overview of tools for mental health outcome measures.
Mental health outcome measures, their interpretation, and respective authors.

Study analysis
The study used Stata version 18.5 to analyze data. The software is developed and maintained by StataCorp LLC, a company specializing in statistical software for professional researchers. Data were collected using Google Forms and downloaded into an Excel sheet that was imported into Stata. Preliminary data cleaning was conducted to ensure the accuracy and consistency of the dataset before analysis. This involved checking for missing values, outliers, and inconsistencies, which were addressed by imputation or exclusion as appropriate, such as variables with missing values >50%. All analyses were performed using Stata software version 18.5, ensuring that the statistical methods applied were robust and suitable for the dataset. The data analysis began with descriptive statistics to summarize the sociodemographic characteristics of the participants, including age, marital status, profession, education level, and economic status. Following this, bivariate analysis was conducted using the Chi-square test of independence to explore associations between predictor variables (age, marital status, profession, education, transferred or not, transferred by, economic status, reason for abortion, pressure to seek abortion, pressure from who, and postabortion psychological support) and outcome variables (self-esteem, anxiety, depression, and satisfaction). The transfer was put into consideration as it may impact women’s needs. The fact that women do not receive ToP service at the lower level (closer to them, which is the health center), can be a source of anxiety as it requires additional costs in terms of money and time. Variables that showed significant associations (p-value < 0.05) in the Chi-square test were then included in a bivariate logistic regression to calculate crude odds ratios (ORs) and their corresponding 95% confidence intervals (CIs). This helped in understanding the strength of the association between each predictor and the outcome variables. Subsequently, a multivariate logistic regression analysis was performed to identify independent predictors while adjusting for potential confounders. Multicollinearity among the predictor variables was assessed using the variance inflation factor (VIF), with a VIF value above 10 indicating significant multicollinearity, but none was detected in exploratory checking. The final model reported adjusted odds ratios (AORs), 95% CIs, and p-values, highlighting the predictors that remained statistically significant after controlling for other factors.
Operational definition of variables
Dependent variables
The dependent variables in this study were life satisfaction, self-esteem, depression, and anxiety following ToP service provision. To be used in a binary logistic regression, self-esteem was dichotomized into two categories: low self-esteem (1) and normal self-esteem (0). Anxiety was categorized into two groups: low to no anxiety (0) and concerning anxiety (1). Grief or depression following the abortion was dichotomized into no depression (0) and depression (1). Lastly, life satisfaction was divided into two categories: dissatisfied (1) and satisfied (0). All these outcome variables were analyzed as dichotomous variables.
Independent variables
The variables of postabortion support, reasons for abortion, and marital status were reduced into two categories each. Educational level and economic status were reduced to three categories, while the variable of pressure to have an abortion was categorized into four groups.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist of cross-sectional studies. 34
Study findings
The study was guided by the following research objectives: to identify the circumstances under which the decision for a ToP was made, to assess the use of available psychological support (social, family, partner, and HCP), and to determine the status of mental health outcomes (life satisfaction, self-esteem, grief, depression, and anxiety) in relation to the presence or the absence of psychological support among women who received ToP services.
Sociodemographic characteristics of the participants (N = 305)
Table 2 presents the sociodemographic characteristics of the participants. The majority of participants were aged between 16 and 24 (n = 169, 55.4%). Most participants were single (n = 194, 63.6%), followed by married individuals (n = 98, 32.1%). In terms of education level, secondary education was the majority, attained by 58.4% of participants (n = 178), followed by tertiary education (n = 82, 26.9%). Regarding economic status, the largest group fell into Category B, representing 51.5% (n = 157) of the sample. Furthermore, most participants were in the Ubudehe category D. The Ubudehe category is a social stratification program determined by household income. In Rwanda, those with less income are classified in Ubudehe category D, and as income increases, a person is classified in categories C to B to A, with A being the wealthier group. Categories C and D represent a significant percentage of the Rwandan population. 35
Sociodemographic characteristics of the participants.

Table 3 indicates that 83.3% (n = 257) of participants reported rape as the reason for seeking an abortion, while 31.8% (n = 97) experienced external pressure to seek abortion services. However, the majority of participants reported internal pressures, such as fear of missing out on education (n = 98, 32.1%). Additionally, the findings show that most participants did not receive postabortion psychological support (n = 279, 88.5%). See Table 3.
Circumstances under which termination of pregnancy was made.

Figure 1 describes postabortion psychological outcomes. The findings on these outcome variables indicate that low self-esteem was the most prevalent among participants, affecting 78.7% (n = 240) of the sample. Depression was also common, experienced by 62.6% (n = 191) of participants. Anxiety was reported by 54.7% (n = 167), while 42% (n = 128) of participants expressed dissatisfaction with life (see Figure 1).

Description of postabortion outcomes.
Chi-square test of the predictors and outcome variables
To predict postabortion outcomes in terms of life satisfaction, self-esteem, anxiety, and depression, we employed a bivariate logistic regression model (AORs). Prior to running the logistic regression, we conducted Chi-square tests to examine the relationships between predictor (independent) variables and outcome (dependent) variables.
The Chi-square analysis revealed that age is significantly associated with self-esteem, with individuals aged 25 and older being more likely to experience low self-esteem (n = 118, 86.8%, p = 0.002). Marital status also played a key role, as married participants predominantly reported low self-esteem (n = 90, 91.8%, p = 0.001). The method of transfer was significant, especially among those transferred by a hospital, where 98.2% (n = 54, p < 0.001) exhibited low self-esteem. The profession was another important factor, with public sector workers more likely to report low self-esteem (n = 17, 89.5%, p = 0.001). Educational level showed significance, as those with tertiary education had a high rate of low self-esteem (n = 76, 92.7%, p < 0.001). Economic status, particularly in Category D, was significantly associated with low self-esteem (n = 14, 100%, p = 0.013). Regarding reasons for abortion, individuals who cited rape as the reason for seeking a ToP were significantly more likely to experience low self-esteem (n = 217, 84.4%, p < 0.001). Pressure to seek abortion services, especially from partners, was also a significant factor, with 95% (n = 57, p < 0.001) reporting low self-esteem. Finally, the presence of postabortion support or lack of it was a determinant of self-esteem, as those who did not receive any psychological support had the highest rates of low self-esteem (n = 235, 87%, p < 0.001).
The Chi-square analysis of predictors of anxiety outcomes revealed several significant variables. Age was strongly associated with anxiety, with participants aged 25 and older being more likely to experience anxiety (n = 112, 82.4%, p < 0.001). Marital status was another significant factor: married individuals had a high prevalence of anxiety (n = 81, 82.7%, p < 0.001), and all divorced participants reported anxiety (n = 13, 100%, p < 0.001). Professionally, public sector workers had a higher likelihood of anxiety (n = 16, 84.2%, p = 0.022). Education level was also a significant predictor, with those holding tertiary education having a higher prevalence of anxiety (n = 63, 76.8%, p < 0.001). Economic status showed a significant association, particularly in Category D, where 92.9% (n = 13, p < 0.001) of participants experienced anxiety. Pressure to seek abortion services was another significant predictor, with participants who experienced pressure more likely to report anxiety (n = 62, 63.9%, p = 0.028). Pressure from partners (n = 52, 86.7%, p < 0.001) and societal pressure (n = 7, 87.5%, p < 0.001) were both strongly linked to anxiety.
The Chi-square analysis of predictors of depression outcomes revealed several significant variables. Age was strongly associated with depression, with participants aged 25 and older more likely to be depressed (n = 118, 86.8%, p < 0.001). Marital status was another key factor, as married individuals were significantly more likely to experience depression (n = 90, 91.8%, p < 0.001), while all divorced participants reported depression (n = 13, 100%, p < 0.001). Participants who were not transferred to the hospital were more likely to be depressed (n = 64, 77.1%, p = 0.001), while those transferred by a hospital also showed a significant association with depression (n = 37, 67.3%, p < 0.001). Professionally, all public sector workers in the study experienced depression (n = 19, 100%, p = 0.002). Education level was a significant predictor, with participants having tertiary education showing a higher prevalence of depression (n = 74, 90.2%, p < 0.001). Economic status was also significantly associated with depression, particularly in Category D, where 92.9% (n = 13, p < 0.001) experienced depression. The reason for abortion was another significant predictor, especially for participants who cited rape (n = 172, 66.9%, p = 0.016). Pressure from a partner was strongly linked to depression (n = 57, 95%, p < 0.001), as was societal pressure (n = 8, 100%, p < 0.001). Lastly, the type of postabortion support received was crucial, with those who did not receive support being more likely to experience depression (n = 175, 64.8%, p = 0.038).
Additionally, the Chi-square analysis of predictors of postabortion life satisfaction revealed several significant associations. Age was a key factor, with participants aged 16–24 being more likely to report satisfaction (n = 107, 63.3%, p = 0.037) compared to those aged 25 and older (n = 70, 51.5%). Education level significantly influenced life satisfaction, with those having tertiary education being more satisfied (n = 61, 74.4%, p = 0.006). Pressure from partners was strongly associated with satisfaction (n = 48, 80%, p < 0.001), as was the fear of missing education (n = 75, 76.5%, p < 0.001).
Adjusted multivariate logistic regression model of the socioeconomic predictors of psychological outcomes of ToP
As shown in the Tables 4 and 5, in the analysis of factors associated with low self-esteem, several variables were found to be significant predictors of postabortion self-esteem. Economic status plays a notable role, with individuals in Category B showing higher odds of experiencing low self-esteem compared to economic status A (AoR = 3.73, 95% CI: 1.18–11.72, p = 0.024). Additionally, those who had an abortion due to rape were more than four times more likely to report low self-esteem compared to those who had an abortion because of being a child (AoR = 4.02, 95% CI: 1.19–13.58, p = 0.025). Furthermore, the presence of pressure to seek abortion services is associated with increased odds of low self-esteem (AoR = 6.63, 95% CI: 1.10–39.68, p = 0.038), and receiving no support postabortion is strongly linked with low self-esteem compared to those who receive it (AoR = 15.47, 95% CI: 2.79–85.64, p = 0.002).
Multilogistic regression model of the socioeconomic predictors of psychological outcomes of termination of pregnancy.

AOR: adjusted odds ratio; Ref: reference sub-group variable.
Bold indicates significantly associated.
Multilogistic regression model of the primary predictors of psychological outcomes of termination of pregnancy.
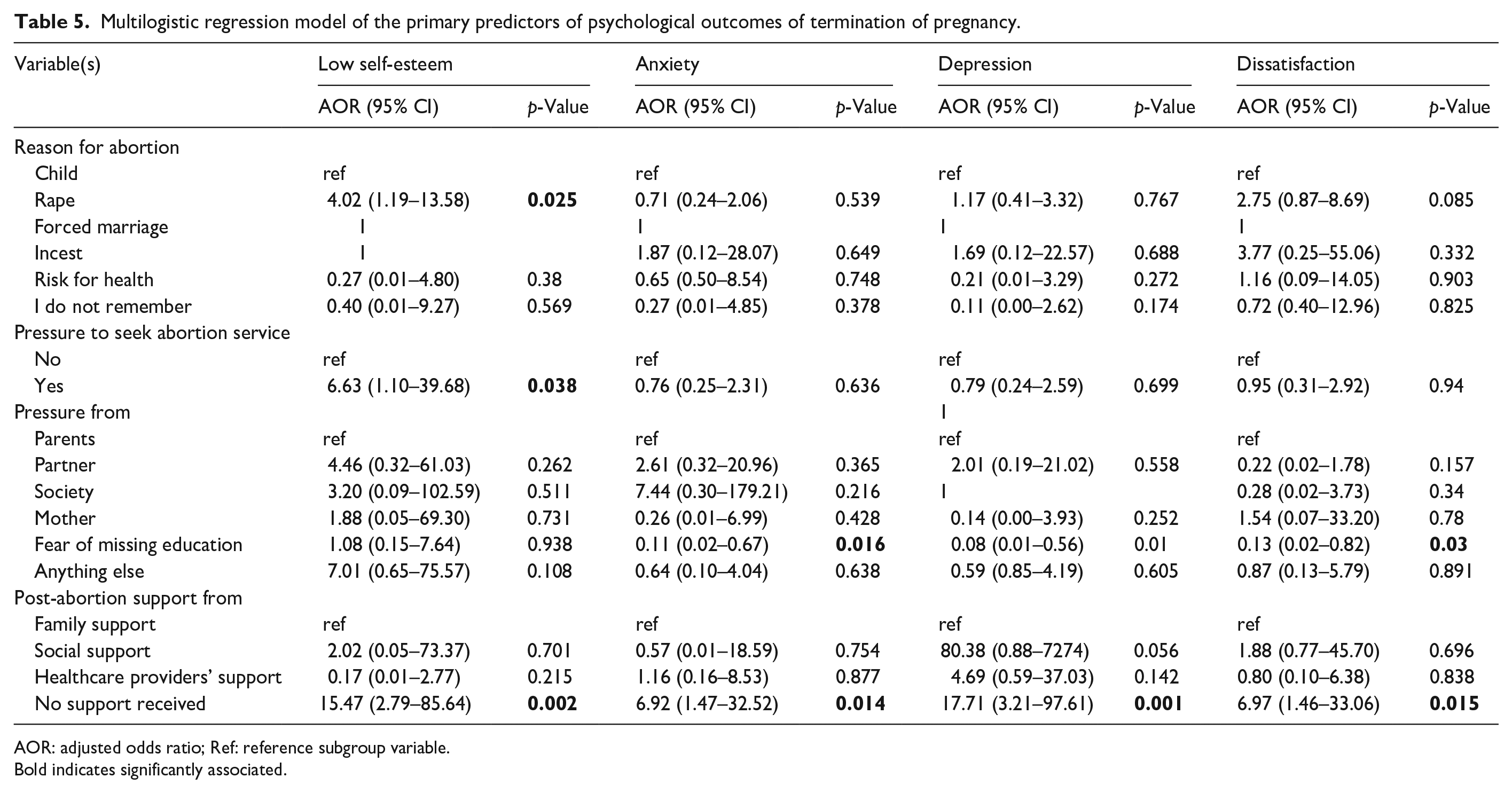
AOR: adjusted odds ratio; Ref: reference subgroup variable.
Bold indicates significantly associated.
For anxiety, significant predictors include the type of facility where the abortion was performed. Those transferred by the health centers have reduced odds of anxiety (AOR = 0.33, 95% CI: 0.11–0.96, p = 0.043). Economic status also shows significant effects, with individuals in wealth-income category C experiencing higher odds of anxiety (AOR = 5.50, 95% CI: 1.71–17.67, p = 0.004). Fear of missing education is another important factor, where individuals reporting this fear have significantly lower odds of anxiety (AOR = 0.11, 95% CI: 0.02–0.67, p = 0.016). Additionally, lack of postabortion support is associated with increased anxiety (AOR = 6.92, 95% CI: 1.47–32.52, p = 0.014).
Depression is significantly associated with several factors. Individuals in category C of economic status have much higher odds of depression (AOR = 6.06, 95% CI: 1.84–20.06, p = 0.003). The fear of missing education is also a critical factor, with those who experienced this fear having lower odds of depression (AOR = 0.08, 95% CI: 0.01–0.56, p = 0.010). Moreover, luck of support postabortion is strongly related to higher depression levels (AOR = 17.71, 95% CI: 3.21–97.61, p = 0.001).
Dissatisfaction with the abortion experience is significantly impacted by economic status, particularly for those in category C (AOR = 3.93, 95% CI: 1.31–11.72, p = 0.014). Fear of missing education also significantly lowers life dissatisfaction by 0.13 times compared to a reference group of those who seek an abortion under the pressure of their parent (AOR = 0.13, 95% CI: 0.02–0.82, p = 0.030). Additionally, a lack of postabortion support correlates with life dissatisfaction 6.97 times compared to those with any postabortion psychological support (AOR = 6.97, 95% CI: 1.46–33.06, p = 0.015; see Tables 4 and 5).
Discussion
This study aimed to explore the circumstances under which women decided to undergo ToP, assess the availability of postabortion psychological support, and examine mental health outcomes (including life satisfaction, self-esteem, anxiety, and depression) in relation to the psychological support provided to women who received ToP services.
Regarding the circumstances leading to the decision to have a ToP, the results indicate that both married and unmarried women of various ages, socioeconomic backgrounds, and education levels sought these services. The findings revealed that women who wanted ToP services were transferred from health to another health institution. This situation indicates that some health institutions do not offer ToP services. The previous study revealed that religious-based hospitals do not offer ToP services, and health centers are not yet allowed to provide ToP services in Rwanda. 4 While this situation is related to the nature of those health institutions, the delay in service and associated expense and inconvenience related to transfers add risks to the health outcomes of those seeking a ToP service is notified. 19 Moreover, the findings also reveal that women pursued ToP for different reasons, with the majority in this study doing so due to pregnancy resulting from rape or concerns about fear of disrupting their education. 36 Rape was a statistically significant predictor of low self-esteem, with an OR of 4.02 and a p-value of 0.025. However, the results of the logistic regression model should be interpreted with caution. For instance, the variable reason for abortion includes six categories, some of which have very few outcome events. This may have contributed to unstable estimates and a wide CI. For example, an OR of 3.77 suggests a potential positive association, but the wide 95% CI (0.25–55.06) and nonsignificant p-value (0.332) indicate a high level of uncertainty and insufficient statistical evidence to support a meaningful effect.
While each reason for seeking an abortion may necessitate postabortion psychological support, certain reasons, such as rape, may require particular attention. For example, deciding to terminate a pregnancy resulting from rape may provide relief, but it raises questions about the adequacy of the services provided. 37 Previous studies have shown that rape is associated with external and internal stigma, feelings of blame and shame, psychological distress, and even hazardous drinking.36 –38 In this context, it is evident that beyond the provision of ToP services, women also require comprehensive postabortion psychological support.
The findings from this study indicated that women received postabortion psychological support from family members, society, and HCPs. However, the majority of participants did not receive any psychological support after their abortion. Due to the scope of the study, we could not determine why only a few women received psychological support from HCPs, while others did not. Nevertheless, our results show that women who did not receive any psychological support had significantly higher odds of experiencing low self-esteem, anxiety, depression, and life dissatisfaction. While some studies have reported a link between abortion and mental health issues,4,13,27 others suggest that abortion is not the sole cause of mental health problems; rather, women who had an abortion often had preexisting mental health conditions compared to those who did not undergo an abortion. 28 Regardless of whether mental health issues developed after or were present before the abortion, research indicates that postabortion psychological support can help mitigate mental health challenges.19,22
Recommendations and future research
The findings showed that women who received postabortion psychological support experienced fewer mental health issues compared to those who did not receive any support. Therefore, psychological support should be an integral part of ToP services. Future research should investigate why some women received support while others did not. Additionally, studies should evaluate the quality and effectiveness of psychological support provided by both laypersons and healthcare professionals.
Strengths and limitations of the study
This study employed a rigorous approach, using valid and reliable tools to collect data. We have clearly outlined our methodology, including the analysis process, to facilitate replication. Furthermore, the study addresses an important but previously unexplored area regarding mental health outcomes following ToP in Rwanda. However, the study also has limitations. It relied on self-reported data and a cross-sectional study design, which limits the ability to determine cause and effect. Additionally, potential selection bias may exist as participants voluntarily enrolled in the study. During data collection, the participants who were registered in the hospital’s registry and do not have phone number as well as those who did not responded up to the third time of calling were automatically excluded; which constitutes a limitation to this study as our findings most likely represent an underestimation of the proportion of women reporting negative feelings since those who self-censure are, based on prior research, more likely to have more negative feelings than those who do agree to participate in the study.
Conclusion
This article presents findings on the circumstances under which women seek ToP services, the availability of psychological support following abortion, and the relationship between postabortion support and mental health outcomes. The primary reasons for seeking a ToP include rape, pressure from a partner, and fear of missing educational opportunities. The findings also highlighted a link between circumstances like rape and partner pressure with adverse mental health outcomes. The study revealed that only a small number of women received postabortion psychological support from family members, the community, or HCPs, while the majority did not. Furthermore, the absence of psychological support significantly increased the likelihood of developing low self-esteem, anxiety, depression, and dissatisfaction with life.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251348990 – Supplemental material for Psychological care and mental health outcomes in women receiving termination of pregnancy in Rwanda: A cross-sectional study
Supplemental material, sj-pdf-1-whe-10.1177_17455057251348990 for Psychological care and mental health outcomes in women receiving termination of pregnancy in Rwanda: A cross-sectional study by Marie Grace Sandra Musabwasoni, Gerard Nyiringango, Peace Uwambaye, Madeleine Mukeshimana, Eugene Ngoga, Thierry Claudien Uhawenimana, Priscile Musabirema, Gerard Kaberuka, Vincent Sezibera, Marie Klingberg-, Stephen Rulisa, Donatilla Mukamana and Oliva Bazirete in Women’s Health
Footnotes
Acknowledgements
Pre-Publication Support Service (PREPSS) supported the development of this manuscript by providing pre-publication peer-review and copy editing. The authors thank all health facilities and health professionals for facilitating the reaching of participants. The authors thank the participants for their active participation in this study.
ORCID iDs
Ethics considerations
Ethical clearance was sought from the University of Rwanda, College of Medicine and Health Sciences/Institutional Review Board (UR-CMHS/IRB; approval notices No. 298/CMHS IRB/2022).
Consent to participate
The gatekeeper who contacted potential participants explained the study to them and explained that participation was voluntary. During the day of data collection, the researcher also explained the study process and purpose. In addition, the researcher explained the principles of voluntary participation, confidentiality, and anonymity. The team was aware that a young girl who come to seek the service and is not accompanied by any of her parents is allowed to have ToP (in the Rwandan guideline for ToP, it notes that when parents are with their daughter when she come for it, and that they have misunderstandings on the issue, the wish of the girl preserves). It is from that background that all of our participants were considered to consent themselves to be part of the study. We noted that the youngest in the study participants had 16 years of age, which is the year that a Rwandan is mature and allowed to have an identity card. Thus, all participants signed a written consent form.
Consent for publication
Participants were informed of data publication and that it will not include any identifiable information of their names, residence, or any other identifiable information. Signing a consent to participate in the study, means they have agreed to participate and to give right authors to publish.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this project data collection: This research was funded with support from Center for International Reproductive Health Training (CIRHT) at University of Michigan, however, CIRHT did not participate in any phase of research development up to the generation of findings or influence any phase of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Also, the questionnaire used is available on the journal site, in a free data repository.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.