
Abstract
Background:
Health literacy varies in multicultural areas due to differing cultural beliefs. In Macao, a multicultural city in China, the blend of traditional Chinese and Western medicine influences health literacy, particularly in maternal–infant health. However, data on this topic are limited, hindering our understanding of healthcare in such regions.
Objectives:
This study investigates maternal knowledge, social support, and psychological stress among perinatal women in Macao.
Design:
A cross-sectional study was conducted with perinatal women between 28 weeks of gestation and 6 weeks postpartum.
Methods:
Maternal knowledge was measured using the Maternal–Infant Health Literacy Scale, social support with the Maternal Social Support Scale, and psychological stress with the Edinburgh Postnatal Depression Scale.
Results:
The overall maternal knowledge score of the 263 participants was relatively modest at 35.5, particularly lower in practical skills. Education level, number of childbirths and monthly income were positively correlated with maternal knowledge. The social support score was 21, indicating moderate support, while the psychological score was 8.8, reflecting generally low stress levels. No significant correlations were found between maternal knowledge and social support or stress.
Conclusion:
This study highlights the importance of addressing knowledge disparities during the perinatal period in multicultural urban areas. Enhancing maternal knowledge can improve healthcare outcomes and inform culturally tailored educational programmes for diverse populations.
Plain language summary
Understanding health information is crucial for mothers to make informed decisions about their health and their baby’s health. However, health knowledge can vary across different cultures, especially in multicultural cities like Macao, China. This study aimed to understand the levels of health knowledge, social support, and stress among new and expecting mothers in Macao. The study found that mothers in Macao had moderate health knowledge, especially in practical skills. They had moderate levels of social support and generally low stress levels. There was no clear connection between health knowledge and social support or stress. The study highlights the importance of improving health knowledge for mothers in multicultural cities like Macao. Future research should focus on developing programmes to increase health knowledge, reduce stress, and strengthen social support for mothers.
Introduction
Maternal–infant health literacy refers to a perinatal woman’s ability to access, understand and apply health information relevant to maternal and infant care. 1 This literacy is vital for informed healthcare decision-making, enhancing the well-being of both mother and child. It enables women to make informed choices about nutrition, ensure timely immunizations and navigate other critical healthcare decisions. Conversely, low health literacy can impair a woman’s ability to interpret health information, leading to negative outcomes such as birth trauma, poor nutrition and mental health issues. Thus, promoting health literacy is essential for reducing risks and fostering healthier families. 2
Maternal–infant health literacy is shaped by various interconnected factors that affect a woman’s ability to access and use health information. Women with higher education and financial resources generally have better health literacy. 3 In contrast, those in non-native language environments face significant barriers to understanding essential healthcare information. 4 Cultural background and religious beliefs also influence health literacy by affecting attitudes toward healthcare. 5 Additionally, family support, emotional well-being, past experiences, geographic location, age and healthcare system complexities further complicate these challenges.6,7 Understanding these factors is crucial for developing effective interventions to promote health literacy and improve maternal and infant health outcomes.
Recent systematic reviews indicate that the prevalence of low health literacy among pregnant women ranges from 15% to 44%. 7 This analysis included 13 randomized controlled trials from various regions, such as Australia, South America, theUnited Kingdom, the United States, South India and South Africa, focussing on enhancing health literacy through tailored interventions. These interventions included face-to-face sessions in-home visits, community health centres and antenatal clinics.8 –10 For instance, a decision-aid intervention in Australia provided a 24-page booklet and pamphlets during consultations with General Practitioners. 11 Written materials, such as information leaflets and computer programs, were also used effectively. 12 Overall, these interventions showed significant improvements in health literacy, but their effectiveness varied based on contextual factors such as healthcare systems, cultural backgrounds, education levels and language proficiency. 7 This highlights the necessity for tailored interventions that consider the unique characteristics of different populations and regions to maximize their impact.
Understanding health literacy is vital for postnatal mental health, as postnatal depression can significantly impact both mother and child. 13 Mothers with this condition often experience sadness, fatigue, irritability and anxiety, which can hinder their emotional bonding with their infants. 13 Such disruptions may delay the child’s emotional and cognitive development, affecting long-term well-being. 13 Research shows a strong link between postnatal depression and maternal health literacy,14,15 indicating that a mother’s understanding of health information is crucial for her mental well-being.
Social support for perinatal women is crucial for their well-being. 16 Enhanced social support not only improves their quality of life but also serves as a protective factor against perinatal depression. 17 Research shows a positive correlation between social support and maternal health literacy,3,18 suggesting that a strong support network helps mothers better understand and use health information. This study aims to explore the relationship between social support and maternal health literacy in the perinatal population of Macao.
Healthcare in Macao’s multicultural context
This study was conducted in Macao, a unique multicultural city that stands out among urban centres worldwide and within China. Its diverse educational system includes schools using different languages, such as English, Chinese and Portuguese, 19 suggesting that language proficiency may significantly affect health literacy levels. Consequently, findings may differ from those in nearby cities like Hong Kong or elsewhere in China. Cultural background and the healthcare system also affect health literacy. 7 Macao’s integration of traditional Chinese medicine with modern Western practices creates diverse patient attitudes that may not exist in other regions. 20 Therefore, interventions to enhance health literacy in Macao should be tailored to these unique characteristics. Currently, maternal health literacy levels among perinatal women in Macao are uncertain. This study aims to address this gap by examining associations between maternal health literacy, postnatal depression and social support, potentially inspiring future research in multicultural contexts.
Materials and methods
Research design
This study employed a descriptive research method to examine maternal knowledge, social support and psychological stress during the perinatal period among pregnant women in Macao, as well as to explore their correlations. We used convenience sampling to recruit participants and distributed online questionnaires through a social media platform. The dependent variable in this study was the antenatal knowledge score obtained from the Maternal–Infant Health Literacy Scale (MIHLS), while the independent variables were derived from the General Information Questionnaire, Maternal Social Support Scale (MSSS) and the Edinburgh Postnatal Depression Scale (EPDS). The manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 21
All questionnaires were originally in Chinese, and participants responded in Chinese. However, for the benefit of our readers of this article, we have provided translations of the questionnaires in the Supplementary Materials. All questionnaires were self-administered, with the authors’ contact information included for participant inquiries. This study was performed between 30 September 2022 and 1 January 2023.
Data collection
Participants were invited to complete the questionnaires through commonly used social media platforms in Macao, including the ‘'Macao Mummy Group’ page on Facebook, the Macao Breastfeeding Association website and the ‘Macao Mummy Group’ on WeChat. Questionnaires were distributed only to participants who read and signed the consent form, which clearly outlined the study’s purpose, confidentiality assurances and participants’ right to participate or withdraw at any time. Written Informed consent was obtained from participants before proceeding with the questionnaire. All questionnaires were completed electronically and anonymously using smartphones or personal computers. The users of the social media platforms have no means of identifying the participants’ identities. All questions must be answered prior to submission. Participants were required to provide contact information for potential inquiries from researchers.
Maternal–Infant Health Literacy Scale
We utilized the MIHLS (Supplementary Material 1), developed by Dai et al. 22 to assess maternal knowledge. The scale comprises 55 items organized into 3 dimensions: basic knowledge and concepts, healthy lifestyles and behaviours and basic skills. Our pilot study indicated that most pregnant women completed it in 8–15 min. Scoring involved assigning one point for correct answers to single-choice questions and two points for correct answers to multiple-choice questions. A score of 60.0% or higher indicated adequate maternal–infant health literacy. 22
The scale exhibited strong reliability, with a Cronbach’s α coefficient of 0.90 and a split-half reliability of 0.80. Structural validity was assessed using principal component analysis (PCA). The Kaiser–Meyer–Olkin coefficient obtained from the PCA was 0.80 and Bartlett’s sphericity test yielded a significance level of p < 0.001, both of which indicate a strong suitability for factor analysis.
General Information Questionnaire
We employed a 10-question General Information Questionnaire (Supplementary Material 2) to collect basic demographic data, including age, education level, marital status, parity pregnancy, monthly income, plan for pregnancy, employment status, history of mental illness, living style and antenatal/postnatal status.
Maternal Social Support Scale
The MSSS, originally developed by Webster et al. 23 to assess social support among pregnant and postpartum women, was translated into Chinese by Li et al. 24 The questionnaire (Supplementary Material 3) consists of 6 items, scored from 1 to 5, with items 4 and 5 reverse-scored. The scale comprises 2 dimensions: items 1–3 and item 6 measure positive social support, while items 4 and 5 assess negative events. Scoring categories are 0–18 for low support, 19–24 for moderate support and above 24 for sufficient social support. In this study, we used the Chinese version of MSSS, which demonstrated good reliability and validity with a Cronbach’s α coefficient of 0.75. The questions were straightforward and easily comprehensible, allowing pregnant women to complete them quickly and assess their social support effectively.
Edinburgh Postnatal Depression Scale
To assess maternal psychological stress during the perinatal period, we utilized the Chinese-translated version of the EPDS (Supplementary Material 4). 25 The original EPDS has been translated into over 20 languages, all demonstrating acceptable validity. 26 The Chinese version of the EPDS exhibited strong validity, with an area under the curve of 0.91, alongside sensitivity and specificity values of 0.786 and 0.834, respectively. 25 This scale consists of 10 items, each scored from 0 to 3, with a total score ranging from 0 to 30. Scores below 9 are generally considered normal, scores from 10 to 12 suggest a possibility of depression and warrant further evaluation or consultation with a specialist, while scores exceeding 13 indicate a high likelihood of suffering from depression, necessitating intervention by a specialist.
Sample size
According to Roscoe’s guidelines, 27 and its related studies28 –30 the sample size for multiple linear regression analysis should be at least 10 times the number of variables. In our study, we had 10 items in the participants’ general information, 3 dimensions for the MIHLS, 2 dimensions for maternal social support and 1 dimension for the EPDS, totalling 16 variables. Thus, the minimum sample size required was 160. However, after reviewing incomplete questionnaire data collected, the final effective sample size for this study was 263 valid questionnaires, which exceeded the minimum requirement.
Participants
This study involved 263 local women from Macao, all of whom were between 28 weeks of gestation and 6 weeks postpartum. The inclusion criteria were Macao residents who were willing to participate, proficient in Chinese and without a history of mental illness. Exclusion criteria include individuals currently using psychiatric medications, those participating in other research studies that may influence the outcomes and residents who have lived in Macao for <6 months. We believe that a duration of 6 months is sufficient to indicate that participants spent the majority of their perinatal time in Macao.
Statistical analysis
Data analysis was conducted using IBM Statistical Package for the Social Sciences (SPSS; IBM Corp.) software (version 26). The first author primarily conducted the data collection and analysis under the supervision of the corresponding author, with verification from all other authors. Descriptive statistics, such as means, medians and standard deviations, were employed to present general demographic information. Inferential statistics included Independent Sample t-tests and one-way ANOVA to compare means of variables. Pearson’s correlation coefficient was used to determine correlations between numerical variables. Multiple regression analysis was employed to investigate the relationship and predictive function between the independent variables (general information, social support and psychological stress) and the dependent variable (level of maternal knowledge). Results were considered statistically significant at p < 0.05.
Results
General demographic information
A total of 269 questionnaires were collected, and 263 of them were valid, exceeding the calculated minimum sample size of 160. The predominant age group was 26–35 years, representing 77.6% of participants. Approximately 66.0% held bachelor’s degrees as their highest educational level. The majority were married (91.6%), with 51.0% having one child, 78.7% were currently employed and 36.1% reported monthly incomes in the range of Macanese pataca (MOP) 20,000–40,000. A majority of participants, 83.3% of participants were pregnant women, 16.7% were in maternity and 76.4% expressed an intention to become pregnant in the future. Sixty-five per cent of them had a history of postpartum depression, while 46.4% resided with their spouses.
The results of the independent sample t-tests and ANOVA analysis indicate that education level, number of childbirths, monthly income, history of postnatal depression and perinatal status affected the maternal-infant health literacy score significantly (p < 0.05; Table 1).
General information and scores on Maternal–Infant Health Literacy Scale among 263 participants.

Multiple linear regression analysis
The results of the multiple linear regression analysis showed a significant relationship between the demographic variables and the dependent variable (maternal knowledge; Table 2). The regression equation indicated that the highest level of education, number of childbirths and monthly income were positively associated with maternal knowledge, while the history of postnatal depression and perinatal status did not show significant associations. The resulting regression equation was:

Multiple linear regression analysis of the scores on Maternal–Infant Health Literacy Scale and other variables.
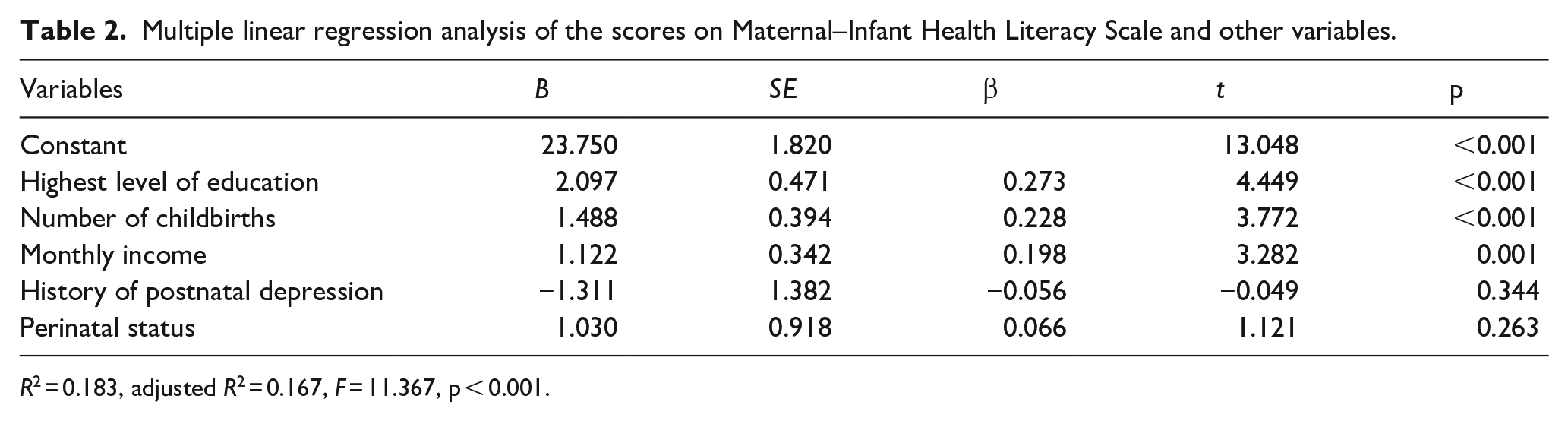
R2 = 0.183, adjusted R2 = 0.167, F = 11.367, p < 0.001.
The regression model had an R2 value of 0.18, indicating that the independent variables accounted for ~18.3% of the variance in the scores on the MIHLS. The adjusted R2 value was 0.17, suggesting that the model had a moderate level of fit. The F-value for the model was 11.37 (p < 0.001), indicating that the regression model was statistically significant.
Maternal knowledge
The total score for maternal knowledge was 35.52 with a standard deviation of 5.84. The MIHLS had a maximum score of 62, with a threshold of 60.0% (equivalent to a score of 37.20) indicating adequate maternal and infant health literacy. 22 Thus, this study indicated the overall maternal knowledge among perinatal women in Macao is relatively low. The MIHLS was divided into three dimensions: basic knowledge and concepts, healthy lifestyle and behaviours and basic skills. Notably, participants scored highest in basic knowledge and concepts while scoring lowest in basic skills.
Social support
The overall social support score was 21.23 ± 2.53. The MSSS determine that scores falling in the range of 0–18 signify low social support, scores between 19 and 24 indicate moderate social support and scores above 24 denote sufficient social support. 24 Our results indicate that perinatal women in our study reported having moderate levels of social support.
Psychological stress
The total score of the EPDS was 8.82 ± 4.66. A score below 9 is considered within the normal range, scores between 10 and 12 suggest a potential risk of depression and scores exceeding 13 indicate a diagnosis of antenatal depression. 25 Thus, our findings suggest that the perinatal women did not experience significant antenatal psychological stress.
The Pearson’s correlation coefficient between maternal knowledge and social support or psychological stress was 0.040 (p > 0.05) and −0.08 (p > 0.05), respectively. These results suggest that there is no significant correlation between perinatal knowledge and either social support or psychological stress among the participants.
Discussion
Most of the participants were first-time pregnant women aged between 26 and 35 years old, who had relatively high levels of education and income and expressed an intention to become pregnant again. These characteristics are consistent with the results of previous studies,31,32 which have highlighted an increased need for pregnancy-related health knowledge among individuals aged 22–36 years, first-time mothers, those with higher levels of education and those with higher incomes.
The participants in this study primarily consisted of members from different ‘Macao Mummy Groups’ on various social media platforms. As previously mentioned, these participants were predominantly first-time mothers with higher educational backgrounds and income levels. This observation may suggest that perinatal women with such characteristics are more willing to join social media groups of this nature and actively participate in sharing pregnancy experiences and discussing pregnancy-related information, as indicated by prior research.33,34 However, it remains unclear whether the knowledge shared by the participants on social media is accurate or not. Misleading or misunderstanding health information can significantly impact the health of both pregnant women and the foetus. 35
Maternal knowledge
The total score on the MIHLS in this study was 35.52, slightly below the 60.0% threshold score of 37.20. This suggests that perinatal women in Macao have a relatively low level of maternal knowledge. This finding aligns with previous research conducted in Beijing’s Haidian District 36 and Shanghai. 37 Both studies indicated that the overall maternal knowledge scores ranged between 50.0% and 70.0%, which is lower than that observed in some developed countries like the United Kingdom and the United States. 7 In terms of the three dimensions of the scale, it’s evident that basic knowledge and concepts received the highest score, while basic skills, such as caregiving, received the lowest score, highlighting the need for improvement in these practical skills.
A study conducted in Mainland China obtained results similar to those of this study. In the obstetrics department of Anhui Provincial Hospital, a study was carried out, revealing that the maternal health literacy of 258 participants was notably low. The study employed a Perinatal MIHLS to assess the maternal knowledge of the participants. Scores on this scale range from 0 to 34, with a score below 27 indicating low maternal health literacy. The average score obtained in this study was 20.50, signifying a low level of maternal knowledge. 38
The data collected in this study revealed that a significant proportion of participants had higher education levels, including bachelor’s degrees or higher. However, even within this educated group, the level of maternal knowledge remained low. Multiple regression analysis in this study identified a positive correlation between the number of childbirths, monthly income, education level and antenatal knowledge, which is in line with existing literature. 39
Association between maternal knowledge and social support or psychological stress
In this study, a total of 263 questionnaires were collected from pregnant women. We used various questionnaires, including general information, the MIHLS, the MSSS and the EPDS, to analyse the relationships between perinatal maternal knowledge, social support and psychological stress. Through statistical analysis, we found no significant connections between these factors. This study indicates that perinatal women in Macao did not meet the threshold for having adequate maternal knowledge, although they have moderate social support and low levels of psychological stress.
Social support can be divided into categorized into formal and informal forms. The results from our MSSS primarily represent informal social support, which mainly derives from friends and family. Prior research suggests that women prefer to seek informal assistance because it is perceived as more accessible and dependable. They like to obtain information and service support from informal social networks, such as online platforms. 40 These informal interactions among participants on social networks may contribute to reducing their psychological stress levels during pregnancy, consequently diminishing the likelihood of perinatal depression. 41
Recommendations
This study highlights the insufficiency of maternal knowledge among participants and we propose conducting a pilot test across various healthcare sectors to gather information about the health needs and ongoing health challenges faced by perinatal women. This approach will enable us to accurately identify the specific requirements of pregnant women in Macao. According to these identified needs, we recommend the implementation of workshops focussed on maternal–infant health literacy. These workshops should cover fundamental knowledge and concepts, promote healthy lifestyles and behaviours and essential caregiving skills. Furthermore, we suggest establishing online resources, such as websites or applications, to provide readily accessible and reliable information for perinatal women. 42 These recommendations aim to help perinatal women acquire the relevant maternal knowledge effectively, potentially leading to improved maternal and infant health, a potential reduction in the rate of caesarean sections and a minimization of the risk factors associated with high-risk pregnancies. 43
Regarding communication techniques, we would suggest using the ‘teach-back’ method. 38 This is an effective approach for improving maternal–infant health literacy, where healthcare professionals provide advice or information to mothers clearly and understandably and then ask the mothers to reiterate the advice or information in their own words. A clinical trial conducted in Anhui, China, involving 258 pregnant women with low maternal health literacy, demonstrated the effectiveness of the teach-back method. 38 It led to improved postpartum health behaviours, such as better breastfeeding techniques and reduced postpartum complications, including uterus subinvolution, acute mastitis, nappy dermatitis, overweight and postpartum constipation. 38 Although the busy healthcare environment in Macao may not widely adopt the teach-back method, its promotion in Macao could contribute significantly to enhancing health literacy among pregnant women.
Limitations
This study collected data through online electronic questionnaires, primarily recruiting participants via ‘Mummy Groups’ on social media platforms. The respondents were members of these groups and may have been more attentive to pregnancy matters. This sampling method may introduce selection bias and limit the generalizability of the findings to the broader population of pregnant women in Macao. However, using social media ‘Mummy Groups’ to recruit participants effectively engages a demographic that actively seeks information and support during the perinatal period. This targeted approach enriches the data collected and may also pave the way for the development of tailored educational programs aimed at improving health literacy and support for vulnerable populations.
This study did not collect data on the specific hospitals attended by participants. The type of hospital providing maternity services, such as private or public, could potentially influence the outcomes of this study. However, this approach enhances the generalisability of our results by reflecting the experiences of participants from various healthcare settings in Macao.
Another limitation of this study is that a power analysis was not conducted prior to data collection to determine the appropriate sample size. While we believe that our sample size of 263 participants is adequate, we cannot definitively assess the statistical power of our findings or ensure that the sample size was sufficient to detect significant effects. This oversight may impact the generalisability of the results and underscores the need for caution when interpreting the findings.
Furthermore, the cross-sectional nature of the study design limits the ability to establish causal relationships between the variables. This study relied on self-reported data, which may be subject to social desirability bias and recall bias. Participants may have provided responses that they perceived to be socially desirable rather than reflecting their true maternal knowledge levels, social support and psychological stress. The use of objective measures or a combination of self-report and objective measures, such as interviews, could enhance the validity of the findings in future studies.
Conclusion
This study included 263 participants with an average maternal knowledge score of 35.5, a social support score of 21 and a depression scale score of 8.8. These results indicate that perinatal women in Macao have relatively low maternal knowledge, moderate social support and no significant antenatal psychological stress. Additionally, higher education levels, more childbirths and greater monthly income are positively associated with maternal knowledge. The findings of this study emphasize the necessity of addressing disparities in maternal knowledge among pregnant women in Macao, as these disparities can significantly influence health outcomes during the perinatal period. It is crucial to develop targeted educational programs that specifically address the identified knowledge gaps, particularly for women with lower levels of education and income. Implementing tailored support and resources can enhance informed decision-making about health. Furthermore, evaluating the effectiveness of these initiatives will be essential to ensure they adequately meet the needs of perinatal women, ultimately contributing to improved maternal and infant health outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251347086 – Supplemental material for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China
Supplemental material, sj-docx-1-whe-10.1177_17455057251347086 for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China by Man I Lai, Jialing Chen, Pedro Fong and Lirong Meng in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251347086 – Supplemental material for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China
Supplemental material, sj-docx-2-whe-10.1177_17455057251347086 for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China by Man I Lai, Jialing Chen, Pedro Fong and Lirong Meng in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251347086 – Supplemental material for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China
Supplemental material, sj-docx-3-whe-10.1177_17455057251347086 for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China by Man I Lai, Jialing Chen, Pedro Fong and Lirong Meng in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057251347086 – Supplemental material for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China
Supplemental material, sj-docx-4-whe-10.1177_17455057251347086 for Association between maternal–infant health literacy, social support, and psychological stress during the perinatal period among women in Macao, China by Man I Lai, Jialing Chen, Pedro Fong and Lirong Meng in Women’s Health
Footnotes
Acknowledgements
The authors thank all the study participants.
Ethical considerations
This study was performed in accordance with the Declaration of Helsinki. Ethical approval for this study was obtained from the Research Ethics Committee of Macao Polytechnic University, Faculty of Health Sciences and Sports (FCSD/MSN-037/2022) before commencing this study. Throughout the research process, strict confidentiality was maintained and participant data were kept confidential.
Consent to participate
Written informed consent was obtained from participants before proceeding with the questionnaire. After each participant completed the questionnaire, the data were securely stored online and used exclusively for research purposes.
Consent for publication
All participants consented to the inclusion of their data in the publication.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
The data underlying this study can be obtained upon request from the corresponding author, subject to approval by the research ethics committee.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.