
Abstract
Background:
Women with neurofibromatosis type 1 (NF1) have an increased risk of breast cancer and poorer 5-year survival. Current breast surveillance patient information resources may be inappropriate for this cohort due to increased cognitive deficits and cancer worry.
Objectives:
This study aimed to develop and evaluate NF1-specific patient-centric educational resources about breast cancer surveillance.
Design:
A pilot, prospective longitudinal cohort study was conducted through a Sydney tertiary hospital (Royal North Shore Hospital) adult NF1 clinic and an established breast cancer risk management clinic.
Methods:
A brochure was developed with input from stakeholders and women with NF1 participating in breast surveillance. The content was adapted to create a webpage and animation evaluated through clinician and patient surveys. Final iterations of the resources were based on stakeholder feedback.
Results:
Nine semi-structured interviews were conducted with women with NF1 after breast surveillance. All considered the brochure acceptable and valuable and supported sharing the resource. Fifty-seven patient and clinician surveys were also completed, with the webpage and animation highly rated regarding acceptability, usefulness, and relevance.
Conclusions:
Information in three media has been developed specifically for women with NF1, considering breast surveillance to increase understanding, provide reassurance, and as a memory aid to support clinician consultation.
Highlights
A brochure, webpage, and informative animation were developed for women with NF1 considering early breast surveillance.
Acceptability, usefulness, relevance, readability, and visual appeal were highly rated.
The majority of participants would recommend the resources to others, very few found the content (e.g., breast cancer risk/biopsy) concerning.
Resources can be adapted for other conditions to reassure and support clinician verbal information.
Introduction
Neurofibromatosis type 1 (NF1) is a genetic condition with an increased incidence of benign and malignant tumors, cognitive deficits, and other comorbidities. There is an increased risk of breast cancer in women with NF1; consequently, the Cancer Institute NSW recommends annual breast surveillance from age 30. 1 This includes annual magnetic resonance imaging (MRI) ± Ultrasound (USS) (30–40 years), annual MRI ± mammogram (MMG) ± USS (40–50 years), and 2nd yearly MMG ± USS (>50 years), where MRI is the preferred option for women between 30 and 50 years. To ensure women with NF1 are supported through the breast surveillance process, targeted patient education, and support resources may be helpful.
Individuals with NF1 have a five-fold malignancy risk compared with the general population.2,3 The breast cancer risk in young female NF1 patients (<50 years) is five-fold higher than the general female population,4,5 with a greater risk of bilateral breast cancer. 6 The overall lifetime risk of breast cancer is three-fold higher for women with NF1 than the general population. 5 In addition, 5-year breast cancer survival is lower in women with NF1 (~68%) compared to women without NF1 (~82%–88%). 3 Several international studies propose women with NF1 undergo breast surveillance from age 30.5–9 In Australia, women with NF1 are recommended to undergo annual breast surveillance, including breast MRI and/or MMG and/or USS between the ages of 30 and 50 years. 1 However, previous studies have demonstrated that adults with NF1 have low uptake and adherence to healthcare surveillance,10–12 and evidence for the uptake of breast cancer surveillance has not been established.
A high prevalence of cognitive impairment in individuals with NF1 affects overall intelligence quotient (IQ), executive and adaptive functioning, learning ability, memory, and attention. These heterogeneous cognitive and adaptive functioning issues and medical complications responsible for some impairment of neurocognitive performance are summarized by Potter and Mendosa in a comprehensive review 13 (see Figure 1). In addition, many individuals with NF1 display features of anxiety, depression, poor self-esteem, and/or poorer quality of life.14–16 As health literacy levels are also lower among those with self-reported learning disabilities, 17 women with NF1 may find traditional resources challenging to understand. Hence, they may benefit from resources with easy readability.

(Color) Cognitive domains and findings in NF1 adapted from Potter. 13 Complete reference list for the graphic in Supplemental Appendix 3.
We previously identified that breast surveillance did not significantly increase psychological distress in women with NF1, with mean cancer worry and anxiety scores decreasing over time. 15 However, some women displayed clinical levels of anxiety before surveillance, and 77% of patients aged 35–50 years recorded an increase in stress-related behaviors between enrolment and receiving the results of their first round of surveillance. 15 In addition, 14% of women did not return for subsequent surveillance rounds, which could result in delayed diagnosis and poorer outcomes. 15 Limited access to patient-appropriate information and/or poor knowledge and understanding of disease and health surveillance guidelines12,18 may contribute to psychological distress and non-attendance. Therefore, it has been recommended that simple, easy-to-read educational resources be developed to support women with NF1. 15
Providing information in multiple formats has been reported to increase accessibility and health literacy.19–23 In breast surveillance, offering patients printed, internet-based, written, and audio-visual material can promote knowledge and attendance.24–27 Indeed, a brochure decision-aid regarding breast surveillance improved participation and attitude toward breast surveillance in women with low education levels, 27 and for those with cognitive deficits, appropriate pictures, diagrams, and charts can support understanding.28–32 It is essential that resources are evaluated by consumers and health professionals (HPs) 30 and tailored to patient preferences—to reinforce information received during a consultation.32,33
For a population with NF1, design, disease-specific readability, health literacy, and the possibility of associated cognitive issues must be considered.12,34 We utilized literature on readability, design, and evaluation principles (Supplemental Appendix 1) to inform the development of three resources specific to women with NF1 considering early breast surveillance. A brochure was chosen as the initial resource as patient information leaflets improve patients’ knowledge and satisfaction. 23 Content from the brochure informed the development of a webpage and animation. Satisfaction/acceptability, perceived utility (including readability), improvement in knowledge, relevance, and the emotional impact of each resource were then evaluated with important stakeholder groups, including women with NF1 who had undertaken breast surveillance.
The overall objective of this study was to develop easy-to-read, visually appealing educational resources that have clinical utility and are acceptable to women with NF1 considering early breast surveillance.
Aims
Design and develop a range of education resources for women with NF1, considering early breast surveillance.
Evaluate the perceived satisfaction/acceptability, utility (including readability), emotional impact, perceived improvement in knowledge, and relevance of these resources for women who participated in breast surveillance, clinicians, and support group representatives.
Use stakeholder feedback to inform the final resources for publication and use in the clinic.
Methods
This pilot, prospective longitudinal cohort study was conducted through a tertiary hospital adult NF1 clinic and an established breast cancer risk management clinic in Sydney, Australia.
Resource development
Resource development followed a sequential iterative process. A brochure was developed and evaluated, which informed the web content, animation, and final version of the brochure. Brochure design and development incorporated reviews of the literature, existing breast surveillance resources, design principles (Supplemental Appendix 1) and considered neurocognitive and psychosocial comorbidities associated with NF1 (Figure 1). The draft brochure was developed using a Flesh–-Kincaid readability grade between 6 and 8,35,36 with text written in active voice and graphics to aid understanding and improve aesthetics. The draft was reviewed by an educator, NF experts, cancer geneticists, and genetic counsellors working with patients with NF1 to ensure accurate, appropriate content and reading level.
Web content and an animation (Consentic®) were designed and developed based on the final brochure, with additional information on the processes involved in breast surveillance and links to further reputable information. A culturally diverse set of images was chosen to represent the diversity of the Australian population. The web (https://www.nslhd.health.nsw.gov.au/genetics/Pages/Our-NF-clinic.aspx) and animation content were reviewed by the same senior HPs who had provided feedback on the brochure.
Resource evaluation
Phase 1: brochure
Participants and recruitment
Twenty-eight women (30–50 years) with NF1 (hereafter referred to as patients) who had undergone initial breast surveillance were invited by email to participate in a telephone interview (May 2019–2021) using purposive sampling. These women were part of a more extensive pilot study describing the introduction of breast surveillance to women with NF1. 37 Exclusion criteria included the inability to provide informed consent or understand an English language consent form or an active cancer diagnosis. All patients read a participant information sheet outlining the goals and reasons for the study and provided written consent before their interview.
Instrument: interview schedule
An interview schedule (Supplemental Appendix 2.1) was prepared based on a previous study. 38 Questions explored knowledge of breast surveillance before and after the study, perceived clinical utility, readability, experience, and acceptability of the resource, and patient demographics. The interview guide was not pilot-tested.
Data collection and analysis
EH (BSc, third-year medical student) conducted semi-structured telephone interviews (June 2019–2021) after training with genetic counsellor AC (MSc) and research manager JF (with ⩾5 years prior qualitative research experience). No repeat interviews were conducted. EH had no relationship with participants prior to the study commencement. Prior to each interview, EH introduced herself and explained the reasons for her interest in the research topic. All interviews were audio-recorded, deidentified, and transcribed verbatim. No field notes were taken. A coding tree was developed iteratively by the interviewer (EH) and two independent coders (AC and JF). All three coders coded three deidentified transcripts independently (90% concordance). The remaining transcripts were coded by EH. Using thematic analysis guided by an inductive approach, 39 the three coders discussed and agreed on emerging patterns and relationships in the data, leading to the identification of relevant themes. Participants did not provide comments on transcripts.
Phase 2: web content and animation
Participants and recruitment
Twenty-eight patients who had breast surveillance and approximately 100 HPs with experience working with patients with NF1 were invited to participate in two online surveys to evaluate the resources (April 2020). The inclusion criteria for the women with NF1 were as above. Inclusion criteria for HPs included experience providing clinical care to women with NF1 and a role as (a) a clinical geneticist or genetic counsellor working in a genetic service in Australasia or (b) a radiologist, breast surgeon, or oncologist involved in breast surveillance at the risk management clinic for more than 6 months. An invitation to participate (including a link to the survey) was circulated (a) through the Human Genetics Society of Australasia listserv or (b) an email sent from the Head of Department to those involved in the high-risk clinic (May 2020). A member of the research team emailed patients. A reminder was emailed 2 weeks later to both patient and clinician cohorts.
For the online component of the study, beginning a survey response was taken as consent for participation. Participants were required to acknowledge that they had read the participant information prior to completing the survey. This included the statement: “For your information, if you submit an online survey, this will be taken as your consent for the use of your data in the study. Also, as this is an anonymous online survey, it will not be possible for us to withdraw your data after it has been submitted as we will not know which survey is yours.”
Instrumentation
Four surveys were designed to evaluate patient and HPs’ views on (1) the web content and (2) the animation (Supplemental Appendix 2.2). The surveys included questions on perceived satisfaction with the information provided (12 items web content/15 items animation), emotional impact (1 item), perceived improvement in knowledge about breast surveillance processes (5 items), relevance (5 items), and whether the patient or clinician would recommend the resources (acceptability; 1 item), all of which were loosely based on a previously published survey. 38 None of the surveys were validated. The survey also included demographic questions (4 items patients/5 items clinicians) and additional ad hoc patient questions about overall acceptability (4 items). Satisfaction and relevance items were rated on a 5-point Likert scale (very good to very poor), and other items were rated either Yes or No with open text boxes for comment. All items were evaluated for readability and adapted to have readability no higher than sixth grade 36 (see Supplemental Appendix 1). The number of HPs working with individuals with NF1 is unknown, so the percentage of HPs who pilot-tested the surveys could not be calculated. Patient surveys were not pilot-tested by patient participants.
Data collection and data analysis
Online survey data were collected securely using survey host REDCap.40,41 Any data from incomplete survey records were excluded. Data were analyzed using descriptive statistics and Fisher exact tests for small numbers using the statistical software program IBM SPSS Statistics (2017 v.25). 42 Data were dichotomized into “far too much/too much” = 1, “much too long/too long” = 1, and “Very good/good/neither good nor bad” = 1, other Likert scale responses = 0.
Phase 3: development and review of the final version(s)
Each resource was amended based on feedback. Patients reviewed the re-designed brochure for overall satisfaction with design and clarity. The brochure was then endorsed by a panel including NF experts, cancer geneticists/genetic counsellors, eviQ, The Children’s Tumour Foundation of Australia (CTF) NF support group, consumer tick Northern Sydney Local Health District (NSLHD), the New South Wales Center for Genetics Education, an Aboriginal liaison officer, and the Cancer Council Australia.
Results
Brochure evaluation
Demographics
Nine patients with NF1 who had completed breast surveillance expressed an interest in and participated in the study. Each patient received the brochure prior to a semi-structured telephone interview (11.5–24 min duration) (40% response rate). Most patients were 30–35 years old and university-educated. Almost half had experienced a biopsy, and most rated their knowledge of breast surveillance as low to moderate (Table 1).
Patient demographic data (brochure) and characteristics of women with NF1 who had undertaken breast surveillance through the risk management clinic.
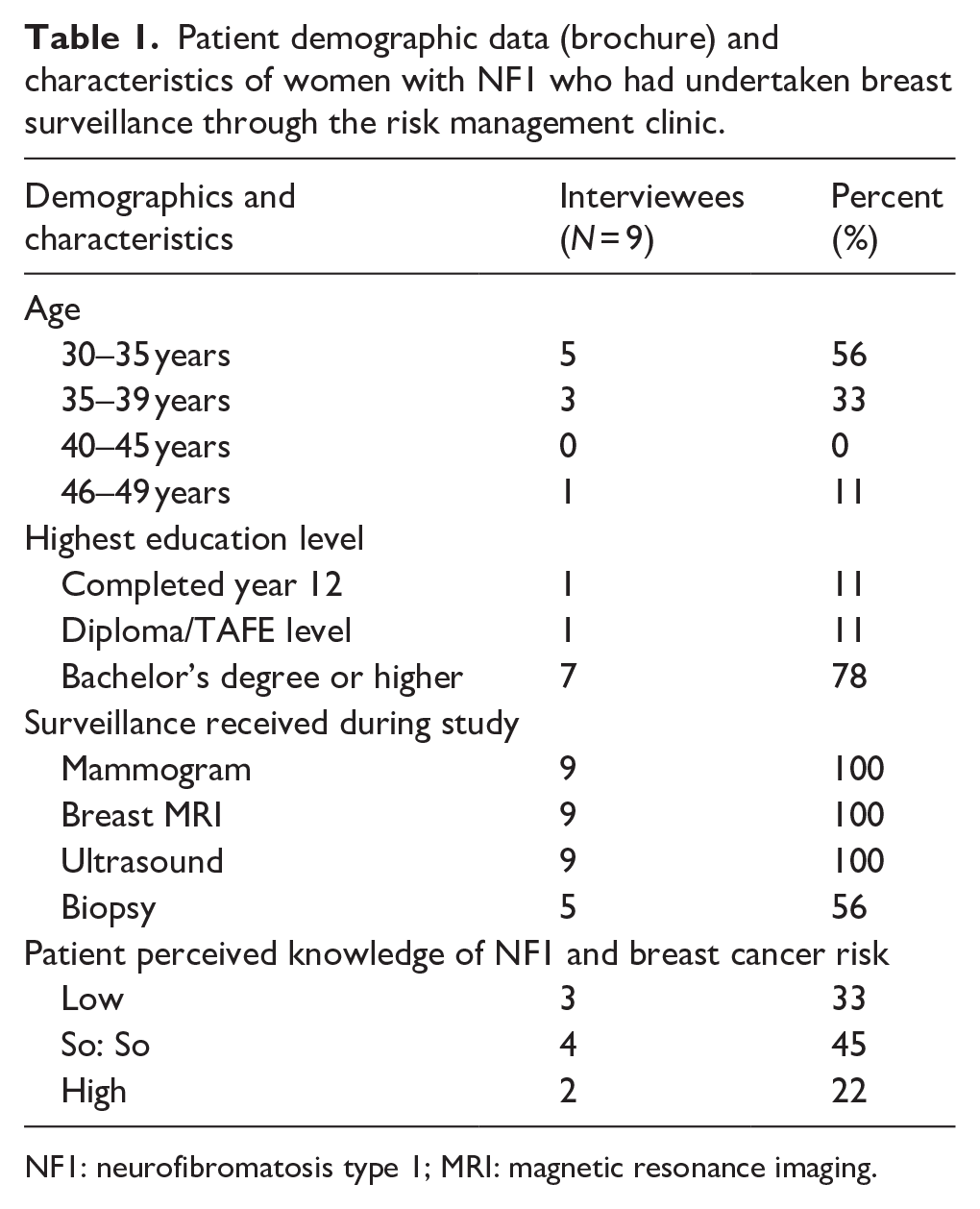
NF1: neurofibromatosis type 1; MRI: magnetic resonance imaging.
Results
Three themes were identified: Acceptability and utility, support for sharing information and experiences about NF1 breast surveillance, support for the brochure, and more resources for NF1.
Data saturation were not measured, but previous studies suggest for qualitative research this can be achieved with nine interviews. 43 Furthermore, “information power” can guide sample size, indicating that a relevant sample reduces participant numbers.44,45 Given the narrow study aims, dense sample specificity, strong quality dialogues, and the case analysis strategy, higher information power was expected to be achieved with fewer participants. Therefore, we believe our sample size was adequate to achieve information power.
Theme 1: acceptability and utility
Patient feedback on the amount and level of information and visual and overall presentation was largely positive. Although patients had varying levels of prior exposure to surveillance, all thought the brochure would be useful to women with NF1 who were considering breast surveillance. One patient wished she had received the brochure before surveillance (P7, 35–39 years); another commented that the brochure would be even more useful to women outside of a research study (P3, 30–35 years). Several patients also felt the brochure had utility as a memory aid, in reassuring women that surveillance did not equal cancer, and as a resource for other women with NF1 and family members. While most interviewees stated they did not learn anything new from the brochure, they perceived the resource as a valuable reminder of the surveillance process. For one participant, this was especially useful in the NF1 context: Because people with NF1 tend to have psychological/learning difficulties, and because we have so much happening with medical stuff, it’s great to have something to refer back to that says pretty much the same things the doctors would have told me. (P3, 30–35 years)
Several interviewees remarked it was helpful to be reminded why they were having surveillance and that it did not mean they had cancer. However, one interviewee wanted reassurance that “having a biopsy did not mean cancer” (P1, 46–49 years).
Theme 2: support for sharing information and experiences about NF1 breast surveillance
All participants supported the introduction of breast surveillance for younger women with NF1. However, some reported anxiety related to breast surveillance generally, with one patient reporting “it was kind of nerve-wracking” (P4, 30–35 years). Indeed, 3/5 women who had a biopsy reported added anxiety (P1, P4, P9). Consequently, feedback included providing reassurance about the biopsy process, that it was “not painful” and would further relieve anxiety. One participant felt reading the brochure increased anxiety (P7, 35–39 years).
Theme 3: support for the brochure and more resources for NF1
All participants reported that they would recommend the brochure to other women with NF1. There was also strong support for additional information on NF1 and breast cancer via online (P2, P3, P5, P6, P8) or hard copy printed information (P7, P8). Feedback included suggestions for improving clarity (related to MRI, MMG, and biopsy procedures), with two participants concerned with the color scheme.
Four patients with NF1 previewed the final brochure, all providing endorsement and positive feedback.
Webpage and animation evaluation
Demographics
In total, 57 surveys were completed, 29 regarding the animation (10 patients; 19 HPs) and 28 regarding the webpage (7 patients; 21 HPs). The patient response rate was 25% for the web information and 36% for the animation. It was not possible to calculate the response rate for HPs, as the number of HPs who opened the invitation was unknown. Most patients who completed the survey were 35–44 years old with a tertiary education. All had undertaken an MRI and an MMG; four (web) and six (animation) patients had a biopsy. Genetic counsellors completed the majority of HP website and animation surveys, and most HPs worked in general genetics (see Table 2).
Demographic data for participants in the online surveys.
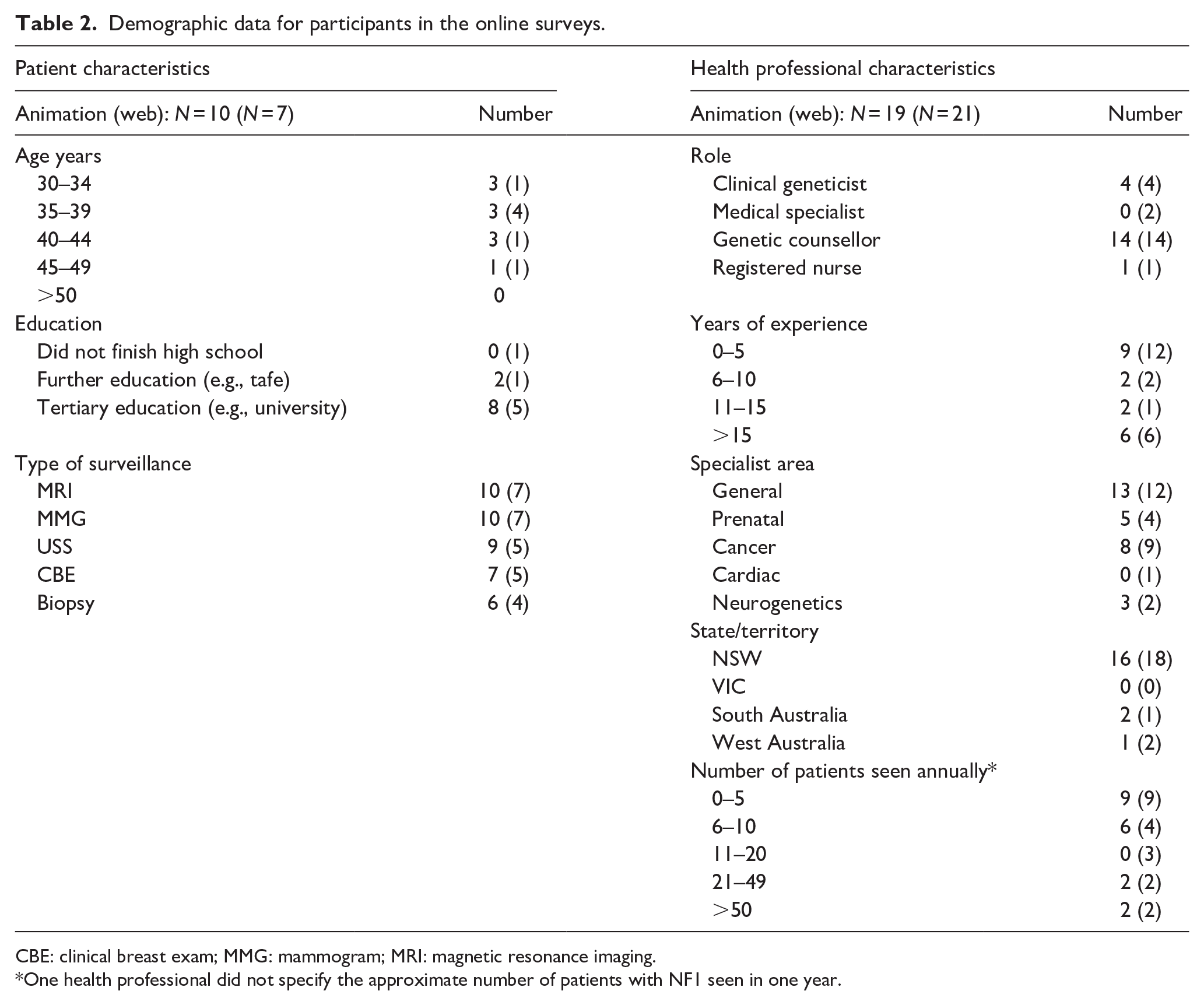
CBE: clinical breast exam; MMG: mammogram; MRI: magnetic resonance imaging.
One health professional did not specify the approximate number of patients with NF1 seen in one year.
Satisfaction/acceptability and utility of online resources
Some HPs and patients had concerns about the amount of information and/or the length of the animation and web resources. One patient and over half HPs felt the website and animation information was too long; around a quarter of the HPs believed there was too much information. Although HPs rated the animation as too long compared to patients (Fisher exact p = 0.008), there was no significant difference between HP and patient rating of the amount of content in the animation (Fisher p = 0.134) or length (Fisher p = 0.184) or amount of content (Fisher p = 0.290) for the web information (Table 3).
Participant feedback on information and specific aspects of e-resources.

CBE: clinical breast exam; MMG: mammogram; MRI: magnetic resonance imaging.
Only 13 participants completed this item.
The majority of patients rated most aspects of the website information and animation highly (Table 3). However, individual HPs rated the readability of text and voice of narration in the animation poorly, and a few HPs rated other aspects of web content design, format, navigation, reading ease, usefulness of graphics, font size, and usefulness of links negatively. There was no significant difference between HP and patient feedback on individual aspects of the animation or website. In free-text responses, three HPs commented that a graph (depicting breast cancer risk in women with NF1) was unclear, unnecessary, and/or should be removed. Another HP and one patient commented that the animation was too slow. One patient also noted some information conflicted with the information provided on links to other websites.
These issues have been addressed.
Relevance
All patients and HPs rated the information on breast surveillance procedures as relevant, although one HP rated the relevance of “clinical breast exam (CBE)” content as “poor” (Table 3). In free-text responses, this HP also commented “I am worried about self-examination, in case young women replace formal surveillance with this. I know breast awareness is listed in eviQ, but there is generally no evidence it is effective.” Another commented that “current eviQ guidelines recommend breast self-awareness rather than breast self-examination.” Despite these reservations, all patients and HPs reported they would be “very likely” (Animation: 90% (patients); 74% (HPs): web 86% (patients); 62% (HPs)), or “somewhat likely” (the remaining patients and HPs) to recommend the e-resources. One HP commented, “I think this website is a good source of information for a patient whose treating team has suggested surveillance,” and two patients reported: “I would most definitely share it [the animation] with my family members,” and two patients stated, “I wish that I had had this [the animation] before undergoing the surveillance just so that I knew what to expect.”
Emotional impact of the web and animation information
One patient described the animation content as somewhat “anxiety provoking”; however, none of the patients found the web information concerning. In contrast, eight HPs rated the animation, and seven rated the web e-resources as having the potential to cause patients concern or distress. Other HP comments (free-text) included: “some patients might be distressed by seeing the graph of their risk and think more deeply about their risk of breast cancer”; another that patients might feel like they are at higher risk than they are. One HP suggested that in the animation, the risk of breast cancer for individuals with NF1 sounded high, and it might be helpful to give examples of professionals with whom patients could speak to if they wanted to consider breast surveillance. All feedback was considered and addressed in the further development of the resources.
In comparison, two patients felt the information was “important and useful” and “reassuring,” with one patient reassured by the web statement, “one in seven women will need a biopsy,” as not knowing this prior to surveillance had caused her a lot of unnecessary distress. One HP also noted that the risk of breast cancer had been adequately addressed in the animation with the provision of appropriate support links.
Educational impact of resources
Several patients perceived improved knowledge about NF1, and that they learned something new about the types of breast surveillance available, breast surveillance programs, and the risk of breast cancer associated with NF1 from both resources. Most HPs (n ⩾ 13) also believed patients with NF1 would learn something new. However, one HP felt an online resource would complement information provided by a HP; “I think this website is a good source of information. . .; but does not replace personally tailored information from their treating doctors.”
Recommendations and final resource review
Based on stakeholder review, several changes were recommended to reduce the readability level, improve design, clarify content, and provide further support information (Table 4).
Amendments based on stakeholder feedback and literature review.

NF1: neurofibromatosis type 1; NSLHD: Northern Sydney local health district; MMG: mammogram; MRI: magnetic resonance imaging.
All comments and recommendations were considered, and most were addressed in the refined resources, with positive stakeholder feedback and relevant organization approval of the final brochure. The final web and animation content has been reviewed and amended based on the findings of this study.
Discussion and conclusion
Discussion
We developed and evaluated educational resources to assist women with NF1 undergoing breast cancer surveillance. Development of the resources considered:
Established design concepts
Recommended readability levels
Content based on current guidelines
Surveillance practices and available support service information
Stakeholder feedback (patients, experts, support group representatives)
The neurocognitive challenges and potential anxieties specific to a subset of individuals with NF1 were considered. All resources were well received by the majority of patient and HP participants, especially relevance and potential to improve understanding with minimal emotional impact.
An average Flesch–Kincaid readability score of 10.0 is reported for existing educational material on breast surveillance, 46 with some web-based resources having lower scores. 47 Although most individuals with NF1 have a normal range of IQ, for those with a mild intellectual disability or specific learning disabilities, Easy-Read resources are more likely to meet individual information needs. The Flesch–Kincaid level of 5.6 achieved in the study resources was important, as it has been reported more people read brochures with simple messages. 48 Furthermore, resources with a lower grade score (5.9) are reported as “easy to understand.” 46
Stakeholder feedback was integral to this study and led to changes likely to improve patient understanding. For example, the revised brochure used a pictograph to convey the number of women needing further investigation after their first breast surveillance. Pictographs have been shown to aid readability, recall, understanding of numerical information, and comprehension of patient information and risk uncertainty.49–51 Questions in the headings were adopted narratively to enhance patient interaction, although questions were avoided in the text.23,26,52–54
Clinicians identified two resource content areas as possibly concerning for patients; “increased breast cancer risk” and “biopsy.” Biopsy has previously been linked to higher anxiety.55,56 However, some patients saw these as essential information points to include. As risk information is important to mitigate potential adverse effects, the information resources were designed to reframe a patient’s focus on the positive health benefits of surveillance and the small likelihood of cancer while gently warning about the possibility of needing a biopsy. Despite the increased risk, it was emphasized most women would not be diagnosed with cancer, with the potential to improve outcomes through early management.
Although breast surveillance in NF1 patients does not increase psychological distress overall, some women experience negative aspects of surveillance and barriers to re-attendance for annual breast surveillance appointments. 15 We considered the possibility this was due to increased anxiety and distress and included sections “Who can I talk to?” and “Where can I find more information?” with links for additional support. This information could be provided alongside clinical discussions to ensure additional support can be provided to those who demonstrate signs of anxiety. Reassuringly, most patients did not have greater anxiety due to reviewing the information provided.
In hereditary cancer, tailored resources to support decision-making are a valuable source of knowledge without causing distress. 57 One of the benefits of developing resources, including web information and a downloadable brochure in (PDF) format, is they are easily updated and disseminated at a small cost. Given the changing evidence-based recommendations for surveillance, continual review will enable an update of the resources to align with best practice guidelines and links to appropriate further information and support groups.
Limitations of the study include the low participant numbers and response rate. This was due to only one clinic offering breast surveillance in a pilot research setting where, at the time of invitation, only 28 patients had received their initial screening as well as the small number of clinicians invited to participate. The small sample size limited the comparison between the HP and patient data. A power analysis for sample size was not performed. None of the surveys were validated. There was also a disproportionate representation of HP types, practice locations within Australia (NSW), and patient educational background (higher). Bias may be attributable to the self-selection of the patient cohort, who may exhibit higher cognitive abilities and engagement with a specialist NF1 clinic. 15
Biopsychosocial complexity, lower verbal IQ, and cognitive performance are associated with non-response.58,59 Despite this, previous studies suggest people with varying education levels can benefit from receiving a brochure, as this can improve participation and attitudes. 27 Lastly, participants’ opinions on the relevance of including “self-examination” were not evaluated, although two HPs raised it as an area of concern.
Future research could include a review of the brochure by a larger cohort of patients and HPs (now that breast screening for women with NF1 has been recommended Australia-wide from 30 years); dissemination through the clinic breast surveillance uptake/adherence (as recommended by Scherr et al. 60 ), and continued engagement in breast surveillance in the NF1 population. Also, the best times for providing the resources, the best pathway/clinicians to distribute the information, and usefulness to family members supporting women with NF1 having or considering breast surveillance.
Including consumers in the process as an innovation was a novel approach to research and resource design. This provided extremely valuable input on using language appropriate for the NF1 community. In addition, the design and development of an animation enabled us to use more culturally diverse images to represent Australia’s multicultural population. Including clinical review was important to ensure the distribution of resources through clinics and health services. Overall, we believe adoption of patient, clinician, support group, and organization feedback and endorsement has ensured the developed resources are current, accurate, fit for purpose, and easy to update, and they will improve access to breast surveillance for women with NF1.
Conclusion
In this study, a brochure, webpage, and animation were developed for young women with NF1 considering breast cancer surveillance. The study demonstrates resources on breast surveillance are useful and welcomed by patients and clinicians as they increase understanding, provide reassurance, and are a memory aid to support clinician consultation. Most of the feedback on key improvements in design, content, and ways to alleviate concerns about breast surveillance were incorporated into the final resource design. We expect the findings of this study will inform future resource development. https://www.nslhd.health.nsw.gov.au/genetics/Pages/breast-screening-neurofibromatosis.aspx
Supplemental Material
sj-docx-1-whe-10.1177_17455057251337118 – Supplemental material for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance
Supplemental material, sj-docx-1-whe-10.1177_17455057251337118 for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance by Caitlin Forwood, Emma Hartley, Jane Fleming, Ashley Crook, Diana Nawara, Mathilda Wilding, Lavvina Thiyagarajan, Katrina Moore, Yobelli Jimenez, Rebecca B. Saunderson, Nicola Poplawski and Yemima Berman in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251337118 – Supplemental material for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance
Supplemental material, sj-docx-2-whe-10.1177_17455057251337118 for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance by Caitlin Forwood, Emma Hartley, Jane Fleming, Ashley Crook, Diana Nawara, Mathilda Wilding, Lavvina Thiyagarajan, Katrina Moore, Yobelli Jimenez, Rebecca B. Saunderson, Nicola Poplawski and Yemima Berman in Women's Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251337118 – Supplemental material for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance
Supplemental material, sj-docx-3-whe-10.1177_17455057251337118 for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance by Caitlin Forwood, Emma Hartley, Jane Fleming, Ashley Crook, Diana Nawara, Mathilda Wilding, Lavvina Thiyagarajan, Katrina Moore, Yobelli Jimenez, Rebecca B. Saunderson, Nicola Poplawski and Yemima Berman in Women's Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057251337118 – Supplemental material for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance
Supplemental material, sj-docx-4-whe-10.1177_17455057251337118 for The development and evaluation of educational resources for young women with neurofibromatosis type 1 undergoing breast cancer surveillance by Caitlin Forwood, Emma Hartley, Jane Fleming, Ashley Crook, Diana Nawara, Mathilda Wilding, Lavvina Thiyagarajan, Katrina Moore, Yobelli Jimenez, Rebecca B. Saunderson, Nicola Poplawski and Yemima Berman in Women's Health
Footnotes
Acknowledgements
We would like to thank the women with NF1 who have undertaken breast surveillance for their input in the development of these resources and information from the CTF, Cancer Council of Australia, NSW Center for Genetic Education, EviQ, NSLHD, and the many clinicians who contributed to the content and design. We would also like to acknowledge graphic designer Krista Recsei from Pangolin Consulting for the brochure’s final design and Peter Swift from One on One design and print for the cognitive graphic in ![]() . We also thank Dr Brian S. Potter for his willingness for the graphical adaption of the comprehensive Book Chapter co-authored with Leanne Mendoza titled “Cognitive Issues Experienced by Individuals Living with Neurofibromatosis,” published in Neurofibromatosis—Current Trends and Future Directions. We acknowledge the original work and contribution of Dr. Emma Hartley and Diana Nawara for the research that informed this article. We would like to acknowledge the original contribution of Joint Venture Partners (Northern Sydney Local Health District and the University of Sydney, School of Health Sciences, Faculty of Medicine and Health) for funding of a Kickstarter grant to support the development of the animation and Rebecca Saunderson and Consentic® for the animation production. We also acknowledge the receipt of the Human Genetics Society of Australia and the Nigel Clarke Memorial Education Bursary awarded to Dr Caitlin Forwood to support this research.
. We also thank Dr Brian S. Potter for his willingness for the graphical adaption of the comprehensive Book Chapter co-authored with Leanne Mendoza titled “Cognitive Issues Experienced by Individuals Living with Neurofibromatosis,” published in Neurofibromatosis—Current Trends and Future Directions. We acknowledge the original work and contribution of Dr. Emma Hartley and Diana Nawara for the research that informed this article. We would like to acknowledge the original contribution of Joint Venture Partners (Northern Sydney Local Health District and the University of Sydney, School of Health Sciences, Faculty of Medicine and Health) for funding of a Kickstarter grant to support the development of the animation and Rebecca Saunderson and Consentic® for the animation production. We also acknowledge the receipt of the Human Genetics Society of Australia and the Nigel Clarke Memorial Education Bursary awarded to Dr Caitlin Forwood to support this research.
Ethics considerations
Ethics approval was obtained from the Northern Sydney Local Health District (NSLHD) Human Research Ethics Committee (REGIS No. 2020/ETH 00762).
Consent for publication
All patients read a participant information sheet outlining the goals and reasons for the study and provided written consent before their interview. For the online component of the study, beginning a survey response was taken as consent for participation. Participants were required to acknowledge that they had read the participant information prior to completing the survey. This included the statement: “For your information, if you submit an online survey, this will be taken as your consent for the use of your data in the study. Also, as this is an anonymous online survey, it will not be possible for us to withdraw your data after it has been submitted as we will not know which survey is yours.”
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant procured from the Children’s Tumour Foundation of Australia and The Honourable Brad Hazzard Minister for Health and Medical Research. The RNSH No. 2 Trust Fund supported the Advanced Trainee Research Program.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rebecca B. Saunderson reports administrative support was provided by Consentic. Rebecca B. Saunderson reports a relationship with Consentic; she is the founder and has board membership and employment. Consentic helped in kind with the animation production, including revisions and production, at cost/not for profit. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Data availability statement
Data and materials may be available on request by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.