
Abstract
Background:
In the United States, Black women have the second highest incidence of cervical cancer (CC) due to high incidence of human papillomavirus (HPV), slow HPV clearance rates, and low receipt of preventive pap smears and vaccines.
Objective:
A Black Feminist Thought framework was used to examine how the media portrayal of Black women, racial identity, and familial factors impact CC prevention behaviors among young Black women.
Design:
Black women enrolled at a large southeastern university consented and participated in an online mixed-methods survey examining facilitators and barriers to CC prevention behaviors. Quantitative items were analyzed via descriptive statistics, and qualitative items were thematically evaluated using an interpretative phenomenological analysis.
Method:
Black undergraduate women completed an online survey that collected quantitative data on demographic information, CC knowledge, perceived eHealth literacy, and CC prevention behaviors. Participants also responded to seven qualitative items that explored how the media portrayal of Black women, racial identity, and familial factors impact their CC prevention behaviors.
Results:
Participants (N = 146) were Black college women aged 18–26 who primarily identified as cisgender, non-Hispanic/Latine/x, and heterosexual. Most participants self-reported as having high e-Health literacy (78.1%, n = 114) but demonstrated inadequate CC knowledge (90.3%, n = 131). All age-eligible participants received pap smears within their lifetime (n = 6), and most received at least one dose of the HPV vaccine (77.5%, n = 86), with the majority reporting series completion. Qualitative findings highlighted participants experiences of oppression co-existed with self-advocacy, primarily in medical settings.
Conclusion:
Results provide insight for culturally tailored interventions in care settings serving young Black women that may encourage preventive care to reduce the prevalence of CC in later adulthood.
Plain language summary
Despite cervical cancer (CC) being one of the few preventable cancers, Black women have among the highest death rates. The present study examined how eHealth literacy, CC knowledge, cultural, and media factors impact CC prevention behaviors in Black college women.
Introduction
Human papillomavirus (HPV) is a highly infectious sexually transmitted infection (STI) that is the cause of virtually all cases of cervical cancer (CC). 1 The HPV is transient and clears naturally within 2 years in most individuals 2 ; however, persistent infection can develop into cancerous lesions of the cervix. 2 Fortunately, CC is one of the few cancers in which primary and secondary prevention can be achieved by completing the HPV vaccination series and routine pap smears, respectively. Primary prevention is achieved through the completion of prophylactic immunizations (i.e., Gardasil), with American Committee of Immunization Practices recommendations to be administered as early as age 9. 3 Furthermore, secondary prevention recommendations reflect the age and risk level of the person being assessed. For women between the ages of 21 through 29, the U.S. Preventive Service Task Force (USPSTF) recommends triennial screening regardless of vaccination status. 3 Although women can be sexually active before the age of 21, research indicates that a CC diagnosis among this age population is rare. 1 Despite the prophylactic benefits of both preventative methods, Black women continue to disproportionately develop this disease. 1
Cervical cancer disparities
In the United States, Black women have the second highest incidence rates of CC, following Hispanic women, but have the highest rates of CC mortality across all racial/ethnic groups. 3 Reasons for Black women’s increased vulnerability are multifaceted and can be partially explained by high rates of HPV acquisition, 4 lower likelihood of engaging in routine pap smears, 5 and persistently low vaccine uptake. 6 HPV vaccination and pap smear non-adherence among Black women is a serious public health concern due to their resulting disparate CC outcomes. Considering the preventable nature of CC, it is imperative to consider factors that contribute to disparities from both individual and structural perspectives. Key individual factors include attitudinal dispositions against the HPV vaccine, 7 history of HPV, 8 poor understanding of cervical screening procedures, 9 younger age (<50), receiving inaccurate test results (i.e., false-positive or false-negative),10,11 and lack of medical treatment related to CC screening. 12 Moreover, a structural context acknowledges historical barriers such as slavery, denied access to education and other major life stressors that have significantly contributed to medical distrust, and prevented Black women access to medically necessary cancer prevention services.13 –15 In efforts to increase prevention services among young Black women, more empirical attention needs to examine platforms that are likely to be frequented among this population, such as online media. 16
Online media and cervical cancer prevention
Medical mistrust in the Black community has been associated with more frequent use of electronic platforms for health advice. 16 In response to this health information dissemination shift, more research has prioritized using social media platforms to promote CC prevention behaviors.17,18 Although the use of online platforms remains an ideal medium to disseminate CC prevention information, the presence of stereotypical images of Black women in media can further complicate dissemination efforts. For example, negative appraisals of stereotypical portrayals of Black women have consequences for low self-esteem, poorer interpersonal relationships, and adverse mental health. 19 Due to the causative agent of CC being an STI, Black women may be more susceptible to negative appraisals such as the Jezebel stereotype, an erroneous depiction of Black women as hypersexualized beings. 20 In efforts to deconstruct Eurocentric frameworks that often misrepresent Black voices, 21 the study was guided by two complementary and culturally sensitive frameworks: Health Skills Literacy Framework (HSLF) and Black Feminist Thought (BFT).
Health skills literacy and Black feminist thought
HSLF supports the tenet that there is an interdependent relationship between the demand for health stimuli and comprehension. 22 The ability to critically evaluate the credibility of sources of information is crucial in the development of health-related behaviors (e.g., HPV vaccine uptake and pap smears) and reducing disparate health outcomes. However, disparities persist beyond structural factors such as cost and access to healthcare resources. 23 As such, BFT can complement the HSLF framework by guiding the examination of the unique health-related experiences of Black women linked to demographic factors that confer identity.
BFT places a greater emphasis on the lived experiences of Black women that positions Black women as experts in the literature, while simultaneously recognizing the importance of employing qualitative methods to more adequately represent their unique experiences.24,25 Additionally, the iterative relationship between BFT and HSLF may also be useful in studying how future healthcare interactions may lead to the adjustment or solidification of young Black women’s thoughts and behaviors related to CC prevention.
To elucidate key factors in CC prevention among young Black women, the present study utilized BFT and HSLF as complementary frameworks to examine the impact that cultural and health influences, including the media portrayal of Black women, familial conversations, racial identity, CC knowledge, perceived eHealth literacy, and perceptions of HPV risk have on CC prevention behaviors among Black college women. To the best of our knowledge, this is the first study to combine BFT and HSLF to examine CC preventive behaviors in Black college women.
Methods
Study design
The overarching study aims to integrate BFT and HSLF to challenge monolithic assumptions of Black women, by considering how racial identity, familial conversations, and media portrayal of Black women impact their CC prevention behaviors. The present study is a subset of a larger cross-sectional, mixed-methods project that examined cultural facilitators and barriers to CC prevention among Black college women.
Participants
Individuals who: (1) self-identified as Black/African American, (2) were between the ages of 18–26, (3) read and understand English, and (4) had a uterus were recruited from Introductory Psychology courses and targeted emails at a large southeastern university. Women were excluded if they (1) did not have a uterus, (2) were under the age of 18/over the age of 26, (3) did not identify as Black/African American, and (4) had inability to read and understand English. All recruited participants were given the option to participate in a gift card lottery as an incentive for participation in the present study. After completing the survey, participants were provided with informational resources about CC and psychotherapeutic services.
Data collection and measurements
Data were collected between February 2021 and October 2022. All study materials and procedures received Institutional Review Board approval (UMCIRB 21-002821). Following written consent, participants completed an online Qualtrics survey that quantitatively inquired about personal/medical demographics, perceived eHealth literacy, 26 e-Health utilization, CC knowledge, 27 CC screening beliefs, 28 HPV vaccination beliefs, 29 CC preventive recommendation from healthcare providers, and CC prevention behaviors.
Personal/medical demographics
Participants were asked questions related to their age, ethnicity, sexual orientation, parental educational attainment, insurance status, sexual activity, number of sexual partners, personal history of CC and HPV, family history of cancer, and contraceptive use.
eHealth literacy
The eHeals scale was used to assess knowledge, evaluation, and use of online health resources. 26 This eight-item measure used a five-point Likert scale, ranging from 1 (strongly agree) to 5 (strongly disagree). An example item included, “I have the skills I need to evaluate the health resources I find on the internet.” The items were summed for a total score, with higher scores indicating higher perception of eHealth literacy.
eHealth utilization
Two items were used to assess for eHealth utilization. Participants were asked about their most frequented online platform to gather health information. Item options included, social media, online search engines, video platforms (e.g., TikTok), social media platforms (e.g., Instagram), governmental medical websites (e.g., CDC), academic medical websites (e.g., MayoClinic), health websites geared to the general public (e.g., WebMD), and denied use of electronic platforms. Another item assessed their frequency engaging in electronic health platforms. Options included, never, 1–5 times a month, 6–10 times a month, or more than 10 times a month.
CC knowledge
Fifteen items from the CDC CC fact sheet 27 were administered to assess knowledge of CC, specifically HPV risk, HPV vaccine, and pap smears. An example item included, “A pap smear is a test to find out if a woman is pregnant?” Response options included, true, false, or I don’t know. Each correct response received one point. All items were summed to yield total scores for overall CC knowledge, where higher scores indicated greater CC knowledge. Participants who scored at least 12 out of 15 total items correctly were categorized as having adequate CC knowledge.
CC screening beliefs
The Pap Smear Belief Questionnaire 28 is a 25-item measure that assesses beliefs toward the benefits and barriers to the pap smear procedure and perceived vulnerability to CC. Response options are on a five-point Likert scale that ranges from 1(strongly disagree) to 5 (strongly agree). The measure yielded a cumulative score (total possible score of 125), with higher scores indicating more positive beliefs toward pap smear uptake. An example item included, “I have other problems more important than getting a Pap smear.”
HPV vaccination beliefs
Items adapted from Darensbourg et al. 29 were used to examine beliefs about the HPV vaccine. This 11-item measure uses a seven-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Higher summed scores indicated more positive beliefs toward the HPV vaccine. An example item from this measure included, “When it comes to getting vaccinated, my family’s opinion is important.”
Provider recommendations
Two items were administered to examine if participants were recommended the HPV vaccine and pap smear by their healthcare provider.
CC prevention behaviors
Three items were used to assess HPV vaccination uptake, completion of HPV vaccination series, and receipt of a pap smear.
Participants were also qualitatively assessed using the following BFT-informed items.
(1) What factors do you think influence your parent’s/guardians’ decision regarding the HPV vaccine?
(2) How has your racial identity influenced your decision regarding receiving a pap smear?
(3) From your perspective how has the media portrayed Black women?
(4) How has that portrayal impacted your perspective on the HPV vaccine?
(5) How has that portrayal impacted your perspective on routine pap smear adherence?
(6) How does your perceived portrayal of Black women in media impact familial conversations surrounding the HPV vaccine?
(7) How does your perceived portrayal of Black women in media impact familial conversations surrounding pap smear adherence?
Data analysis/statistical analysis
Both quantitative and qualitative data were downloaded from Qualtrics and analyzed using IBM SPSS Statistics 26 Software 30 and SocioCultural Research Consultants Dedoose coding software, 31 respectively. The sample size of the present study was determined via a G*Power analysis, 32 in effort to reach sufficient power for a larger mixed-method study. However, the present data met saturation requirements with respect to data richness and depth of understanding.33,34
Participant and medical demographic information, perceived eHealth literacy, CC knowledge, CC screening beliefs, HPV vaccination beliefs, e-health utilization, provider recommendations, and CC prevention behaviors were analyzed descriptively. An interpretative phenomenological analysis (IPA) approach was used to analyze the qualitative portion of the present study. 35 An IPA approach, informed by BFT, aimed to deconstruct the generalized perceptions of Black women by taking a close examination of how participants make sense of their unique experiences navigating healthcare and other oppressive systems.
The coding team consisted of three cis-gender women. Two of them self-identified as Black, and the third woman self-identified as White. All coders completed a reflexive journal during the analysis process in which thoughts, biases, and assumptions of the data were noted and discussed during subsequent group coding sessions. 36 Participants’ responses were transcribed verbatim. IPA involved close reading of the transcript, extracting recurring sentiments from participant narratives, transforming codes into emergent themes, seeking relationships, and clustering themes. 37 Mixed-method article reporting standard guidelines were consulted when preparing this article. 38
Results
Demographic statistics
All participants (N = 146) identified as Black/African American, between the ages of 18 through 26 (M = 19.21, SD = 1.77). Participants were primarily non-Hispanic Black (89.6%, n = 131), heterosexual/straight (66.4%, n = 100), cisgender women (74.8%, n = 107), sexually active (88%, n = 60.3), no personal history of CC (94.5%, n = 138), no personal history of HPV (98.6%, n = 144), and adequately insured per college enrollment requirement, with their mothers’ earning at least a bachelor’s degree (24.7%, n = 36).
Cervical cancer knowledge, e-health literacy, and provider recommendations
The vast majority of participants (90.3%, n = 131) did not demonstrate adequate CC knowledge, with many participants (92.5%, n = 135) erroneously identifying the correct purpose of a pap smear, which many believed it was a method to detect for pregnancy. In addition, well over half of participants (78.1%, n = 114) self-reported that they had an adequate perception of e-health literacy or confidence in navigating general online health information. Beliefs toward CC prevention behavior were primarily neutral for both CC screening and HPV vaccine uptake. Roughly 45% of participants indicated that their provider recommended the HPV vaccine, with even fewer (16.4%, n = 24) indicating a provider recommendation for pap smears during their medical visits, which is likely explained by the USPSTF guidelines and age-ineligible participants in the present study.
E-health utilization
There were 89 participants (61%) who reported internet search engines as their most frequented e-Health platforms and social media, such as Facebook and Instagram, as their least frequented platforms (4.8%, n = 7). Of the 146 participants, 69.2% reported searching electronic-based platforms at least one to five times a month.
CC prevention behaviors
Of the participants that responded to the vaccination status inquiry (N = 111), most (n = 86) received at least one-dose of the HPV vaccine, with comparable rates (n = 74) of series completion, with seldom indication of no receipt of the vaccine (n = 25). Regarding pap smear receipt, most respondents were under the age of 21 and had yet to reach the recommended age for pap smears (n = 140). Although all of the participants that were pap smear eligible (n = 6) received a pap-smear within their lifetime, only two noted being up to date on their tri-annual pap test. However, all participants who reported an abnormal pap-test (n = 2) indicated adhering to the recommended follow-up procedure. Notably, participants who fell outside of the age-based recommendations for pap smears reported receipt of pap-testing (n = 42) and appropriate follow-up (n = 3), suggesting favorable beliefs toward preventive behaviors. Additional medical demographics and CC-related descriptive statistics are found in Tables 1–4.
Participant demographics.
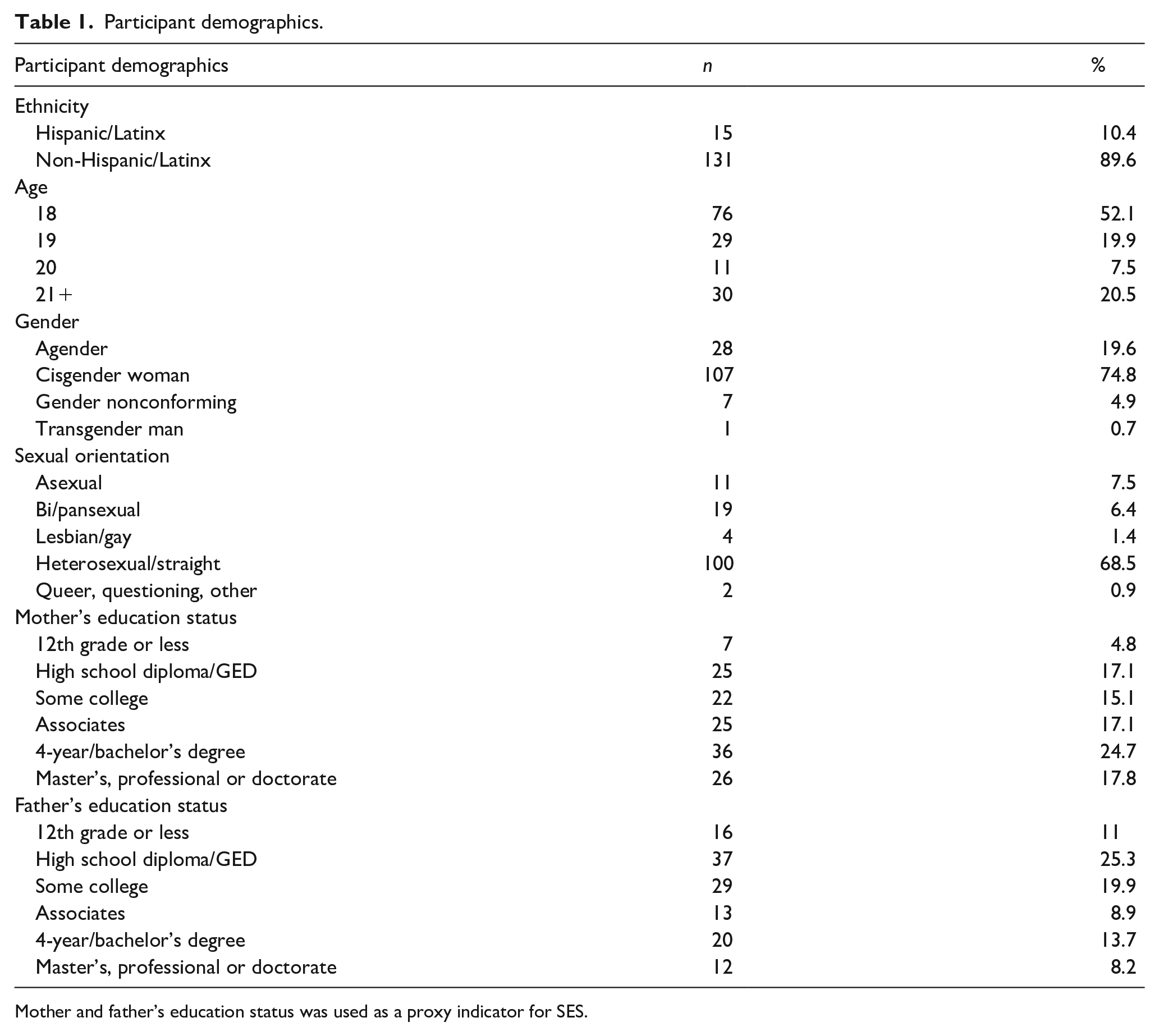
Mother and father’s education status was used as a proxy indicator for SES.
Medical demographics.

Number of sexual partners within a lifetime.
Participants had an option to select more than one contraceptive used in the past 12 months.
Key study variables descriptive statistics.

Cervical cancer prevention behaviors.
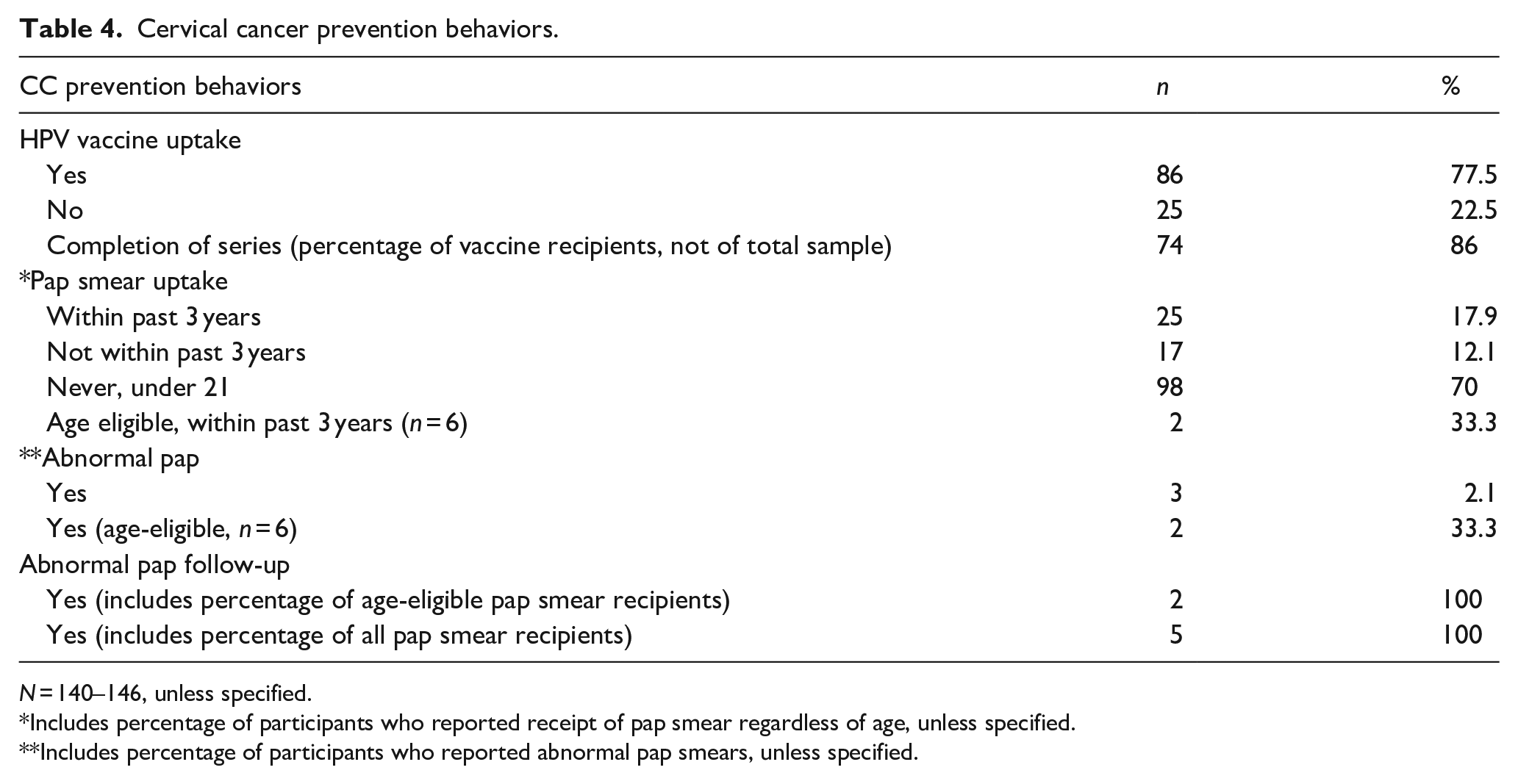
N = 140–146, unless specified.
Includes percentage of participants who reported receipt of pap smear regardless of age, unless specified.
Includes percentage of participants who reported abnormal pap smears, unless specified.
Qualitative results
Data reduction techniques, as described by Namey et al., 39 were followed, leaving approximately one-third of the collected qualitative data to be analyzed. Participant responses were extracted verbatim; however, brackets were used to ensure clarity of certain narratives. The study coders identified initial codes from each of the respective research question responses; then, each question-specific code was collated into overarching themes across all seven questions. 37
Coders completed a reflexive journal during the analysis process in which thoughts, biases, and assumptions of the data were noted and discussed during subsequent group coding sessions. 36 Coders noted their reactions to participants’ responses that resonated with them. Highlighted reflective journal excerpts can be found in Table 5. Based on the inter-coder agreement, a total of six overarching themes were developed: (1) Strong Black Woman, (2) Oppression/Intersectionality, (3) Medical Mistrust/Mistreatment, (4) Health Literacy, (5) Medical Autonomy, and (6) Cultural Health Factors, with several related emerging subthemes. Researchers report that BFT is an appropriate theoretical framework to utilize when investigating Black women’s lives. In keeping with the core tenets of BFT, highlighted passages reflect similar yet nuanced differences in participants’ understandings of their own lived experiences. 40
Reflexive journal excerpts.

Themes and subthemes
The following participant quotes were used to provide context for the emergent themes. Additional information on the respective themes, subthemes, and related excerpts can be found in Tables 6–8.
Themes central to the identity of Black women: strong Black woman and oppression.

Medical mistrust/mistreatment and health literacy selected quotes.

Medical autonomy and cultural health factors selected quotes.

Strong Black woman
Participants were asked three separate questions regarding media portrayal of Black women and how such portrayal impacts familial conversation about CC prevention behaviors. The most salient portrayal of Black women centered around their strength. The Strong Black Woman (SBW) theme is characterized by culturally specific gendered expectations from Black women that can be perceived as both favorable and unfavorable. The four relevant subthemes of this theme were (1) Independence, (2) Education, (3) Selflessness, and (4) Masculinity. Participants reflected on ways in which the SBW narratives have impacted their lived experiences.
Independence
The portrayal of Black women as being overly self-sufficient was a recurring theme in many participants’ responses. Interestingly, independence was often conceptualized through a dichotomized (i.e., good or bad) and context-specific lens. Specifically, in relationships, independence was seen as a barrier when navigating romantic partnerships but possibly a protective factor within an academic setting. Results indicate the narrative that Black women are immune from needing assistance has a potential impact on overall well-being. In keeping with this theme, participants noted phrases like “overly, or hyper-independent.” Another participant noted,
. . .these characteristics can be damaging because we [Black women] are not seen as needing help and don’t get the help that we [Black women] may need (18-year-old, cis-woman, HPV-vaccine received [completed series], pap-smear not recommended based on age)
Education
Participants reflected on increases in educational attainment and career advancement among Black women, and how being well-educated was a favorable trait. Like prior SBW-related subthemes, there were also contradictory reflections. Participants noted how educational attainment in Black women is sometimes overlooked and undermined by their physical appearances. In keeping with this theme, participants noted phrases as “Black excellence,” “uneducated,” and “ignorant.” Other participant responses exemplifying this narrative include,
I’ve been seeing Black women on a climb up in wealth, schooling, and jobs, being at the top of their class, and graduating early. (18-year-old, cis-woman, HPV-vaccine received [did not complete series], pap-smear not recommended based on age) [Black women] are portrayed as incompetent sexual objects, when we really are smart, more than just a nicely shaped body. (19-year-old, cis-woman, HPV-vaccine received [completed series], pap-smear not recommended based on age) I hate the way we bash and uplift different parts of us. I wish [B]lack women were respected no matter how they are portrayed. (18-year-old, cis-woman, HPV-vaccine not received, pap-smear not recommended based on age)
Selflessness
Several participants reflected on the narrative of Black women prioritizing others before themselves. Other participants’ sentiments related to the dismissal of Black women and being socialized to take a caregiver role suggest that selflessness is a core feature of their identity that is likely to cause mental taxation and viewed as an additional internal struggle. One participant stated,
. . .[B]lack women are always there for those who need it but sometimes it seems like no one is there for [B]lack women. (25-year-old, cis-woman, HPV vaccine not received, pap-smear received [not up to date])
Masculinity
Phenotypical and personality descriptions of the Black women were often reflected as aggressive or having masculine characteristics. In reference to anger, which is often viewed as an unfavorable trait for women, participants noted the unique challenges their marginalized identity created in their personal and professional lives. The media portrayal of Black women as masculine, angry, manly, and aggressive continues to perpetuate the misconception that Black women continue to face interpersonal difficulties due to their “angry and masculine” disposition. One participant noted that,
. . .[B]lack men think that [B]lack woman are “masculine” and aggressive more than any other race. . .it’s really your own people. (18-year-old, cis-woman, HPV-vaccine received [completed series], pap-smear not recommended based on age)
Oppression/intersectionality
The oppression theme is characterized by participants’ descriptions of their experiences marked by unjust treatment and reference to the overlapping and interdependent systems of discrimination. Intersectionality describes the unique oppressive experiences of Black women. 41 The four relevant subthemes include (1) Racism, (2) Sexism, (3) Colorism, and (4) Misogynoir. Participants reflected ways in which “[B]lack women are the most oppressed person [people] in society.”
Racism and sexism
Considering intersectionality and the significant overlap between gender and race, the subthemes of racism and sexism will be described together. Racism describes the endured discriminatory experiences due to participants’ racial identity. Participants highlighted racism in different settings, including churches, work, and schools. The related sexism theme indicates how the media often portrays Black women as inferior compared to men and White women. For many participants, due to their battles with racism and sexism, their authenticity comes at a psychological and potentially physical cost. In keeping with this theme, participants noted phrases like “underdogs” and being seen “in a negative light.” One participant noted,
. . .[Black women] aren’t on the same level as a white person, the media looks at a black person as someone that has to run the extra mile to get to the same spot as a white people [person] that only took two steps to get where they are. (18-year-old, cis-woman, HPV-vaccine received [did not complete series], pap-smear not recommended based on age)
Misogynoir
Misogynoir refers to anti-Black misogyny. Some of the participants’ responses reflected their experiences regarding the intersection of race and gender. Participants noted how anti-Black misogynistic comments come from both non-Black individuals and Black men. Participant narratives also noted situations of internalized misogynoir, suggesting that anti-Blackness from same-gendered and racial peers was another pressing concern. Quotes that exemplify this theme include,
. . .[B]lack men and or non[B]lacks that feel that [B]lack women aren’t worthy of love or should seek love elsewhere. (18-year-old, cis-woman, HPV-vaccine received [completed series], pap-smear not recommended based on age) . . .there is always a negative connotation around them [Black women], and black women are usually the ones who say it.
Colorism
The media portrayal of dark-skinned women as a mere commodity was reflected in some participants’ responses. Specifically, participants highlighted ways in which Eurocentric features are more of a societal preference compared to Afrocentric features. In addition to gender and race, discrimination based on darker skin complexion was another difficult experience among some participants. One participant stated,
The media only portrays Black women with a lighter skin tone and more Eurocentric features (small nose, loosely curled hair, etc) in a positive light and they’re portrayed a lot more. Black women with a darker skin tone or with more Afrocentric (larger nose, more coily or afro hair, etc.) features are portrayed more negatively if they’re even portrayed at all. . . (20-year-old, cis-woman, HPV vaccine status unknown, pap smear not recommended based on age)
Medical mistreatment/mistrust
The third theme was medical mistreatment/mistrust, which reflects negative beliefs and experiences within the healthcare system that add barriers to healthcare access. Contrary to the quantitative assessment of medical mistrust in clinical research, skepticism toward the medical system was a salient concern among many participants. When queried about racial identity in relation to CC prevention behaviors, participants spoke to their increased risk for disparate outcomes and their preference for Black healthcare providers. Additionally, poor patient–provider interaction was another factor that impacted CC prevention adherence. Despite negative experiences, some participants reflected on their resilience and their ability to overcome mistreatment in efforts to prioritize their health. Fortunately, such interactions did not preclude some participants’ ability to engage in health-promoting behaviors. Quotes that exemplify medical mistreatment/mistrust include,
My health care provider is an African American woman it has made me more proud to receive a pap smear without fears of being hurt. (21-year-old, agender, HPV vaccine received [completed series], pap-smear received [not up to date]) It is no mystery how some hospitals may treat [B]lack women. Some believing they have a higher tolerance than others. I am all for a vaccine. But you never know how you will be treated. (21-year-old, cis-gender woman, HPV vaccine received [completed series], pap-smear received [not up to date])
Health literacy
This theme was defined as the ability to find, use, and understand health information. The two related subthemes include (1) Adequate Health Literacy and (2) Inadequate Health Literacy.
Adequate health literacy
Some participants were able to identify the causative agent behind this disease, were knowledgeable about Black women’s heightened risk toward CC, and expressed the importance of engaging in both primary and secondary preventive measures. Other participants highlighted the lack of transparency from their healthcare providers and discussed actions taken to prioritize their health. Quotes used to exemplify health adequacy include,
HPV is so transmittable there is no reason not to get it [HPV vaccine] (21-year-old, gender non-conforming, HPV vaccine received [did not complete series], pap-smear received [up to date]) [HPV Vaccine] it will possibly protect me in the long run. (18-year-old, agender, HPV vaccine received, pap-smear not recommended based on age) As a [B]lack woman, it seems as if I have a higher risk of things wrong when it comes to the medical field, so I get everything I can do to prevent those problems from arising. (21-year-old, agender, HPV vaccine received [completed series], pap-smear received [up to date]) . . .they [Providers] don’t try to warn [B]lack women of preventive measures. . . take steps to ensure my protection. (18-year-old, cis-woman, HPV-vaccine received [completed series], pap smear not recommended based on age) . . .doing more research about providers and . . .need to further research on the topic [CC]. (18-year-old, cis-woman, HPV vaccine not received, pap-smear not recommended based on age)
Inadequate health literacy
Although several participants acknowledged their health, safety, and recommendations from the doctor as primary reasons for getting the vaccine, some participants expressed their aversions and misperceptions of the vaccine. Regarding inadequate health literacy, there were some participants who misidentified the purpose of the HPV vaccine. Limited exposure to CC information was identified as a potential precipitant toward inadequate knowledge. Furthermore, the age of the participants was also highlighted as an obstacle for CC-related conversations with family. Quotes used to exemplify health inadequacy include,
I believe that HPV is given to many of those who receive the vaccine. (18-year-old, cis-woman, HPV vaccine not received, pap-smear not recommended based on age) You’re still a baby. (18-year-old, cis-woman, HPV vaccine received [completed series], pap-smear not recommended based on age) . . .too young to speak in detail about going to the obgyn. (18-year-old, cis-woman, HPV vaccine received [completed series], pap-smear not recommended based on age)
Medical autonomy
Medical autonomy refers to the ability to make one’s own health-related decisions. Due to the recommended age to begin the HPV vaccination series (9 years old), many participants reflected on their limited role in HPV vaccine decision-making. However, some participants chose to obtain the vaccine. Additionally, medical autonomy was precipitated by medical mistrust. Participants reflected on their sense of agency when navigating the healthcare system. The ability to prioritize their health during such a formative period in terms of healthcare utilization served as a protective factor for many participants. Quotes used to exemplify medical autonomy include,
Increased personal health advocacy and importance of communicating with doctors because I know how negatively black women are impacted in the health system. (18-year-old, cis-woman, HPV vaccine received [did not complete series], pap-smear not recommended based on age) I’m always having to ask more questions, get data and statistics on it before I follow through. (19-year-old, cis-woman, HPV vaccine received [completed series], pap-smear not recommended based on age)
Cultural health factors
Cultural health factors include shared attitudes and behaviors in the Black community, including media representation, familial communication, and healthcare navigation that impact health decisions and behaviors. Participants noted that the negative experiences of Black women seen in the media were a contributing factor to their fear of pap smears. The strength of the Black women and poor delivery of health information from providers were identified as barriers when navigating the medical system. Quotes used to exemplify cultural health factors include,
. . .[in the B]lack household it was really rare to discuss anything sexual. (18-year-old, cis-woman, HPV vaccine received [completed series], pap-smear not recommended based on age) . . .[STIs are a] taboo topic that get brushed over by families. . . conversations make the situation worse and could lead to stress in the families. (18-year-old, cis-woman, HPV vaccine received [completed series], pap-smear not recommended based on age) . . .although we are thought to be so strong, I understand that this is not the case when it comes to healthcare and that all issues need to be taken seriously. (18-year-old, cis-woman, HPV vaccine not received [completed series], pap smear not recommended based on age) a [B]lack woman is talked down to or is talked to in a way that goes over her head she may seem like she isn’t supposed to be there. (21-year-old, cis-woman, HPV vaccine received [completed series], pap smear received [not up to date]
In sum, media portrayal and stereotypical narratives among the Black community had an interdependent relationship with participants’ health behaviors and experiences.
Integrated qualitative and quantitative results
Qualitative results complimented the quantitative findings, such that participants’ narratives added additional context to their CC prevention behaviors. Despite a narrative theme of medical mistrust, several participants adhered to HPV vaccination and pap smear guidelines, even following up when results of their pap smear were abnormal or receiving pap smears earlier than recommended. These findings may speak to their resiliency when navigating oppressive medical systems, as evidenced by their commitment to engage in life-saving CC prevention despite their dismissive healthcare experiences.
Furthermore, quantitative findings also indicated a significant lack of CC-related knowledge, specifically as it relates to accurately indicating the purpose of pap smears.
Qualitative findings corroborated the participants’ limited CC literacy, in which participants elaborated on their CC prevention misperceptions. These perceptions included the mis-attributed function of the vaccine and parental beliefs, informing participants own beliefs that their age and sexual activity status (e.g., being too young to have sex) deemed them ineligible to receive the HPV vaccine. Although familial conversations likely informed participants’ current limited CC knowledge, participants’ commitment to exercise their medical autonomy via query of medical providers and other health-information platforms suggests an appreciation for preventive health behaviors.
Discussion
In this study, participants described being inundated with contradictory, stereotypical, and problematic portrayals of Black women in the media, which may have contributed to a “double bind” regarding CC preventative behaviors. Specifically, Black women receive images suggesting that people who look like them are hypersexual, while also receiving messages that CC prevention behaviors are not accessible to people who look like them. 20 Although most participants in the study completed the HPV vaccination series (a STI-related vaccine), they reflected on various challenges grappling with cultural systems that often perpetuate stereotypical narratives of Black women. Participants also attributed their vaccine receipt primarily to caregivers or requirements for school. Pap smear adherence rates in the study are relatively higher compared to data from other studies that prioritize racial/ethnically diverse and college-age populations.13,42 All participants who indicated receiving an abnormal pap test result reported following up with their provider. Participants reported online search engines as their most frequented platform to gather their health information. Additionally, participants’ reflections corroborated findings in the current literature in which identifying as an SBW can serve as a protective factor, increasing self-efficacy and self-preservation,43,44 in that participants discussed increased health self-advocacy in the form of research and asking questions of providers.
Participants in the present study surpassed the current national HPV uptake average of 40% among young adults; 45 however, this elevated rate of HPV uptake may be explained by protective factors mentioned by participants, including maternal education status, personal educational attainment, and health insurance. 1 Considering the recommended age to begin the HPV vaccination series (9 years old), unsurprisingly, the participants indicated that uptake of this vaccination was largely the decision of their parents/guardians or a requirement for school. In an effort to leverage the benefits of parental/guardian awareness of HPV, global interventions have been implemented to educate parents about HPV/CC46,47 with a particular focus to create culturally tailored interventions for racial/ethnic, high-risk populations.48,49
Despite most study participants reporting provider HPV vaccine recommendation and acknowledging uptake of at least 1 dose of the HPV vaccine, some reported not receiving any vaccines in the series. Perceptions of vaccine ineffectiveness, insufficient information to make informed decisions, and uncomfortable encounters with healthcare professionals are health stymieing factors highlighted by the participants and corroborated in other qualitative studies that used a predominately Black women sample.41,50,51 While all age-eligible women received a pap smear in their lifetime, not all indicated receiving a pap smear within the past 3 years as USPSTF recommended. It was encouraging that, despite inappropriate follow-up to abnormal pap tests being a known driver for increased CC mortality among Black women, 52 all participants who indicated receiving an abnormal pap test result reported following up with their provider. As previously mentioned, participants’ high rates of insurance coverage, individual/maternal educational attainment, and increased self-advocacy likely served as health-promoting factors that are also well documented in cancer prevention literature.53,54
Despite social media serving as a popular health promotional tool among young adults, 55 most participants reported social media as their least frequented platform to gather their health information. Although social media can be helpful for disseminating cancer prevention education, some media can exhibit problematic and prejudiced themes that reinforce the objectification of Black college students and center lived experiences of White individuals. 56 Given the resulting psychological harm when exposed to such objectification, including low self-esteem,57,58 participants reported preference for Google and other online search engines can be considered protective.
The different types of oppressive experiences endured by the Black female collective and unjust experiences navigating the medical system were highlighted in several participants’ responses. Despite personal experiences with disparate treatment and mistreatment compared to their racial/gender counterparts, participants recounted how such injustices seemingly catalyzed their sense of resiliency and contributed to their sense of identity, including being a SBW. Participants in the present study reflected on how adhering to this archetype is both an asset and a liability, which is consistent with existing literature.59,60 Furthermore, Black women’s ability to reconceptualize unhelpful racially gendered stereotypes (e.g., hypersexuality of Black women) has been proposed to increase sexual health outcomes, in which STI prevention is reframed as liberating and empowering, as opposed to a solely risk-reduction behavior. 61
Clinical implications
Findings indicate that low CC knowledge remains a significant issue among undergraduate Black women. Given that CC is one of the few preventable cancers, educational interventions should use media and community spaces (e.g., historically Black colleges and universities (HBCUs), Black churches) for accurate prevention messaging, remaining mindful of the presence of diverse and often contradictory messages received online. Importantly, undergraduate institutions have an integral role in both pap smear and HPV vaccine uptake. As most students are required to have university-issued or private health insurance, students enrolled in higher education institutions have reduced barriers to accessing CC prevention services. Notably, HBCUs experience disparate access to CC screening services compared to predominantly White institutions. 62 Combined with the heightened risk for CC among Black women, the allocation of associated screening resources should prioritize HBCUs to reduce CC disparities.
Limitations
While Black women college students are a developmentally and culturally important group to prioritize in terms of CC prevention, findings from the study cannot be generalized to the larger Black female community. The primary recruitment source of undergraduate freshmen yielded a smaller sample of pap-smear-eligible participants. Furthermore, participants reported maternal educational status (a proxy for SES) was generally high and yielded a restricted range of maternal educational attainment. Future research should make concerted efforts to recruit a more representative sample of Black college women over 21, and with a wider range of SES, to get a better understanding of their perspective on CC prevention. Additionally, future studies should include similarly aged women who are not attending college, HBCU students, unvaccinated, uninsured women, women with lower SES, women at mid-life, and older adult women.
Due to the unique challenges gender and sexually marginalized populations face, 63 future studies should also prioritize these understudied populations who may face more barriers to healthcare access. It may also be interesting to query more directly about the unique role of universities and explore the ways in which enhanced student understanding of the HPV vaccine can be a catalyst to improving prevention/treatment uptake for other STI-related chronic conditions.
Call to action
Given that CC is one of few preventable cancers that disproportionately affect Black women, it is important to broaden our understanding of how the lived experiences of Black women, including the exposure to anti-Black racism and sexism, continue to perpetuate this disparity. Focusing on and amplifying sociocultural aspects and strategies that enable Black women to maintain a healthy sense of self, including self-advocacy and validation of their discriminatory experiences, warrants greater attention utilizing both quantitative and qualitative research methods.
Conclusion
Prevention and early intervention via vaccination and pap smears are vital to reducing CC rates. Despite having the second highest incidence of CC due to the high incidence of HPV, Black women have low utilization of preventative measures. Findings from the study yield educational attainment, resiliency from racially/medically oppressive experiences, and positive beliefs toward CC prevention behaviors as facilitators to CC prevention behaviors among young Black women. Given the large preference for online health-information among young adults, and the known negative media portrayal among Black women, digital interventions must utilize culturally sensitive messaging to avoid the internalization of misogynistic stereotypes and increase pap smear receipt and HPV vaccination uptake.