
Abstract
Background:
Research suggests women feel there is a lack of information and support around menopause leading them to be unprepared for the transition. Menopause care requires the practitioner to provide women with accurate information regarding symptoms and treatment. Advanced nurse practitioners (ANPs) have been found to have the knowledge and skills to provide high-quality, safe, individualized holistic healthcare. An ANP-led menopause clinic was established following intense mentorship/competency assessment and completion of industry standard courses to ensure evidence-based best practice.
Objectives:
To evaluate any change in quality of life (QoL) and menopause symptoms of patients pre- and post-education and initiation of menopause hormonal treatment (MHT) using the QoL assessment tool, the Greene Scale in an ANP-led menopause clinic.
Design:
This interventional study was carried using GUIDED, Guidance for reporting intervention development studies in health research. This quantitative audit used the Greene Scale tool to measure symptoms and QoL before and after the appointment with the ANP.
Methods:
A search of the patient database was conducted to identify patients returning for the 3-monthly review post initial consultation and initiation of MHT (n = 15). Data were collected on the modified Greene Scale instrument. The sample was randomly selected by identifying every second patient on a single medical surgery database. Statistical analysis was ascertained utilizing central tendency excel functionality. The statistical significance of the data was assessed using a two-tailed paired t-test. p-values of less than 0.05 were considered statistically significant.
Results:
An ANP-led menopause clinic in accordance with evidence-based guidelines, including education and treatment improved the overall QoL to a statistical significance. In addition, menopausal symptom reduction occurred in all 20 symptoms as measured in the modified Greene Scale, 19 of which to a statistical significance.
Conclusion:
The study revealed an improvement in QoL and menopausal symptoms in an ANP-led menopause clinic. ANP-led menopause clinics could be a great addition to the workforce providing patients with timely menopause care. Further studies could build on this analysis by including other variables such as comorbidities, demographics, and patient’s perspective.
Plain language summary
Women feel there is a lack of menopause information and support. Menopause care needs practitioners who can provide accurate facts on symptoms and treatment. Advanced Nurse Practitioners have the knowledge and skills to provide high quality, safe, individualised care. An ANP led menopause clinic was set up after the ANP completed menopause courses and mentorship. A study was undertaken to assess the impact on quality of life (QoL) and menopause symptoms before and after attending the ANP menopause clinic. The information was collected using a menopause symptom assessment tool, called the Greene scale. The information was analysed using both excel and a two tailed paired t test. The ANP led menopause clinic improved the overall quality of life to a statistical significance and reduced menopausal symptom in all 20 symptoms assessed, 19 symptoms were reduced to a statistical significance. ANP led menopause clinics could be a great addition to the workforce providing patients with timely menopause care. Further studies could provide more information including co-morbidities, demographics and patient’s perspective.
Introduction
Menopause is defined as the last menses, with perimenopause being the time leading up to the final menses and post-menopause being 1 year since the last menstrual period.1 –3 The average age of menopause is 51, 4 with the average life expectancy of a woman in Europe being 82 years, 5 meaning, women are spending approximately a third of their life in menopause. 4 The depletion of estrogen can lead to women experiencing a vast array of symptoms including hot flushes, night sweats, lethargy, sleep disturbance, depression, cognition impairment, decreased sex drive, joint and muscle pain, and genitourinary issues that is, vaginal dryness, dyspareunia, and recurrent urinary tract infections, 6 leading to a decrease in quality of life (QoL). While media attention for menopause has grown in recent times, women remain feeling unheard.
A survey of 1132 women carried out in Ireland in 2020 revealed that 80% of women were unprepared for menopause. About 79% of the women surveyed felt that information and support surrounding menopause was poor, and almost 50% did not feel confident discussing menopause with their General Practitioner (GP). 7 Bacon 8 stated, “a clear understanding of the physiology of the menopausal transition, clinical symptoms, and physical changes is essential for individualized patient management, maximizing benefits and minimizing risks for the present and the future.” Knowledge and treatment of menopause is an area not always understood by clinicians. 9 Lin et al. 10 demonstrated menopause training gaps led to half of healthcare professionals studied not being aware of contra-indications to prescribing menopausal hormonal treatment (MHT). With doctor shortages and increase demand for menopausal treatment, advanced nurse practitioner (ANP)-led clinics could be valuable additions to the workforce and improve access to care. 11
The International Menopause Society 1 and NICE guidelines 3 recommend that menopause management needs an individualized approach, requiring the practitioner to have extensive knowledge on assessment, investigations, and ANP as “A generalist or specialist nurse who has acquired, through additional graduate education (minimum of a master’s degree), the expert knowledge base, complex decision-making skills, and clinical competencies.” 12 The ANP-led menopause clinic was established after intense mentorship with GPs (special interest in menopause) and completion of courses with the British Menopause Society and the International Menopause Society to ensure evidence-based and best practice be provided. Alexander and Moore 13 found that nurse practitioners had a significant role in patient assessment, patient interaction, and management leading to overcoming bothersome menopausal symptoms that affected women’s QoL.
Objective
The objective of this research is to audit QoL and menopausal symptoms after 3 months of menopause hormonal treatment (MHT) following the establishment of an ANP-led menopause clinic using the QoL tool, the modified Greene Scale. 14
Design
This article was a quantitative audit using the Greene Scale tool to measure symptoms and QoL before and after the appointment with the ANP. Patient variables were not included at this stage of the study.
Methods
This interventional study was carried out using GUIDED, Guidance for reporting intervention development studies in health research. The information for this study was collected from January to April 2022. Women were asked to complete the Greene Scale questionnaire before the initial menopause appointment and prior to commencement of MHT and again 3 months post-treatment in a single General Practice Surgery in urban Dublin. The questionnaires were retrospectively, systematically, and randomly selected by choosing every second patient on the health one database (n = 15). The women ranged from 46 to 56 years, mean age (n = 50; SD = 2.84).
The menopause clinic instigated an initial appointment time between 30 and 40 min, which differed from the previous 10-min slot, which did not allow for adequate education be provided. The ANP addressed patient education including definitions of menopause, symptoms, impacts to patient, partner, family, work, and social interaction. Lifestyle advice was provided by way of diet, exercise, and psychological interventions (such as CBT/Yoga). Contra-indications and risk factors were addressed. The ANP carried out a breast check, routine bloods, blood pressure, weight, height, and BMI. Finally, treatment options were discussed in depth: MHT or other.
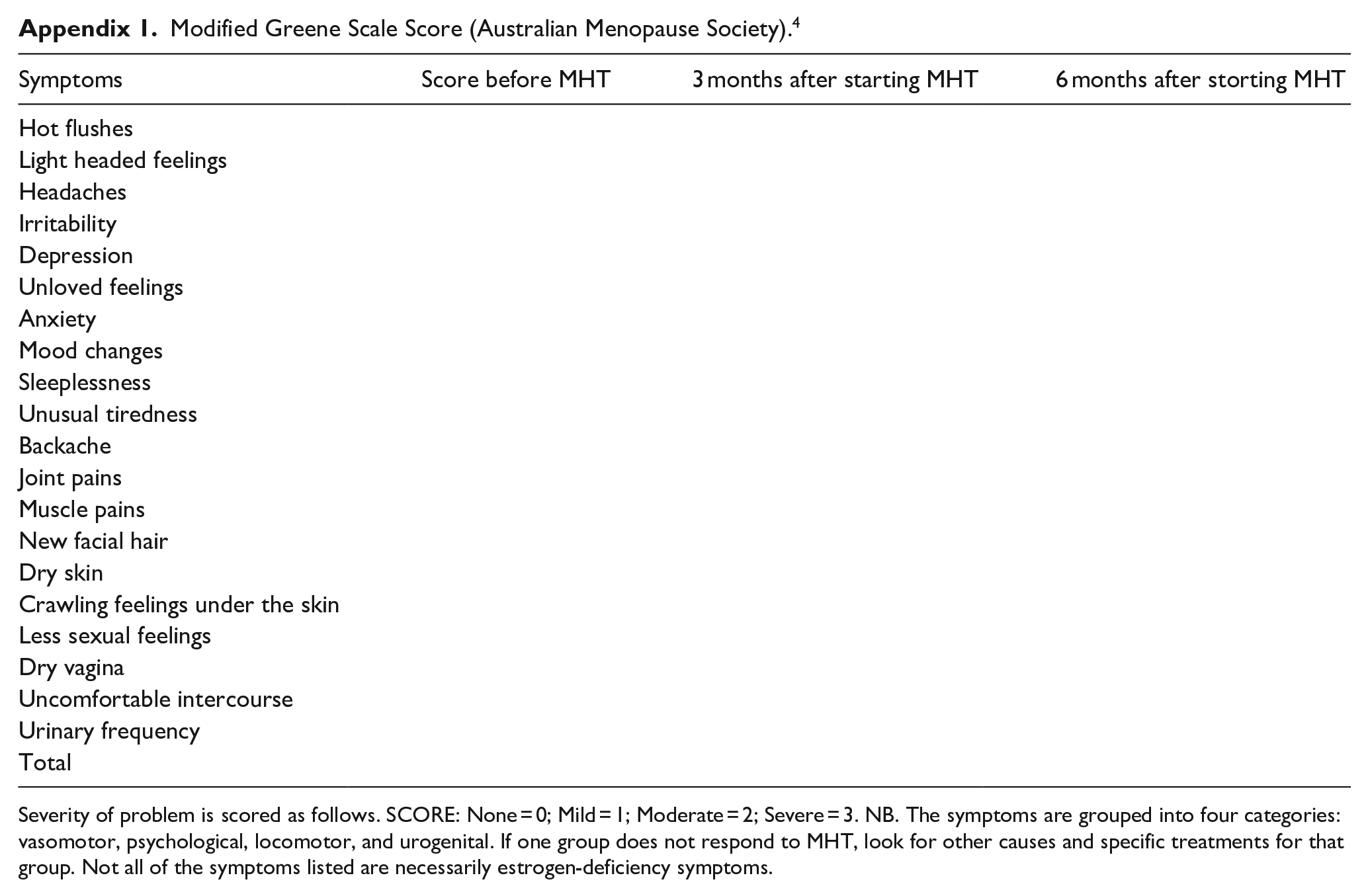
The patient completed a modified Greene Scale form (QoL tool) before the appointment (Appendix 1); this provides the basis of the conversation regarding symptoms and what the patient hopes to get out of the consultation. NICE 15 referred to health-related QoL as “a combination of a person’s physical, mental and social well-being; not merely the absence of disease.” QoL assessment tools are used to identify patient needs and assess the efficacy of an intervention. 16 The QoL tool used consists of 20 menopausal symptoms which are graded on a Likert scale from 0 to 3 (3 being most severe), a score of 12–15 is considered estrogen deprived. 14 The higher the score, the lower the QoL. 17 As women live up to a third of their lives post-menopausal, the assessment of menopauseal symptoms and QoL in menopausal women should be of great public-health interest. 18 The Greene Scale 19 is a valid and reliable method of measuring menopausal symptoms and QoL20 –22; the scale used in this report is a modified Greene Scale from the Australian Menopause Society. 14 At the end of the consultation, a collaborative treatment plan is agreed and if appropriate MHT is initiated. Collaborative care has been shown to improve communication, patient understanding, QoL, patient satisfaction, and reduction in medication errors.23,24 The first follow-up appointment, which lasts 20 min is at 3 months, after which appointments are 6 monthly unless the patient requests an earlier review due to increase in symptoms or side effects. The follow-up for all patients included in the study was 3 months.
The treatment received was estrogen via either transdermal patch or gel with the progesterone component being delivered via “Mirena” intra-uterine devise (IUD) or combined in patch or orally (micronized progesterone), in line with evidence-based guidelines incorporating patient preference. Patient involvement in treatment decision-making leads to patient empowerment and better outcomes.25,26 Transdermal hormonal treatment is the safest form of MHT from a venous thromboembolism (VTE) perspective. 27 Transdermal estrogen with micronized progesterone reduces VTE risk, cardiovascular risk, and cholecystitis, while also having a neutral effect on blood pressure when compared to synthetic progestogens.28,29 Synthetic progestogens, found in oral MHT and combined patch have a slightly higher clot and stoke risk; this is avoided by using micronized progesterone. 30 The use of “Mirena” IUD as the progesterone component provides the patient with added benefits such as contraception and often better bleeding patterns. 31
This study included n = 15 participants. A sample size of n = 12 was calculated based on 99% responsiveness due to the nature of study, using the number of patients in the menopause clinic as the population (n = 50) with confidence level 95% and margin of error of 5%. 32
Statistical analyses were conducted using a two-tailed, paired t-test, p-values of less than 0.05 were considered statistically significant. A summary of findings was produced using the central tendency functionality in Excel.
Patient participation and consent was not required as part of this pilot study, the Greene score before and after scores were compared to establish improvement in symptoms and QoL.
Ethics approval was not obtained as per the Health Research Authority, which coordinates and regulates ethical approval of research involving human subjects, specifically excludes projects from requiring ethical approval if they fall into the categories of clinical audit, service evaluation, research, and usual practice/surveillance work in public health, which this pilot study was deemed to have met. https://d7g406zpx7bgk.cloudfront.net/x/832fac1a65/gdpr_assessment_table_-_clinical_audit.pdf
Statistical analysis/results
The results of the two-tailed paired t-test revealed a statistically significant improvement in overall QoL (p < 0.001). Individual analysis of the symptoms showed an improvement in all symptoms with 19 of the 20 improving to a statistical significance (Table 1).
Two tailed paired t-test.

NS: not statistically significant.
Mean values and standard error of the mean (SEM) of the Greene scale scores at baseline and 3 month follow-up.
A summary of findings demonstrated on average each person was likely to experience 14 symptoms with an average severity of 1.97 per symptom prior to MHT, and this was reduced to an average of 8 symptoms with a severity index of 0.74. Out of 20 potential associated symptoms 2 were experienced in 100% of cases (irritability and sleeplessness), and a further 15 symptoms were experienced in more than 50% of the patients (hot flushes, lightheaded feelings, depression, unloved feelings, anxiety, mood changes, unusual tiredness, backache, joint pains, muscle pains, new facial hair, dry skin, less sexual feelings, dry vagina, urinary frequency). About 11 out of these 17 most prevalent symptoms experienced a severity score of 2 or higher (hot flushes, irritability, depression, unloved feelings, anxiety, mood changes, sleeplessness, unusual tiredness, joint pains, crawling feelings under skin, less sexual feelings). MHT improved the severity of symptoms by over 50% in 10 out of these 11 (or 91%) of patients with the most prevalent and severe symptoms (Table 2). The top six most prevalent symptoms were present in over 85% of patients, and the severity of these symptoms was greatly reduced post-MHT.
Irritability (prevalent in 100% of patients) severity was reduced by 62%.
Sleepless (prevalent in 100% of patients) severity was reduced by 59%.
Mood changes (prevalent in 93% of patients) severity was reduced by 52%.
Unusual tiredness (prevalent in 93% of patients) severity was reduced by 72%.
Depression (prevalent in 87% of patients) severity was reduced by 81%.
Hot flushes (prevalent in 87% of patients) severity was reduced by 85%.
Percentage improvment.


Red = above 50% prevalence Orange = Greene score above 2 Green = above 50% improvment.
The remaining symptoms all show improvement in severity, ranging from dry skin at 33% to crawling feeling under the skin severity reduction of 71% (Table 2).
Further analysis revealed a percentage reduction in symptoms ranging from 33% to 98%, averaging a 60% reduction in symptoms (Figure 1). This overall reduction in symptoms demonstrates the value of an ANP-led menopause clinic.
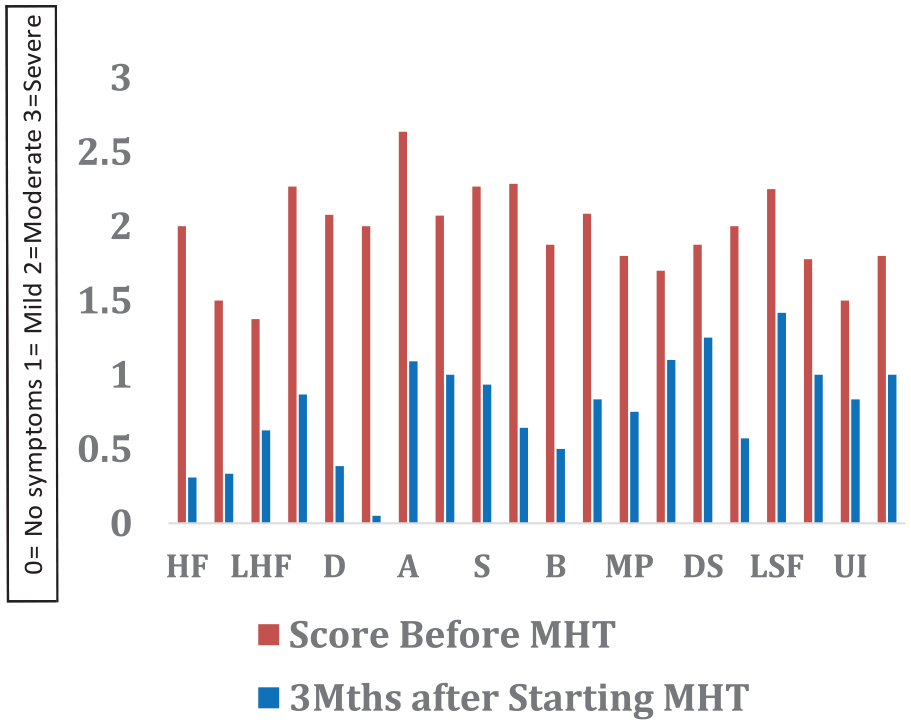
Bar Chart.
Discussion
This small-scale study is in keeping with results found by Martins et al. 33 where body identical HRT demonstrated an overall improvement in both symptoms and QoL of menopausal women and provides a snapshot into the benefits of ANP-led menopause care. There is a dearth of studies in this field, with only two articles located as part of this research. The first in 2007 34 with findings highlighting ANPs ability to provide individual care for menopausal patients. The second focused solely on ANP management of Genito-urinary syndrome of the menopause (GSM), the findings revealed the integration of patient education, counselling, holistic care, and shared decision-making, ideally places ANPs in a role to maximize women’s health. 35
Strengths
This study was conducted using GUIDED, Guidance for reporting intervention development studies in health research, promoting transparency and improving the quality of the reported intervent. 36 The systematic random selection process was chosen due to simplicity, time efficiency, and its reduction of intentional or unconscious bias. 37
The results of the two-tailed paired t-test demonstrated an overall improvement in QoL of menopausal women to statistical significance. The two-tailed paired t-test analysis of each symptom demonstrated an improvement in all 20 symptoms with 19 improving to statistical significance. Santoro et al. 38 stated the importance of clinicians to identify early symptoms of menopause and initiate treatment to reduce same. This is also echoed in a retrospective study on how menopausal symptoms impacted well-being, finding that there was a significant negative impact on mental health and overall QoL when not treated. 39
While the study is retrospective, the data were recorded at the time of appointment eliminating patient recall bias. Measurement bias can occur due to the assessment methodology being self-reporting 40 ; however, the use of a reliable and validated QoL tool (Green Scale) reduced this risk.
The follow-up for all patients included in the study was 3 months with zero dropouts and all patients completing the pre- and post-QoL questionnaires.
Limitations
As this was a pilot study with a small sample size and conducted in one clinical setting, the representativeness and generalizability of the study are limited. The follow-up data were collected at 3 months, limiting ability to make longitudinal conclusions.
However, this data could lay the foundations for large-scale, longer studies with an increased sample size and multiple clinics.
While the sample size was small, it was selected randomly and provided a timely, reliable method to audit the effect of a newly established ANP-led menopause clinic.
This article did not review peri/post-menopausal women using testosterone. Testosterone is an often-overlooked hormone in women, 41 and deficiency can lead reduced libido. 42 NICE 3 advised testosterone can be added to MHT should estrogen and progesterone not be sufficient in improving libido. Further studies including testosterone would be beneficial in assessing all aspects of QoL including sexual desire.
Patient demographics/variables (with exception of age/gender) were not recorded as part of this study. Future studies, including income, education, occupation, family structure, and medical conditions, could reduce confounding bias, 43 while providing stakeholders with valuable information regarding the provision of menopause care and further demonstrate the need for individualized care as recommended by Thuraisinghan and Nalliah. 44
Conclusion
The objective of this interventional study was to ascertain the impact of an ANP-led menopause clinic on QoL and symptoms among peri/post-menopausal women using evidence-based guidelines. Results from the two-tailed paired t-test demonstrated a statistically significant improvement in QoL. All 20 of the symptoms revealed a reduction with 19 of the 20 reaching statistical significance. Further analysis revealed a reduction in individual symptom’s severity ranging from 33% to 98%, highlighting the overall benefits to the patients and the positive impact of the ANP-led menopause clinic. ANPs are ideally placed and are trained to treat patients holistically, addressing not only their medical requirements but also educational and emotional needs; this approach potentially contributes to better patient engagement and improvements to menopausal QoL outcomes. However, due to the limitations of the study, further robust research justified, across multiple clinics, using larger sample sizes with longer follow-up, and the inclusion of patient demographics to influence key stakeholders in the potential investment in ANP-led menopause clinics.
Footnotes
Appendix
Modified Greene Scale Score (Australian Menopause Society). 4
| Symptoms | Score before MHT | 3 months after starting MHT | 6 months after storting MHT |
|---|---|---|---|
| Hot flushes | |||
| Light headed feelings | |||
| Headaches | |||
| Irritability | |||
| Depression | |||
| Unloved feelings | |||
| Anxiety | |||
| Mood changes | |||
| Sleeplessness | |||
| Unusual tiredness | |||
| Backache | |||
| Joint pains | |||
| Muscle pains | |||
| New facial hair | |||
| Dry skin | |||
| Crawling feelings under the skin | |||
| Less sexual feelings | |||
| Dry vagina | |||
| Uncomfortable intercourse | |||
| Urinary frequency | |||
| Total |
Severity of problem is scored as follows. SCORE: None = 0; Mild = 1; Moderate = 2; Severe = 3. NB. The symptoms are grouped into four categories: vasomotor, psychological, locomotor, and urogenital. If one group does not respond to MHT, look for other causes and specific treatments for that group. Not all of the symptoms listed are necessarily estrogen-deficiency symptoms.
Acknowledgements
Dr Jarlath Varley RCSI, Dr Alan Byrne Scholarstown Family Practice and Dr Anya Bowers.