
Abstract
Background:
Primary dysmenorrhea (PD), menstrual pain in the absence of pathology, is the main cause of gynecological consultation in young women. There are many studies that suggest a possible relationship between a low level of physical activity (PA) and a greater intensity of menstrual pain, and others that find no relationship between these variables.
Objectives:
To identify the level of PA and menstrual pain intensity among women with PD, as well as the relationship between these variables.
Design:
An observational, cross-sectional study was carried out on a cohort of adult population.
Methods:
Data collection instrument was an online self-administered questionnaire. Main variables were pain intensity (Numeric Rating Scale; McGill Pain Questionnaire, short version) and PA level (International Physical Activity Questionnaire).
Results:
A total number of 216 responses from the total responses obtained were considered PD cases. A 38% of women did not perform any intense PA during the last 7 days, and a 32.4% did not perform any moderate PA. No significant differences were found in menstrual pain intensity during the three last menstruations among women who performed PA, moderate, or intense. Nor were significant differences found between women who performed PA less than 3 days a week, compared with those ones who did it at least three times a week, or more.
Conclusion:
Menstrual pain intensity does not differ between the types of PA. A large number of participants did not perform any PA in the last 7 days.
Background
Dysmenorrhea, cyclic menstrual pain, is the leading cause of chronic pelvic pain, according to the World Health Organization. 1 It represents the leading pathology of gynecological morbidity in women of reproductive age,2,3 regardless of age, nationality, and economic status.3 –5 The most common clinical presentation of dysmenorrhea is recurrent, jerking abdominal cramps and suprapubic pain. There are two types of dysmenorrhea, primary and secondary. Secondary dysmenorrhea is menstrual pain caused by an identifiable pathology. 6 Primary dysmenorrhea (PD) is menstrual pain that occurs in the absence of an underlying pathology.2,6 –8 The cause of PD is not fully accepted, although the most-supported hypothesis is an increased hormonal production of prostaglandins that promote uterine ischemia and uterine contraction, such as PGF2α. 9
There are a series of risk factors that could increase the possibilities of suffering PD and the severity of its symptoms.2,7,10 –12 These include psychological factors (anxiety, depression, stress),52,54 demographic factors (family history of dysmenorrhea),4,11,13 –15 lifestyle factors (smoking, alcohol consumption, diet, and physical activity (PA)),10,11,16,17 reproductive factors (menorrhagia, early menarche, and long or irregular menstrual cycle),18,52,54 and clinical factors (weight, age, and nulliparity).12,16,19 –21
There are numerous studies that link the breakdown of the social support network and anxiety, depression, or stress with PD.4,5,10,11,13,22 There is a controversy about the relationship between smoking and body mass index (BMI), since some studies indicate that a high BMI could be related to a more acute clinical picture of PD, even if this habit is current or has been present in the past.5,22,23 Other studies maintain that this relationship is not statistically significant 24 or would be related to a low BMI.16,21,23 Caffeine, theine, and chocolate consumption appear to be associated with an increased risk of PD, 11 although further research is needed to determine the influences of diet on the PD picture. 11
Long, irregular, and heavy menstruation, as well as a family history (especially close kinship), would increase the likelihood of developing PD.4,10,24 –27 Early menarche, before the age of 12 years, and being nulliparous, seems to increase its frequency.10,11,24,25 Scientific literature suggests that a low educational level, the breakdown of the social support network, alcoholism, the presence of associated pathologies, and reduced PA are associated with PD.10,11,22,25,28
Despite the identification of these risk factors, further research is needed to learn more about the relationship between these elements, their interaction with genetic factors, and the patient’s environment.3,11,27 The processes of interaction between the factors can be complex and modifiable. They are not completely clarified in the scientific literature.10,29
Exercise therapy in PD is a technique recommended in clinical practice guidelines.30 –33 It can be effective in relieving pain, improving the level of stress, and reducing medication intake and absenteeism from work and school. But there are still aspects, such as the most appropriate type of exercise or dosage, that must be clarified. 44 A larger number of studies with higher quality are needed to identify these aspects.30,33,34 A relationship has been found between a low level of PA and a greater possibility of suffering PD.30,35 There is another study that identifies that there is no relationship between low-level PA and PD. 36 To the knowledge of this research team, this is the first study that details in a more detailed way the PA performed by women than in other existing studies in the literature.
There were weak indications that exercise performed for approximately 45–60 min each time, at least three times per week, regardless of intensity, may provide a significant reduction in menstrual pain intensity (Visual Analogic Scale, VAS or MPQ). 33 Following PA, the overall effect is an increase in antinflammatory cytokines (interleukin-10) and a decrease in proinflammatory cytokines (interleukin-6 and tumor necrosis factor-alpha) which are responsible for pain reduction. Aerobic exercise relieves PD-associated pain through inflammatory cytokine-mediated mechanisms.9,37 Pain reduction is related to the release of endogenous opioids, a reduction in the level of PGF2α, and a decrease in the level of stress.30,37,38 These mechanisms are present during exercise and in the postexercise period. Mobilization can generate proprioceptive stimuli in nonnociceptive periarticular sensors (A-beta fibers) and promote pain modulation in the spinal cord, via the release of endogenous opioids.30,37,38
Following the International Physical Activity Questionnaire (IPAQ), vigorous physical activities refer to activities that take hard physical effort and make breathe much harder than normal. Moderate activities refer to activities that take moderate physical effort and make breathe somewhat harder than normal. Sedentary behavior include time spent at work, at home, while doing course work and during leisure time. This may include time spent sitting at a desk, visiting friends, reading or sitting or lying down to watch television.
This study is necessary to identify the intensity of menstrual pain during the last menstruation and the last three menstruations in women with dysmenorrhea. Also, to clarify the average level of PA that these women usually have, as well as to identify the existence or not of a relationship between these variables. These are aspects that are missing in some scientific research on dysmenorrhea and its approach through therapeutic exercise.
The goals of this study are to identify the level of PA and menstrual pain intensity among women with PD, as well as the relationship between these variables.
Method
Design
This manuscript followed the guidelines from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) conference list. 39 An observational, cross-sectional study was carried out from July 2020 to December 2022.
Selection criteria are based on scientific literature. The inclusion criteria were nulliparous women, aged between 18 and 25 years (age group with the highest PD incidence and most exacerbated clinical manifestations6,7,24,40), regular menstrual cycles (between 21 and 35 days34,41 –43), and score of at least 4 on a Numeric Rating Scale (NRS), on average in the last three menstrual periods.43,44 The exclusion criteria were consumption of oral contraceptives, use of an intrauterine device, previous pelvic surgery, or gynecological pathology.9,11
Participants themselves marked this option in the questionnaire. If they did so, they were redirected to the end of the questionnaire.
For the sample calculation, the number of women enrolled in undergraduate, postgraduate, or doctoral studies between 18 and 25 years of age at the University of A Coruña was obtained. In addition, the prevalence of PD, estimated by Fernández-Martínez et al., 45 of 76% in the Spanish female university population, was taken into account. A sample size of 189 questionnaires was established. The significance level was 5%, and the statistical power was 95%. The following formula was applied for the sample calculation in finite populations 46 :

An initial pilot study was carried out, which was followed by the main study. The pilot study was conducted on a sample of 48 people, and a total of 41 responses were obtained (81.4% of the total). In the main study, a total of 736 responses were obtained. Of these, 216 were considered PD cases since they met the established inclusion and exclusion criteria and were analyzed (Figure 1).

Flow chart of selection process of participants.
This study ensured compliance with ethical principles and legal regulations related to research. Compliance with the standards of good clinical practice and the ethical principles proposed in the Declaration of Helsinki, of the World Medical Association (Finland, Helsinki, 1964) was assumed.
Procedures
The data collection process was conducted by completing a self-administered questionnaire on an online platform (Microsoft Forms). The questionnaire used was obtained after having conducted a Delphi methodology and a pilot study. Potential participants received information by email, and they voluntarily decided to participate. For this, it was necessary to sign the informed consent.
Pain intensity was obtained using the NRS. Each participant indicates on this line the intensity of the perceived pain. The higher the score, the greater the intensity of pain. 47 Description, location, and perception of pain were obtained using the Short Form MacGill Pain Questionnaire (SF-MPQ).47,48
The analysis of moderate and intense PA (IPA) was carried out according to the interval of days in which these were performed, per week. World Health Organization instructions were followed. 49
Statistical analysis
A formula for sampling calculations in finite populations was used. A sample size of 189 questionnaires was developed. Statistical analysis was performed using SPSS statistical software (V. 23.0; IBM Corporation, Armonk, NY, USA) and R (version 4.1.0; R Core Team, 2019). 50 For multiple response variables, the database was recoded using R statistical software. A descriptive analysis was carried out on all the variables included in the study.
A Mann–Whitney U test was performed to test whether there were differences in pain intensity depending on medication consumption and smoking habit. The alpha significance level was set at 0.05.
Outcome measure
Pain intensity was obtained using the NRS, where each participant indicated on this line the intensity of the perceived pain. The higher the score, the greater the intensity of pain. 47 Description, location, and perception of pain were obtained using the SF-MPQ questionnaire.47,48 In this study, the results of pain descriptors used in the questionnaire and their scores are presented.
IPAQ contains questions about the level of PA during the 7 days prior to filling in the questionnaire. Information was obtained on the number of days and minutes that the person spent doing activities of moderate intensity, vigorous intensity, walking, and sedentary lifestyle (number of hours sitting). The score obtained allowed the level of PA to be classified as low, moderate, or high. To calculate it, weekly activity was recorded in METs (metabolic equivalent of task or metabolic index units) per minute and week, according to the reference values of the activities (walking: 3.3 METs; MPA: 4 METs; IPA: 8 METs). To obtain the number of METs, each one of the values for the time in minutes of carrying out the activity in a day and for the number of days per week.33,44,51
Results
Flow of participants
A total of 736 responses were obtained. Of these, 216 (29.34%) were considered PD cases since they met the established inclusion and exclusion criteria. A total of 86.6% of the women (186 women) were bachelor students, 12.5% master students (27 women), and 1.9% PhD students (4 women).
Table 1 shows demographic characteristics of the study sample and data about PA.
Demographic characteristics of the sample and physical activity data.

IPA: intense physical activity; MPA: moderate physical activity.
The number of days in the last seven (at the moment of filling up the questionnaire) was IPA or moderate PA (MPA) that was performed is also shown. The minutes per day referred to IPA or MPA are related to days each was performed.
The high number of women who does not carry out any type of IPA in the last 7 days stands out (38%, 82 women). In the same direction, 32.4% of women (70 women) did not perform any MPA in the last 7 days. In relation to sedentary behavior in the sample, it is worth noting that 17.1% of women (37 women) indicated spending 8 h in a sitting position per day. Likewise, 17.1% of women (37 women) indicated spending 6 h in a sitting position per day. The mean was 7.21 (standard deviation (SD) = 3.33). The median was 7 h (interquartile range (IQR) = 60).
On the other hand, 38.4% of women (83 women) walked at least 10 min continuously in the last 7 days.
In this study, IPA was considered lifting heavy weights, digging, aerobic exercises, riding a fast bike (static), or similar activities that raised your breathing intensely, according to IPAQ. MPA was considered carrying lightweights, riding a (static) bicycle at regular speed, or similar. Activities that elevated your breathing above normal, but it did not include walking.
Figure 2 shows the frequency distribution with percentages of pain intensity during the last three menstruations.

Frequency of pain intensity during last three menstruations.
Pain intensity during the last three menstruations was not significantly different (Mann-Whitney U test = 5039; p = 0.465) in those women who performed MPA less than 3 days a week (M = 6.75; SD = 1.30; Median = 7; IQR = 2), compared to those who did do it for at least 3 days a week or more (M = 6.91; SD = 1.44; Me = 7; IQR = 2) (Figure 3(a)).
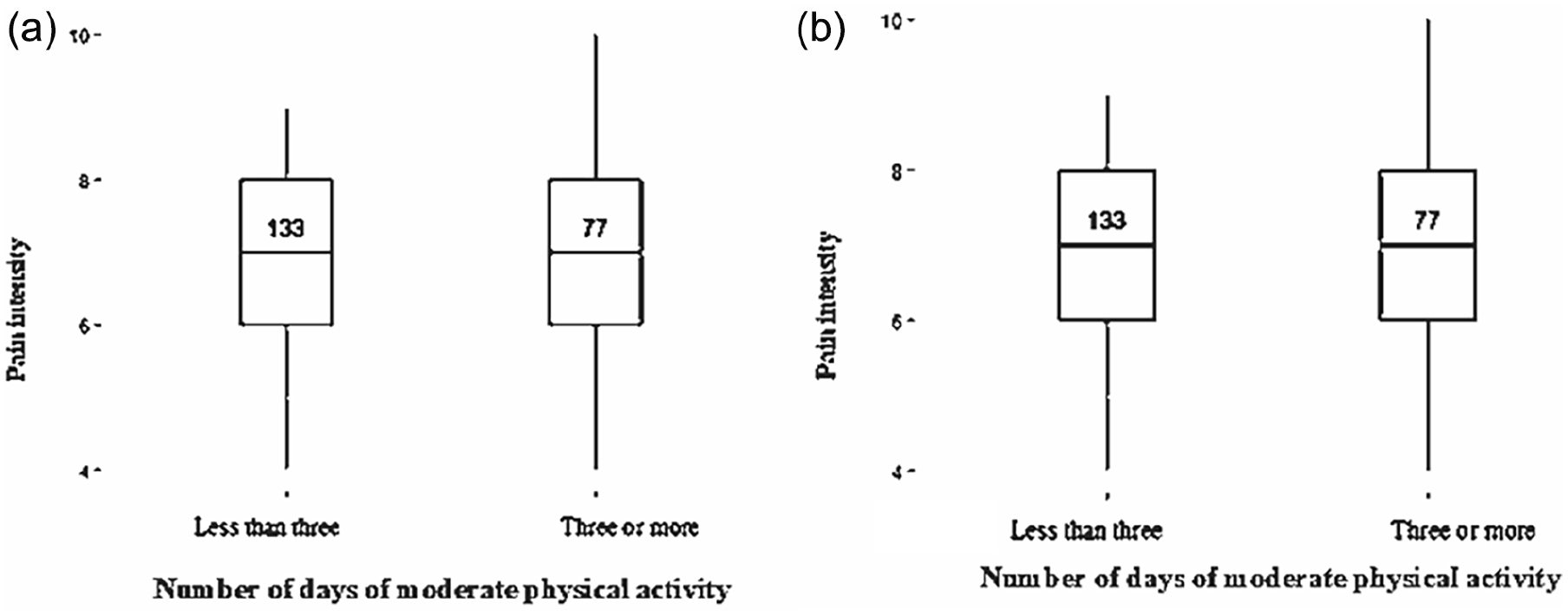
Box plot of the number of days of moderate physical activity per week, the intensity of pain during the last three menstruations, and SF-MPQ test score. (a) Pain intensity during the last three menstrual periods in women who performed MPA less than 3 days a week, or for at least 3 days a week or more. (b) SF-MPQ total test score among women who performed MPA less than 3 days a week, or for at least 3 days a week or more.
No statistically significant relationships were found (U-MW = 3784.5; p = 0.353) between the total score of the SF-MPQ test and those women who performed MPA less than 3 days a week (M = 21.94; SD = 8.5; Me = 21; IQR = 13), compared to those who did do it for at least 3 days a week or more (M = 21.16; SD = 9.08; Me = 19; IQR = 1.5) (Figure 3(b)).
No significant differences were found in the intensity of pain in the last three menstruations (U-MW = 5039; p = 0.465) among women who performed IPA less than 3 days a week (M = 0.82; SD = 0.895; Me = 0; IQR = 2), compared to those who did do it for at least 3 days a week or more (M = 3.94; SD = 1.15; Me = 4; IQR = 1.5) (Figure 4(a)).

Box plot of the number of days of intense physical activity per week, the intensity of pain during the last three menstruations, and SF-MPQ test score. (a) Pain intensity in the last three menses among women who performed IPA less than 3 days per week, compared to those who performed IPA at least 3 days per week or more. (b) SF-MPQ total test score among women who performed IPA less than 3 days a week compared to those who performed IPA at least 3 days a week or more.
Nor were significant differences found (U-MW = 1370.55; p = 0.958) in the total score of the SF-MPQ test between those women who carried out IPA less than 3 days a week (M = 21.94; SD = 8.5; Me = 21; IQR = 13), compared to those who did do it for at least 3 days a week or more (M = 21.55; SD = 10.83; Me = 19; IQR = 14) (Figure 4(b)).
Nor were significant differences found between those women in the total score of SF-MPQ test (U-MW = 1370.5.5; p = 0.958) in those women who carried out IPA less than 3 days a week (M = 21.94; SD = 8.5; Me = 21; IQR = 13) compared to those who did it for 3 days a week or more (M = 21.55; SD = 10.83; Me = 19; IQR = 14) (Figure 4(b)).
No significant relationship (ρ = 0.023; p = 0.708) was found between total METs (including IPA, MPA, and walking), and pain intensity of the last three menstrual periods. No statistical significant relationship has been found between sedentary lifestyle and menstrual pain intensity (p = 0.882; ρ = 0.009).
Discussion
This is the first study that addresses the relationship between menstrual pain intensity and level of PA, in METs and intensity, that found no significant relationship between these variables. Furthermore, it explores the relationship between different risk factors and menstrual pain from the limitations of a self-administered questionnaire.
In this research, there is a lack of differentiation between pain experienced during menstruation and other phases of the menstrual cycle, which is considered a limitation. To identify the degree of PA in a self-reported way is also considered a limitation because there could be a recall bias. Future research would need to improve this data collection with the use of objective tools, such as PA wristbands, accelerometers to measure PA, and more accurate pain assessment methods, such as portable pain trackers or validated pain diaries. Future research could also address PA habits in women with PD and those who do not have it.
In this study, we found a high sedentary lifestyle or low level of PA among participants. Matthewman et al. 30 indicated that PA could be a potentially effective treatment for PD pain. Armour et al. 33 and Heidarimoghadam et al. 34 studies are also along the same lines. The latter identified PA in their study as effective in significantly reducing the intensity of menstrual pain, although a greater number of studies of higher quality would be required.
World Health Organization recommendations speak of an interval of 150–300 min of MPA per week, or 150 min of IPA per week. 49 The IPAQ is a validated questionnaire. It would be interesting to assess more precisely the relationship between the specific type of PA and menstrual pain. There is no validated scale that measures the type of exercise that can be performed. Likewise, it would be important to do so with other types of more objective devices (activity bracelets, etc.). This measurement is outside the scope of this study because it is a self-administered questionnaire study. We believe that greater details could be necessary regarding the type of PA performed, the minutes and days per week used, as well as the time spent sitting, to better understand this relationship.
The most appropriate type of PA is not clarified, although there are different modalities that seem to show beneficial effects in reducing the VAS scale, such as stretching, strength training, or interval exercise. 33 The studies by Kannan et al.37,43 indicate that high-intensity aerobic exercise could be beneficial in reducing pain associated with PD and suggest that certain hormonal and inflammatory mechanisms, involved in nociceptive processing in these women, could be modulated. The review by Carroquino-García et al. 40 talk about therapeutic exercise in PD, and they maintain that a program between 8 and 12 weeks could be effective in reducing the intensity of pain, although their results should be considered with caution. They consider studies in which stretching, isometric exercise, and aerobic exercise have been performed. 40 There is heterogeneity in the naming of exercise modalities between the different studies. For future research, to standardize the names used and getting to know the interventions performed could facilitate the comparison between studies and the analysis of their results.
These types of findings may suggest that future research includes these recommendations to better identify the most appropriate exercise protocol or modalities to reduce the intensity of pain in women with PD, as well as the number of associated clinical manifestations and their impact on quality of life. More research is needed to identify the nature of the relationship between menstrual pain intensity and PA.
Clinical practice could use the data presented in this study to implement therapeutic exercise strategies to address menstrual pain. Future research could implement studies which compare PA habits in nondysmenorrheic women, a therapeutic exercise effect on pain intensity, and to determine its effect duration.
It has been shown that PA can influence pain reduction. 33 On the other hand, it is also known that the perception of pain may be different between people who are physically active and people who are not, which could influence the results achieved. 52
Despite these inconclusive results, further research is needed with more reliable devices (wearables) than a self-reported report, as well as the description of the type of exercise.
Studies have investigated the possible relationship between exercise and the intensity of menstrual pain, but the results are inconclusive.30,35,36 This is the first study to link PA with menstrual pain intensity. Other studies with visceral pain have not found a link either.33,53,54 Some studies have shown that this type of pain would be reduced with specific exercise, localized in this area (lumbopelvic mobilization). Although there is research indicating that simply overall PA is beneficial in other conditions with no differences found between exercise modalities. 52 In other pathologies, there are already studies indicating that certain exercise modalities seem to be more effective than others in low back pain. 55
Limitations
There are factors influencing menstrual pain that have not been considered in this study, such as diet and the time of the menstrual cycle when filling in the questionnaire. It would be necessary to collect PA with more objective devices. Further research is needed to determine the most appropriate type of PA for women with dysmenorrhea and that it is measured with objective devices as well as to determine the impact of lifestyle by relating the number of hours spent sitting as a possible determinant factor.
In this research, there is a lack of differentiation between pain experienced during menstruation and other phases of the menstrual cycle. To identify the degree of PA in a self-reported way is also considered a limitation because there could be a recall bias.
Future research would need to improve this data collection with the use of objective tools, such as PA wristbands, accelerometers to measure PA, and more accurate pain assessment methods, such as portable pain trackers or validated pain diaries. Future research could also address PA habits in women with PD and those who do not have it.
Conclusion
Menstrual pain intensity did not differ between the types of PA. A large number of participants were sedentary as they did not perform any PA in the last 7 days.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251323014 – Supplemental material for Physical activity level in women with primary dysmenorrhea: A cross-sectional observational study
Supplemental material, sj-docx-1-whe-10.1177_17455057251323014 for Physical activity level in women with primary dysmenorrhea: A cross-sectional observational study by Zeltia Naia, Paula Clara Santos and Olalla Bello in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.