
Abstract
Background:
Mortality rate of female gynecologic cancer is higher among individuals without affordable health insurance.
Objectives:
We determined the impact of Medicaid expansion on the number of female gynecologic-related cancer inpatient admissions in Virginia (VA) relative to North Carolina (NC), the latter of which did not expand Medicaid.
Design:
This quasi-experimental study was restricted to women between 18 and 64 years old admitted to general, acute, and short-term hospitals with gynecologic cancer.
Methods:
We used Poisson fixed-effect event study regression to examine differences in the predicted number of female gynecologic-related cancer admissions in the quarters before and after Medicaid expansion (implemented in January 2019) in VA, compared to the same period in NC.
Results:
Even though not significant, the predicted number of female gynecologic cancer-related inpatient admissions in VA increased by 4.8%, 4.9%, and 5.5% in the second, third, and fourth quarter of 2019, respectively, compared to the first quarter of 2019.
Conclusion:
Medicaid expansion in VA increased access to health services for Medicaid members, possibly due to initial pent-up demand among uninsured individuals.
Introduction
Female gynecologic cancers include cancer of the vulva, vagina, cervix, uterus, fallopian tubes and ovary. 1 All women are at risk for gynecologic cancer, and the risk increases with age. All cancers, including female gynecologic cancers, have higher mortality rates among low socioeconomic status (SES) populations with a lack of access to health care through affordable health insurance; the mortality of all cancers is 12% higher in U.S counties with consistent poverty status.2,3 Lack of access to health care is a known factor among low SES populations that leads to higher cancer mortality. 2 Access to care through affordable health insurance increases the probability of having a usual source of care and, as a result, increases the probability of cancer screening, early diagnosis, and appropriate treatment that have led to a reduction in cancer mortality.
Health care must be affordable and convenient to be considered accessible. In Virginia (VA), more than 10% of non-elderly adults were uninsured before Medicaid expansion.4,5 On January 1, 2019, VA expanded Medicaid eligibility for adults ages 19–64 with household incomes up to 138% of the federal poverty level (FPL) to improve access to and affordability of care. As of 2021, Medicaid enrollment has increased by about 27%. 6
Previous studies on the effect of Medicaid expansion showed increased access to the healthcare system and the utilization of low-cost healthcare services such as preventive and outpatient services among cancer patients. Medicaid expansion is correlated with the improvement of cancer screening and early diagnosis (e.g., pap smear, fewer treatment delays, and more treatment options in academic facilities being available for cancer patients), so Medicaid expansion decreases the disparities of income in access to cancer care.7,8
We expect to see a reduction in high-cost healthcare utilization, for example, inpatient services over time. However, immediately after Medicaid expansion, more cancer patients who did not have access to care through affordable health insurance entered the healthcare system with undiagnosed, more complicated, late-stage cancer. So, we might face a high demand for high-cost hospital services, for example, inpatient cancer treatment or surgery for cancer management. No study has measured the effect of Medicaid expansion on high-cost inpatient admissions that can be prevented by having regular screening tests and early treatment in outpatient settings. So, this study aims to examine the effect of Medicaid expansion on female gynecologic cancer-related inpatient admissions.
Method
This is a quasi-experimental study to find the effect of Medicaid expansion on female gynecologic cancer inpatient admissions in VA. We chose North Carolina (NC) as a comparative state since it expanded Medicaid in December 2023 which was not the same time as VA. In addition, the demographic and geographic location of NC are comparable with VA, and NC has a similar female gynecologic cancer incidence and mortality between 2016 and 2020 (Supplemental Appendix Table 1).
Data source
Our analysis compares VA inpatient claim data 9 to NC Healthcare Cost and Utilization Project (HCUP) data 10 by quarter year over the years 2017–2019. VA inpatient claims data are comparable to HCUP inpatient claims data in terms of the availability of information on the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes of female gynecologic cancer. This information makes these data sets suitable to answer our research question. HCUP is based on data from community hospitals, defined as short-term, non-Federal, general, and other hospitals, excluding hospital units of other institutions (e.g., prisons), long-term care, rehabilitation, psychiatric, and alcoholism and chemical dependency hospitals. Therefore, the data for both states are restricted to admissions to general, acute, and short-term hospitals for problems related to female gynecologic cancer. Further, we identified the county of residence for each individual by county-level Federal Information Processing System codes available in the claim datasets and used Small Area Health Insurance Estimates (SAHIE) databases to merge the information on the percentage of uninsured as a proxy variable for individual household income and FPL in VA and NC. The United States Census Bureau’s SAHIE program produces the only source of data for single-year estimates of health insurance coverage status for all counties in the United States. 11 This study used publicly available deidentified data, which is exempt from Virginia Commonwealth University Institutional Review Board review. 12
Inclusion criteria
We included inpatient admissions for all female adults between 18 and 64 years admitted to the general, acute, short-term hospital with the diagnosis of any gynecologic cancer. Admissions are restricted to ages 18–64 years old because they are the age groups eligible for Medicaid expansion. To assess the impact of Medicaid expansion on the female population, we included individuals with all types of insurance coverage, including those who were uninsured (i.e., whose admissions were self-paid or paid through hospital charity care programs). This is especially important for assessing the effects of Medicaid expansion since Medicaid admissions alone are likely to increase due to the increase in Medicaid eligibility, but overall admissions may decrease due to increased access to preventive care for people who were previously uninsured. While it would have been optimal to further target the sample to admissions for people who were lower income, information on patient income was not available in the admissions data.
Exclusion criteria
We excluded all females 65 years and older because this age group is eligible for Medicare benefits for cancer care. 13
Description of measures
The original data was admission-level; however, we aggregated the number of female gynecologic cancer admissions for each county (and independent cities in VA) for county-level analysis. Admissions for each county were aggregated by quarter so that the unit of analysis is the county/quarter. For VA, there are 1596 observations—133 (95 counties and 38 independent cities) by 12 quarters (January 2017 through December 2019). For NC, there are 1200 observations—100 counties by 12 quarters.
Independent variable
The main independent variables are time periods corresponding to the implementation of the Medicaid expansion in VA in the first quarter of 2019.
Dependent variable
The main dependent variables are the number of female gynecologic cancer admissions for each county by quarter. Admissions for female gynecologic cancer are defined based on ICD-10-CM codes (Supplemental Appendix Table 2). 14 The female gynecologic cancer diagnosis could occur in any position in the claim from primary diagnosis, to secondary, or beyond.
Statistical analysis/data analysis
We performed descriptive analyses of the average number of female gynecologic cancer inpatient admissions by county (and independent city) from the first quarter of 2016 until the last quarter of 2019 in VA and NC.
We used Poisson fixed-effect event study regression to examine the number of female gynecologic cancer inpatient admissions in the quarters before and after Medicaid expansion in VA and compare these trends to the same quarters in NC. This analysis expands the difference-in-difference analyses by creating a separate parameter for each quarter of interest.
To control for time-invariant characteristics of counties and independent cities, we include county-level fixed effects in all multivariate analyses. We also include time dummies and a quarter-specific measure of the uninsured percentage under 65 years old as a time-varying measure that might have an impact on our dependent variable in each quarter. 15 The information on the uninsured percentage under 65 years old was obtained from the United States Census Bureau’s SAHIE Program. 11

Ψ t represents a full set of quarterly dummy variables (1 quarter is a reference + 11 dummy variables). Statet*Ψ t represents the set of interactions between a dummy variable for VA and the quarterly dummies starting with the first quarter of 2017 to the fourth quarter of 2019 with an indication of the fourth quarter of 2018 as a reference. xit is the percentage of uninsured. α i is the county fixed effect. uit notates the error term.
By estimating the number of inpatient admissions through a Poisson model, we avoid the potential estimation bias that could result from estimating rates of admissions for female gynecologic cancer. For example, the total inpatient admissions might change (higher or lower) concurrent with the female gynecologic cancer admissions, making the female gynecologic cancer admissions rate biased. In addition, the Poisson model is appropriate for some counties where there is a low count of inpatient admissions.
We conducted a power analysis and sample size justification by approximating the count of inpatient admissions as a continuous variable, using a Normal approximation to a Poisson distribution. Assuming a general linear model, we found that a sample size of 54 geographical units in each group (VA versus NC) would give us 90% power to detect a small effect size (delta = 0.3). This is based on a difference-in-differences design, using a generalized least squares estimation framework with a 5% two-sided significance level. We used eight timepoints before Medicaid expansion and three timepoints after, with a conservative assumption of a compound symmetry correlation structure (rho = 0.25) between the inpatient admissions within each time period.
Given that we actually have 133 counties in VA and 100 counties in NC, the sample size required to detect even larger effects would be much smaller. This clearly indicates that our study has sufficient power to determine if there is a meaningful difference between the two groups. 16
We estimated the effect of Medicaid expansion on the number of female gynecologic cancer inpatient admissions after Medicaid expansion in January 2019 (three quarters). Parameters for the interactions between the VA dummy variable and each quarterly time dummy variable estimate the proportional difference in admissions for VA relative to NC. We computed standard errors that are robust to heteroskedasticity for all multivariate models.
All models were estimated using Stata statistical software 13, and p < 0.05 was considered statistically significant. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 17
Results
There were a total of 2796 county/quarter observations from 2017 to 2019. The average age of patients who were hospitalized for female gynecologic cancer was 42 years for both VA and NC. The mean county average length of hospital stay for cancer was around 4 days in both VA and NC (Table 1).
Mean patients’ characteristics who were admitted for female gynecologic cancer.
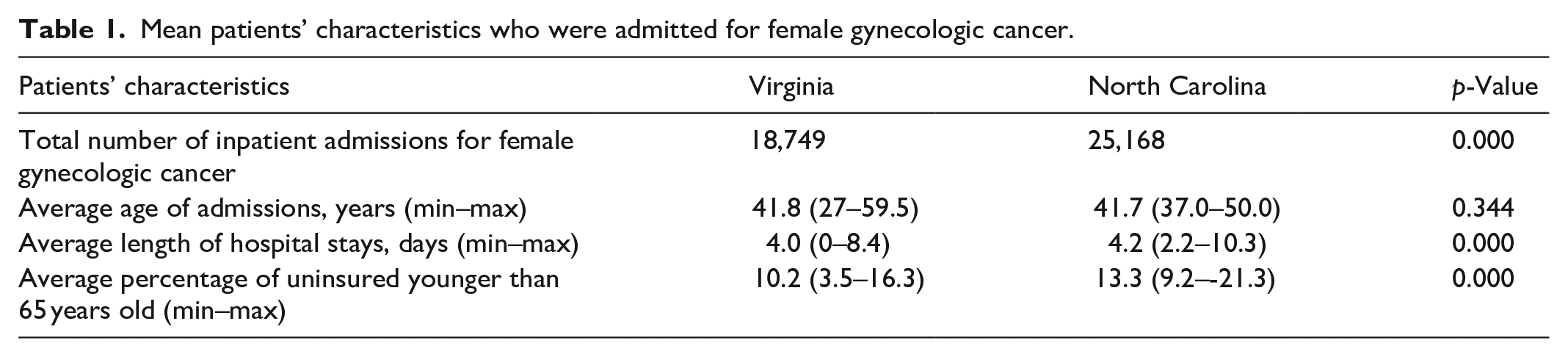
The total inpatient admissions for female gynecologic cancer was 18,749 in VA. In NC, there were a total of 25,168 inpatient admissions for female gynecologic cancer (Table 1).
The average unadjusted number of inpatient admissions per county per quarter for female gynecologic cancer before and after Medicaid expansion in VA and NC showed an increase after Medicaid expansion in VA, but virtually no change in NC (Figure 1).
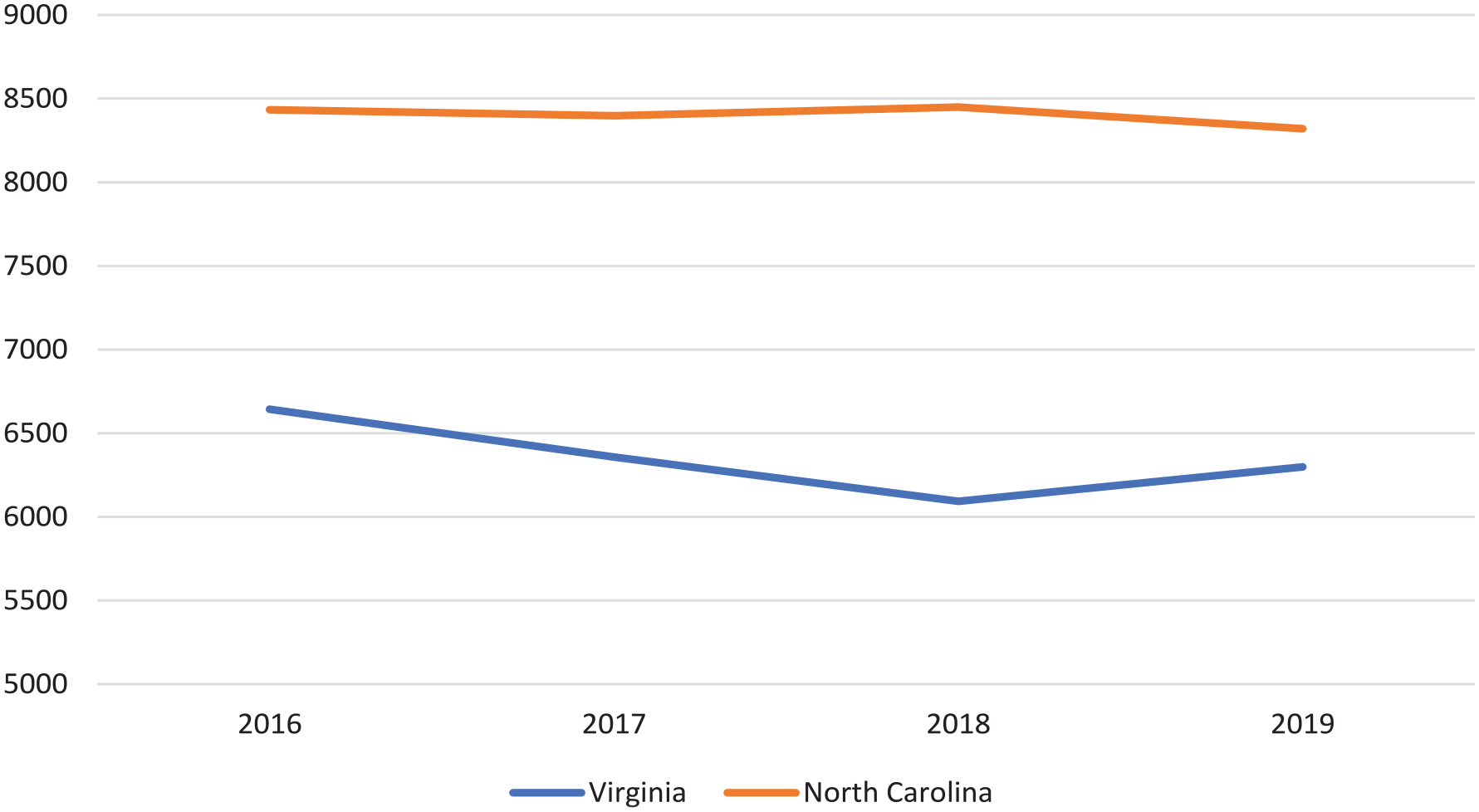
Average unadjusted number of female gynecologic cancer inpatient admissions between 2016 and 2019.
Results of the Poisson fixed-effect event study regression for the dependent variables are shown in Table 2. The predicted number of inpatient admissions for female gynecologic cancer in VA showed a significant increase in the third and fourth quarters by 11.2 (95% CI: 4.2, 18.3) and 9.2 (95% CI: 3.6, 16.0) compared to the first quarter of the year 2019 when Medicaid expanded. Further results showed that following Medicaid expansion in VA relative to NC, even though not significant, the predicted number of female gynecologic cancer inpatient admissions in the second quarter of 2019 increased by 4.8% (95% CI: −3.5, 13.1) compared to the first quarter of 2019 (the beginning of the Medicaid expansion). The rise in female gynecologic cancer inpatient admissions continued at 4.9% (95% CI: −4.6, 14.5) in the third quarter of 2019 and at 5.5% (95% CI: −3.5, 14.7) in the fourth quarter of 2019 compared to the beginning of the Medicaid expansion in VA relative to NC.
The Poisson regression percentage change (%) of female gynecologic cancer-related inpatient admissions in Virginia compared to North Carolina after and before Medicaid expansion.

CI: confidence interval.
Discussion
In this study, we examined the effect of Medicaid expansion on the total number of inpatient admissions of female gynecologic cancers in VA compared to NC, which did not implement similar reforms during this time period. We compared acute inpatient admissions for female gynecologic cancers at the county level for each quarter for 2017 through 2019, assessing changes in inpatient admissions in VA after the implementation of Medicaid expansion in January 2019, relative to changes in admissions in NC. The average unadjusted and adjusted numbers in VA showed an increase in female gynecologic cancer inpatient admissions in 2019. Using Poisson fixed-effects event study regression analysis, although insignificant, we observed an increase in the predicted number of female gynecologic cancer admissions in VA in each of the three quarters following Medicaid expansion relative to NC.
The rise in the number of inpatient admissions due to female gynecologic cancer following Medicaid expansion is consistent with the detection of more undiagnosed, complicated, and late-stage cancer in now accessible health services such as preventive and outpatient services for low-income populations who were uninsured before Medicaid expansion.
This result is consistent with prior research showing that expanding health insurance coverage increases utilization of all types, including inpatient services. 18 Ultimately, VA did not observe a statistically significant increase in female gynecologic cancer inpatient admissions in the first year of Medicaid expansion relative to the pre-expansion; although, the quarterly estimates for 2019 suggest such differences began to emerge in the fourth quarter of 2019. It is possible that a Medicaid expansion “effect” on inpatient admissions may have been more pronounced in 2020 and later years; although the beginning of the COVID-19 pandemic may have further disrupted these trends.
Limitations
The findings in this paper are subject to some limitations. First, admissions data do not have information on patient characteristics that might be most affected by Medicaid expansion, for example, household income or FPL. We used the uninsured percentage by county level as a proxy variable to address this issue. Second, Medicaid expansion policies were not randomly assigned. Although our difference-in-differences methods control for some sources of bias, we cannot rule out the possibility that some other change occurred differentially in VA compared to NC at the same time as these policies were adopted, potentially biasing our difference-in-differences estimates. However, we estimated event study regressions, comparing changes between VA and NC to assess parallel trends in the pre-policy period, which showed that VA and NC had similar trends prior to the Medicaid expansion.
Third, we used a single state to compare the effect of Medicaid expansion in VA on gynecologic cancer-related inpatient admissions, and therefore generalizability of the study results may be somewhat limited. It is possible that the results would differ if other states were included as comparisons. However, NC is a reasonable comparison state with VA in terms of both geographical proximity and population characteristics. Finally, we analyzed the effect of Medicaid expansion in 1 year. To see the impact of Medicaid expansion on gynecologic cancer-related inpatient admission throughout the year, we use the quarters as a unit of time. However, with the COVID-19 pandemic starting in 2020, we expected a reduction of all admissions that could potentially bias the effect of the Medicaid expansion policy. 19
Conclusion
Female gynecologic cancer-related admissions steadily increased in VA compared to NC following Medicaid expansion. In VA, it is possible that initial pent-up demand among uninsured individuals with undiagnosed female gynecologic cancer could have contributed to the increase in inpatient admissions. The Medicaid expansion “effect” is difficult to follow into 2020 due to the beginning of the COVID-19 pandemic. Policymakers should note that eligibility expansion may lead to different effects on inpatient admissions compared to the expansion of benefits for covered members.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241307080 – Supplemental material for The effect of Medicaid expansion on female gynecologic cancer-related inpatient admissions
Supplemental material, sj-docx-1-whe-10.1177_17455057241307080 for The effect of Medicaid expansion on female gynecologic cancer-related inpatient admissions by Shiva Salehian, Michael Preston, Peter Cunningham, Dipankar Bandyopadhyay and Emmanuel Taylor in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.