
Abstract
Background:
Breast cancer survivors (BCS) may experience cardiotoxicities from chemotherapy and oral endocrine therapy. Although a few studies have documented that palpitations are prevalent and associated with poorer outcomes, there is limited to no information on BCS’ reporting of palpitations to healthcare providers.
Objectives:
To compare BCS who did and did not report their palpitations to a healthcare provider and describe how those who did report palpitations recalled their provider responding.
Design:
This was a cross-sectional, national, electronic, pilot survey of BCS enrolled in the Love Army of Women registry.
Methods:
Participants (n = 52 with palpitations) completed standardized and investigator-designed questionnaires. Data were analyzed using frequency and descriptive statistics, chi-square tests, and Mann–Whitney tests. Responses to one open-ended question were analyzed using frequency counts and standard content analysis.
Results:
Compared to BCS who reported palpitations to a provider (n = 34), BCS who did not report their palpitations (n = 18) were significantly more anxious (p = 0.002) and more likely to feel palpitations as an irregular heartbeat (70.6% versus 38.9%, p = 0.027). Among the 34 BCS who reported palpitations to a provider, 32 completed the open-ended question. Of these 32 BCS, a majority (n = 27, 84%) indicated their provider recommended cardiac testing and/or referral to a cardiologist. Most (n = 24) reported completing testing. Test results included diagnosis of a new arrhythmia or other cardiac abnormality (n = 11, 46%), receipt of a new prescription (n = 5, 21%), or normal results (n = 5, 21%). Five (16%) of the 32 BCS did not receive recommendations for testing or referral and felt their provider normalized or dismissed their symptoms.
Conclusion:
Palpitations are a salient topic for further research and clinical practice recommendations to address cardiac health in BCS.
Plain language summary
Women who survive breast cancer can develop heart problems as a result of treatment. A common report of these women is feeling like the heart is beating faster, pounding, or beating irregularly. There is little research on what happens when breast cancer survivors have palpitations. Do they report them to a healthcare professional? If so, how does the healthcare professional respond? There were 52 survivors with palpitations who filled out an electronic survey; 34 reported their palpitations to a provider and 18 did not. Those who did not report palpitations were more anxious and more likely to feel their palpitations as an irregular heartbeat. Most of the women who reported palpitations to a provider received a recommendation for tests or referral to a heart specialist. Most completed the testing which resulted in finding a heart rhythm disturbance or other heart abnormality, getting a new prescription, or reassurance that things were normal. There were five women who did not get any recommendations for testing or referral. These women felt like their healthcare provider dismissed their symptoms as unimportant.
Introduction
Palpitations in peri- and post-menopausal women are an important clinical issue. Palpitations are more common in women 1 and may be experienced by up to 40% of peri-menopausal and 54% of post-menopausal women. 2 Palpitations may be related to underlying cardiac arrhythmias or other cardiovascular disease. In the Women’s Health Initiative study, palpitations were associated with a 20% increase in incident cardiovascular disease. 3
When women report palpitations to a healthcare provider, providers can follow recommendations for evaluating palpitations. These include obtaining a thorough health history, physical examination, 12-lead electrocardiogram (ECG), and/or multi-day ambulatory ECG monitoring.4 –6 However, problems may arise when women do not report their palpitations to a healthcare provider or when providers do not follow recommendations. In a recent qualitative study of 14 peri- and post-menopausal women without breast cancer, only half reported their palpitations to a healthcare provider and not all underwent recommended testing. 7 Failure to report and failure to respond can both lead to missed or delayed cardiac care.
Palpitations in peri- and post-menopausal breast cancer survivors (BCS) require special attention as cardiac issues are more likely to affect BCS. Like surgical menopause, chemotherapy can cause an early menopause. Surgically induced early menopause is a known risk factor for coronary artery disease and heart failure. 8 In addition, several breast cancer chemotherapies (e.g., anthracyclines, alkylating agents) have been linked to arrhythmias, left ventricular dysfunction, and/or congestive heart failure.9,10 Oral endocrine therapies for breast cancer are associated with increased coronary artery disease, ischemic events, and heart failure. 9 Thus, reporting of palpitations by BCS is a particularly salient topic to study to address cardiac health in this population.
Previous studies have documented palpitations prevalence in endocrine therapy users.11,12 These studies show 15%–48% of BCS report palpitations. Other studies have examined demographic, clinical, symptom, and genetic differences between BCS with and without palpitations.13 –15 These studies show BCS with palpitations report lower functional status, higher comorbidity burden, higher symptom burden, and poorer quality of life.14,15 However, none of these studies investigated (1) individual differences in BCS who do and do not report palpitations to their provider nor (2) the healthcare provider’s response to BCS reporting palpitations.
There were two objectives of this analysis. The first was to compare differences in demographics, clinical factors, palpitations, symptoms, and attitudes toward menopause between symptomatic BCS who did and did not report their palpitations to a healthcare provider. The second objective was to explore how those who did report palpitations remembered their provider responding (e.g., recommendations for additional testing, referrals, follow-up care).
Methods
Design
This was a cross-sectional, electronic, pilot survey of BCS enrolled in the national American research registry formerly called the Love Army of Women Research Registry that is now part of the Tower Cancer Research Collective. 16 At the time this survey was operating, the Love registry consisted of BCS who were willing to receive notifications about studies seeking research participants. All participants who completed the survey did so between May 6, 2023, and October 27, 2023.
We followed the strengthening the reporting of observational studies in epidemiology (STROBE) statement. 17 To avoid bias in attracting only those survivors who had palpitations, the study was described as “understanding feelings and symptoms after breast cancer.”
Inclusion and exclusion criteria
Participants who were included were: (1) biologically female, (2) age 18 and older, (3) with a history of breast cancer, (4) at least 1 month past finishing any intravenous chemotherapy, radiation, or surgical treatment for breast cancer, and (5) either peri-menopausal (past 3 months with less regular or skipped periods) or post-menopausal (no periods past 12 months), (6) able to confirm that menstrual changes were not due to uterine ablation or an intrauterine contraceptive device.
Participants were excluded if they: (1) had other past cancer diagnoses, major psychiatric disorders (e.g., schizophrenia, psychosis), or history of heart attack or congenital heart disease, (2) were pregnant or lactating, or (3) were males or transgender individuals (to control for the effects of male hormones).
Sample size
There was no a priori power analysis. We aimed for pilot data from 50 or more BCS.
Procedures and setting
Once approved, email and newsletter notices were sent by the registry staff to registry participants who had opted in for such notices (total n unavailable). Each notice included an invitation to respond, some basic information about the study, and a quick response code which led to the screening and consent forms. After completing the screening form, ineligible BCS saw a screen thanking them for their time and attention. Eligible BCS saw the consent form. BCS indicated consent by clicking an “I agree” button. Those who agreed were able to complete the online survey from a location of their choosing (e.g., home, work). All documents were launched in Qualtrics.
Measures
Attention check questions
The survey included attention check questions; instructed-response items which have an obvious correct response and are used to verify participants are reading questions carefully.18 –20 For example, one item was “Please select strongly agree for this question.” BCS who did not answer all attention check questions correctly were excluded from analysis as they were considered to have engaged with the questionnaire in a careless manner. This process allowed more accurate study conclusions to be formulated.
Demographic and clinical form
Using standard forms,21,22 BCS were asked to self-report demographics (e.g., age, race, ethnicity, marital status, education, employment status, income) and clinical variables. For clinical variables, participants self-reported height and weight for calculation of body mass index, history of breast cancer treatment including adjuvant endocrine therapy, gravidity and parity, history of thyroid disease, smoking history, menopausal status using Stages of Reproductive Aging+10 standardized definitions,23,24 history of coronavirus disease test, and history of heart conditions.
Palpitations assessment tool
An investigator-designed 27-item Palpitations Assessment Tool was used to gather information about palpitations occurrence, sensations, frequency, severity, distress, interference, and concomitant cardiac symptoms. Items were based on a published review 25 and prior qualitative study that elicited words/phrases women used to describe palpitations. 7 At the top of the questionnaire, a definition of palpitations was offered as “a sudden and unusual feeling with your heart beats.” BCS who endorsed having palpitations in the past 2 weeks (yes or maybe/unsure) were shown the subsequent questionnaire items, whereas those who answered no skipped to the next questionnaire. BCS were asked whether they felt each of 18 palpitations sensations (yes, no). These responses were examined individually and also summed to represent the total number of sensations each participant endorsed. BCS were also asked how frequently they had palpitations in the past 2 weeks (once or twice a week, several times a week, every day, or many times a day), and to provide ratings for palpitations severity, distress, and interference using separate 0 (not at all) to 10 (extreme) numeric rating scales. All of those items were examined individually. BCS indicated no, maybe, or yes as to whether they felt concomitant cardiac symptoms in the past 2 weeks of (1) pressure, tightness, or pain in chest; (2) dizziness, faintness, or lightheadedness, and (3) feeling out of breath for no reason. These responses were summed to reflect greater endorsement of a greater number of concomitant cardiac symptoms.
Palpitations reporting items
BCS who responded yes or maybe to having had palpitations in the past 2 weeks, were asked “Have you ever told your healthcare provider that you have palpitations?.” Response options were no or yes. BCS who endorsed yes were asked “What happened? Did your healthcare provider recommend any additional tests or follow-up? Please describe.” A 500-word text box was provided for women to write-in their responses. These data were qualitatively examined as described in more detail below.
Symptom measures
Four symptom variables were assessed using standardized, valid, and reliable self-report measures: hot flash interference, insomnia severity, anxiety, and psychological distress. First, the Hot Flash Interference Scale 26 is a 3-item self-report measure of the degree hot flashes interfere with sleep, mood and concentration. Participants mark each item to reflect the prior week using a 0 (do not interfere) to 10 (completely interfere) scale. Overall mean scores (sum of items/no. of items) are calculated. 26 Branching logic enabled BCS without hot flashes to skip this questionnaire. The scale’s developer Dr. Carpenter (author of this article) granted permission to use this scale.
Second, the seven-item Insomnia Severity Index 27 assesses the severity of initial, middle, and late insomnia over the past 2 weeks. Total scores are interpreted as none (0–7), subthreshold (8–14), moderate (15–21), and severe (22–28) insomnia. Items for this scale are widely available and it is considered in the public domain.
Third, the seven-item Hospital Anxiety and Depression Scale Anxiety-subscale28,29 assessed generalized anxiety over the past week. Total scores range from 0 to 21 and are interpreted as: normal or no anxiety (0–7), mild anxiety (8–10), moderate anxiety (11–14), and severe anxiety (15–21). Items for this scale are widely available and it is considered in the public domain.
Fourth, the 20-item Psychological Distress Profile 30 assessed psychological distress in terms of depression, hopelessness, anxiety, and anger. Respondents rated how they felt at the moment using 5-point Likert response options ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). Summed total scores range from 20 to 100, with higher scores indicating greater psychological distress. The scale’s developer Dr. Elkins (coauthor of this article) granted permission to use this scale.
Attitudes toward menopause
The seven-item Attitudes Toward Menopause Scale (ATMAS 31 ) assesses attitudes toward menopause and aging. Response options are agree (1), feel neutral (2), or disagree (3). For example, one item reads “The older a woman is, the more valued she is.” After reverse scoring some items, total higher scores indicate more positive attitudes. The scale’s developer Dr. Sommer granted permission to use this scale (personal email communication).
Statistical analysis
The first author completed quantitative analyses using International Business Machines Corporation Statistical Product and Services Solution version 29.0.1.0. After using frequencies to describe attrition related to ineligibility or failing attention checks, frequency statistics were used to explore missing data. Less than 5% of data was randomly missing and mean imputation was used to calculate standardized questionnaire scoring.
Bivariate analyses using chi-square tests or Mann–Whitney tests were performed to compare characteristics of BCS who had and had not reported palpitations to a provider. These non-parametric tests were deemed most appropriate based on the small pilot nature of this study and fact that variables were not normally distributed. Also in keeping with the pilot nature of this study, results of statistical analyses are described in terms of being statistically significant (p < 0.05), trending toward significance (p < 0.10), and not significant (p > 0.10). This was done to identify potentially important variables to include in future studies.
Content analysis
The first and fourth author completed the analysis of the qualitative responses to the open-ended questions using both frequency counts and standard content analysis. 32 For the content analysis, both authors read the written responses. One author extracted the main text units of each response. The other author verified those extractions. Next, one author coded each relevant text segment to capture its essential meaning and grouped similarly coded text units together into categories. The responses were categorized into type of provider response, type of cardiac testing, and outcomes of cardiac testing. Both authors verified those categorizations. Both authors contributed to the written summary of the analysis.
Results
There were 159 eligible BCS who consented and completed the survey out of 201 unique survey attempts. Only 82 of the 159 (62%) passed attention checks and only 52 of the 82 (63.4%) reported experiencing palpitations in the past 2 weeks. Of these 52, 34 BCS (65.4%) reported they had told a healthcare provider about their palpitations and 18 BCS (34.6%) had not. The percentages who told their healthcare provider were not statistically different between those who endorsed yes (71.4%) versus maybe/unsure (52.9%) about having had palpitations in the past 2 weeks (p = 0.189).
Differences in demographics, clinical factors, palpitations, symptoms, and attitudes between BCS who did and did not report palpitations to a healthcare provider
As shown in Table 1, there were no statistically significant group differences in categorical level demographics, clinical factors, palpitations, or symptoms, but there were two trends toward significance. Compared to BCS who reported their palpitations to a provider, BCS who did not report their palpitations to a provider trended to be more likely to (1) have received intravenous chemotherapy (83.3% versus 58.8%, p = 0.073) and (2) report moderate-to-severe anxiety (27.8% versus 8.8%, p = 0.072).
Differences in categorical demographic, clinical, and symptom variables between BCS who did (n = 34) and did not (n = 18) report their palpitations to a healthcare provider (n = 52).

ATMAS: Attitudes Toward Menopause; BC: breast cancer; BCS: breast cancer survivors; HFI: Hot Flash Interference; ISI: Insomnia Severity Index; HADS-A: Hospital Anxiety and Depression Scale-Anxiety Subscale; PDP: Psychological Distress Profile; PVC: premature ventricular contraction.
p-Values for chi-square comparisons.
Answered yes to ever being told by a healthcare professional they had “an irregular heart rhythm (arrhythmias such as PVCs, atrial fibrillation, tachycardia, etc.).”
Answered yes to ever being told by a healthcare professional they had “heart disease (such as coronary artery disease, peripheral vascular disease, heart attack, congestive heart failure, etc.).”
As shown in Table 2, there were no statistically significant differences in continuous level demographics, clinical factors, palpitations, or attitudes, but there were statistically significant and trending significant differences in symptoms. Compared to BCS who reported palpitations to a provider, BCS who did not report their palpitations to a provider were (1) significantly more anxious (p = 0.002) and (2) trended to higher psychological distress (p = 0.066).
Differences in continuous demographic, clinical, symptom, and attitudinal variables between BCS who did (n = 34) and did not (n = 18) report their palpitations to a healthcare provider.
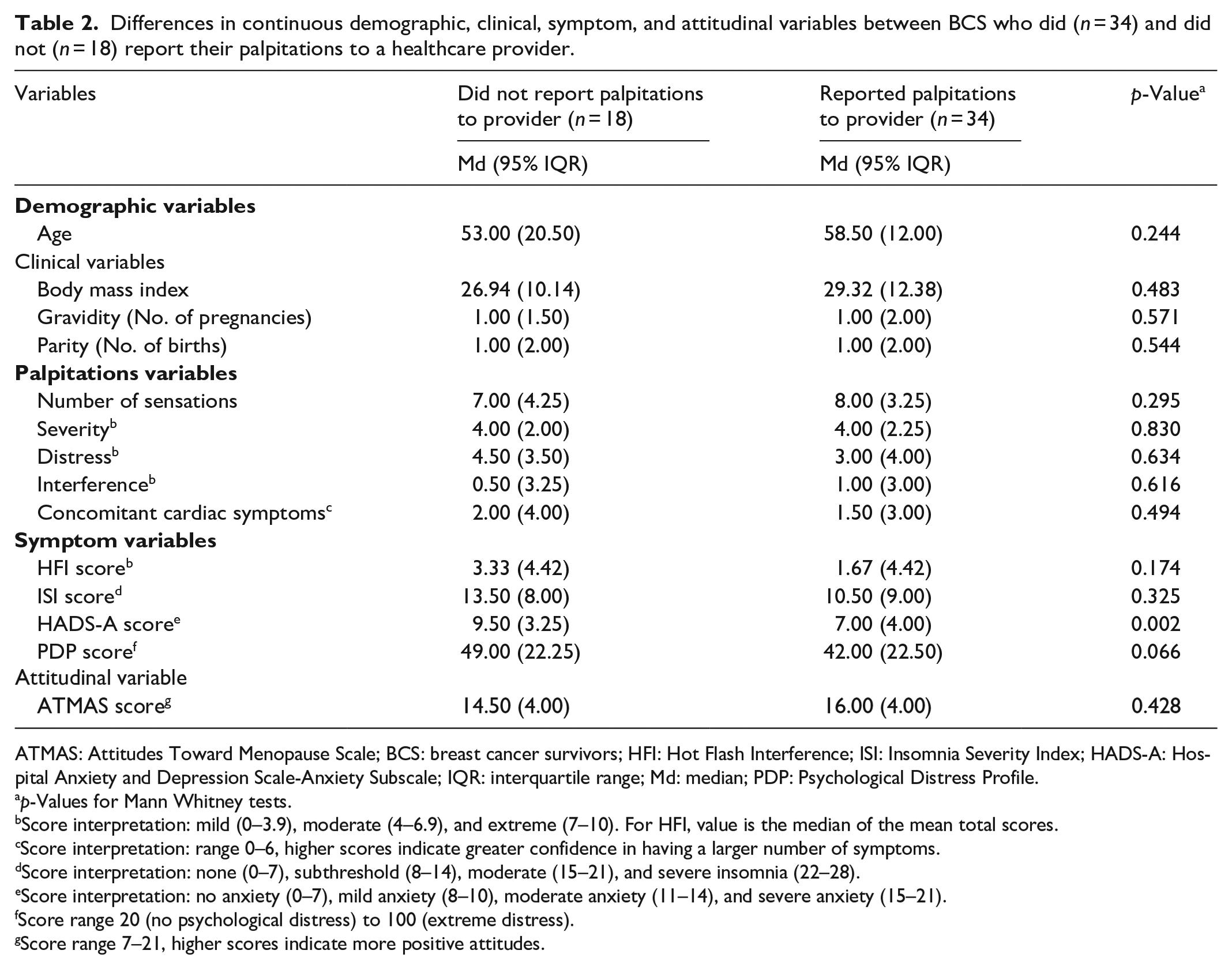
ATMAS: Attitudes Toward Menopause Scale; BCS: breast cancer survivors; HFI: Hot Flash Interference; ISI: Insomnia Severity Index; HADS-A: Hospital Anxiety and Depression Scale-Anxiety Subscale; IQR: interquartile range; Md: median; PDP: Psychological Distress Profile.
p-Values for Mann Whitney tests.
Score interpretation: mild (0–3.9), moderate (4–6.9), and extreme (7–10). For HFI, value is the median of the mean total scores.
Score interpretation: range 0–6, higher scores indicate greater confidence in having a larger number of symptoms.
Score interpretation: none (0–7), subthreshold (8–14), moderate (15–21), and severe insomnia (22–28).
Score interpretation: no anxiety (0–7), mild anxiety (8–10), moderate anxiety (11–14), and severe anxiety (15–21).
Score range 20 (no psychological distress) to 100 (extreme distress).
Score range 7–21, higher scores indicate more positive attitudes.
As shown in Table 3, BCS who reported their palpitations to a healthcare provider were significantly more likely to endorse the sensation of irregular heartbeat than those who did not report their palpitations to their provider (70.6% versus 38.9%, p = 0.027). There were no other significant differences in the palpitations sensations endorsed by those who did versus did not report palpitations to a healthcare provider. The top three most frequently endorsed sensations were the same in both groups: awareness of heartbeat, heart beating strongly, and heart racing.
Differences in palpitations sensations between BCS who did (n = 34) and did not (n = 18) report their palpitations to a healthcare provider.
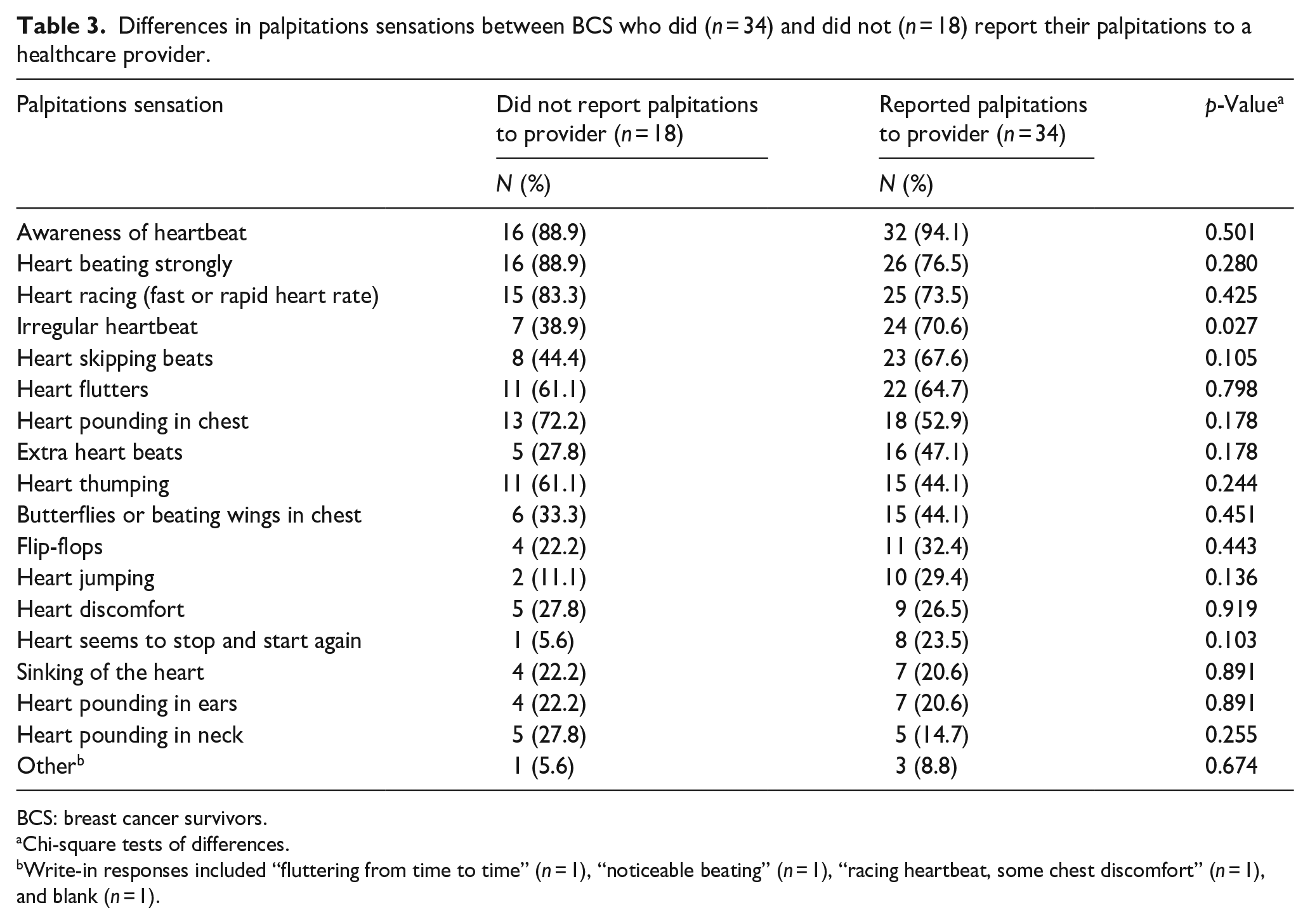
BCS: breast cancer survivors.
Chi-square tests of differences.
Write-in responses included “fluttering from time to time” (n = 1), “noticeable beating” (n = 1), “racing heartbeat, some chest discomfort” (n = 1), and blank (n = 1).
BCS’ descriptions of providers’ responses after reporting palpitations
Of the 34 BCS who reported palpitations to a provider, two did not write in a response to the open-ended question. Thus only 32 responses were available for content analysis.
Most (n = 27, 84%) of the 32 BCS indicated their provider responded with recommendations for testing or referral to see a cardiologist. Most (n = 24) stated they had completed cardiac testing, though the exact tests varied. Table 4 shows the number of participants who completed various combinations of cardiac tests and the outcomes. Among 24 BCS completing cardiac testing, tests completed included an ECG (n = 8, 24%), multi-day ECG monitoring (n = 14, 58%), echocardiogram (n = 7, 29%), stress test (n = 7, 29%), an unspecified combination of tests (n = 4, 17%), an electroencephalogram (n = 1, 4%), and heart catheterization (n = 1, 4%). Outcomes among the 24 participants included no description of results (n = 4, 17%), normal results (n = 5, 21%), an arrhythmia or other cardiac abnormality (n = 11, 46%), and/or receipt of a new prescription for a beta-blocker or unspecified medications (n = 5, 21%). Four of the five women with normal results stated they were told the palpitations were likely due to “anxiety,” “stress,” or “a large amount of caffeine.” One BCS whose palpitations were attributed to anxiety was told to walk on the treadmill to reduce stress. Most (n = 18, 67%) of the 27 participants did not describe what type of healthcare provider had initiated the cardiac testing. Of nine women who received a cardiology referral, six completed that referral and subsequent testing and are included in Table 4. For the remaining three BCS, one indicated follow-up was in progress and for two BCS it was unclear whether they had initiated or completed that follow-up.
Number and descriptions of tests and results following report of palpitations to a healthcare provider.

A-fib: atrial fibrillation; ECG: electrocardiogram; EEG: electroencephalogram; ECHO: echocardiogram; Heart cath: cardiac catheterization; PVCs: premature ventricular contractions; BCS: breast cancer survivors.
One BCS completed contrast test, one BCS was unable complete due to insurance denial of the test.
Three BCS who had some cardiac testing described problems they had encountered. One stated that although she had completed a stress test, her insurance denied a “contrast test.” Another described not fully understanding when she was told she had “normal” mild arrhythmias: “Normal for what, I don’t know. Normal for my age? Peri-menopause? Post COVID? Post chemo? They just said it was normal as in ‘not worrisome’. . .[I] had worn a monitor about a decade prior that did not show any.” Another BCS described issues with care coordination after having multiple tests and being diagnosed with intermittent ventricular arrhythmia. She stated “[the] cardiologist insists that my heart is not the problem. Something is acting on my heart. Refuses to work with other specialists to see what that might be.”
The remaining 5 (16%) of the 32 BCS did not receive any recommendations for testing or referral to see a cardiologist. Three indicated their provider normalized the palpitations by suggesting the symptom was “hormone-related,” “normal with menopause,” or “normal to aromatase inhibitors.” One BCS said her provider “pretty much dismissed” her palpitations. Another BCS said she planned to follow-up with the provider at her next visit.
Discussion
The present study adds to the very limited available research on palpitations in BCS. No prior studies in BCS have compared women who did and did not report their palpitations to a healthcare provider nor described women’s reports of their provider responses. Therefore data on BCS who did not report their palpitations to health care providers has been lacking. One finding from this study fills this gap—one-third of BCS who did not report their palpitations to a healthcare provider reported significantly higher HADS-A generalized anxiety scores. The group difference was nearly equivalent to a categorical difference in anxiety—means and standard deviations indicate that those reporting palpitations to a provider were in the none to mild anxiety range whereas those who did not report palpitations to a provider were in the mild-to-moderate anxiety range.28,29 The chi-square analysis of categorical differences indicated those who did not report palpitations trended to be more likely to report moderate-to-severe anxiety compared to those who did report palpitations (p = 0.072). Consistent with these anxiety findings, BCS who did not report their palpitations to a healthcare provider trended toward greater psychological distress. Reviews of common causes of palpitations in BCS include anxiety as a probable cause, yet anxiety is rarely measured. 33 Our findings suggest that anxiety was related to whether women reported their palpitations to a provider, with women who were less anxious being more, rather than less, likely to report them to providers.
A second new finding was that BCS who did report their palpitations to a healthcare provider were more likely to endorse feeling an irregular heartbeat (p = 0.027) but not other sensations like a racing heartbeat. Potential explanations might be that women who felt an irregular heart beat might have interpreted the sensations as more unusual, concerning, or distressing, and therefore they were more likely to report these sensations to a provider. Additional research is needed as it is difficult to fully interpret this finding without more information from the participants.
A third new finding is that those who did not report their palpitations to a provider trended toward being more likely to have received intravenous chemotherapy (p = 0.073). Authors posit that this finding may be related to BCS anxiety or fears. Those who received chemotherapy are likely to have received education about chemotherapy’s cardiotoxic side effects from their oncology nurses and/or physicians. It is possible that these BCS may not report palpitations due to fear of finding out there is a cardiac problem. Future research is needed to confirm or refute this trend as this finding may indicate that those who most need to report cardiac symptoms may be the least likely to report them.
Fourth, although most BCS reported their providers were appropriately responding to their reported palpitations, some women did not. BCS reported problems they encountered with testing and/or incomplete workup of their symptoms included providers’ normalization or trivialization of palpitations. The latter is particularly concerning given that most of the BCS who completed testing received a new diagnosis or a new prescription. Use of good clinical practice recommendations, such as those issued by the European Heart Rhythm Society 6 need to be consistently followed.
Clinical and research implications
Our pilot study findings have important implications for clinical practice. It is likely that palpitations are relatively common and that most providers are responding to BCS’ symptom reports. Findings also suggest that providers may need to directly query BCS about palpitations in order to capture the one-third of BCS who did not report their palpitations to their provider. The palpitations sensations we measured could be useful prompts in clinical practice to elicit BCS’ awareness and reporting of palpitations, as many women may not understand the word “palpitations.” Providers might particularly focus on those BCS who are anxious, distressed, or have received intravenous chemotherapy in order to capture those women who are under-reporting their palpitations.
In terms of future research, our findings suggest additional research is needed. A larger study that is powered to find significant between group differences could help to validate or refute the findings from this analysis. Findings from this study could help in power calculations to ensure sufficient sample sizes in future research. A larger study of BCS could clarify the relationships we describe and lead to cognitive-behavioral interventions to reduce BCS’ anxiety and distress to improve palpitations reporting. A larger study could also clarify providers’ responses through directly querying providers or reviewing medical records to verify tests ordered and results and could lead to educational interventions for providers to decrease normalization or trivialization of this symptom. Given that the majority of participants that reported palpitations did not describe the type of healthcare provider that initiated cardiac testing, it may be helpful to request this information in future studies, in order to target psychoeducational interventions to specific provider groups. In addition, future studies can build on this pilot study by expanding recruitment to include multiple racial and ethnic groups.
Limitations
While the present study adds to our understanding of palpitations among BCS and associated factors, there are some study limitations that must be noted. Specifically, this was an analysis of a subset of data from a pilot study and the sample size was relatively small, with little racial/ethnic representation. Findings may not hold true in other populations of BCS. Although nearly all women responded to the open-ended question, gaps in their responses indicated that multiple open-ended questions or a full qualitative interview should be used in the future to elicit more detailed descriptions. Due to a desire to keep the pilot survey as brief as possible to reduce cognitive load and increase response rates, authors did not include measures shown to be related to (1) palpitations in prior studies of BCS (e.g., menopausal symptoms, 14 sleep and fatigue, 15 quality of life 15 ) or women with breast cancer (e.g., cortisol 34 ) or (2) to menopausal symptoms in general (e.g., perceived control over symptoms 22 ). There also may have been recall bias, as we were asking participants to remember interactions with health care professionals. There also may have been non-response bias from women who never experienced palpitations, though the description of the study was intentionally broad to prevent non-response bias (see methods). Future larger studies designed to validate or refute our study findings should consider inclusion of these additional measures. As this was a pilot study, there was no power analysis.
Conclusion
This pilot study (1) identified some differences between BCS who did and did not report their palpitations to a healthcare provider and (2) analyzed BCS’ descriptions of how providers responded to their reporting of palpitations. Findings have some immediate implications for clinical practice and support the need for a future, larger study of palpitations in this population.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241305077 – Supplemental material for A pilot survey of breast cancer survivors’ reporting of palpitations to healthcare providers
Supplemental material, sj-docx-1-whe-10.1177_17455057241305077 for A pilot survey of breast cancer survivors’ reporting of palpitations to healthcare providers by Janet S Carpenter, Ying Sheng, Morgan Snyder, Rileigh Fagan, Vindhya Ekanayake and Gary R Elkins in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.