
Abstract
Background:
Despite a high prevalence, menstrual issues are often normalised or trivialised and undermanaged in young people (YP). Uncontrolled dysmenorrhoea and heavy menstrual bleeding have a vastly negative impact on the quality of life of YP, especially when these issues are compounded by the social and emotional complexities of navigating adolescence.
Objectives:
The Longitudinal Study of Teens with Endometriosis, Period and Pelvic Pain (LongSTEPPP) project is a 5-year study aiming to understand factors that contribute to endometriosis, period and pelvic pain in YP and to examine long-term outcomes.
Design:
Focus groups (FGs), held as part of co-design, sought to ensure that the perspectives and concerns of YP and their parents were incorporated into the longitudinal study design.
Methods:
YP and their parents were invited to participate in an online FG after completing a survey about periods. The online survey was also part of the co-design of LongSTEPPP and was advertised primarily through social media channels.
Results:
Four FGs were held, including three with YP (n = 12) and one with parents (n = 3). Major themes to emerge were (1) YPs experiences, including the physical and psychological impact of pain and bleeding; (2) pain and pain management; and (3) education. Mental health burden was significant on YP, with some reporting suicidal ideations. YP and their parents reported a lack of knowledge and awareness about menstrual issues among societies, healthcare professionals, and schoolteachers.
Conclusion:
This study identified the substantial impact of periods on YP, and their parents’ lives, the challenge of navigating a chronic pain condition in adolescence, and the lack of awareness in society and among professionals. Through the co-design model, these findings have informed the longitudinal study to ensure that it will adequately measure the concerns of YP and their parents.
Introduction
We acknowledge all people who have periods, regardless of gender identity. We will hereto refer to “women and girls” who are the majority, without intending exclusion or disrespect.
Dysmenorrhoea is one of the most common gynaecological problems, affecting between 42% and 90% of women.1,2 Up to 91% of school-aged young people (YP) in Australia are affected by dysmenorrhoea. 3 Similarly, heavy menstrual bleeding has a high prevalence in YP, affecting up to 30%. 4 The impacts of menstrual symptoms on the lives of YP are significant with higher rates of school absenteeism and interference with social and sporting activities.5,6 The repercussions of severe pain extend into adulthood; disrupted cognitive development, interrupted education and academic performance may result in missed career opportunities, and poor psychosocial and physical outcomes.7 –11
In Australia, only one-third of girls with menstrual issues seek help from a general practitioner (GP), 12 thus demonstrating how underrecognised and undermanaged menstrual symptoms are. Pain management for dysmenorrhoea is important as evidence shows that recurrent dysmenorrhoea is associated with a higher rate of chronic pain conditions such as chronic pelvic pain, 13 migraine, irritable bowel syndrome, musculoskeletal, and myofascial pain syndromes. 14 The phenomenon of central sensitisation is suspected as the underlying mechanism. 15 Early intervention with effective pain management could potentially prevent these chronic conditions from occurring.
The reasons for the undermanagement of dysmenorrhoea are unclear, although the societal ‘normalisation’ of dysmenorrhoea, negative attitudes towards menstruation and reluctance to discuss menstruation with healthcare practitioners may play a role.16 –18 Qualitative research allows increased understanding from the patient’s perspective, specifically their experience and main concerns. Only a few qualitative studies have been undertaken among YP with menstrual issues12,19 and even fewer among their parents. 20 That YP desire to better understand menstruation and associated symptoms is true for both high-income countries like Australia and low-middle-income countries. 21
The Longitudinal Study of Teens with Endometriosis, Period and Pelvic Pain (LongSTEPPP) follows the development and trajectories of period and pelvic pain, and endometriosis in YP, aiming at determining factors associated with pain, quality of life, mental health, and health utilisation. Including patients as partners is increasingly recognised as necessary and valuable in designing research projects. 22 Before starting the longitudinal study, we employed a model of co-design, which included survey 23 and focus groups (FG). In this paper, we report the outcomes of the FG, which aimed to explore the experience of menstruation in YP and their parents and to better understand the issues they experience, to adequately represent their concerns of priority in the longitudinal study.
Methods
Participants
Inclusion criteria for enrolment in the YP FG were age 12–18 years, periods started at least 3 months ago, proficiency in English, and written or verbal consent. Participants were excluded if they were not proficient in English. Importantly, trans and gender-diverse YP menstruating were eligible to participate in this study.
Participants were invited by telephone and or email to participate in a single FG after completing the LongSTEPPP Periods Survey. This online cross-sectional survey was run over 6 weeks from September to October 2021 and advertised on social media and outpatient clinics in a tertiary paediatric hospital in Australia. All participants who expressed interest in participating in an FG were offered the possibility to do so.
Parents/guardians (PGs) were invited to participate in a separate FG. PGs were called, provided with information, and invited to participate. Informed consent was verbally obtained.
Procedure
The online FG were semi-structured, in-depth discussions run via Zoom with only the researchers and participants present. To preserve anonymity, names were changed to random numbers. The video was only enabled for facilitators. FG questions were crafted to be open-ended and flexible to permit discussion of noteworthy threads that emerged. FGs were facilitated by female healthcare professionals (a paediatric research nurse and intern doctors) experienced in working with YP. A relationship was established at the beginning of each FG with introductions by the researchers (reasons for doing the research and interest in the topic) and icebreaker polls for participants. Field notes were made during and after the FG by JC, MF and EW. Audio from Zoom was recorded and stored online, in a password-protected database. Transcription was undertaken using Otter-AI. Transcripts were not returned to participants for comment or correction.
Data analysis/statistical analysis
The phases of thematic analysis were done per the Braun and Clark method. 24 Themes were derived from the data. Two authors (CM and MF) listened to the FG independently to extract prominent themes. Themes were reviewed, discussed, and subsequently refined until the salient themes and categories were decided (CM, MF, LK and SG). Lincoln and Guba’s evaluative criteria for trustworthiness and techniques for establishing credibility, transferability, dependability and confirmability were also considered. 25 Inductive thematic saturation was reached for the YP FG but not the PG FG.
Ethics approval was granted by the Royal Children’s Hospital Human Research Ethics Committee (#65911).
The COREQ guidelines were followed in preparing this manuscript. 26
Results
Of 1811 YP who completed the LongSTEPPP Periods Survey, 61 YP consented to attend an FG, with 12 YP attending. Four FGs were held in total; three YP FGs (n = 12), and one PG FG (n = 3). YP were aged 12–18 years. The three PGs who attended were mothers. Each FG was between 60 and 90 min.
Three overarching themes emerged from the FGs: (1) YPs experience of periods, (2) symptom management and (3) education and knowledge. Table 1 depicts the subthemes identified within each overarching theme.
Major themes and subthemes arising from FG.
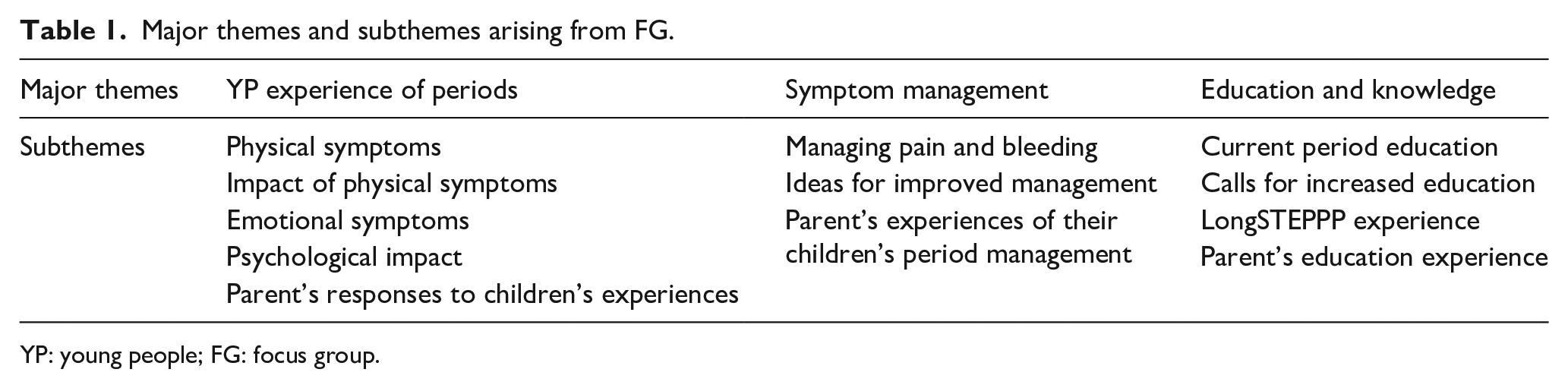
YP: young people; FG: focus group.
Theme 1: YP experiences
The main physical symptoms associated with menstruation were dysmenorrhoea and heavy menstrual bleeding. Debilitating pain was associated with a constellation of physical symptoms including nausea, vomiting, fatigue, dizziness, headaches, bloating and acne (Table 2).
YP and parents describing the impact of periods.
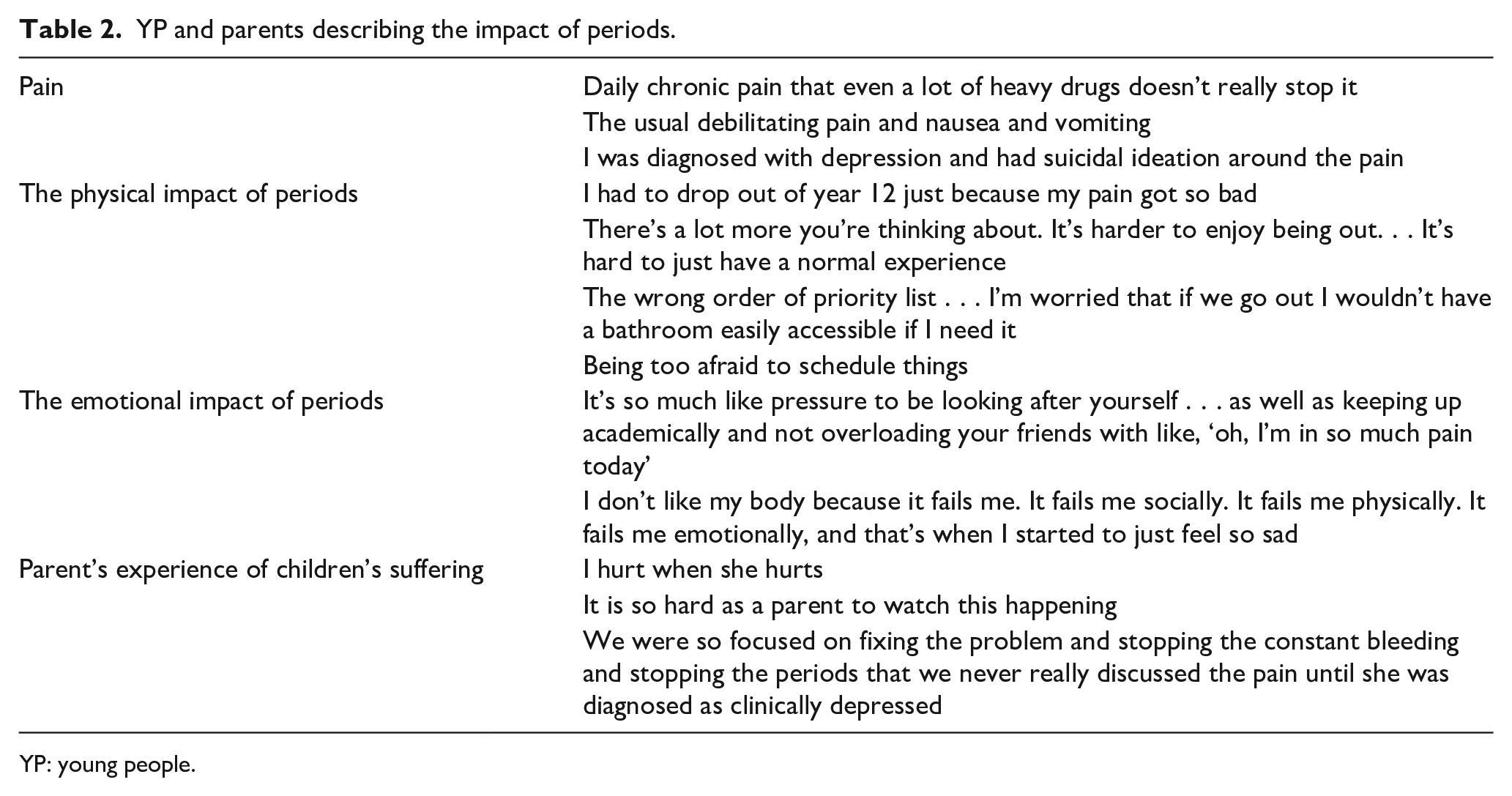
YP: young people.
These symptoms impacted the school, social and sporting lives of YP, resulting in absenteeism or a lack of focus (presenteeism). School absenteeism occurred for days or weeks at a time. A lack of focus occurred due to pain or concerns about bleeding through clothing. Interestingly, some YP reported a positive impact of COVID-19 lockdowns on schooling due to increased flexibility with the school routine and attire. Sport posed a practical challenge with participation limited by personal preference for sanitary products. Not all YP could use tampons for personal or physical reasons, and this prevented engagement in some sports.
YP expressed a range of complex emotions in response to the impact of periods on their lives. Managing periods created pressure, with YP reporting they felt a responsibility to perform academically and maintain friendships whilst dealing with immense pain and the uncertainty of bleeding. This resulted in emotional alienation from peers, and physical alienation where YP anticipated pain or bleeding and would skip events. YP felt their bodies were failing them, as they compared themselves to peers who did not have to manage period problems whilst also navigating adolescence. This mental load resulted in YP feeling depressed, being diagnosed with clinical depression and some reporting suicidal ideation.
Parent’s response to the impact on their children’s lives
All parents reported that their primary concern was watching their children suffer pain. One parent described the difficult position of guiding their child through medical interventions to manage pain, without knowing whether the treatment would be successful.
Parents were concerned about school absenteeism and the impact on YPs social lives, with them ‘missing out on living’. One parent was less concerned about the academic impact of school absenteeism, and more concerned about missed social excursions and the subsequent emotional impact, especially considering recent COVID-19 restrictions.
Theme 2: symptom management
All YP used both non-pharmacological and pharmacological approaches for managing their periods (Table 3). Bleeding was managed primarily with pads and tampons, with alternative products trialled such as re-useable period underwear and period cups. Reusable options were impractical to change outside of the home and some YP found they were not absorbent enough for a heavy flow. YP felt frustrated with period management, which required a ‘trial and error’ approach to find the best method. To achieve satisfactory symptom control, some YP were making complex medical decisions at a young age, which impacted their mental health. YP also considered the environmental impact of their choice of sanitary products. This consideration was occasionally empowering but also created further anxiety for some.
YP and parents’ experience with period management.

YP: young people; GP: general practitioner.
YP called for free and available access to sanitary items to improve period management. Ideas included free dispensers in bathrooms and placing pads in classrooms or common areas so students could access them without having to ask.
Many YP had difficulties with medical doctors. Some found GPs were unsympathetic to their period concerns or were dismissive of complementary medicine and allied health in managing pain. Others experienced that empathetic GPs and gynaecologists often had long appointment wait times. YP suggested increased collaboration between medical and allied health approaches such as naturopaths, physiotherapists and psychologists for pain management.
Parent’s opinion on symptom management
Parents reported pain management as the most difficult aspect of their children’s periods in three key ways. Firstly, some GPs failed to recognise the severity of YPs pain, often dismissing it as normal pain associated with early menstrual cycles. Secondly, once convinced that the YP was experiencing severe pain, parents felt that GPs were often inexperienced in providing appropriate strong pain relief to YP. Lastly, when referred to gynaecologists, parents found arranging appointments with these doctors very difficult. Parents additionally acknowledged mental health and the importance of a well-rounded approach to managing period problems.
Theme 3: education and knowledge
Sources of period education
YP received sexual and reproductive health education from their family, friends, and school. YP had different experiences regarding the period education they received from their families. Some YP described a positive, open discussion with mothers who were similarly affected by period problems. Other YP described family environments with limited discussion where their period problems were not acknowledged or recognised.
School-based reproductive education was universally viewed as insufficient, with YP describing it as ‘superficial’, ‘purely anatomical’ and ‘shame-based’ education (Table 4). YP felt whilst the anatomical approach to reproductive education taught them the logistics of periods, it did not outline normal and abnormal periods, nor when YP should seek help. It was the opinion of YP that endometriosis, adenomyosis and associated pain syndromes should be introduced. One YP wished they had ‘been taught when to ask for help’, and another stated that [if it had been] they ‘would have recognised earlier what was going wrong’ and sought medical help. YP found that information presented in school-based education was at times inaccurate; one YP recalled correcting a teacher who stated it was not safe to skip periods when using the combined oral contraceptive pill (COCP). Furthermore, some schools divided classes by sex for health education. YP called for increased education for male classmates, teachers and even parents; and for gender-neutral education, promoting inclusion for trans and gender-diverse individuals.
YP and parent’s response to period education.
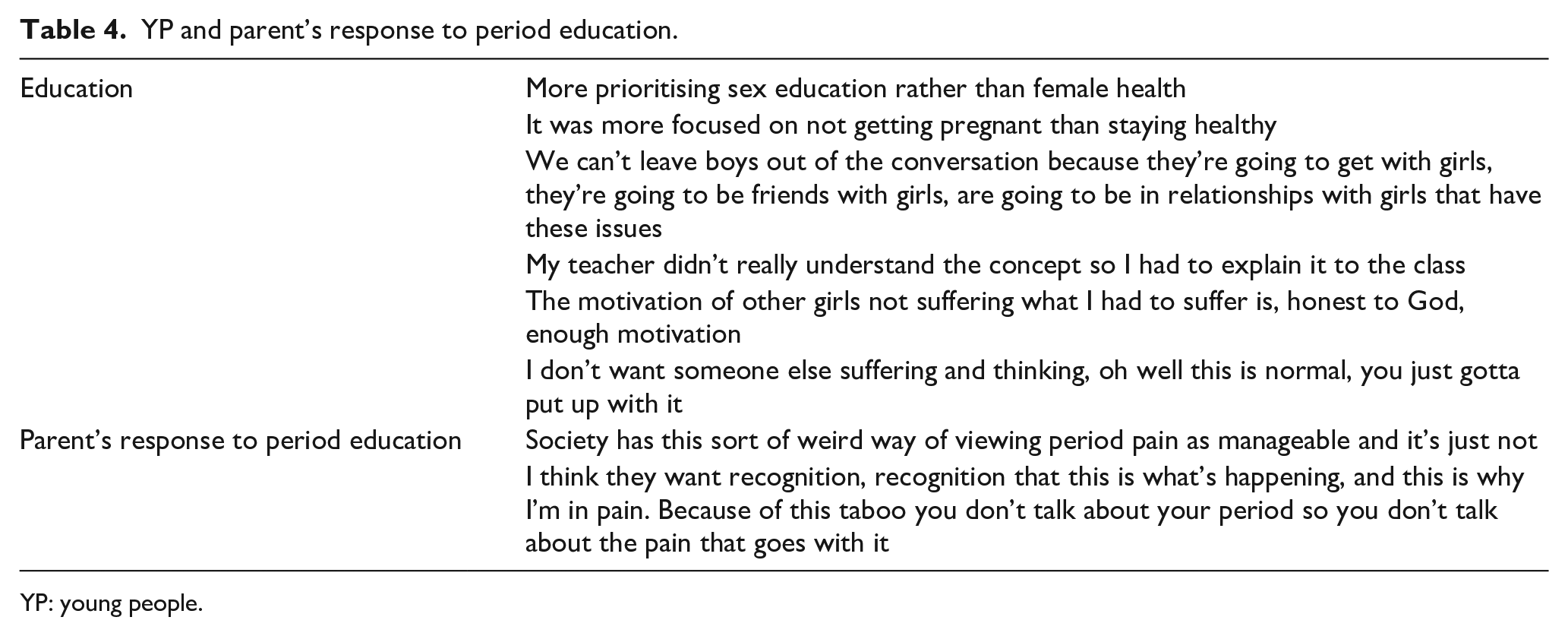
YP: young people.
Motivation for participating in the LongSTEPPP study
One motivation to participate in the FG was the connection to YP with similar period problems. This therapeutic connection was described as ‘validation’, ‘refreshing’ and ‘feeling heard’ which created a ‘sense of community’. Secondly, YP were motivated to ‘help other young women’ by sharing their personal experiences to ‘get more people talking about [period problems]’, to improve knowledge about dysmenorrhoea and to prevent other YP suffering.
Parent’s attitudes to education
Parents described their children as navigating an ‘area [of medicine] that is so far behind’. A lack of understanding of period problems prompted advocacy by parents, as they educate their relatives on the period problems their children face. Parents described the effects of generational change accompanying education, noting that the COCP was previously principally used for contraception, however now it is widely used for period management. Parents understand that their children ‘want recognition’ for their experience of period problems and agree with their calls for increased education. All parents found participating in LongSTEPPP to be validating for their children; one parent stated that this study ‘changed her [daughter’s] world’, as they recognised that they are not alone in suffering from these medical conditions.
Discussion
Whilst recent qualitative studies have described the unmet needs of girls with menstrual issues from their accounts and that of their parents,12,20 this is the first study to our knowledge to combine qualitative data regarding suffering associated with periods from separate FGs of YP and one FG of their parents.
Dysmenorrhoea impacted YPs quality of life across multiple domains, including physical, emotional, and social well-being. The psychological impact of pain and bleeding was significant. YP expressed anticipatory anxiety, shame, and a sense of failure from their bodies. Furthermore, they felt frustrated towards people with a comparatively easy experience of periods, and isolated due to this complicated emotional burden. Previous studies have described associations between dysmenorrhoea and depression and anxiety,27,28 and our study supports these findings as all participants described a range of emotions from low mood to clinical depression and suicidal ideation.
Few studies have addressed menstrual hygiene access in high-income countries. 19 In our study, YP reported that sanitary products were generally accessible in schools, although they had to ask for them, which was a significant barrier. Most YP preferred to ask their peers. Consistent with previous studies surveying the unmet needs of YP with period problems,12,20 YP wanted products that were convenient, absorbent and discrete. Interestingly, YP desired access to reusable products to limit environmental impact.
Effective pain management was a great challenge and all YP had tried multiple pharmacological strategies. Pain management is critical for improving quality of life; and there is increasing evidence that recurrent dysmenorrhoea may contribute to central sensitisation and a higher risk of persistent pain conditions,14,15 making the case for effective pain management stronger.
Reaching menstrual health, which is a ‘state of complete physical, mental and social well-being in relation to the menstrual cycle’, implies that individuals receive valid and age-appropriate information about the menstrual cycle. 29 In this study, YP described school-based education that failed to teach normal menstruation physiology, preventing them from recognising abnormal periods. A lack of comprehensive period education is a longstanding issue, with many Australian women reporting low rates of menstrual health literacy. 17 YP and parents called for an overhaul of period education within schools, elucidating a need for educational programmes focusing on female health and physiology, gynaecological conditions, and supportive allied health services. Bush et al. reported an increase in teen awareness of endometriosis and earlier presentations for specialised health services following the delivery of a menstrual health education programme to YP in schools in New Zealand. 30 Participants called for education targeting YP of both genders, but also for adults. YP felt better education and more open conversations around menstruation would result in increased awareness, de-stigmatisation, and increased support for menstruating YP.
YP found sharing their experiences alleviated a sense of isolation and helped them emotionally. They expressed a desire for online chatrooms and support groups where they could share experiences and alleviate the emotional burden associated with period problems. This finding is in line with studies that emphasise the importance of social support in managing the physical symptoms of periods.31,32
Strengths and weaknesses
This study provides contemporary knowledge, building on previous qualitative studies, about YP and their parents of dysmenorrhoea.12,20 It is the first to have interviewed YP and parents separately, which may have resulted in more candid answers.
One of the main limitations of this study was the low attendance of YP and particularly parents in the FGs.
Another limitation was the risk of selection bias, as YP with menstrual issues may have been more likely to participate. In addition, recruitment for the FG was made following the participation in the LongSTEPPP cross-sectional study which was advertised on social media and at an outpatient clinic in a tertiary paediatric hospital, therefore the participants may not be representative of the general teen population. Lastly, inclusion criteria required the ability to speak English, limiting the generalisation of our findings to people from non-English-speaking backgrounds (NESB) in Australia. Concerningly, this inadvertent exclusion of people from NESB is frequently employed in medical research, contributing to the higher pain burden experienced by women from NESB backgrounds. Future studies should endeavour to include people from NESB through the inclusion of professional translators.
We found the use of Zoom videoconferencing for the FG to be well-accepted with limited technical difficulties. The technology overcomes geographical and financial barriers when compared to in-person interviews. The ability to preserve anonymity was appreciated by YP and parents alike and the researchers were able to build rapport quickly to facilitate participant engagement. There were minor disadvantages to using Zoom for FGs. There were occasional difficulties in reading the body language of YP. This resulted in people attempting to talk at the same time or having longer periods of silence during discussion. There were also interruptions that briefly halted conversation due to poor internet connection or other people present in the background of a participant’s screen. The use of Zoom videoconferencing for this cohort and subject matter overcame many barriers, but consideration certainly needed to be given to planning, privacy and operations. 31
Conclusion
The LongSTEPPP Co-Design FG study provides contemporary knowledge on YPs experience of periods and how those supporting and caring for YP may be missing and dismissing the impact of periods.
Herein we have surmised the outcomes of FGs (for YP and their parents) with the major themes emerging being the YPs experience, pain and symptom management and education. The challenge of navigating a chronic pain condition in adolescence and the lack of awareness among societies, healthcare providers and schoolteachers were highlighted. These findings have directed the LongSTEPPP longitudinal study’s design to ensure that the needs and concerns of YP and their parents are adequately represented. This is a first step in encouraging YP to share their lived experience of periods, to best accommodate their needs in research design and in establishing suitable patient-reported outcome measures that capture the impact of period concerns and the success, or otherwise, of management strategies.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057241303003 – Supplemental material for Missing and dismissing the impact of periods. Outcomes of focus groups of teens with period concerns
Supplemental material, sj-pdf-1-whe-10.1177_17455057241303003 for Missing and dismissing the impact of periods. Outcomes of focus groups of teens with period concerns. by Courtney Bree Munro, Madeline Flanagan, Dehlia Moussaoui, Lauren Kite and Sonia R Grover in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.