
Abstract
Although the translation of sex and gender evidence into clinical practice guidelines (CPGs) is strongly advised by specialists, this commitment may be limited to presenting findings on women for specific diseases and topics. The inclusion of sex and gender evidence should deploy available data on health and illness, taking human diversity into consideration, especially when drafting CPGs. This work examines 21 guidelines from Spanish CPGs from 2018 to 2022, scraping sex and gender evidence across documents under the lens of 59 keywords related to sex and gender. Three out of four CPGs included relevant keywords to analyse. Then the set of words was analysed in terms of their frequency, as well as the context of the words (nature and location of the information in the CPG). It found that masculine keywords were widespread in CPGs as a result of an androcentric orientation in clinical research, except for those CPGs centred on women’s issues. CPGs focused on technical procedures tended to omit considerations regarding sex and gender. CPGs developed under the lens of a more sensitive gender approach formulated relevant Patient, Intervention, Comparison, Outcomes (PICO) questions and showed a greater diversity of situations, detailing different types of patients. Even though some CPGs do express good intentions regarding gender mainstreaming – for example, using gendered language and a balanced developers’ group – important omissions and a lack of precise information were still found.
Plain language summary
This work examines 21 guidelines from Spanish CPGs from 2018-2022, scraping sex and gender evidence across documents under the lens of 59 keywords related to sex and gender. Three out of four CPGs included relevant keywords to analyse. Then the set of words was analysed in terms of their frequency, as well as the context of the words (nature and location of the information in the CPG). It found that masculine keywords were widespread in CPGs as a result of an androcentric orientation in clinical research, except for those CPGs centred on women’s issues. CPGs focused on technical procedures tended to omit considerations regarding sex and gender. CPGs developed under the lens of a more sensitive gender approach formulated relevant PICO (Patient, Intervention, Comparison, Outcomes) questions and showed a greater diversity of situations, detailing different types of patients. Even though some CPGs do express good intentions regarding gender mainstreaming – for example, using gendered language and a balanced developers’ group – important omissions and a lack of precise information were still found.
Introduction
The inclusion of sex and gender evidence is essential for learning about human health, in which diversity is considered crucial to promote health equity.1 – 4 Although journal editorials and gender guidelines continue to call for the inclusion of sex and gender in medicine, whether there actually is a complete and accurate implementation of sex and gender outcomes in clinical practice guidelines (CPGs) has been questioned.5 –8
A CPG is a tool for transferring knowledge on health and illness from research to practice, but the development of CPGs involves a complex process of collecting and interpreting the information. ‘[A] guideline is not based on evidence alone [. . .] it is interpreted and weighed for its clinical relevance and cost-effectiveness by representatives of the end-users of a guideline’ (p. 18). 9 With regard to the inclusion of sex and gender evidence, although there is broad consensus that these dimensions must be considered as determinants of health, certain presumptions of objectivity (mainly gender blind) may lead to a lack of awareness of the potential bias. It requires the inclusion of the findings of experiments and analysis that distinguish males and females (sex) and also the implications of being men and women as a consequence of social roles and lifestyles (gender).
Indeed, the collection of evidence on women only for specific illnesses or health concerns (reproduction, breast cancer, etc.) is often used as an argument for ‘inclusion of gender approach’, ignoring the different implications for men and women in almost every field of human health. The goal of gender mainstreaming is to show evidence and concrete information on how sex (biological determinants) and gender (social practices, habits and cultural factors) affect human health and illnesses in different ways.1,10 –12 Incomplete and inaccurate information on male and female characteristics, as well as the inclusion of stereotypical information about women or men, will be detrimental to advancing knowledge and achieving equity.
The aim of this work is to create a methodology to assess what type of sex and gender information the developers have included in CPGs. The analysis is intentionally oriented towards discovering if gender mainstreaming (involving clear evidence related to sex and gender determinants in health) has been included in the knowledge corpus and recommendations detailed in the CPGs. Gender mainstreaming should provide evidence on how males and females are affected differently, and how social determinants on men and women have an influence on illness and health processes. CPGs should display significant evidence on health and illnesses, attending to the diverse characteristics of the population and producing separate recommendations.
One of my previous works examined the CPGs of the Spanish National Health System (SNHS). It provided evidence of the insufficient attention to sex and gender issues in the methodological framework for constructing CPGs. 13 It analysed the differences between Spanish and English gender markers in methodological frameworks and the impact of the gender balance composition of the development teams for Spanish CPGs produced by SNHS under the GuíaSalud Programme (www.GuiaSalud.es). 14 In this work, I continue to analyse the open-access CPGs of the SNHS GuíaSalud Programme, delving deeper into information related to sex and gender-related words.
Materials and methods
Data was collected from the SNHS Programme GuíaSalud, which ensures the open-access publication of guidelines for practitioners, users and managers. Recent and updated CPGs were selected through June 2022 (published in the past 5 years, 2018–2022), resulting in 21 CPGs that were analysed by scraping in 2023.
This computerised method is useful for extracting information from websites and simulating human navigation on the internet. Scraping identifies words of interest across independent documents. The word was located in context (on which pages and sections it appears) and the literal quote was displayed where it was found. The automated search method using scraping was useful for overcoming the variability of the guidelines’ topics and formats. First, a list of words was created and iterated across the CPGs, looking for new words or ways of expressing masculine or feminine references to health conditions. In the end, 59 words were found in the body of the text.9,10 The collection of words includes categories related to men and women (gender), male and female (sex) and related words, for example, mother (‘madre’), father (‘padre’) and parents (‘padres’). All morphological variations were included (e.g. pregnancy ‘embarazo’ and pregnant ‘embarazada’), gender and number markers (girl ‘niña’, boy ‘niño’, girls ‘niñas’, boys ‘niños’ and boy/girl ‘niño/a’). The complete set of keywords is in Appendix 1.
Once the scraping was completed, the set of words was analysed in terms of frequency (quantitative analysis) and the content was analysed in its context (qualitative analysis). A quantitative analysis provides a classification of the evidence revealed in the CPGs, whereas a qualitative analysis informs on the nature and contextualisation of the information (what it says and where it is located, examples, in a table, providing a definition, a comparison, a recommendation. . .). The quantitative and qualitative analyses provided information on the number of keywords, their frequency, and the absence of sex and gender considerations in the SNHS Programme of CPGs. This absence is revealed by the lack of mentions of the keywords included on the list used by scraping. It provides information about the context and type of information in which these keywords were used. The evidence provides information on the intention and awareness of gender in relation to the disclosure of data on men’s and women’s health.
Gender mainstreaming here is a comprehensive assessment of the nature of the information found in the 21 documents expressing sex features, women’s experiences, roles and habits. The analysis points out what kind of approach, if any, is implemented in the production of the CPG based on the following aspects:
Words, including nouns, related to sex and gender (mother, father, boys, girls), and distinguished by gender markers (his parent / her parent).
Contexts in which the keywords are mentioned. The context may indicate the importance of this information (if it is substantial or anecdotal). For instance, if it appears in the main body and in several sections of the document in parallel; conversely, if it only appears once in the document, or it shows examples expressing limited information and providing non-substantial information.
The content and nature of the information provided. What evidence is revealed from a sex and gender approach (e.g. it shows a clear advance in knowledge on human populations, compares differences, shows rates or describes lifestyles and beliefs that lead to healthy behaviours/recovery) and the intention of the message (e.g. if it says that gender differences are important and provides concrete information on which features this comprises; sex and gender are not employed interchangeably and are correctly used). Conversely, evidence is inaccurate, it states the intention and there is no concrete data, or it is mentioned but in vague terms, where the findings and recommendations show uncertain information on sex and gender outcomes.
The Spanish context is important for understanding the peculiarities of this work in three ways. First, the Spanish language (oral and written) presents a handicap since nouns and adjectives are always gendered, and the generalisation of male markers is highly unsatisfactory from the viewpoint of gender equality. Secondly, equality legislation includes the recommendation to use inclusive language in science and to publish male and female results in science as an effective gender equality policy. 15 All these issues are at the basis of citizens’ awareness, with different degrees of socialisation in both expert and lay users. It is in this context that GuíaSalud develops the guidelines for the preparation of Spanish CPGs, in which it recommends the inclusion of evidence with balanced data for men and women (p. 25) 16 and, even if it recognises the importance of using male and female markers in Spanish writing, the decision is made to use male words (p. 1). 16 After that, the developers independently decide whether to give visibility to or ignore the information that informs about sex and gender content and language used in their work elaborating CPGs.
As an initial hypothesis, 14 the author thought that the subject of the CPG would matter and would determine the inclusion of keywords and the importance of inclusion of gender mainstreaming. Those CPGs focusing on techniques and procedures would pay less attention to keywords related to sex and gender issues, as a result of describing processes without mention of patients; whereas CPGs focused on ‘women’s health’ (e.g. breast cancer and reproductive health) would extensively employ evidence and data on women and the female body.
Results
Only 16 of the 21 CPGs include some wording related to patients’ sex and/or gender. The variety of topics where these words are included or excluded refutes the idea that certain types of topics are more likely to be related to the sex and gender of patients. The CPGs focused on techniques and procedures also mention these words (e.g. Nursing Haemoculture) and, conversely, the CPGs focused on the treatment of patients do not mention them, like the guide to Chronic Obstructive Pulmonary Disease or pharmacological treatment. The topic does not seem to explain the presence/absence of wording related to sex and gender.
Table 1 summarises the frequency of words mentioning sex (varón/es and hembra/s) and gender (hombre/s and mujer/es) in CPGs. All variants of the Spanish words and 21 CPGs were included in the search. The displayed data (Table 1) refers to those CPGs in which some of these words were mentioned, disregarding those in which none of them were mentioned. It also shows the frequency of appearance of those words used at least once, while it excludes words that were not mentioned (e.g. none mention ‘macho’, so it does not appear, but ‘hembra’ has three mentions in one specific technical guideline).
Word frequency related to male/female, men/women in CPGs.

Source: Own elaboration.
CPG: clinical practice guideline.
The total frequency (Table 1) shows more mentions of women (‘mujeres’, 81.75%) than men (9.2% for both words: ‘hombres’ 5.52%, and ‘varones’ 3.68%). But, while men are widespread throughout the guidelines, women (‘mujer’ and ‘mujeres’) are only mentioned in three guidelines: antimicrobial therapy, contraceptive methods, and breast cancer. The other two guidelines where female and women (‘hembra’, ‘mujer’ and ‘mujeres’) are mentioned more times than male and men: COVID paediatric (23 versus 14) and nursing haemoculture (4, none); while men (all types) are cited more often than women in basal cell carcinoma (2, none) and thoracic trauma (6, none).
Language issues
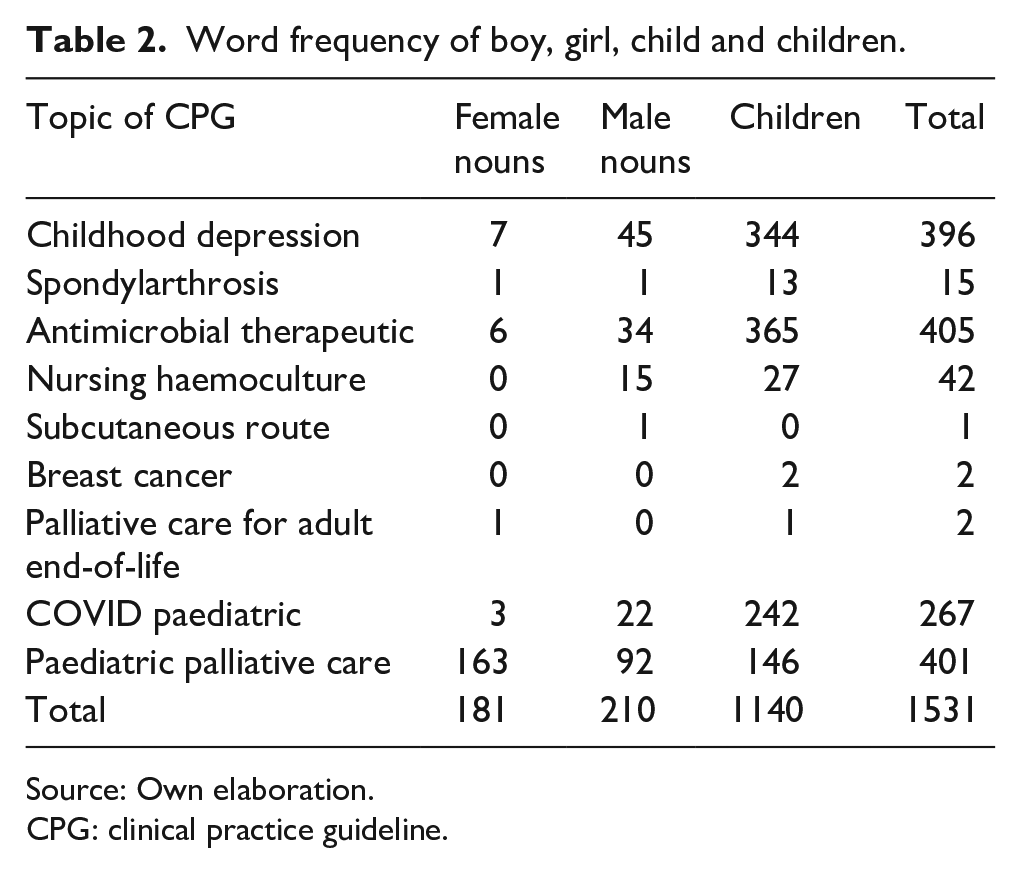
Gender markers in the Spanish language are important for understanding the following results (Tables 2 and 3), which usually bear in mind gender equality protocols of using inclusive language. To include both sexes (without female exclusions), language usage guides recommend using collective nouns instead of singular nouns (children instead of boy, parents instead of mother).
Word frequency of boy, girl, child and children.
Source: Own elaboration.
CPG: clinical practice guideline.
Word frequency of mother, father and parents.

Source: Own elaboration.
CPG: clinical practice guideline.
In the wording of their guidelines, most developer groups try to follow inclusive language protocols (Table 2). They show a higher use of collective nouns (‘niño/a’, ‘niños/as’, ‘hijo/a’) than girl/s (‘niña’, ‘niñas’, ‘hija’, ‘hijas’, ‘chicas’) and boy/s (‘niño’, ‘niños’, ‘hijo’, ‘hijos’). These categories are grouped together under the labels: children, female nouns and male nouns, respectively. Table 2 shows that male nouns outnumber female nouns when mentioned in the singular, indicating an incorrect use of gender inclusion markers, or a male preference to include boys rather than girls in data collection.
About the context of these wordings, the qualitative analysis indicates blind gender mainstreaming. The lack of information on how girls and boys are treated differently for health issues was particularly significant in the three guidelines that focused on the adolescent population. The feminisation of caretakers is clear when the CPG analyses the frequency of use of the words mother (‘madre’), father (‘padre’) and parents (‘padres’). Table 3 below shows that ‘mother’ is mentioned more often than ‘father’. It reveals that women continue to be in charge of family care, but constant repetition confirms their stereotypical role. The role of women in the family’s healthcare is overused in all these guidelines where women are always considered the caretakers of children, the elderly and the ill.
Analysing specific CPGs
Further analysis requires attention to the CPGs as a whole. This section draws some learnings from four of them. The CPG commissioned by the Spanish Rheumatology Society on the treatment of gout patients deserves special attention for good reasons. 17 Although the topic would suggest technical information, disregarding sex and gender, and even though this stereotypical disease traditionally has a greater prevalence among males, information on females appears in this guideline, as well as information related to gender. First, quantitatively, ‘hombre/s’ and ‘mujer/es’ are mentioned an equal number of times (26). Further, the content and contextual information detailed in the phrases in which they appear make it clear that the CPG adopts a sex and gender approach. Second, it presents sex information separately on how gout affects men and women differently; third, it mostly includes an intersectional analysis, meaning that it considers overlapping factors that affect patients in combination, rather than each factor in isolation (e.g. ‘By sex, the adjusted Disability Adjusted Life Years rates for gout in Spain are four to five times higher in men than in women throughout the period 1990–2017’ (p. 31) 17 ). It presents textual and graphical information showing data differences between men and women for disability, race and age throughout the CPG (on pages 32, 33, 34, 77, 96, etc.), which is, fourth, a valuable insight. Fifth, the information is presented broadly in the whole guideline, rather than on just a few pages, which demonstrates a strong commitment to show evidence from a gender perspective, rather than an erratic interest.
The gout CPG explains findings on sex: ‘Gout is more common in males, with prevalence increasing with age. However, female prevalence rises faster after menopause’ (p. 35). 17 The guideline also identifies gender issues related to social roles, linked to prejudices about men and women: ‘There are also women who were initially reluctant to accept the diagnosis of gout from their GP because of the beliefs and stigma associated with the diagnosis’ (p. 107) 17 and ‘There is a distinction to be made about gout in women. Some women do not understand the disease well and find it difficult to find information that seems relevant to them because most of it is aimed at men’ (p. 112). 17 Gender mainstreaming is not only focused on how women react to the illness but also on men’s reactions, for example, ‘In the search for published studies, the role played by the ideal of masculinity appeared and how some men refused to go to the doctor, out of “shame”, after the first acute attack of gout [. . .]. Patients wonder why gout is more frequent in men than in women’ (p. 113). 17
Spondylarthrosis, commissioned by the same medical association, is another good example of a guideline created by developers with an awareness of gender mainstreaming. 18 Both documents (gout and spondylarthrosis) share the same features: a balanced number of mentions of ‘hombre/s’ and ‘mujer/s’, separate information (ratios and factors) for males and females throughout the document, and key sentences considering the gender roles of men and women: ‘The mothers identify their problem and highlight the impediment to being capable of handling the workload of caring for their children. Parents describe as very important the change in their family life caused by the difficulties of being able to play with their children, a problem that is in addition to the lack of energy they experience to be able to help with household chores’ (p. 104) 18 and ‘It is a more pronounced trait in men, for whom the satisfactory feeling of being supermen disappears (a Superman capable of everything), which is a great blow to masculinity. The disease affects the ability to be the ideal father that, within the socially established criteria, is expected of them’ (p. 106). 18
The CPG on paediatric palliative care does not report differences between girls and boys in diagnosis, treatments or behaviours. 19 Some mentions do not provide substantial information: ‘a 17-year-old adolescent described how 50% of her understanding came from the healthcare team and 50% from her parents’ interpretation’ (p. 119) 19 and imprecise information (p. 114) 19 : ‘The dosage depends on the intensity of the pain, the intensity of the patient’s pain, the patient’s previous history of analgesic requirements and the patient’s body weight and sex (the highest plasma concentrations occur in females [originally ‘mujeres’])’ (p. 114). 19 How large is the plasma concentration in female patients? To what degree does this influence the female and male doses?
Likewise, the COVID-19 paediatric guideline, where male nouns exceed female nouns, seemingly asks about the sex of the patients: ‘The risk of poor prognosis has been associated with various factors by different studies: age outside 1–4 years old (especially those younger than 1 month), male sex, suffering from underlying diseases’ (p. 8), 20 but it does not provide quantitative data or details. The CPG on childhood depression presents ambiguous Patient, Intervention, Comparison, Outcomes (PICO) questions that prevent the collection of evidence and recommendations by sex and gender: ‘Target population: the groups considered by the CPG are children (5–11 years old) and adolescents (12–18 years old) with major depression (depressive episode according to ICD-10/major depression according to DSM-5)’ (p. 36). 21 Accordingly, the guideline presents a lack of knowledge on patients’ diagnosis, treatment, outcome and recovery by sex and gender.
The lack of reference to sex and gender differences (in diagnosis, treatment and care) in practical guidelines on adolescent conditions deserves attention. The childhood depression CPG includes a social approach (due to interest in learning about the family setting), but it falls short of gender mainstreaming and does not provide information on how it affects girls and boys differently. The COVID paediatric CPG could be attributed to scant research because of fast publication to respond to physicians’ demands (its publication date is 2022), but paediatric palliative care displays imprecise and irrelevant data related to patients’ sex and gender. This weakness suggests that more attention should be paid to the accuracy of data on human health.
Discussion
The analysis reveals how CPGs handle sex and gender. A result that derives from the Spanish context (Spanish writing norms, inclusive language protocols, gender equality legislation 15 ), the GuíaSalud Methodological Guide for drafting guidelines, 16 and the specific work of guideline developers on each CPG.
The findings show room for improvement, despite progress and good examples. CPGs are compromised by inaccurate or incomplete information, which threatens their value and quality, as well as their recommendations for professionals, patients, families and managers.7,8 Despite consensus on sex and gender as health determinants and explanatory variables for illness and recovery,1,2,5,22 one in four guidelines still does not include information on sex and gender.
The topic of the guidelines does not seem to be important in explaining this lack of information. CPGs related to patients’ conditions contain few words and phrases informing about sex and gender issues, whereas other topics related to technical procedures (which could be assumed to be less deserving of attention to patients’ sex and social roles) include information on consideration of sex/gender. An alternative hypothesis stated a positive relationship based on the balance of men and women comprising the developers’ group. 14 However, this hypothesis was rejected (p = 0.583). 14 There are CPG examples of male predominated groups of developers that do pay attention to sex and gender issues, confirming no relationship between the gender balance of the developers’ group and the adoption of gender mainstreaming. A better explanation emerges from the findings related to the inclusion of relevant PICO questions involving sex and gender issues. When teams introduce PICO questions with gender mainstreaming, such as the Spanish Rheumatology Society (SER), they show sex and gender-related outcomes. Thus, a recommendation to developers and medical societies should be to consider relevant sex and gender issues in the PICO questions; and manuals and guidelines to prepare CPGs should display good practices and advice to include more evidence on sex and gender.
As Ballantyne and Rogers 12 have explained, clinical guidelines still fail to select data-presenting studies where men and women are recruited equally in experiments and studies. Androcentrism breeds gender blindness. Therefore, CPGs fail when there is a lack of information on sex and gender, and when this evidence and the recommendations are not presented differently to explain the particular illness processes for men and for women. Women are absent from guidelines on most topics, except when guidelines are related to reproductive issues, precisely when men are absent.1,22 The lack of reference to men in the contraceptive guideline reflects the scant attention they receive as subjects of contraception. Similarly, although breast cancer has a low prevalence in the male population, it seems relevant to collect the available evidence, precisely because of its exceptionality. A rare condition seems a good reason to include the available evidence to help guide professionals and patients.4,22
This opens the discussion on the selection of evidence in the production of clinical guidelines, which are subject to interpretation beyond medical and objective data. 9 Eicher and Burke 3 have argued that guidelines reflect power hierarchies in society, with a discourse contaminated by sexism and racism. The results of this research suggest that stereotypes about women’s caretaking roles remain and that the male responsibility of caring for the family is not represented.
Recent debates on sex and gender, as well as the expression of gender identity, may influence the people involved in the research and preparation of CPGs 4 ; on the one hand, to enhance awareness and, on the other, to add complexity to their work. It raises the recommendation of training practitioners and organising workshops to discuss the issues that may concern them. Open discussions may resolve doubts and create common understandings. Further, regarding training, inclusive language is acknowledged as the first step to overcoming sexism, 16 but this rule is useless if people ignore the purpose: to make the diversity visible that affects health equity. When it is used incorrectly in the production of clinical guidelines, inclusive language can create confusion surrounding to whom and why the recommendation is presented. Eventually, it generates doubts about the evidence of how sex and gender have an influence on disease and recovery. Study results recommend training for practitioners and developers in using gender markers and explaining why accurate language creates benefits for patients.
A limitation of this study is the confinement of the Spanish case, which refers to a narrow context and peculiarities of languages and culture. First, the number of documents is small compared to large databases containing CPGs written in English. Second, language may involve difficulties in translating evidence from trials and clinical practice to CPGs, particularly because the meta-analysis of evidence is mainly collected from English-language literature. Third, Spanish culture and political discourses may have an important influence on the decisions of the development group.
Conclusion
The present work addresses the lack of evidence and nature of information included in the SNHS CPGs related to a sex and gender approach. The results confirm small steps in this direction but also reveal problems related to a complete and correct inclusion of sex and gender mainstreaming in clinical guidelines. Those CPGs with relevant PICO questions whose aim is to show the variability of human health, considering men and women from a biological sex and gender role viewpoint, provide more quantitative and qualitative information.
Gender balance in CPG developers’ groups and the use of gender markers are good practices for a variety of reasons. However, they are insufficient to advance awareness and the correct inclusion of sex and gender mainstreaming in the development of CPG content.
The sex and gender approach opens the door to learning about human health and disease processes, even when stereotypes and prevalence suggest that the condition is exclusive to one sex, age or race. It is not only a question of justice, but also about recognising diversity and overcoming the androcentrism that prevails in medicine.
Footnotes
Appendix 1
‘sexo’, ‘sexos’, ‘género’, ‘generos’, ‘genero’, ‘sexual’, ‘sexuales’, ‘homosexual’, ‘homosexuales’, ‘hombre’, ‘hombres’, ‘varón’, ‘varon’, ‘varones’, ‘mujer’, ‘mujeres’, ‘hembra’, ‘hembras’, ‘masculino’, ‘masculinos’, ‘femenino’, ‘femeninos’, ‘femeninas’, ‘femenina’, ’madre’, ‘madres’, ‘padre’, ‘padres’, ‘embarazada’, ‘embarazadas’, ‘embarazo’, ‘embarazos’, ‘gestante’, ‘gestantes’, ‘intersexual’, ‘intersexuales’, ‘niño’, ‘niños’, ‘niña’, ‘niñas’, ‘niño/a’, ‘niños/as’, ‘hijo/a’, ‘hijo’, ‘hijos’, ‘hija’, ‘hijas’, ‘chicas’, ‘male’, ‘female’, ‘mother’, ‘parents’, ‘father’, ’girl’, ‘child’, ‘children’, ‘boy’, ‘kid’, ‘kids’.
Acknowledgements
I thank Eduardo Rojas Vázquez for programming the scraping process under my own methodological decision, also Mary T. Bauer for language support during the writing and editing of this work. I feel very thankful for the collaboration of people in Guía Salud at the IACS (Instituto Aragonés de Ciencias de la Salud – Aragon Health Sciences Institute), their help and warm cooperation in preparing this work were unique and one of a kind. I also want to express my gratitude to the Sociedad Española de Reumatología (SER, Spanish Society of Rheumatology) for their valuable input on the telephone and for answering my questions to complete information in this work.