
Abstract
Background:
Stigma and lack of social support are barriers to HIV prevention, especially among cisgender Black women in the United States. While HIV pre-exposure prophylaxis (PrEP) can decrease HIV transmission, PrEP initiation and adherence remains low among Black women, especially in the U.S. South.
Objectives:
The purpose of this study was to characterize experiences with stigma and social support among PrEP-naïve and PrEP-experienced Black cisgender women in Mississippi.
Design:
Qualitative study in which semi-structured interviews and focus groups were conducted.
Methods:
We purposively recruited PrEP-naïve cisgender Black women who met PrEP indications to participate in focus groups and all PrEP-experienced cisgender Black women at a sexual health clinic in Jackson, Mississippi to participate in one-on-one semi-structured interviews. Inductive thematic analysis was used to analyze focus group and interview transcripts.
Results:
A total of 37 PrEP-naïve Black cisgender women participated across 6 focus groups and 8 PrEP-experienced cisgender Black women completed semi-structured interviews. Four themes were identified: (1) the intersection of gendered racism, discrimination, and HIV stigma, (2) enacted and anticipated PrEP stigma, (3) stigma mitigation strategies and PrEP adherence, and (4) social support’s role in PrEP initiation and adherence. PrEP-naïve and -experienced Black women discussed the negative consequence that sexual stigmatization and gendered racism has on HIV testing. PrEP-naïve Black women discussed how HIV stigma decreases PrEP initiation. Conversely, PrEP-experienced Black women were able to identify strategies they utilized to mitigate stigma. PrEP-experienced Black women discussed how differing levels of social support impact their PrEP use.
Conclusion:
Improving social support and stigma mitigation strategies could help improve PrEP initiation and adherence among cisgender Black women at-risk of acquiring HIV in the U.S. South. Educating communities on PrEP, and training providers on stigma-mitigating strategies when serving Black women in the U.S. South who are seeking HIV prevention is paramount.
Plain language summary
Why was the study done?
Stigma and lack of social support have been demonstrated as barriers to HIV prevention, especially among cisgender Black women in the United States (U.S.). While HIV pre-exposure prophylaxis (PrEP), a HIV prevention medication, has the ability to decrease HIV transmission, rates of starting PrEP remain low among Black women, especially in the U.S. South. Improving PrEP programs for US Black women calls for understanding how stigma and social support impact PrEP use among Black women.
What did the researchers do?
We recruited cisgender Black women who was eligible for PrEP but have never taken PrEP (PrEP-naïve) to participate in focus groups and cisgender Black women who have taken PrEP (PrEP-experienced) to participate in one-on-one in-depth interviews from healthcare clinics in Jackson, Mississippi. Inductive thematic analysis was used to analyze focus group and interview transcripts.
What did the researchers find?
A total of 37 Black cisgender women across six groups participated in focus groups and eight cisgender Black women were interviewed. PrEP-naïve women reported: · HIV stigma in the community, which can lead to anticipated PrEP stigma · Experiencing sex-based sexual stigmatization at provider’s offices when seeking HIV testing PrEP-experienced Black women reported: Experiencing stigma when disclosing their PrEP use, such as their family and friends thinking that the woman and/or her partner is living with HIV. PrEP-experienced Black women who were in serodifferent partnership and had others in their network who knew about PrEP received support to take PrEP.
What do the findings mean?
Improving social support and stigma mitigation strategies could help improve PrEP initiation and adherence among cisgender Black women at-risk of acquiring HIV in the U.S. South. This includes educating communities on HIV and PrEP, and training providers on stigma-mitigating strategies when serving Black women in the U.S. South.
Introduction
HIV pre-exposure prophylaxis (PrEP) is an effective biomedical intervention that can decrease HIV transmission, yet uptake among Black cisgender women in the United States remains suboptimal. 1 Black women comprise almost half (47%) of new HIV infections among all U.S. women. 2 As a result of high HIV transmission, Black women are listed as a priority group within the Ending the HIV Epidemic (EHE) plan. 3 Yet, in 2018, less than 5% of all PrEP users were cisgender women, with Black women making up a fraction of these users. 4 In 2019, the Centers for Disease Control and Prevention (CDC) estimated that only 12.4% of women who could benefit from PrEP were being prescribed it. 5 Addressing the persistently low uptake of PrEP among Black cisgender women in the United States is imperative to achieving the goals of the EHE plan and reducing the disproportionate impact of HIV on this vulnerable population.
Mississippi faces a disproportionate burden of new HIV diagnoses, particularly among Black women. In Mississippi, the rate of new HIV diagnosis is five times higher among Black women compared to white women. 6 Mississippi has one of the highest rates of new HIV diagnoses across the United States, with a rate of 17 new HIV cases per 100,000 people compared to a rate of 13 per 100,000 in the country. 7 Black people make up the majority of these new cases (73.7%) despite comprising less than half (44.3%) of PrEP users in the state. 7 Sociostructural barriers, such as a lack of Medicaid expansion, contribute to HIV disparities. 8 Addressing these stark disparities in HIV diagnoses and PrEP utilization among Black women in Mississippi demands urgent attention and targeted interventions to ensure equitable access to preventive healthcare and reduce the disproportionate burden of HIV within this community.
The intersection of sociostructural factors, systemic barriers, and healthcare disparities in the U.S. South profoundly impacts HIV-related outcomes and PrEP initiation. High levels of poverty, low health literacy, HIV stigma, and a lack of Medicaid expansion disproportionately affect HIV-related outcomes in this region.8 –10 Moreover, racism, discrimination, and medical mistrust hinder PrEP initiation, which create barriers to healthcare utilization for Black women. 11 Intersecting social positions (i.e., race, class, gender) and power compound these challenges by constraining Black women’s decision to initiate PrEP.1,12 For example, Black women can fear judgment over their decision to take PrEP,12 –14 such as their social network assuming they are taking PrEP because they have HIV rather than trying to prevent acquisition. 12 Addressing these barriers is critical to enhancing PrEP initiation in this region. Addressing and mitigating PrEP stigma is crucial for improving PrEP access and adherence, particularly among marginalized populations such as Black women in the U.S. South.
Widespread HIV-related and PrEP stigma has also affected PrEP coverage,15 –17 PrEP stigma has led to disparities in PrEP uptake, with uptake being slower among key populations such as communities of color.18,19 Although current and potential PrEP users often face stigma at the community level, this stigma is reinforced and intensified by factors at other levels, including PrEP programming, policies, and procedures (e.g., the wording of clinical guidance for PrEP eligibility).18,19 PrEP stigma not only impacts potential user’s interest in PrEP but also the adherence of current PrEP users.18,19 For example, PrEP users are often stereotyped as promiscuous or as having risky sexual behaviors, which has influenced perceived PrEP candidacy (i.e., PrEP interest), adherence, and discontinuation. 19 In the U.S. South, PrEP stigma has diminished Black women’s engagement in PrEP care. 20
Social support may be an effective strategy for addressing experienced and anticipated stigma.21,22 Social support can function in a variety of ways for HIV prevention and treatment, such as emotional (e.g., affection), appraisal (e.g., affirmations), informational (e.g., advice), and instrumental (e.g., money) support. 23 For stigmatizing conditions, social support groups can help to reduce stigma by serving as a source of information exchange and dissemination, which equips individuals with vital information to manage their diagnosis. 24 Social support programs led by peers can combat HIV stigma by promoting empathy and mutual understanding for those living with HIV, aiming to prevent HIV, and their advocates. 25 For people living with HIV in Mississippi, they reported how social support groups helped them to cope with their diagnosis and to build a sense of belonging in the community but were difficult to find. 25 While most existing literature has focused on the use of social support groups for managing diagnoses such as HIV, there is an opportunity to examine how social support may impact HIV prevention in Mississippi to improve PrEP initiation.
While prior research has studied the effect of stigma on HIV-related outcomes among individuals living with HIV and on HIV prevention outside of the U.S. South, expanding this work to Jackson, Mississippi affords the opportunity to decrease HIV transmission among Black women. Given the pervasiveness of HIV and disparities in PrEP initiation, understanding how stigma and social support contribute to sociostructural barriers that Black women experience could help to increase PrEP initiation for Black women in this region. Therefore, the purpose of this study was to characterize experiences with stigma and social support on PrEP initiation and adherence among Black cisgender women in Jackson, Mississippi. Notably, our study included both PrEP-experienced and PrEP-naïve Black women. Comparing and contrasting experiences across these two groups could provide insights into the factors influencing both PrEP initiation and adherence among Black women to inform future interventions.
Methods
Focus group discussions (FGDs) with PrEP-naïve cisgender Black women and individual semi-structured interviews with PrEP-experienced women who are involved in PrEP clinical services at a sexual health clinic in Jackson, Mississippi were conducted.
Focus groups
Methods presented in this manuscript have been previously published. 26 PrEP-naïve Black women (n = 37) were recruited between February and June 2019 through a combination of flyers left at a sexual health clinic and posted to the clinic’s Facebook page. The flyers directed potential participants to an online eligibility screener and also had a phone number where Black women could call to opt-in for the study. Women were eligible to participate if they: (1) were aged 18 or older; (2) self-identified as a Black or African American cisgender woman; (3) self-reported HIV-negative status; (4) resided in Mississippi; (5) spoke English; and (6) self-reported at least one substantial risk factor for HIV infection per the 2017 CDC PrEP Eligibility Guidelines for heterosexual women. Substantial risk factors included having a sexual partner living with HIV or with an unknown HIV status, being diagnosed with a bacterial sexually transmitted infection (STI), having two or more sexual partners, using condoms inconsistently or not at all, and engaging in sex work. 27 Eligible women were invited to participate in one-time, 90-min FGD. During the six FGDs, women were asked about: (1) PrEP knowledge; and (2) PrEP uptake barriers and facilitators (Appendix 1). Participants were remunerated $50 for their time.
Interviews
Methods presented in this manuscript have been previously published. 28 PrEP-experienced Black women (n = 8) were recruited between June 2019 and June 2020. Only eight Black women were recruited since these were the only PrEP-experienced Black women in the clinic at the time of study recruitment. Black women were purposively sampled from a PrEP program within a sexual health healthcare clinic in Jackson, Mississippi. Women were eligible to participate if they: (1) were aged 18 or older; (2) self-identified as a Black or African American cisgender woman; (3) spoke English; and (4) had a history of PrEP use, as indicated by a current or former PrEP prescription. The interview included questions regarding social, structural, and health system factors related to their experiences during PrEP initiation, adherence, and retention (see Supplemental Files: Appendix 1). Interviews were conducted over the phone or in-person and lasted 45–60 min. Participants were remunerated $40.
Shared data collection procedures
All interviews and focus groups were conducted by Black cisgender women public health researchers trained in qualitative research methods. After each session, the research team debriefed and wrote analytical memos. Interviews and FGDs were audio-recorded and transcribed verbatim by a HIPAA-compliant transcription company. All study procedures were approved by Institutional Review Boards at Brown University and Johns Hopkins Bloomberg School of Public Health.
Defining terms
In this manuscript, we use cisgender woman to denote someone whose assigned sex at birth was female and who also culturally identifies as a woman. 29 We use HIV stigma to denote the stigma experienced by individuals living with HIV, their intimate partners, and their caretakers. 30 We use PrEP stigma to denote stigma surrounding what the PrEP medication is and what the medication does for individuals who are thinking about using and currently using PrEP, including any negative assumptions of individuals who use PrEP. 18 We use sexual stigmatization to denote differential judgment of women for engaging in the same sexual acts as men. 31 Anticipated stigma is used to denote real or imagined concerns that attitudes and thoughts could result in future discriminatory behaviors. 32 Conversely, experienced stigma is used to denote actual discriminatory behaviors that has been directed at an individual based on a condition or specific attribute. 32
Data analysis
Transcripts from the FGDs and interviews were coded, and thematic analysis was completed using a general inductive approach. To utilize this approach, an interdisciplinary team of four coders, including the interviewer and one of the focus group moderators, open-coded two interviews and FGDs to determine initial inductively derived codes. Next, we conducted line-by-line coding using those derived codes to finalize separate codebooks for the interviews and FGDs using those inductive codes through an iterative process. The remaining interviews and FGDs were coded based on their respective finalized codebook by two coders. This iterative process allowed us to determine that thematic saturation was achieved. Team meetings were used to discuss inconsistencies in code application and interpretation as well as prior assumptions and experiences that shaped data interpretation. All transcripts were coded using Dedoose Version 4.5. 33 Consolidated criteria for reporting qualitative research (COREQ) guidelines were followed while preparing the manuscript (see Supplemental Files). 34
Reflexivity statement
The first author is a Black cisgender woman from the U.S. South who helped to code the data and lead analysis of the coded segments for interpretation of results for this manuscript. Two Black women co-authors facilitated all the FGDs. Of the moderators, one is from Mississippi, assisted with development of the interview guide, served as the point of contact with the recruitment site, and assisted with interpretation of results. The other moderator, the senior author, is from the U.S. South, conducted all the interviews, was trained in qualitative research methods, and oversaw the analysis of the data. The two main coders were also Black cisgender women from the U.S. South. Information on the identities of the team was disclosed to participants at the time of recruitment and data collection.
Results
Sociodemographic characteristics
Table 1 summarizes the characteristics of the 37 PrEP-naïve Black women who participated in 6 FGDs and the 8 PrEP-experienced Black women who participated in interviews. FGD participants had an average age of 32, were mostly employed, and heterosexual. Most FGD participants had access to healthcare services within the past year. Among the eight individual interview participants, the average age was 33. The majority of these women were employed, heterosexual, and single. Most individual interview participants had taken PrEP within the past month.
Focus group and individual interview participants demographic and sociodemographic characteristics.
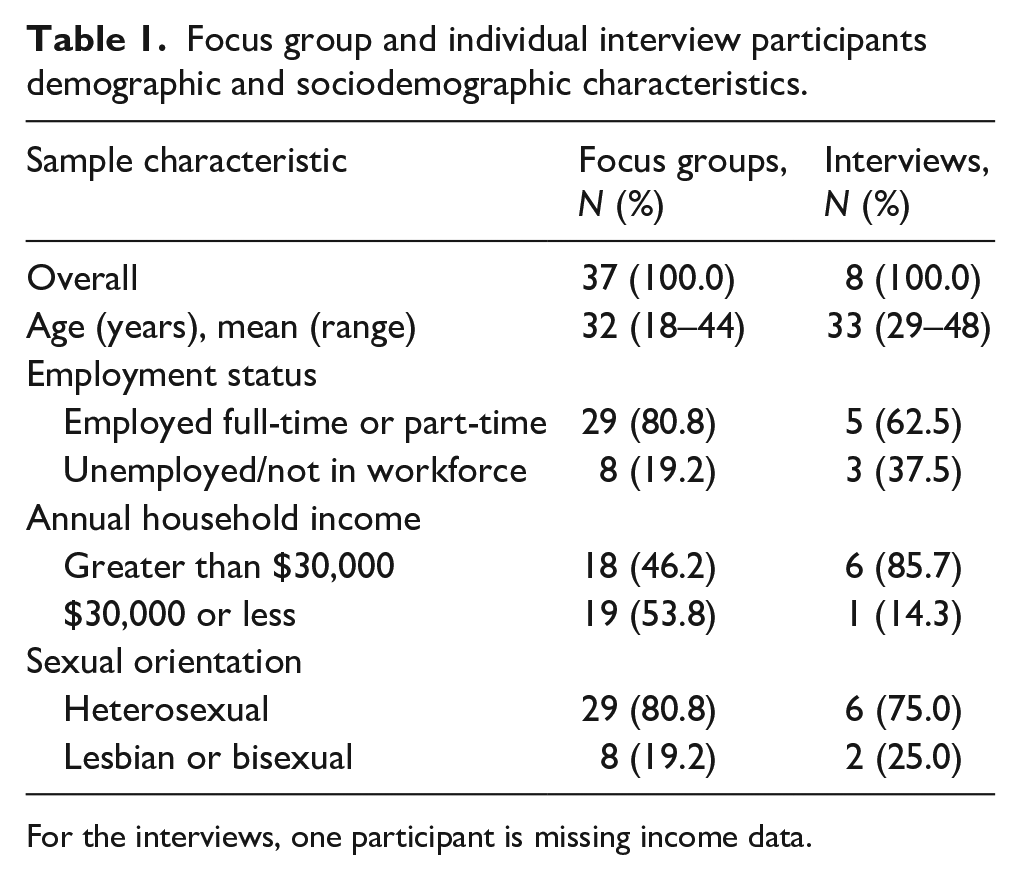
For the interviews, one participant is missing income data.
Themes
Intersection of gendered racism, discrimination, and HIV stigma
Some PrEP-naïve Black women shared experiences of times when they trusted their partner and later found out that the partners were dishonest. For example, this PrEP-naïve Black woman compared acquiring a STI to having an “invisible scarlet letter.”
“I guess, an invisible scarlet letter [to have an STI] . . .you’re trusting your partner that everything is well. And you end up having a STI and you’re questioning yourself, as well as your partner.”—PrEP-naïve FGD Participant 6
In this quote, the scarlet letter symbolized the emotional suffering and social consequences of acquiring a STI from your partner, which can be stigmatized by the larger community. Gendered racism has legitimized hypersexual activity among Black women as a victim blaming strategy for STI acquisition. However, this quote illustrates that Black women are getting STIs from trusted partners, not because of their own hypersexual activity. The emotional suffering of acquiring a STI is so great because people assume that they acquired the STI due to their own behavior, instead of the behavior of their partner.
Black women also experience sexual stigmatization when seeking HIV prevention services. When Black women asked for an HIV test, a few women were met with judgmental questions from healthcare providers. In some cases, women were even denied a test and had to advocate for themselves to be tested, as discussed by this PrEP-naïve Black woman.
“. . .I asked for a STI test last year when I did my wellness, and she was like, ‘We don’t give it if I don’t think you promiscuous.’ But you don’t know me to know if I’m promiscuous or not, but she denied [the HIV test]. . .Why do you have to be promiscuous though?”—PrEP-naïve FGD Participant 6
Experiences such as these made it impossible for women to access HIV testing because this healthcare access was solely dependent on their providers’ perceptions of women’s sexual behavior, and women were also concerned about future instances of sexual stigmatization from medical providers. This quote also is an example of gendered racism and medical paternalism in healthcare settings, where Black women are stating what they need from their providers and are being told that they do not need it. In this case, this Black woman is stating that she needs STI testing and is being restricted from HIV testing, which is a discriminatory behavior that could have future consequences such as restricting her access to PrEP since HIV testing is a precursor to PrEP initiation.
Enacted and anticipated PrEP stigma
PrEP-experienced Black women discussed the lack of HIV disclosure in the Black community. Despite conversations that Black women initiate about HIV and sexual health in their relationships, they stated that individuals may be dishonest about their HIV status. For example, this PrEP-experienced Black woman shared that individuals may not disclose their HIV status because of HIV stigma in the community.
“. . .they are not going to be quick to tell somebody they [HIV] positive. We are having unprotected sex or whatever, protected sex or whatever, and they [think the partner] negative. . .So they can talk about it [HIV status], but I still think that everybody’s going to say they [HIV] negative. . .I don’t know how fast people are willing to admit [they are living with HIV]. . .that’s a negative image. . . .when HIV first came out, people were dying from it. . .I think for average people sex [and HIV] is not an easy topic. Let’s say that. I don’t want to use the word dirty. . .to have HIV is not a good. . .”—PrEP-experienced Interview Participant 5
This Black woman suggests that one reason people do not disclose their HIV status is the fear of being stigmatized and judged by others. This anticipated HIV stigma leads them to protect themselves by limiting disclosure of their HIV status. Yet, the resulting consequence could be HIV transmission to sexual partner, such as Black women, who are not fully informed of their HIV risk in that sexual relationship.
HIV stigma experienced by Black women’s partners who are living with HIV prevented Black women’s disclosure of PrEP usage. For example:
“. . . his friends that he hangs around, they don’t know [he is living with HIV]. Because, you know, a positive person feel like their friends and family will disown them and they have to be by them self. . . But then once you tell somebody that I’m negative and I’m taking PrEP, you know, the first thing they going to say, ‘What’s PrEP?’ PrEP for people that are negative that have been dealing with people that’s positive. And, see, his friends, my friends, my family, his family know that me and him been talking for years. And, see, if they find out I’m taking PrEP, they’ll know [he is living with HIV]. . .it hard for other women to come out and say that because they feel like family and then friends going to know that they’re dealing with is positive or they’ve dealt with someone that’s positive.”—PrEP-experienced Interview Participant 1
For PrEP-experienced Black women in serodifferent relationships, they feared that disclosing their PrEP usage would also disclose their partner’s HIV status to individuals who were previously unaware of their partner’s status. This fear was a result of witnessing their partner experiencing HIV stigma and were later ostracized from their community or disowned from their families. Therefore, witnessing this HIV stigma influenced some PrEP-experienced Black women’s desire to hide or not disclose their PrEP use. When some PrEP-experienced Black women overcame their fear of disclosing PrEP, they experienced difficulties with people thinking that they were living with HIV, as detailed by this PrEP-experienced Black woman.
“So, the only time that I would say that taking it [PrEP] was a problem is when someone like, looked it up because it’s Truvada. And it’s the anti-retroviral thinking that I’m [HIV] positive, and so that has been the most difficult part in taking or dealing with the PrEP. Like, my daughter, thought that you know, my mom must be positive—the reason why she is taking this medication. And the same thing with my aunt. She did the same thing, you know.”—PrEP-experienced Interview Participant 5
While this quote highlights stigma experienced from family members, PrEP-experienced women who had HIV-negative partners also experienced PrEP stigma from their partner when disclosing their PrEP usage. For example, this Black woman reported facing negative feedback from her partner and father, who both made assumptions about who qualified for PrEP and her sexual activity.
“Well, he [partner] was kind of, like, the Truvada’s not for general people. It’s for the gay community. But I told him heterosexuals take them too. It’s for precaution to prevent the virus. I just told him what I knew, but he said he had seen the commercial. . .my dad would kind of say like ‘. . ., you probably got a sex addiction or something.’ ‘You have to learn how to slow down, you know.’ And then, when I went and finally took my first STI test before my second pregnancy, I was clean. I rubbed it all in my daddy’s face. I was like, ‘I’m clean, daddy. Don’t know what you are talking about. I’m clean.’”—PrEP-experienced Interview Participant 6
For this woman, her partner and father highlighted their assumptions that PrEP is for specific communities. Instead of supporting her PrEP usage, she was stereotyped as someone who was overly sexual and just needed to change her sexual behavior.
PrEP-naïve Black women also discussed the consequences of marketing PrEP to specific communities and of branding it as a “HIV medicine.” Subsequently, they stated that the marketing and branding prevents them from initiating PrEP since they anticipate stigma from using PrEP. For example:
“For me, it’s even at the pharmacy. You have to go to the pharmacy. You never know who works there. You don’t know who works where, who got access to your medical records and all that. Like—Judgment. [multiple FGD participants in agreement]”—PrEP-naïve FGD Participant 6
In an FDG where multiple Black women agreed with her, a PrEP-naïve Black woman shared her experiences of anticipating stigma while picking up a PrEP prescription from the pharmacy. This quote highlighted the social context that Black women consider as they think about initiating PrEP and how stigma shapes their decision-making.
Alternatively, PrEP-experienced women iterated lived experiences that were like the anticipated stigma that PrEP-naïve women feared by also sharing stories of how they experienced stigma when picking up PrEP from the pharmacy. For example:
“I had to go pick it [PrEP] up. . .people are looking at it, like, you’re nasty or something. To me, I’m protecting myself because condoms do break and stuff. . .”—PrEP-experienced Interview Participant 7
Stigma mitigation strategies and PrEP adherence
PrEP-experienced Black women discussed several strategies they utilized to mitigate PrEP stigma while they maintained their regimen. One strategy PrEP-experienced Black women discussed was avoiding disclosure of PrEP usage. To decrease the risk of people finding out about their PrEP usage, this Black woman reported saying she is taking vitamins.
“In their relationship, they ask them, ‘What you taking?’ She responds, Oh, I’m just taking my vitamins. Then, they’ll leave it alone. But if they see that bottle with that word on there [PrEP]. . .They google it. And then once they Google it and find out they think, ‘Oh, you’ve been messing around with somebody. Oh, man, you got [HIV]—we can’t talk no more.’ You know, it’s a big issue. . . So, they’re [women on PrEP] not going to go to leave it [PrEP] laying around. . .So they just keep quiet about it.”—PrEP-experienced Interview Participant 1
This quote highlights the importance of maintaining privacy around taking PrEP for Black women. Black women feared that if their PrEP usage was disclosed, assumptions would be made about their HIV status, and they could experience consequences, like the end of their relationship. In addition to stating that they are taking their vitamins, which was highlighted by at least two women, another strategy that was discussed was taking the label completely off the bottle, as detailed by this PrEP-experienced Black woman. This strategy prevents people from being able to look up the medication name, thereby reducing the chances of them finding out about PrEP.
“That’s why I don’t even put them [PrEP medication] in the medicine cabinet. I have nosy kids. They’d be all in my medicine cabinets, so, nope. I take the label off.”—PrEP-experienced Interview Participant 2
Though most PrEP-experienced Black women in our study discussed using mitigation strategies that concealed their PrEP usage, one Black woman stated that she confronts individuals who choose to judge her because of her PrEP usage. She does this by stating that she cares about her partner, she is doing what is best for her health, and that she will choose not to discuss private matters anymore.
“I just kind of say stuff like, ‘Well, your relationship’s not all perfect, unicorns and stuff too so you can’t put me down for sharing something with you’ . . .And I try to be nice about it, but I tell them, ‘I just, I care about him, and I’m sorry you don’t see it that way. But it is what it is. I’m leaving it at that, and I won’t talk to you about anything anymore.”—PrEP-Experienced Interview Participant 4
Social support’s role in PrEP initiation and adherence
PrEP-experienced Black women experienced differing levels of social support while taking PrEP. PrEP-experienced Black women reported receiving social support if they were in a serodifferent relationship or if someone in their network was also taking PrEP. Black women in serodifferent relationships received support from their partner to initiate and/or continue to take PrEP as a way of protecting themselves from acquiring HIV. For example, this PrEP-experienced woman discussed her partner disclosing his status and asking her to visit the doctors with him, which led her to initiate PrEP.
“. . .we met, and he started crying one day. And he’s like, ‘I have HIV and Hep-C.’ And he was like, ‘Will you come see this doctor with me?’ . . .They helped me get insurance-type stuff. And I sat down with the doctor. . . And then, of course, I research everything because everybody has Google. You know? then got on PrEP. . .”—PrEP-experienced Interview Participant 4
For this Black woman, attending a doctor’s appointment with her partner was a catalyst for her getting on PrEP. This quote also highlights the mutual adherence support to PrEP and ARTs that she and her partner shared. Another PrEP-experienced Black woman who is in a serodifferent relationship received support to take PrEP. She described a mutually supportive relationship where she would remind him to take his HIV medication, and he would remind her to take her PrEP.
PrEP-experienced Black women stated that group support settings would be best and suggested different uses for the group. Black women discussed the need for social support groups as a way to educate other Black women, who may or may not be taking PrEP, about PrEP and to share thoughts about PrEP. One PrEP-experienced woman thought support groups would be beneficial in letting women know that they are not alone in this PrEP journey.
“Like once a month. . .Everybody comes in and sit down and talk. Even though they may not have experienced it [PrEP]. They may just want to have questions and concerns because they may know someone. . .And they could pass the word on. . .And they may have a sibling or a relative that’s in that situation and is scared to come out and say something about it.”—PrEP-experienced Interview Participant 1
In addition to providing a safe space to discuss PrEP, another Black woman discussed how these support groups could include a wide range of sexual health topics.
“I think it should be a support group to other women that are interested in safer sex and stuff for themselves. . .I think that all that goes with the birth control, like, also taking care of themselves too. . .”—PrEP-experienced Interview Participant 6
These two quotes highlight Black women’s opinion of the importance of social support in getting Black women to initiate and adhere to their PrEP regimen. In summary, PrEP-engaged Black women experienced differing levels of emotional and instrumental social support from their social network when initiating and taking PrEP.
Discussion
This study aimed to explore how sociostructural factors affect PrEP interest and experiences among PrEP-naïve and PrEP-experienced Black women in Jackson, Mississippi. We found that Black women experienced and anticipated multiple forms of stigma that impacted their PrEP interest and experiences. Black women reported experiencing sexual stigmatization, gendered racism, and discrimination while attempting to obtain an HIV test at the doctor’s office, when picking up their PrEP medication, and when disclosing PrEP usage. Based on witnessing previous occurrences of HIV stigma, PrEP-experienced Black women were hesitant about disclosing their PrEP use and utilized multiple strategies to prevent PrEP disclosure, especially when in serodifferent relationships. Black women in serodifferent relationships feared disclosing their partner’s HIV status by disclosing their own PrEP use. Social support varied among those in serodifferent relationships. Social support also varied based on whether others in Black women’s networks were taking PrEP, with Black women feeling more supported if they knew others also engaged in PrEP. PrEP-experienced Black women suggested social support groups to improve knowledge about PrEP among Black women.
Gendered racism and medical paternalism impacted Black women’s experiences seeking HIV testing, which is a precursor to PrEP initiation. The consequences of gendered racism and medical paternalism on Black women’s health is well documented.35 –38 Provider biases that are rooted in gendered racism can lead to discriminatory practices, which can consequently negatively affect Black women’s health.35,36 Though experiences of gendered racism from a healthcare provider can be difficult to detect in the moment, the feelings of dismissal and denial of services leave a lasting impact on the lives in Black women. 36 Specifically, consequences of gendered racism and medical paternalism from being denied services or Black women’s concerns going unaddressed has included Black mothers having stillbirths, 38 limited informed consent and medical autonomy, 39 and poor mental health outcomes. 37 Gendered racism also has a negative impact on Black women’s sexual health decision-making by making them feel less empowered to make decisions for themselves and decreasing their interest in learning new safer sex information. 40 In our study, gendered racism was a barrier for PrEP-naïve Black women who had an interest in initiating PrEP. Though the Black women who requested HIV testing had access to resources that afforded them the opportunity to get tested, these resources alone did not buffer against mechanisms or oppressive experiences that denied them such testing. When providers not only denied HIV testing but also suggested that HIV testing was only for sexually promiscuous individuals, it contributes to HIV stigma within the community. Perpetuating HIV stigma, in addition to stereotypes of Black womanhood, in these medical interactions could lead to less Black women initiating PrEP, even when they believe that it would decrease their HIV risk.
Patient–provider interactions are important for HIV prevention, especially PrEP engagement, for Black women. 41 Patient–provider relationships and communication are essential to the ongoing satisfaction of providers 42 and the health of Black women.28,43 –45 Black women have described communication challenges with their providers, including instances where their doctors were judgmental, insensitive, patronizing, and condescending, all of which impacted their trust in their provider. 42 Black women also reported experiencing differential treatment from their providers, inadequate communication, and a limitation of health choices. 44 Though this study focused on the perinatal period, these findings are similar to the experiences reported in this study about limiting HIV testing choices. Interactions with healthcare providers could and do, in our study, influence Black women’s access to HIV testing.
In addition to gendered racism, medical paternalism, and patient–provider interactions, additional sociostructural barriers such as a lack of Medicaid expansion in Mississippi may also impact Black women’s decision to initiate and adhere to PrEP. At the time of this study, Mississippi was one of the few states where Medicaid has neither been expanded nor have implemented Medicaid waivers to allow people without insurance to obtain necessary HIV prevention services. 8 High rates of individuals living in poverty and uninsured in the South, coupled with a lack of Medicaid expansion and high medical care costs, creates barriers to PrEP initiation. 8 Expanding Medicaid would significantly reduce financial barriers to PrEP initiation for individuals living in the South and, specifically, Mississippi.
HIV stigma in the community was discussed among PrEP-experienced and PrEP-naïve Black women, which had an impact on PrEP-experienced women’s decision to disclose their own PrEP use. HIV stigma affects the health of Black women.1,9 Prior research has shown that while men’s HIV testing is influenced by individual-level stigma, women’s HIV testing is influenced by community-level stigma. 46 For women, more community-level stigma results in decreased HIV testing for women. 46 PrEP-experienced women in our study, who anticipated PrEP and HIV stigma as a result of the disclosure, utilized mitigation strategies to overcome PrEP stigma: (1) telling others that PrEP is vitamins, (2) hiding or removing the label from PrEP, and (3) confronting people in their network directly about the benefits of using PrEP. In addition to the individual strategies discussed, several other macro-level strategies that are aimed at addressing PrEP stigma could help to increase PrEP uptake and adherence. For example, PrEP guidelines could be expanded and reworded to focus less on stigmatizing language and PrEP assessments could be initiated by patient concerns about their sexual health. 18
The intersection of social support, sexual stereotypes, and sex positivity plays a crucial role in shaping PrEP initiation and adherence among Black women, highlighting both barriers and potential strategies for improving sexual health outcomes. Lack of social support was also a barrier to PrEP initiation and uptake for PrEP-naïve and adherence for PrEP-experienced women. Lack of social support negatively influences health outcomes,47 –49 as well as PrEP decision-making and adherence.1,50 For example, Black women who had network members with negative perceptions about PrEP decreased their interest in PrEP, whereas Black women with supportive network members increased their interest and ability to take PrEP. 50 The effects of sexual stereotypes of Black women were seen our results, as one Black woman described being questioned about her sexual behaviors as she disclosed her decision to initiate PrEP. Black women bear an unjustly heavy burden of sexual stereotypes, perpetuating misconceptions about their sexual health, defining what is socially acceptable for Black women, and contributing to significantly poorer sexual health outcomes. 51 Social support groups were discussed by Black women in our study as a strategy to increase social support for Black women. Promoting safe spaces and prioritizing sex positivity and pleasure are proven strategies that effectively encourage preventive sexual health behaviors and mitigate stigma. 51 Leveraging sex positivism for PrEP uptake among Black men who have sex with men has increased sexual freedom, agency and empowerment to use PrEP, positive associations with PrEP use, and opportunities to engage in better behavioral health practices.52,53 Applying sex positivism have the potential to also increase PrEP uptake and adherence for Black women as well, while also combating gendered racism that they experience. Integrating lessons learned from intervention strategies in Mississippi specifically for Black women, such as using Black women as peer educators, tailoring PrEP education to Black women, and providing PrEP education in public spaces where Black women frequent could also help in these endevors. 54 Considerations for utilizing social support groups should include making sure the group is culturally sensitive, provide accurate and complete information, build on existing social structures, and providing safe and confidential spaces.54,55 Part of providing accurate and complete information can include creating tailored marketing messages about PrEP with a sex positive lens that could help Black women to embrace their sexuality and to take charge of their sexual health. Addressing these interconnected factors through targeted interventions and fostering supportive environments could not only enhance PrEP uptake and adherence among Black women but also mitigate the pervasive effects of sexual stereotypes and promote more equitable sexual health outcomes.
Limitations
While this study is important, it is not without limitations. Our study participants were purposively recruited from a single sexual health clinic in Mississippi, which could have limited recruitment of potential participants who received healthcare elsewhere. Additionally, the recruitment flyer for PrEP-naïve included full details of the study, which could have limited potential participants who feared experiencing HIV or PrEP stigma as a result of being seen interacting with the flyer. Though there were 12 PrEP-experienced women at the clinic, only 8 of these women were Black. Since PrEP-experienced women were all recruited from a PrEP program, specifically, they may have different experiences that could have facilitated their PrEP use as compared to PrEP-naïve women. This also could serve as selection bias, as women taking PrEP who are not part of an actual program may experience additional barriers to sustained use of PrEP. However, this means we were able to interview all of the women who met our inclusion criteria. Additionally, PrEP-experienced Black women were interviewed by researchers who recruited from a PrEP program. Therefore, the data could be subject to social desirability bias, where participants are telling us what they think we want to hear about their PrEP experiences. For PrEP-naïve Black women, they could have also agreed with their peers, even when their opinions or thoughts of PrEP deviated from the group attitudes. However, we completed peer debriefing with staff and debriefing with individuals outside of the data collection team to ensure that the interpretations of findings made sense.
Conclusion
This study critically examined the impact of stigma and social support on PrEP initiation and adherence among both PrEP-naïve and PrEP-experienced Black women in Jackson, Mississippi. We found that several forms of stigma and differing levels of social support impacted Black women’s PrEP initiation and adherence. Addressing gendered racism and sexual stigmatization in healthcare settings, creating tailored marketing messages and education strategies for Black women, as well as increasing sex positivity through safe spaces for Black women all have the power to decrease stigma and increase social support for Black women. Subsequently, these changes could also help Black women initiate and adhere to PrEP, thereby decreasing HIV transmission in Jackson, Mississippi.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057241296905 – Supplemental material for PrEP initiation and adherence among Black cisgender women in Mississippi: The role of HIV and PrEP stigma and social support
Supplemental material, sj-pdf-1-whe-10.1177_17455057241296905 for PrEP initiation and adherence among Black cisgender women in Mississippi: The role of HIV and PrEP stigma and social support by Deja Knight, Mauda Monger, Karlye Phillips, Amina Antar, Stefan Baral, Jamila K. Stockman, Amy Nunn, Philip Chan, Kenneth Mayer, Leandro Mena, Trace Kershaw and Tiara C Willie in Women’s Health
Footnotes
Appendix
Sample FGD and interview questions.

| Sample FGD questions | Sample interview questions |
|---|---|
| What kind of support do you think would be good for women to get them on PrEP? | Some women have told us that they struggle with discrimination, or that they believe their loved ones might think they have HIV or are sleeping around if they take PrEP. Some mentioned that affected their interest in continuing to take PrEP. Did any of those things affect your decisions to continue PrEP? Tell me about that. |
| Why are you not taking PrEP? | Do you feel you had support by friends and loved ones to stay in PrEP care? Why or why not? Did that affect your ability to keep taking PrEP? |
| Discuss some of the concerns you think African American women have about using PrEP? | In terms of offering support or counseling services to help people stay on PrEP, do you think a one-to-one program or a group setting program would be most helpful? |
FGD: focus group discussion; PrEP: pre-exposure prophylaxis.
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.