
Abstract
Background:
Abortion-related complications are the third leading cause of maternal mortality in Uganda, accounting for approximately one-fourth of all maternal deaths. Most are preventable through adequate use of the full package of postabortion care (PAC) services.
Objective:
We aimed to assess the level of utilization of PAC services and the associated sociodemographic, obstetric, gynecological, and system-related factors at a high-volume tertiary health facility in Northern Uganda.
Design:
A cross-sectional survey was conducted among women receiving PAC at the Gulu Regional Referral Hospital from March 2023 to June 2023. Participants were recruited consecutively and exit interviews were conducted using structured questionnaires.
Methods:
Utilization of PAC was defined as the use of four or more of the following: counseling, emergency treatment, family planning services, linkage to other sexual and reproductive health services, and community health service provider cooperation. Modified Poisson regression analysis was used to determine the independent predictors of PAC utilization.
Results:
A total of 364 participants were enrolled in the study. Overall, 21.1% (n = 77) of the participants had used four or more PAC services. Having a supportive partner (adjusted prevalence ratio (aPR): 1.9, 95% confidence interval (CI): 1.19–2.88, p = 0.006), knowledge on PAC services (aPR: 1.7, 95% CI: 1.19–2.48, p = 0.004), low parity (aPR: 2.2, 95% CI: 1.16–4.35, p = 0.016), nulliparity (aPR: 2.4 95% CI: 1.19–4.73, p = 0.014), and provision of privacy(physical privacy during prescription, counseling, procedures) (aPR: 2.3 95% CI: 1.14–4.47, p = 0.02), were significantly associated with utilization of PAC.
Overall, only one in five participants utilized four or more PAC services. Use of four or more PAC services was significantly associated with women having a supportive partner, knowledge of PAC services, low parity, nulliparity, and provision of privacy while receiving PAC services.
Conclusion:
Approaches such as advocating male partner involvement, bridging the knowledge gap through health education, and promoting respectful care may improve the utilization of PAC services.
Introduction
Abortion-related morbidity and mortality are global public health concerns. 1 Approximately 21.9 million unsafe abortions occur globally, 97% of which occur in low-income countries. 2 Abortion complications are estimated to contribute to 13% of global maternal deaths. 2 In Uganda, 52% of pregnancies are unintended, and one-quarter of these end in induced abortion each year. 3 The consequences of abortions include physical complications (incomplete abortion, pelvic infection, hemorrhage, shock, and secondary infertility), emotional sequelae, and enormous costs to the healthcare system for treating abortion complications. 4 Abortion-related morbidity and mortality can be prevented through timely and adequate use of postabortion care (PAC) services. 5
PAC is a package of services offered to women after abortion. 6 This provides a comprehensive approach to preventing maternal morbidity and mortality from abortion and its complications. There are five important elements of PAC: treatment; family planning services; counseling; other reproductive and related health services (screening, diagnosis, and treatment of sexually transmitted infections; nutrition screening and education; hygiene education; screening, counseling, and treatment of reproductive-related cancers; and services addressing gender-based violence); and community service provider cooperation (Community linkage). 7 Each of these elements is important in ensuring that women receive holistic woman-centered care, and it is recommended that every woman who needs PAC receive the complete package. 8 According to studies from Uganda and Ethiopia, utilization of PAC has been shown to be positively influenced by having a supporting partner, having knowledge about PAC elements, a higher level of education, provision of privacy during services, a good health worker attitude, younger age, accessibility, and availability of services in the health facility.6,9,10 The Ugandan government has made a long-standing commitment to address abortion-related morbidity and mortality by providing quality health services for the management of complications from abortion. 11 Nevertheless, barriers such as lack of access to information and services, lack of proper referral linkages, and limited women’s access continue to fuel the problem of low utilization of PAC services. 6
There is a scarcity of evidence on the utilization and factors associated with the utilization of PAC in the country, specifically in Northern Uganda, where there is high maternal morbidity and mortality due to abortion-related complications. Therefore, this study aimed to assess the level of utilization of PAC and the associated factors among women receiving PAC services at a tertiary health facility in Northern Uganda.
Methods
Study design and setting
A cross-sectional study was conducted among women receiving PAC services from the gynecology unit of the Gulu Regional Referral Hospital, Gulu, Uganda, between March and June 2023. This study site was selected because it is a high-volume facility that provides PAC services to a large number of women. Therefore, it was easier to achieve the estimated sample size during the study period. The gynecology ward has two general wards where patients rest, a procedure room where evacuations are conducted, a counseling room where family planning services and counseling is provided, and a changing room for staff. The general ward also has a reception area where triage is done which also doubles as the nurses station.
The reporting of this study conforms to the STROBE statement. 12
Sample size estimation
The sample size was calculated using the Kish-Leslie formula (1965) for cross-sectional studies and was based on the study conducted by Zemene et al., 10 which found 31.4% utilization of PAC. The calculated sample size was 331 participants; however, our target sample size was 364, accounting for a 10% nonresponse rate.
Recruitment
A list of all women receiving PAC was obtained daily from the gynecology ward register for 4 months. Women who were due to be discharged that day were approached, and informed consent was obtained from those who met the inclusion criteria. The participants were selected using consecutive sampling.
Eligibility criteria
We included all women of reproductive age (15–49 years) who sought PAC services from the gynecology ward of Gulu Regional Referral Hospital during the study period and excluded women who were very ill or had altered mental status, which hindered them from providing valid information.
Variables
The dependent variable was the utilization of PAC, which was a binary variable. The independent variables were sociodemographic, obstetric, gynecological, and system-related factors. Sociodemographic factors included age, tribe, marital status, occupation, level of education, religion, partner support (any emotional, physical, and financial support), and previous use of PAC services. Obstetric and gynecological factors included knowledge of PAC services (any knowledge on components and availability of PAC), desire to get pregnant, parity, number of living children, and number of abortions. Participants were asked about various health system-related factors, including the time to evacuation, which was defined as the time from diagnosis to the initiation of uterine evacuation, the respect for privacy, which was defined as the level of physical privacy afforded to the participant during counseling, prescription, and the evacuation procedure, and their perceived attitudes of the health workers during the PAC.
Age, parity, number of living children, and number of abortions were collected as continuous variables and categorized during the analysis. Other independent variables were categorized as categorical variables.
In their study, Zemene et al. defined PAC users as women who used all components of PAC; 10 however, in this study, we operationally defined PAC utilization as receiving at least four or more of the five essential components of PAC which includes counseling, emergency treatment (mainly uterine evacuation and other medical interventions), family planning services, linkages to other sexual and reproductive health services, and community health service provider cooperation. In the context of this study, the researchers defined utilization as the use of at least four of the PAC components. This was necessary because the community health department at the study site, which was responsible for establishing formal community linkages, was not operational during the study period.
Data collection tools and techniques
Interviewers administered pretested structured questionnaires to collect data on sociodemographic, obstetric/gynecological, and system factors, and PAC services, including postabortion counseling, family planning, other reproductive health services, and community linkages. Trained midwives conducted the exit interviews upon hospital discharge.
Statistical analysis
The questionnaire data was entered into Microsoft Excel 2021, checked for completeness, cleaned, and coded. The coded data were imported into STATA version 15 (StataCorp LLC.). Numerical variables are presented as medians and interquartile ranges because the data were not normally distributed, and categorical variables are presented as frequencies and percentages. The association between numerical variables and utilization of PAC services was tested using the Mann-Whitney U test and with categorical independent factors using Pearson’s chi-square or Fisher’s exact test, depending on the number of cells on cross-tabulation. Factors in the bivariate analysis with p < 0.2 were taken for a modified Poisson regression analysis with robust standard error to determine predictors of the utilization of postabortion family care services among the participants. Factors with p < 0.2 were supportive partner, knowledge of PAC services, desire to get pregnant, parity, accessibility of PAC, respect of privacy, and health worker attitude and those that had p > 0.2 were, age, tribe, having a partner, occupation, religion, previous use of PAC, number of living children, and number of abortion. The decision to include factors with a significance level of p < 0.2 from bivariate analysis in our study was based on the necessity to account for potential predictors in a small sample size scenario. This approach enables a broader consideration of variables while acknowledging the limitations imposed by limited data. Factors meeting this criterion were included in our analysis, while those failing to meet it were excluded. This strategy aims to capture potentially important associations while maintaining statistical rigor within the constraints of our study’s sample size. The findings were then presented as adjusted prevalence rate ratios with corresponding 95% confidence intervals (CI) and p-values. p < 0.05 was considered statistically significant.
Ethical considerations
Ethical approval was obtained from the Gulu University Research and Ethics Committee (grant no. GUREC-2022-301). Administrative clearance was obtained from the Gulu Regional Referral Hospital. Participation in this study was voluntary. Written informed consent was obtained from all participants and interviews were conducted individually in a private room. Participants’ personal identification details were replaced with an identification number in the questionnaires. The completed questionnaires were stored confidentially with restricted access to the research team and relevant institutional stakeholders.
Results
Descriptive characteristics of women receiving PAC services at Gulu Regional Referral Hospital
In total, 364 participants were interviewed. More than half of the respondents (52.5%) were 25 years and above. Of the participants, 274 (75.3%) had previously received PAC and the majority (65.4%) had knowledge about PAC.
Overall, 230 (63.2%) pregnancies among the participants were intended, and most (72.5%, n = 264) participants experienced abortion for the first time.
Of the 364 participants, 261 (71.7%) felt that the health workers had an understanding attitude toward them, 256 (70.3%) found it easy to access PAC services, and 255 (70%) participants felt their privacy was respected as they received PAC services (Table 1).
Descriptive characteristics of women seeking postabortion care services from the gynecology unit of Gulu Regional Referral Hospital.

PAC: postabortion care; IQR: interquartile range.
Utilization of PAC among women who sought PAC services at Gulu Regional Referral Hospital
Overall, 21.1% (n = 77) of the participants had received at least four of the five basic components of PAC.
The majority of the participants (287, 78.9%) received three or fewer PAC services, including uterine evacuation. Almost all the participants (99.7%, 363) underwent uterine evacuation. Only 0.4% (2) of the 364 participants were linked to a community health worker (Table 2 and Figure 1).
Utilization of postabortion care services among women seeking PAC services from the gynecology unit of Gulu Regional Referral Hospital.


Utilization of PAC services among women seeking PAC from the gynecology unit of Gulu Regional Referral Hospital.
Factors associated with utilization of PAC services among women who sought PAC services at Gulu Regional Referral Hospital
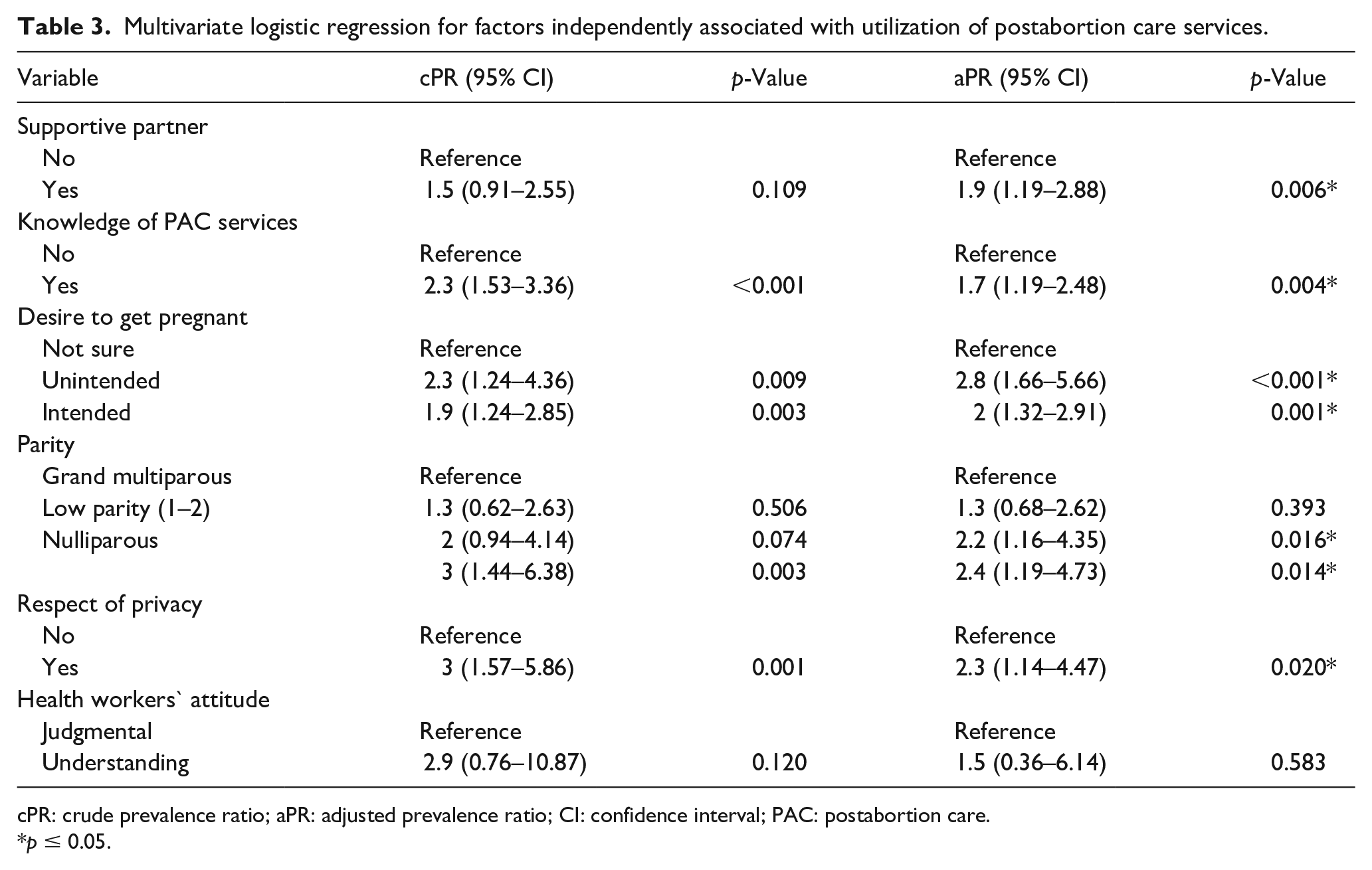
In multivariate analysis, the utilization of PAC services can be categorized into individual and health-services-related factors. Individual characteristics such as having a supportive partner (adjusted prevalence ratio (aPR): 1.9, 95% CI: 1.19–2.88), possessing knowledge on PAC services (aPR: 1.7, 95% CI: 1.19–2.48), experiencing unintended pregnancy (aPR: 2.8, 95% CI: 1.66–5.66), intended pregnancy (aPR: 2, 95% CI: 1.32–2.91), Having low parity (aPR: 2.2, 95% CI: 1.16–4.35), and being nulliparous (aPR: 2.4, 95% CI: 1.19–4.73)] were found to significantly increase the likelihood of utilizing PAC services. On the other hand, Health services-related factors such as provision of privacy during care also played a crucial role in enhancing the utilization of these services (aPR: 2.3, 95% CI:1.14–4.47) (Table 3).
Multivariate logistic regression for factors independently associated with utilization of postabortion care services.
cPR: crude prevalence ratio; aPR: adjusted prevalence ratio; CI: confidence interval; PAC: postabortion care.
p ≤ 0.05.
Discussion
This study assessed the utilization of PAC services and associated factors among women receiving PAC services at the Gulu Regional Referral Hospital, Gulu, Northern Uganda. Overall, the PAC utilization rate was 21.1%. PAC use was significantly associated with having a supportive partner, knowledge on PAC services, and the provision of privacy.
In our study, the level of PAC service utilization was 21.1%. This is comparable with a similar study in southwestern Ethiopia, which found that PAC utilization was 25.1%. 13 However, these rates are lower than those reported by Addis Ababa, Ethiopia (31.4%) and Guangzhou, China (42%).10,14 This difference may be due to the small sample size of their study in Ethiopia (n = 153). The variation in the Chinese study may also be attributed to differences in the accessibility of PAC services and legal frameworks governing abortions. In China, abortions are legal throughout pregnancy, unlike in Uganda, where abortions are restricted to cases of abuse, fetal abnormalities, and pregnancy that pose a risk to the mother. Under such strict laws, fewer women may seek PAC services and health workers may be reserved in providing services. Comparing Uganda to Ethiopia and China, PAC is a relatively new phenomenon, and much must be done to create awareness and improve access to these services at all levels of health facilities in Uganda.
In this study, women with supportive partners were more likely to utilize PAC services than those with non-supportive partners. This is consistent with studies conducted in Nigeria, Ethiopia, and China.14 –16 In contrast, a study in Ethiopia showed that women with supportive partners were less likely to utilize PAC services. 17 This difference is likely because partner support is associated with less stigma and, consequently, more vigilance in utilizing PAC services; supportive partners tend to encourage and influence women to take up more PAC services. However, some partners may have a negative attitude toward PAC services, so these women are less likely to use the available services because of fear of the consequences.
In addition, our study found that women who previously had knowledge of PAC were more likely to utilize PAC services than those who had no knowledge. These findings are consistent with those of similar studies in Ethiopia.10,18 Women who have knowledge of PAC services may have an idea about the services they are expected to receive and understand the importance of using PAC; therefore, they are likely to utilize more PAC services than those who have no knowledge.
Furthermore, this study found that low-parous and nulliparous women were more likely to utilize PAC services than grand multiparous women. This could be because women with lower parity are younger and wish to delay unintended pregnancies; therefore, they are likely to utilize more PAC services, while grand multiparous women could be older and have more experience with pregnancy losses and may only be interested in utilizing specific services.
This study found that women whose privacy was respected were more likely to use PAC services than those whose privacy was not respected. A cross-sectional study conducted in Tanzania revealed similar findings. 6 Women for whom privacy is provided during uterine evacuation are likely to have positive experiences and use more PAC services.
Finally, this study revealed that women who had unintended and intended pregnancies were more likely to use PAC services than those who were unsure about their pregnancies.
We recommend that there is a need for health authorities and health care providers to put forward strategies such as creating awareness on the availability of PAC, encouraging partner involvement during PAC, and ensuring privacy during all steps of PAC service provision to improve utilization of PAC services. A more robust multicenter study involving stakeholders in the community, health care providers, health authorities, and users of PAC services is recommended to give more representative data.
Limitations
This study’s findings should be considered in light of several limitations. First, the facility-based nature of this study means the findings may not be representative of women who seek PAC in Northern Uganda. Compared to wealthier and married women, less well-off and unmarried women are respectively less likely to have access to a wider range of healthcare providers that are typically available in hospital settings.19,20 Second, the cross-sectional of this study, would not be able to establish a causal relationship between PAC utilization and associated factors. There may have been response biases to some questions due to the sensitive nature of the topic; however, we mitigated this by ensuring that participants were interviewed in a private room and assured confidentiality. Third, the complex health system factors were not included in this study. Despite all these limitations, this study provides useful evidence that could be harnessed to improve PAC in similar settings.
Conclusions
According to this study, the utilization of PAC services remains low. Most participants received fewer than four of the five key elements of the PAC, as recommended by the World Health Organization. PAC utilization was significantly associated with having a supportive partner, knowledge of PAC services, low parity, nulliparity, and provision of privacy while receiving care at the facility. Based on these findings, there is a need to advocate male involvement in PAC, strengthen public awareness, and promote respectful PAC.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241295896 – Supplemental material for Exploring the utilization of postabortion care services and related factors among women at a tertiary health facility in Gulu, Northern Uganda
Supplemental material, sj-docx-1-whe-10.1177_17455057241295896 for Exploring the utilization of postabortion care services and related factors among women at a tertiary health facility in Gulu, Northern Uganda by Ayikoru Jackline, Jimmyy Opee, Felix Bongomin, Harriet Akello, Sandra Fiona Atim and Pebalo Francis Pebolo in Women’s Health
Footnotes
Acknowledgements
We appreciate the fraternity of the Gulu Regional Referral Hospital and Gulu University for their support during the study. We thank our data collectors and data analysis team. Pre-Publication Support Service (PREPSS) supported the development of this manuscript by providing author training, pre-publication peer review, and copy editing.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.