
Abstract
Background:
Rates of perinatal depression and anxiety increased during the COVID-19 pandemic. It remains unclear how the COVID-19 pandemic influenced risk perception and help-seeking behaviours among pregnant and postpartum individuals.
Objectives:
To explore pregnant and postpartum individuals’ decision-making process about when and how to seek support for feelings of depression and/or anxiety during the COVID-19 pandemic.
Design:
A qualitative descriptive design was used.
Methods:
The current study is a secondary analysis of qualitative data collected for a larger mixed-methods project that recruited participants who gave birth from 1 May 2020, to 1 December 2021, in Ontario and British Columbia, Canada, using maximum variation and purposive sampling. Seventy-three semi-structured interviews were conducted over Zoom or telephone. This analysis focuses on 56 individuals who discussed their self-identified feelings of prenatal or postpartum depression and/or anxiety. Conventional (inductive) content analysis was employed with iterative stages of open coding, focused coding and cross-checking themes.
Results:
Most participants recognized their need to seek help for their feelings of depression and/or anxiety through discussions with a mental health professional or someone within their social circle. Nearly all participants accessed informal social support for these feelings, which sometimes entailed social contact in contravention of local COVID-19 public health policies. Many also attempted to access formal mental healthcare, encountering barriers both related and unrelated to the pandemic. Participants described the pandemic as having the dual effect of causing or exacerbating their feelings of depression and/or anxiety while also constraining their ability to access timely professional care.
Conclusion:
Participants struggled to address their feelings of perinatal depression and anxiety during the COVID-19 pandemic, with many describing a lack of readily available resources and limited access to professional mental healthcare. This study highlights the need for improved provision of instrumental mental health support for pregnant and postpartum populations.
Plain language summary
It is not unusual for pregnant and postpartum individuals to experience feelings of depression and/or anxiety. Studies have shown that this became more common during the COVID-19 pandemic. Depression and anxiety can be challenging to recognize and treat in pregnant and postpartum individuals but may lead to long-term negative effects if not addressed. The COVID-19 pandemic brought on public health measures, including social distancing, which created barriers to accessing mental health professionals or social interactions. In this study, we wanted to understand when and how pregnant and postpartum people chose to seek support for their feelings of depression and/or anxiety during the COVID-19 pandemic. We interviewed people who gave birth during the pandemic in either Ontario or British Columbia, Canada and asked them about whether they experienced feelings of perinatal anxiety or depression, and how they chose to seek help for those feelings.
Most participants acknowledged their feelings of depression and/or anxiety through discussions with a mental health professional or someone within their social circle, even though many experienced barriers to accessing these supports. Nearly all participants interacted with friends or family outside of their household to cope with their feelings, which sometimes meant acting against local COVID-19 public health policies. Although some participants talked about facilitators for accessing mental health professionals, many who tried also encountered challenges, and a few were unsuccessful. Participants in this study shared that the pandemic sometimes caused or worsened feelings of depression and/or anxiety while also making it harder to access the support they felt was necessary to cope with their feelings. These findings show that there is a need for more frequent conversations about mental health during healthcare appointments and more readily accessible mental health resources for pregnant and postpartum people.
Introduction
Rates of self-reported depression and anxiety were elevated during the COVID-19 pandemic among pregnant and postpartum individuals.1,2 The COVID-19 pandemic is an example of an unforeseen, persistent and severe stressor 3 that disproportionately impacted the mental health of pregnant people compared to their non-pregnant counterparts. 4 The disproportionate burden experienced by pregnant and postpartum individuals may stem from an increased vulnerability to severe illness from COVID-19 infection, inequities accentuated by the pandemic and novel stressors brought upon by public health measures, including disruptions to the provision of perinatal healthcare, transition to virtual care and social isolation.5 –8 Structural and socioeconomic inequities were intensified by the pandemic as marginalized groups (i.e. women, low-income, gender-diverse, racialized and Indigenous people) were more susceptible to poor mental health, COVID-19 infection, food and housing insecurity and precarious employment.9,10 Indirect consequences of the pandemic, including income loss and resulting financial stress, increased rates of sex-based violence and increased caregiving responsibilities, were also felt more acutely by women and may have contributed to the increase in mental health concerns. 5
Perinatal depression and anxiety are not unusual; pre-pandemic, the prevalence of perinatal depression was 15%, whereas anxiety affected approximately 29% of perinatal individuals.2,11 –14 During the first wave of the pandemic in Canada, rates of perinatal depression and anxiety rose to 40% and 72%, respectively. 2 While the rates of depression and anxiety were higher during the pandemic, accessing necessary support to mitigate stressors was challenging due to the impact of public health infection prevention and control policies, which restricted access to essential support services, including vital mental health resources.2,3,5,15,16
In Canada, where this study was conducted, there is limited publicly resourced mental health support, and mental health specialists reported a particular strain on services and struggled to meet needs during the pandemic.15,16 Feelings of depression and anxiety may be particularly difficult to identify and address in pregnant and postpartum people, as approximately 70% of those who screen positive for perinatal mental health disorders choose not to seek support, and less than 15% receive formal mental healthcare. 16 Information about how perinatal individuals addressed their feelings of depression and/or anxiety during the COVID-19 pandemic is still emerging, with remaining questions about how people made decisions about accessing mental health support during the perinatal period and their experiences of trying to access support. To help address this knowledge gap, we sought to understand how people who experienced feelings of perinatal depression and/or anxiety made decisions about seeking mental health support, and their experiences throughout the process.
Methods
Study design
This study was part of a larger parallel convergent mixed-methods project about how people who gave birth during the first 2 years of the COVID-19 pandemic made pregnancy-related health decisions. 17 The project was conducted in Ontario (ON) and British Columbia (BC), two large, populous, and demographically diverse provinces in Canada. 18 Semi-structured interviews were conducted with 73 people who gave birth from 1 May 2020 to 1 December 2021. This study focuses on responses from the 56 participants who reported feelings of depression and/or anxiety while pregnant or in the year after birth. Ethics approval was obtained from the Hamilton Integrated Research Ethics Board (#14632) and the University of British Columbia Behavioural Research Ethics Board (H22-01905). Written informed consent was secured from all participants in advance of the interview, with additional verbal consent affirmed immediately before data collection.
Methodology
We used a qualitative descriptive approach to stay close to the participants’ explicit meanings and words with minimal abstraction or interpretive inference, allowing us to portray their experiences in their own words.19,20 Five people with lived experience of pandemic pregnancies (MP, NS, CM, SK, JL) participated as members of the primary study research team as either co-investigators (MP, SK, JL) or paid research assistants (NS, CM). We reported our study following the Consolidated Criteria for Reporting Qualitative (COREQ) Research Guidelines. 21
Recruitment
The eligibility and exclusion criteria, sampling and recruitment strategies for the larger study have been previously reported. 17 Briefly, people over the age of 18 who gave birth to a live baby between 1 May 2020 and 1 December 2021, in ON or BC and were able to complete an interview in English were eligible. Excluded participants include those who gave birth outside ON or BC, had a stillbirth or were unable to participate in an interview in English. ON and BC were chosen as the two provinces of interest for this study as they both had a large number of live births and high rates of COVID-19 infection during the pandemic.22,23 Potential participants were recruited via advertisements placed on social media and in public places frequented by parents of young children (e.g. libraries, pharmacies, childcare centres). The advertisements directed potential participants to an online consent-to-contact form that collected basic demographic information, which was used to determine eligibility and to operationalize purposive and maximum variation sampling as the study progressed. This analysis was a secondary focus of the larger study. While the data on mental health has not been analysed in any other publication, identifying potential participants who experienced feelings of depression and/or anxiety was not a recruitment goal for the larger project.
Data collection
We developed a semi-structured interview guide (Supplemental Material) that focused on understanding perceptions of COVID-19 risk as they related to health decisions in three areas of interest: mental health, vaccination and prenatal care. Our published protocol 17 provides more information on interview guide development, piloting and content. Further refinement to the guide occurred to respond to insights from preliminary data analysis, which occurred iteratively with data collection.
Interviews were conducted by multiple female interviewers of reproductive age with training in qualitative research and varying levels of educational attainment, including a BSc, master’s degree, MD and PhD (KS, MS, NS, ST, AC, CK and CM). Participants completed a single one-on-one semi-structured interview over Zoom or telephone from July 2022 to August 2023. The participants had no previous relationship with the interviewer. However, they were aware that the interviewer was a female employed as health science research staff investigating how pregnant and postpartum people’s perceptions of COVID-19 risk and pandemic circumstances influenced their healthcare decision-making related to pregnancy. Interviews lasted approximately 19–60 min (average: 44:48 min). Audio recordings of interviews were transcribed verbatim and de-identified for data analysis. To maximize the diversity of perspectives collected, interviews continued past thematic saturation when they no longer provided new information about areas of interest. 24 Additional data were collected to affirm that the findings continued to hold in additional participants who exhibited diversity in age, family composition and race.
Data analysis
We employed a conventional (inductive) approach to content analysis, adapting the staged coding methods of qualitative description to iterate data collection and analysis.19,20 One researcher (KS) open-coded all transcripts to identify and organize recurring themes in the data relevant to experiencing and seeking support for feelings of depression and/or anxiety. Initial insights were discussed with the larger research team, who offered suggestions for a refined coding framework. KS conducted two additional rounds of focused coding. Then, two researchers (CK and AC) co-coded the transcripts and cross-checked the themes to prompt critical dialogue and ensure consistent application of the codes. Constant comparative analysis was conducted across participant groups, 25 such as those who discussed their first pregnancy or those who intended to become pregnant during the COVID-19 pandemic. Triangulation was achieved across analysts and across participants. 26 Written memos were recorded after conducting each interview and reviewed throughout the analytic process to foster reflexivity and assist in recalling initial interpretations of participants’ experiences. Regular meetings were held with the broader research team to share preliminary findings and receive feedback. NVivo 14 (QSR International, Melbourne, Australia) was used to manage data. Transcripts or findings from the final analysis were not returned to participants.
Results
In total, of the 65 participants in the original study 17 who discussed their mental health, 56 participants reported feelings of depression, anxiety or both during pregnancy or within 1 year postpartum (Figure 1). These 56 participants were mainly White (70%), university-educated (72%) and primiparous (66%) (Table 1). The most common feelings reported were postpartum anxiety (n = 14) and a combination of perinatal depression and anxiety (n = 14). Overall, 44 participants experienced feelings of anxiety, and 31 participants experienced feelings of depression (Figure 1). Nineteen participants (34%) reported a diagnosis of depression and/or anxiety prior to becoming pregnant.
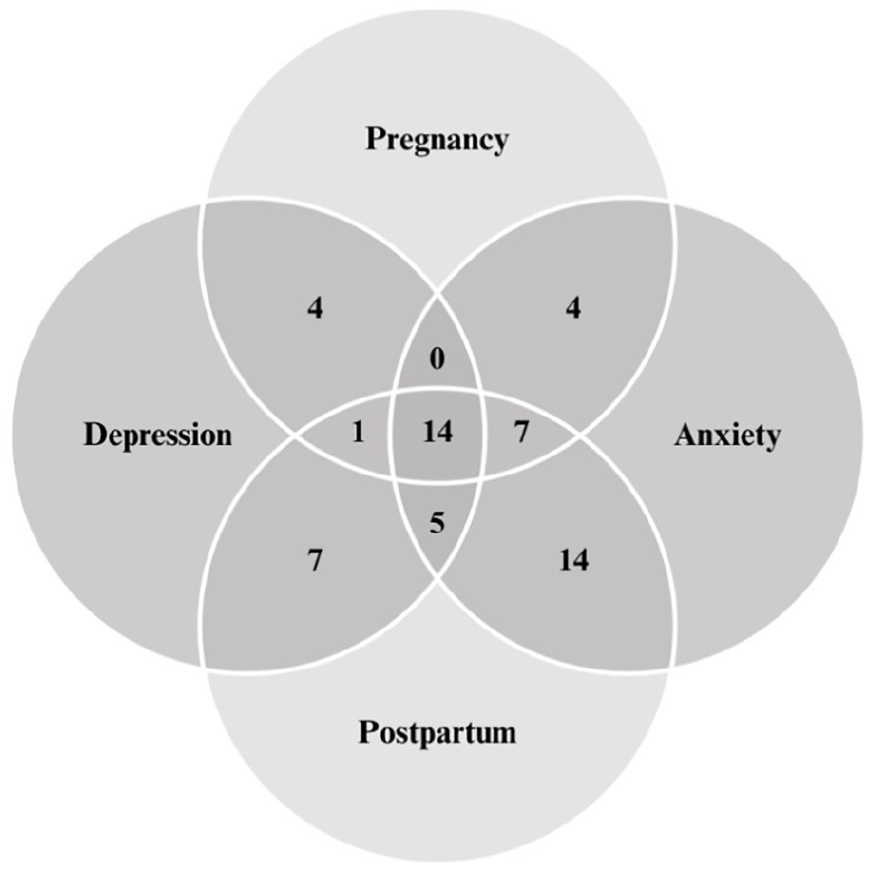
Feelings of depression and/or anxiety (n = 56).
Demographics table of participants.

Participants who conceived before the beginning of the COVID-19 pandemic, or who conceived unintentionally during the pandemic are described as having ‘unintentional pandemic pregnancy’. Those who conceived intentionally, within the COVID-19 pandemic are described as having ‘intentional pandemic pregnancy’.
Four overarching themes were identified in participant interviews and are described here temporally in relation to the process of seeking mental health support. Participants’ help-seeking processes typically began with identification and attribution of their feelings of depression and/or anxiety, followed by decision-making and experiences around accessing support for these feelings.
Identification of feelings of depression or anxiety
Identification is the process through which participants recognized that they needed to seek support to address their feelings of depression and/or anxiety. Most participants who experienced feelings of depression and/or anxiety came to identify their need for support from two main catalysts: receiving external feedback from family, friends or healthcare providers, and/or experiencing an adverse event.
External feedback
More commonly, participants were told to seek help by someone who showed concern for them, for example:
‘One of my best friends [. . .] was concerned because of the way that I was withdrawing and the fact that some of the things that I was expressing that I was feeling were not normal. [. . .] She kind of stepped up and said, “No, you have to think about this, it’s not just a normal sadness; this is like a grief that you need to address”’. (ON19, primiparous, 2021 birth)
Sometimes, healthcare providers played a pivotal role in helping participants identify feelings of depression and/or anxiety and encouraging participants to seek help.
‘[. . .] [A]fter talking to my GP [General Practitioner] and showing signs he said, “No, what you’re going through, you need medical help”. So, he did share resources, and I voluntarily reached out to [a support organization] because I wanted to proactively deal with this my way’. (BC204, primiparous, 2020 birth)
Although many participants reported wanting more healthcare provider-initiated conversations about mental health or formal mental health screening, few recalled identifying their feelings through these methods. Instead, participants typically described spontaneously reporting behaviour or feelings to their healthcare provider, who then helped them name and recognize these feelings as depression and/or anxiety.
Adverse event
Adverse events triggered the recognition that support was needed for some participants. These adverse events typically involved intense feelings such as anger or intrusive thoughts about harming their baby. This prompted participants to acknowledge that they needed help managing their feelings.
‘I went to my doctor – it was month three of being postpartum – and I said to her, “this is not working for me. I want to throw my baby [. . .] I hate it. I don’t want to be around it”. I was at a really bad place’. (P09, primiparous, 2020 birth)
Attribution
Many participants attributed their feelings of depression and/or anxiety to pandemic-related changes that strongly influenced their experience of pregnancy, birth and parenting. Those who gave birth in 2020 were more likely to attribute their feelings to the uncertainty of the pandemic and fears of COVID-19 infection, while those who gave birth in 2021 tended to attribute their feelings to isolation. No differences in attribution were identified between those who intended to become pregnant during the pandemic compared to those who did not plan to be pregnant during a pandemic.
Participants described four categories of pandemic-related factors that contributed to their experiences: COVID-19 infection risk and isolation, social tension due to personal beliefs around COVID-19 prevention efforts, missed baby celebrations and milestones due to physical distancing and pandemic healthcare policies that impacted birthing experiences (Table 2). Individuals who reported feelings of anxiety and/or depression typically attributed these experiences to one or more of these categories. Multi-parous participants provided particularly clear accounts of pandemic-related contributors to feelings of anxiety and depression, typically comparing with previous pre-pandemic pregnancies:
‘My [pandemic pregnancy], I had postpartum depression – I’ve never had it before [with my 3 previous pregnancies], and I believe a lot of it was the isolation’. (ON35, multiparous, 2020 birth)
Attribution factors for feelings of depression and anxiety.

Parity
Primiparous participants reported feeling particularly isolated when other parents provided support or advice that did not apply to their pandemic circumstances.
‘So, when other moms talked to me about the challenges and everything through that, I said I would divide my life into two phases: pre-COVID and during and post-COVID and all that phase. Because they said. . . things were hard for them. I would say it was 10 times harder [during the pandemic]’. (BC204, primiparous, 2020 birth)
Additionally, several multiparous participants expressed sympathy for primiparous parents during the pandemic because they recognized how its associated circumstances might magnify the difficulties of pregnancy.
‘I’m glad that this is our third and not our first because I think it would be really isolating and scary and sad to be doing this [becoming a parent] your first time during this [the pandemic]’. (BC205, multiparous, 2020 birth)
Experience of help-seeking
After identifying and attributing their feelings of anxiety and depression, all participants who reported feelings of depression and/or anxiety made decisions about whether and how to seek help for these feelings. Attribution was often linked to the type of help sought. While most participants sought mental health support from their social circles, some also sought formal support from different types of healthcare providers (see Figure 2). Similar help-seeking patterns between ON and BC participant groups were identified.

Types of formal support accessed (n = 35).
Social support
Almost all participants sought support from their social connections, engaging either in-person or virtual discussions with friends, family or online parenting groups. Most participants preferred in-person support as they found it helpful ‘to just be present and have a conversation’ (ON08, multiparous, 2021 birth), which could alleviate feelings of isolation for those who attributed isolation as an important contributing factor. Discussing challenges and concerns with these friends provided valuable encouragement and reassurance, ultimately reducing feelings of loneliness.
‘they [friends with young children] were able to really help uplift me and not make me feel like I was alone in any of it. So that was really helpful’. (ON09, primiparous, 2020 birth)
Influence of public health policies
Nevertheless, some participants reported that accessing social support meant sometimes contradicting public health policies that encouraged physical distancing from non-household members. In some cases, the need for support prompted individuals to prioritize their mental well-being over strict adherence to provincial or municipal guidelines: ‘I had no support aside from my mother-in-law down the street, and at that point, it was like, I’m going there. Like I need the help. I cannot do this alone’ (ON37, primiparous, 2020 birth).
In contrast, some participants who experienced feelings of depression and/or anxiety became more socially withdrawn or isolated in an attempt to closely follow public health measures. For these individuals, fear of COVID-19 infection became a prominent barrier to accessing social support.
‘No family, no friends, just me and my husband. [. . .] There was no village of support, and even [. . .] the few people that I could count in my village, we couldn’t because we had to be super careful’. (BC204, primiparous, 2020 birth)
Loss of community
Participants reported that COVID-19 prevention measures affected their ability to seek face-to-face or hands-on social support, particularly for those with families living far away or those who lived in an area with high transmission rates.
‘Just like a lack of support because I felt like I couldn’t [ask for in-person support] because I would be putting my family at risk. So it was really just, it just felt like such a lonely, sad time, when I felt like should’ve been happy. I wished it would’ve been different’. (ON22, multiparous, 2021 birth)
Many participants also spoke about how closures of community social or recreational resources for new parents due to COVID-19 prevention measures meant missing out on ‘shared experience[s]. . . [as] it’s almost like therapy [when] sitting in a group of other moms’. (ON43, primiparous, 2020 birth) Regardless of whether participants chose to seek social support during the pandemic, all individuals discussed their desire to connect more than had been possible with family, friends or other new parents during this isolating time.
Formal mental health support
Of those who experienced feelings of depression or anxiety, 35 individuals proactively sought formal mental health support, which we defined as support provided by health or social care professionals. The forms of formal support reported by these participants were therapy, medication or both (see Figure 2 for more details).
Barriers
Of those who sought formal support, two individuals were unsuccessful in accessing their first choice of care provider due to barriers related to or exacerbated by the pandemic, including extensive waitlists, time-limited resources, lack of childcare, finances, previous negative experiences and delivery of services (see Table 3). One of these participants felt deterred from accessing counselling as an avenue of support as they felt it was too late to benefit by the time it was offered and instead pivoted to medication as an alternative while on the waitlist. Even when participants could access their first choice, some reported that it took longer than a year to receive an appointment. As a result, a few participants only received postpartum mental health support because they anticipated these feelings before they arose and proactively sought these services during pregnancy.
Experiences with barriers and facilitators to accessing support.

One participant felt that they were fortunate to be prioritized for mental healthcare after experiencing a traumatic injury and surgery postpartum, as they were able to receive support immediately despite previously being on the waitlist for years. Many participants spoke about the decreased accessibility of mental healthcare due to pandemic closures and reported wanting more support and resources from their healthcare providers.
Facilitators
While many participants acknowledged the barriers that impacted their experiences accessing formal mental health support, some outlined potential facilitators, including strong relationships with support providers, history of successfully accessing care for depression and/or anxiety, and flexible or convenient modes of delivery for mental health services (Table 3).
Outcome of help-seeking
Thirty-three individuals described their overall experiences with formal mental health support as positive. Some participants described the process of seeking help as ‘life-changing’ (ON09, primiparous, 2020 birth), ‘a turning point’ (ON11, primiparous, 2020 birth) and wished they ‘wouldn’t have waited so long’ (ON13, multiparous, 2021 birth) to start.
‘I ended up going on depression medication, and it changed that time for me. It made me so much happier. I was able to be a good mom. I was able to get up every day and focus on my son and my health and caring for myself during that time’. (ON09, primiparous, 2020 birth)
Most participants were still accessing formal mental health support at the time of the interview. Four participants stopped seeking formal support because they felt their feelings of depression and/or anxiety had resolved over time, and three participants chose to discontinue treatments for other reasons (e.g. side effects of medication, unhelpful treatment).
Discussion
In this study, we report the diverse experiences of 56 individuals who described how the COVID-19 pandemic modified whether and how they sought support for their feelings of depression and/or anxiety during the perinatal period. These individuals cited COVID-19 infection risk, missed baby celebrations or milestones, social tension due to personal beliefs around COVID-19 prevention efforts and changes to policies that impacted birthing experiences as challenges and sources of stress that affected their mental health. These indirect and direct impacts of the COVID-19 pandemic changed their experience of these feelings of depression and/or anxiety; fear of infection contributed to participants’ feelings and simultaneously increased their sense of isolation. Consequently, pandemic circumstances directly impacted how participants identified their feelings and the amount of informal and formal support sought for these feelings. Consistent with a systematic review of studies published before the COVID-19 pandemic, informal sources of help were more frequently accessed than formal support by those experiencing perinatal mental health challenges. 27
Although 33 out of 35 participants who sought formal mental health support reported positive experiences, many of them also had difficulties accessing these services. Extensive waitlists, economic restraints, continuity of care limitations, community program closures and inadequate mental health services were significant barriers to help-seeking cited by participants. However, several participants in this study and others also relayed facilitators to accessing care, including the availability of virtual appointments and flexibility from care providers who made extra efforts to arrange timely mental healthcare.28,29 The findings of previous research echo overarching sentiments shared by participants in the current study, with most emphasizing the amplified psychosocial burden on pregnant and postpartum individuals during the pandemic1,30 –40 due to the downstream effects of public health policies that decreased access to timely and adequate mental health services or community social resources.2,5,15,16,27,28 Pandemic circumstances further compounded existing inequities and barriers to culturally safe and trauma-informed mental health support, such as stigma, healthcare provider training, attitudes and screening practices, socioeconomic limitations and sparse publicly funded mental health resources. 29 These barriers to accessing perinatal mental health support existed before the pandemic,41 –43 but reports from many regions emphasize the magnification experienced by many as a result of COVID-19.28,44,45
This is the first qualitative study, to our knowledge, to examine whether and how pregnant and postpartum Canadians executed help-seeking for feelings of depression and/or anxiety during the COVID-19 pandemic. Our findings highlight important implications for clinicians and policymakers related to the provision and delivery of perinatal mental health support. Ontario and BC have established different protocols for perinatal mental health screening using standardized health records (ON, BC) and a formal perinatal mental health program (BC).46 –48 In Ontario, universal perinatal mental health screening is not mandated, and individual health units develop independent protocols, most typically involving mental health screening during pregnancy and again at 6–12 weeks postpartum with validated screening tools. 47 British Columbia has established a strategy that strongly encourages mental health screening for all birthing individuals between weeks 28–32 of pregnancy and 6–8 weeks postpartum with validated tools.47,49 Despite the robust screening processes in ON and BC, few participants in this study recalled their healthcare providers initiating inquiries about their mental health or conducting mental health screening at the time they were experiencing feelings of depression and/or anxiety, suggesting potential low implementation during the early COVID-19 pandemic. One potential explanation for these discrepancies was disruptions to in-person prenatal and postpartum care during the pandemic, which may have decreased opportunities for providers to execute mental health screening at a time when participants were actively experiencing feelings of depression and/or anxiety.5,50 Another is participant recall; perhaps the screening questions were asked in earlier perinatal care appointments when the questions were not yet relevant to their feelings, decreasing the likelihood they would be remembered during the time of the interview.
Overall, participants in this study reported wanting more healthcare provider-initiated conversations and screening for mental health; this finding is echoed in other literature investigating public and perinatal individuals’ preferences for mental health screening.51 –53 Universal perinatal mental health screening is controversial, with wide endorsement but also longstanding contestations of efficacy.46,51 The Canadian Task Force on Preventative Health Care (CTFPHC) recommends against universal perinatal mental health screening, suggesting providers conduct targeted screening only for individuals with evident symptoms. 49 BC has since published a provincial position statement in support of universal screening (opposing the CTFPHCs recommendation), further affirming participant narratives in this study about the value of regulatory screening protocols and implementation into practice. 49 Existing research has endorsed the efficacy of validated perinatal mental health screening tools in identifying and improving health outcomes related to depression and/or anxiety.54,55
Implications
Healthcare provider-initiated screening and conversations about mental health can play a key role in the early identification of feelings of depression and/or anxiety while reducing the perceived stigma associated with addressing mental health concerns.12,56,57 The lived experiences of these study participants call attention to the shortcomings of perinatal mental healthcare infrastructure, the need for more readily accessible virtual and in-person resources, and the need to implement more frequent mental health screening throughout pregnancy and postpartum care appointments. While guidelines for perinatal mental health screening currently exist, they could be strengthened to ensure accessible and culturally safe screening occurs at multiple points in the care trajectory.16,44 In line with ongoing conversations about the value of universal screening, current guidelines could advocate for enhanced training for healthcare providers to appropriately target, conduct and follow up effectively on screening for perinatal depression and anxiety. This will facilitate the participation of healthcare providers in working with patients to identify the need for psychosocial support. 16 Alternative delivery options for perinatal mental healthcare and screening, such as virtual, home visitation or community-based interventions, may better meet the needs of this population and ensure support remains accessible during public health emergencies.44,58,59 Our findings extend beyond pandemic circumstances and offer valuable insight into everyday experiences of mental health during pregnancy, including the importance of social and instrumental support for new parents.
Strengths and limitations
With a qualitative descriptive approach, we capture pregnant and postpartum individuals’ lived experiences navigating the help-seeking process and report themes grounded in their subjective perspectives and interpretations with rich detail. A possible limitation of this study is its retrospective nature and reliance on self-reported data. Recall accuracy and social desirability bias of participants could reduce the accuracy of the data. Nevertheless, the proportion of participants who self-identified as experiencing feelings of depression and/or anxiety is reflective of existing literature that reports high rates of these mental health conditions in perinatal populations, especially during the COVID-19 pandemic.1 –3,16 The majority of participants in this study were White (70%) and university-educated (72%). While participant demographics in this study reflect the wider demographics of people of reproductive age in Canada (70% identify as White and 76% have a college or university education),18,60 it may be important for future work to focus specifically on the experiences of culturally and economically marginalized pregnant and postpartum people to understand potentially distinct experiences, equity issues and policy-relevant needs. 61 Lastly, while we intended to collect self-reported genders of participants, an administrative error resulted in missing gender data for approximately one-third of the study sample.
Conclusion
Pregnant and postpartum individuals who gave birth during the COVID-19 pandemic experienced feelings of depression and/or anxiety due to a combination of factors, including isolation, fear of infection and uncertainty. Those who chose to seek formal support for their experiences encountered barriers to access that were likely pre-existing but amplified by the pandemic. Self-reported perinatal depression and anxiety were prevalent in this study and can potentially impact the well-being of pregnant and postpartum people as well as their children and families. The findings from this study highlight the importance of periodic mental health screening to improve the accessibility of mental healthcare and support. Recognizing how and why pregnant and postpartum individuals seek support for feelings of depression or anxiety can inform future health policy to better serve this population.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241282258 – Supplemental material for Seeking mental health support for feelings of perinatal depression and/or anxiety during the COVID-19 pandemic: A qualitative descriptive study of decision-making
Supplemental material, sj-docx-1-whe-10.1177_17455057241282258 for Seeking mental health support for feelings of perinatal depression and/or anxiety during the COVID-19 pandemic: A qualitative descriptive study of decision-making by Katrina Shen, Cassandra Kuyvenhoven, Andrea Carruthers, Manisha Pahwa, Dima Hadid, Devon Greyson, Hamideh Bayrampour, Jessica Liauw, Caroline Mniszak and Meredith Vanstone in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241282258 – Supplemental material for Seeking mental health support for feelings of perinatal depression and/or anxiety during the COVID-19 pandemic: A qualitative descriptive study of decision-making
Supplemental material, sj-docx-2-whe-10.1177_17455057241282258 for Seeking mental health support for feelings of perinatal depression and/or anxiety during the COVID-19 pandemic: A qualitative descriptive study of decision-making by Katrina Shen, Cassandra Kuyvenhoven, Andrea Carruthers, Manisha Pahwa, Dima Hadid, Devon Greyson, Hamideh Bayrampour, Jessica Liauw, Caroline Mniszak and Meredith Vanstone in Women’s Health
Footnotes
Acknowledgements
The authors thank Sujane Kandasamy, Shipra Taneja, Njideka Sanya and Marina Sadik for their contributions to study conceptualization, data collection and/or participant recruitment.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.