
Abstract
Background:
Kidney transplantation is a superior treatment for end-stage renal disease (ESRD), compared with hemodialysis, offering better quality of life and birth outcomes in women with ESRD and lower fertility rates.
Objectives:
To investigate the pregnancy, maternal, fetal, and graft outcomes following kidney transplantation in women with ESRD and evaluate the improvements in quality of life and associated risks.
Design:
A systematic review and meta-analysis performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and the Meta-analysis of Observational Studies in Epidemiology guidelines.
Data Sources and Methods:
A thorough search of multiple databases, including PubMed, Embase, Scopus, ATC abstracts, and Cochrane Central Register of Controlled Trials, was conducted to identify studies that analyzed pregnancy outcomes in kidney transplant patients. The search was conducted from the inception of each database to January 2023.
Results:
The study reviewed 109 studies that evaluated 7708 pregnancies in 5107 women who had undergone renal transplantation. Of these, 78.48% resulted in live births, 9.68% had induced abortion, and 68.67% had a cesarean section. Miscarriage occurred in 12.54%, preeclampsia in 20.87%, pregnancy-induced hypertension in 24.30%, gestational diabetes in 5.08%, and preterm delivery in 45.30% of cases. Of the 853 recipients, 123 had graft loss after pregnancy and 8.06% suffered acute rejection.
Conclusion:
Pregnancy after kidney transplantation is associated with risks for mother and fetus; however, live births are still possible. In addition, there are reduced overall risks of stillbirths, miscarriages, neonatal deaths, and gestational diabetes.
Registration:
PROSPERO (CRD42024541659).
Introduction
Kidney transplantation, compared with hemodialysis, has significantly improved the quality of life of patients with end-stage renal disease (ESRD). 1 However, women of childbearing age (18–49 years) with ESRD have significantly lower fertility rates than do healthy women; besides, they have an increased risk of adverse pregnancy outcomes, such as preeclampsia, intrauterine growth restriction, preterm birth, and a decline in renal function.2,3 Therefore, renal transplantation is crucial for improving the prognosis and maternal and fetal outcomes in pregnant women with ESRD; in addition, it increases the rate of fertility in non-pregnant women owing to the rapid restoration of hormonal function. 2 Successful pregnancies have been reported in kidney transplant recipients since 1958, offering hope to those who wish to conceive. 4
Pregnancies in kidney transplant recipients are considered to have a better prognosis, compared with pregnancies in dialysis patients 1 ; however, such pregnancies pose challenges, including adverse maternal and fetal outcomes, such as preeclampsia, gestational diabetes, fetal growth restriction, preterm birth, and a high incidence of cesarean section. Exposure to immunosuppressants increases the chances of congenital disabilities in the unborn child, necessitating rigorous antenatal care and monitoring.5,6 Kidney transplantation is a common treatment option for women of childbearing age with ESRD; however, the limited availability of high-quality data has made it challenging to guide clinical decision making and support pregnant patients with kidney transplants. The increasing occurrence of such pregnancies in recent decades poses escalating challenges for nephrologists and obstetricians. Moreover, there is a paucity of literature, specifically panoptic meta-analyses, addressing the effects of renal transplantation on pregnancy, thus underscoring the need for further investigation. To address this gap, we aimed to conduct a systematic review and meta-analysis to provide a comprehensive overview of post-kidney transplantation pregnancy outcomes.
Methods
Data sources and search strategy
We conducted a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Meta-analysis of Observational Studies in Epidemiology guidelines7,8 to assess pregnancy outcomes in women older than >18 years who underwent kidney transplantation. This review was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42024541659). We conducted a comprehensive search of several databases, such as PubMed, Embase, Scopus, ATC abstracts, and the Cochrane Central Register of Controlled Trials, spanning from inception of the database till January 2023. Our search strategy incorporated relevant Medical Subject Headings terms and pertinent keywords associated with pregnancy outcomes and kidney transplantation. The PubMed search string is provided in Supplemental File 1.
Study selection
All articles identified through the systematic search were exported to EndNote reference library version 20 (Clarivate Analytics, (US), LLC), where duplicates were removed. We included observational studies (prospective cohort, cross-sectional, and retrospective cohort studies), case series, and case reports (with >10 pregnancies) that assessed pregnancy, maternal, and fetal outcomes in women of reproductive age (>18 years of age) who had undergone kidney transplantation. Studies on patients with multiple organ transplants, studies that examined the teratogenic effects of sirolimus or mycophenolate, and non-English publications were excluded. Two investigators (MSM and FJ) independently reviewed the titles and abstracts of the identified studies. If eligibility could not be determined from the abstract, a full-text review was conducted. Any discrepancies were resolved by a third independent investigator (AAR).
Data extraction and quality assessment
Data extraction and quality assessment were performed by three authors (MUS, SR, and AAR) according to established protocols. All three authors verified the accuracy of the data, and any discrepancies were addressed through consultation with a fourth team member (MSM). The location, length, and duration of the study, the number of recipients of kidney transplants, number of pregnancies, mean maternal age, and mean time between kidney transplant and pregnancy were included in the extracted data. In addition, the number of live births, miscarriages, induced abortions, stillbirths, and ectopic pregnancies were included in the pregnancy outcomes. The following data were also included: the number of women with preeclampsia, gestational diabetes mellitus, and cesarean sections; the number of preterm births, mean gestational age, mean gestational weight, and number of neonatal deaths; and the number of graft failures and acute rejection episodes during and after pregnancy. The number of pregnancies was used as the denominator for outcomes, such as live births, miscarriages, induced abortions, stillbirths, ectopic pregnancy, preeclampsia, pregnancy-induced hypertension (PIH), and gestational diabetes mellitus, to guarantee uniformity of the collected data. However, the denominator for preterm delivery, cesarean section, and neonatal mortality was the count of live births. For acute rejection, the denominator was the total number of recipients. A live delivery before 37 weeks of gestation was considered preterm.
Statistical analysis/meta-analysis
The study presented patients’ demographic parameters as frequencies and expressed pregnancy incidence as the proportion of women per 1000 live births. Prevalence with 95% confidence intervals (CIs) was used to demonstrate each included study’s estimates, and a random-effects model was used to pool the data from individual studies. The Higgins I 2 statistic value was used for heterogeneity evaluation, and a value of >50% was considered significant. For binary outcomes, the Der Simonian and Laird approach was applied; for continuous outcomes, the weighted average methodology was used to compute the pooled estimates and 95% CIs. Furthermore, the study investigated the association between maternal age, the gap between kidney transplants and pregnancy, and pregnancy success. It also offered incidents per 100 observations for continuous outcomes. A location-based subgroup analysis of the pregnancy, maternal, and fetal outcomes was performed. R meta package was used for the analyses. In addition, we conducted a sensitivity analysis using leave-one-out analysis to identify the trials causing significant heterogeneity.
Results
Of the 4425 articles that were retrieved, 2088 full-text articles were reviewed, and 109 were eventually selected for inclusion in the final study,9 –116 as shown in the PRISMA flow diagram (Figure 1). The total number of pregnancies was 7728 in 5107 transplant recipients. The mean maternal age was 30.3 ± 3.21 years, and the mean interval from transplant to pregnancy was 5.6 ± 1.95 years. Baseline characteristics of the included studies are presented in Table 1. Maternal demographics and pregnancy, maternal, and fetal outcomes are presented in Table 2. Forty-one studies conducted in Asia, 5 in Africa, 39 in Europe, 9 in South America, 10 in North America, and 5 in Oceania were included (Table 3).

PRISMA flow chart summarizing the systematic review process according to PRISMA guidelines, showing the number of records identified, screened, assessed for eligibility, and included in the systematic review and meta-analysis.
Baseline characteristics of included studies.

N/A: not applicable.
Maternal demographics, pregnancy outcomes, obstetric complications and delivery outcomes among kidney transplant recipients.

Reported in mean ± standard deviation. Remaining outcomes reported in rates in percentage.
Number of studies according to region.

Pregnancy outcomes
The total number of events reported was 5974, of which live births comprised 78.48% (n = 4505; 95% CI, 75.48–81.49), which was higher than the percentage in the United States (US) general population (56.6%) 117 and was favorable across all geographic locations. The percentage of induced abortions was 9.68% (n = 567; 95% CI, 7.67–11.69) and that of miscarriages was 12.54% (n = 688; 95% CI, 10.61–14.47), both of which were lower than those in the US general population (24.8% and 19.8%, respectively). 118 The rate of stillbirths was 3.06% (n = 189; 95% CI, 2.35–3.77), which was lower than that in the US general population (5.74%). 119 Ectopic pregnancies were reported in 0.94% (n = 25; 95% CI, 0.12–1.77) of transplant recipients, which was lower than that in the US general population (1.4%). 120 The rate of ectopic pregnancy in the present study differed from the result of a previous meta-analysis, which found an ectopic pregnancy rate higher than that in the US general population (2.4% vs 1.4%). 120 Globally, the live birth rate was highest in Europe (84.50%); however, it was generally favorable across all geographic regions: Africa (80.69%), Asia (74.41%), North America (70.57%), South America (76.90%), and Oceania (76.35%) (Figure 2). The induced abortion rate was highest in South America (17.02%), followed by Asia (11.91%), Oceania (10.28%), North America (8.07%), Europe (7.03%), and Africa (6.39%) (Figure 3). The overall miscarriage rate was low, with the lowest incidence in Oceania (8.64%), followed by Asia (12.02%), Europe (12.24%), Africa (12.71%), North America (14.59%), and South America (17.07%) (Figure 4). The overall stillbirth rate was linear worldwide, with the highest rate in Asia (3.7%) and the lowest in North America (1.48%) (Figure 5). The overall incidence of ectopic pregnancy was low, with the highest rate in North America (2.64%) (Figure 6).
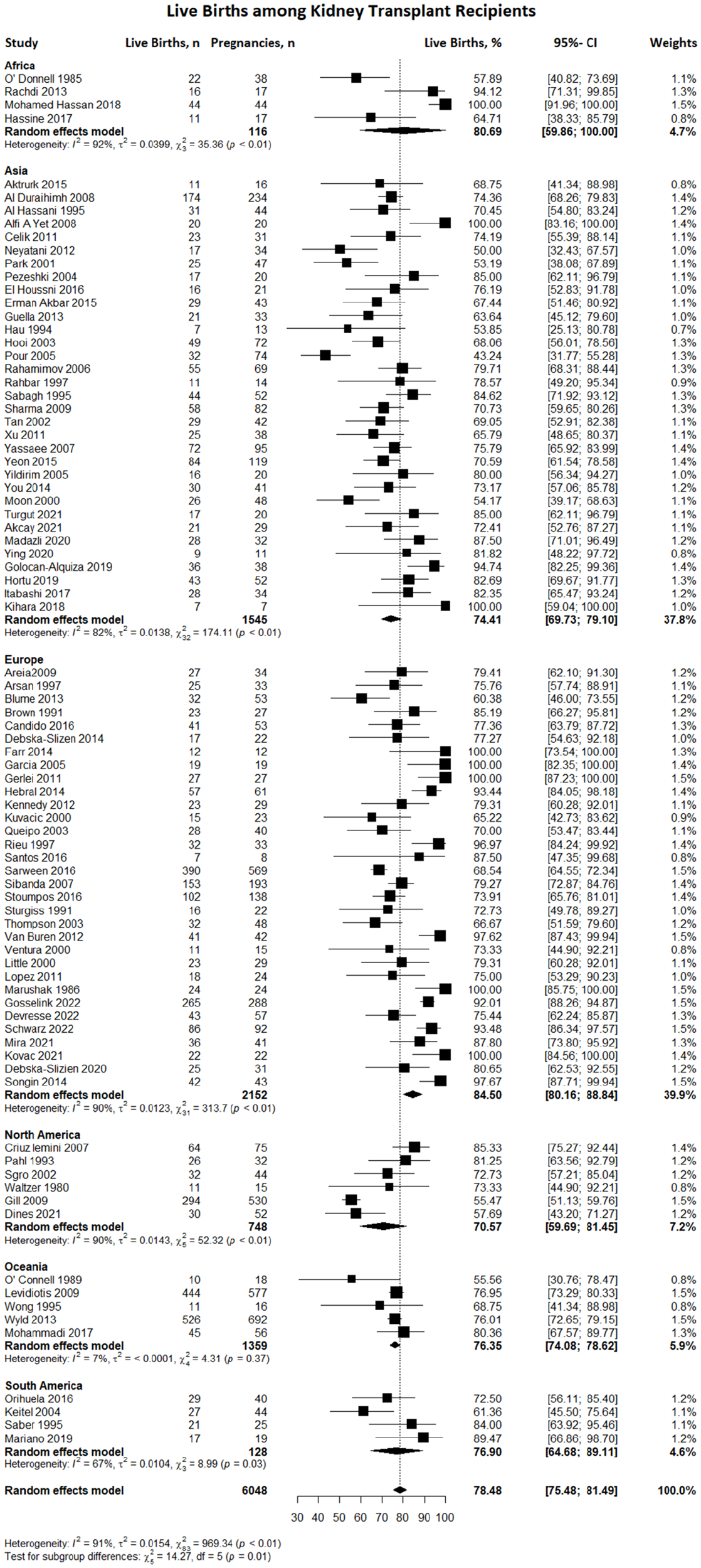
Forest plot illustrating the incidence of live births among kidney transplant recipients, both globally and within distinct geographical regions.

Forest plot illustrating the occurrence of induced abortions among kidney transplant recipients overall and in various geographical regions.

Forest plot illustrating the incidence of miscarriages among kidney transplant recipients overall and in diverse geographical regions.

Forest plot depicting the occurrence of stillbirths among kidney transplant recipients overall and across various geographical regions.

Forest plot illustrating the outcomes of ectopic pregnancies among kidney transplant recipients both overall and across different geographical regions.
Maternal outcomes
The maternal outcomes included in our study were preeclampsia, cesarean section, gestational diabetes, and PIH. Of these, the most frequently reported outcome was a cesarean section, at 68.67% (n = 2043; 95% CI, 63.95–73.39), which was twice as high as that in the US general population (32.1%). 121 This was followed, in descending order, by PIH (24.30%) (n = 491; 95% CI, 18.40–30.20), preeclampsia (20.87%) (n = 864; 95% CI, 18.25–23.48), and gestational diabetes (5.08%) (n = 224; 95% CI, 3.61–6.55). Although the rate of preeclampsia in the US population was six times lower than that in our study (3.8%), 122 the rate of gestational diabetes in the US population was higher than that in our study (7.8% vs. 5.08%). 123 Globally, the overall cesarean section rate was high, with the highest rate reported in South America (89.4%), followed by Africa (70.6%); the lowest rate was reported in North America (61.4%) (Figure 7). There was an overall increase in the rate of preeclampsia, with the highest rate reported in Oceania (27.3%), followed by North America (25.6%), Asia (22.0%), Europe (19.17%), South America (18.27%), and Africa (16.21%) (Figure 8). Gestational diabetes rates were significantly promising worldwide, with the lowest incidence reported in Oceania (0.65%) and the highest in Europe (7.09%) (Figure 9). Lastly, the rate of PIH was highest in South America (51.3%) and lowest in Africa (15.5%) (Figure 10).

Forest plot displaying the outcomes of cesarean sections among kidney transplant recipients overall, as well as across different geographical regions.

Forest plot depicting the occurrence of preeclampsia among kidney transplant recipients overall and in various geographical regions.

Forest plot illustrating the incidence of gestational diabetes among kidney transplant recipients overall and across diverse geographical regions.

Forest plot demonstrating the occurrence of pregnancy-induced hypertension among kidney transplant recipients overall and in various geographical regions.
Fetal outcomes
The fetal outcomes considered in our study included preterm delivery, neonatal mortality, mean gestational age, and mean birth weight. Preterm birth is defined as babies born alive before 37 weeks of gestation. 124 Neonatal mortality is defined as the number of deaths during the first 28 days of life per 1000 live births each year or in another period. 125 The overall rate of preterm birth was 45.3% (n = 1620; 95% CI, 41.26–49.34), compared with 10.8% in the US general population 117 ; neonatal mortality was 1.89% (n = 60; 95% CI, 1.07–2.71), compared with 3.4% in the US general population. 126 The rate of preterm births was highest in South America (59.8%) and lowest in Asia (39.3%) (Figure 11). Neonatal mortality was highest in Africa (31%), followed by Asia (2.69%), showing a significantly lower rate; no neonatal mortalities were reported in North America (0.00%) (Figure 12). The average birth weight of the infants was 2387.7 g (US mean birth weight, 3389 g), and their mean gestational age was 34.3 weeks (US mean gestational age, 38.7 weeks)127,128 (Table 2).

Forest plot illustrating the occurrence of preterm births among kidney transplant recipients overall and across various geographical regions.

Forest plot illustrating the occurrence of neonatal mortality among kidney transplant recipients overall and across diverse geographical regions.
Graft outcomes
Regarding 911 kidney transplant recipients, the total acute rejection rate during pregnancy was 8.06% (n = 92; 95% CI, 5.61–10.51). This rate is comparable to the average rejection rate in transplant recipients in the US general population (7.1%). 129 The following are the rates in each region: Asia, 12.14%; South America, 9.6%; Oceania, 9.09%; North America, 6.67%; Europe, 5.54%; and Africa, 4.76%. Asia had the highest acute renal allograft rejection rates (Figure 13). Although there was a significant variation in graft failure during the follow-up period (1–14 years), there were 123 cases of graft loss (14.42%) among 853 recipients in 19 studies in which 2-year post-pregnancy graft loss was reported. Mean creatinine before pregnancy (mg/dL) and mean creatinine after pregnancy (mg/dL) were 1.16 ± 0.16 and 1.36 ± 0.18, respectively.
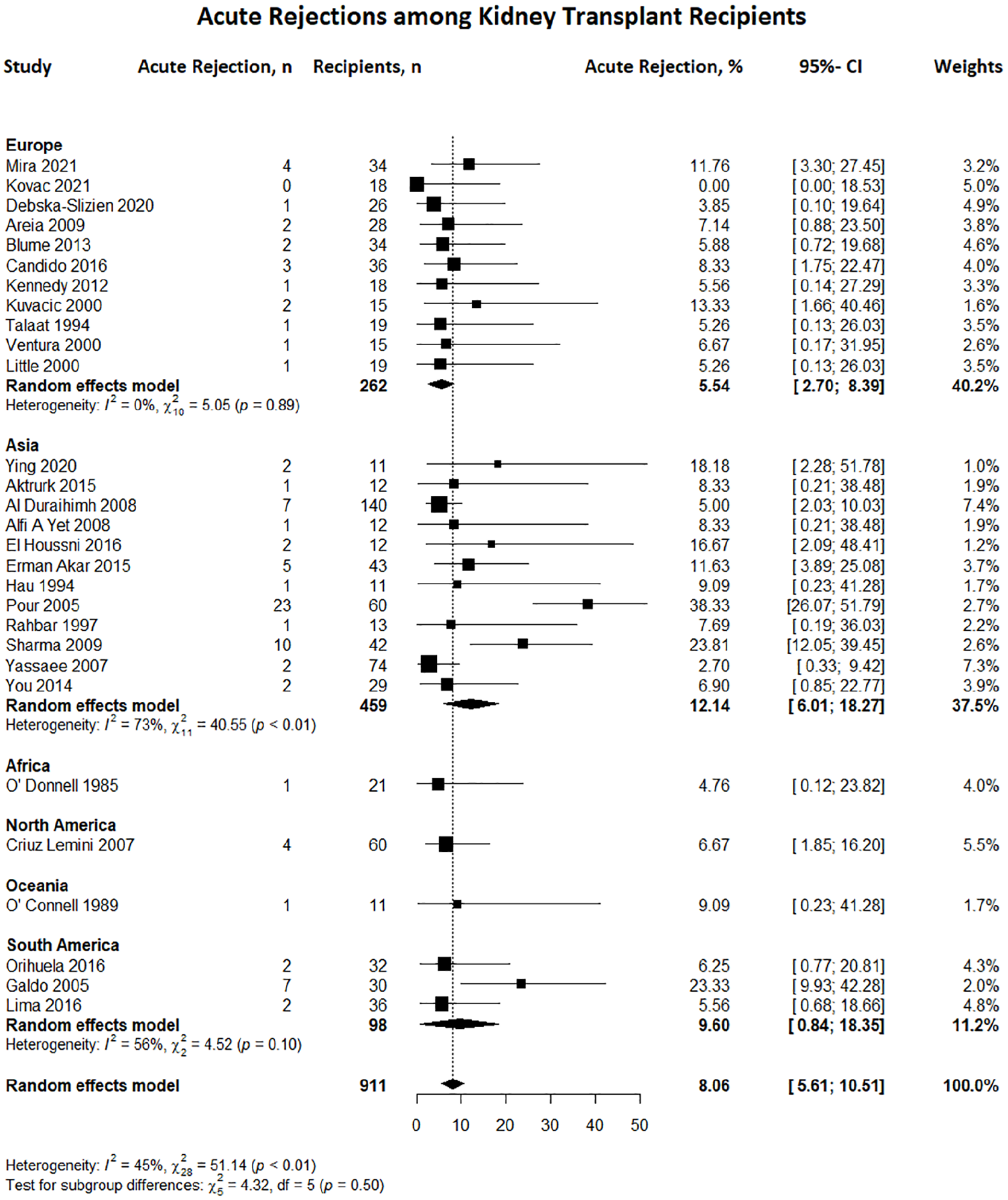
Forest plot displaying the rates of acute rejection among kidney transplant recipients overall and across various geographical regions.
Sensitivity analysis
Sensitivity analyses were performed using the leave-one-out method for some outcomes with high heterogeneity to evaluate the studies responsible for heterogeneity, enhance the accuracy of our research findings, and provide more reliable results. The live birth rate after sensitivity analysis was 74.6%, compared with the mean of 56.6% in the US. 117 The miscarriage rate was 13.6%, compared to 19.8% in the US general population. 118 The rate of induced abortions was 7.1%, compared with 24.8% in the US general population. 118 The rates of preeclampsia and gestational diabetes were 20.36% and 3.7%, respectively, compared with 3.8% 122 and 7.8%, 123 respectively, in the US general population. After sensitivity analysis, the rate of PIH was lower than that in the US general population (24.3% vs. 13.7%), whereas the cesarean section rate was higher (74.5%) than the rate in the US (32.1%). 122 Ultimately, the preterm birth rate was 45.3% in the sensitivity analysis. The preterm birth rate in the US general population was 10.8% (Supplemental Figures 1–8). 116
Interval between renal transplant and pregnancy
The study analyzed pregnancy-related outcomes, based on the interval between renal transplantation and the time of conception, which was categorized into three groups: <2, 2–3, and >3 years. The <2-year interval analysis was based on four studies comprising 141 pregnancies; the 2–3-year interval analysis was based on 11 studies that included 400 pregnancies; and the >3-year interval analysis was based on 66 studies, encompassing a total of 4748 pregnancies.
In cases where the interval between pregnancies was <2 years, the live birth rate was 81.96%, whereas the rates of induced abortion, spontaneous abortion, stillbirth, and neonatal death were 3.59%, 12.72%, 8.04%, and 2.44%, respectively. The maternal outcomes in these cases included a cesarean section rate of 54.6%, a preeclampsia rate of 18.6%, and a PIH rate of 15.9%. Fetal outcomes revealed a preterm delivery rate of 45.2%, a mean gestational age of 37.11 weeks, and an average birth weight of 2868.5 g. The acute rejection and graft loss rates were 11.95% and 16.67%, respectively.
In cases where the interval between pregnancies was 2–3 years, the live birth rate was 73.13%, whereas the rates of induced abortion, spontaneous abortion, stillbirth, and neonatal death were 14%, 12.61%, 3.31%, and 2.80%, respectively. Maternal outcomes in these cases included a cesarean section rate of 74.02%, preeclampsia rate of 25.95%, PIH rate of 28.79%, and gestational diabetes rate of 8.76%. Fetal outcomes revealed a preterm delivery rate of 47.70%, a mean gestational age of 33.7 weeks, and an average birth weight of 2463.74 g. Regarding graft outcomes, the acute rejection rate was 19.58%.
In cases where the interval between pregnancies was >3 years, the live birth rate was 81.89%, whereas the rates of induced abortion, spontaneous abortion, stillbirth, and neonatal death were 10.72%, 12.67%, 2.65%, and 1.65%, respectively. Maternal outcomes in these cases included a cesarean section rate of 70.76%, preeclampsia rate of 21.81%, PIH rate of 21.69%, and gestational diabetes rate of 5.25%. Fetal outcomes revealed a preterm delivery rate of 45.30%, a mean gestational age of 35.32 weeks, and an average birth weight of 2470.77 g. Regarding graft outcomes, the acute rejection rate was 4.21%, whereas the graft loss rate was 14.49% (Table 4; Supplemental Figures 9–20).
Pregnancy-related outcomes stratified by study mean interval between transplant and pregnancy.

N/A: not applicable.
Maternal age at conception
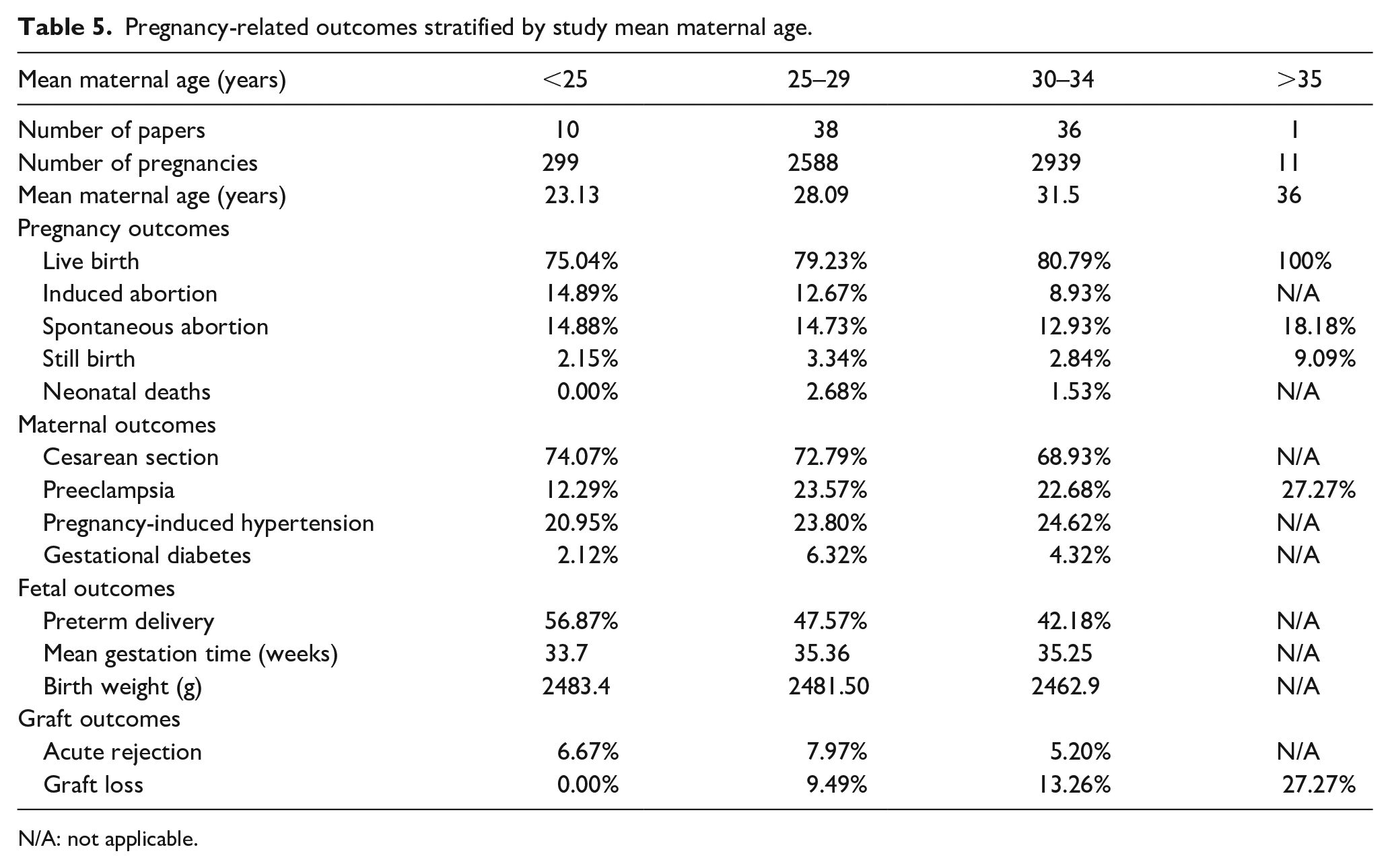
Pregnancy-related outcomes were stratified into four groups based on the mean maternal age: <25, 25–29, 30–34, and >35 years. The analysis for the <25-years age group was based on 10 studies with 299 pregnancies. For the 25–29-year age group, we analyzed 38 studies with 2588 pregnancies. The analysis of the 30–34-year age group was based on 36 studies with 2939 pregnancies. For the >35-years age group, we included only one study with 11 pregnancies.
The live birth rate was 75.04% among individuals aged <25 years. The rates of induced abortions, spontaneous abortions, and stillbirths were 14.89%, 14.88%, and 2.15%, respectively. Maternal outcomes included a cesarean section rate of 74.07%, preeclampsia rate of 12.29%, PIH rate of 20.95%, and gestational diabetes rate of 2.12%. Fetal outcomes revealed a preterm delivery rate of 56.87%, a mean gestational age of 33.7 weeks, and an average birth weight of 2483.4 g. Graft outcomes showed an acute rejection rate of 6.67% and a graft loss rate of 0.00%.
For individuals aged 25–29 years, the live birth rate was 79.23%. The rates of induced abortions, spontaneous abortions, stillbirths, and neonatal deaths were 12.67%, 14.73%, 3.34%, and 2.68%, respectively. Maternal outcomes included a cesarean section rate of 72.79%, preeclampsia rate of 23.57%, PIH rate of 23.80%, and gestational diabetes rate of 6.32%. Fetal outcomes revealed a preterm delivery rate of 47.57%, a mean gestational age of 35.36 weeks, and an average birth weight of 2481.50 g. Graft outcomes showed an acute rejection rate of 7.97% and a graft loss rate of 9.49%.
For individuals aged 30–34 years, the live birth rate was 80.79%. The rates of induced abortion, spontaneous abortion, stillbirth, and neonatal death were 8.93%, 12.93%, 2.84%, and 1.53%, respectively. Maternal outcomes included a cesarean section rate of 68.93%, preeclampsia rate of 22.68%, PIH rate of 24.62%, and gestational diabetes rate of 4.32%. Fetal outcomes revealed a mean preterm delivery rate of 42.18%, a mean gestational age of 35.25 weeks, and an average birth weight of 2462.9 g. The graft outcomes showed an acute rejection rate of 5.20% and a graft loss rate of 13.26%.
For individuals aged >35 years, the live birth rate was reported to be 100%. However, the rates of spontaneous abortion, stillbirth, and preeclampsia were reported to be 18.18%, 9.09%, and 27.27%, respectively. As for graft outcomes, the graft loss rate was 27.27% (Table 5; Supplemental Figures 21–32).
Pregnancy-related outcomes stratified by study mean maternal age.
N/A: not applicable.
Discussion
The findings of our meta-analysis suggest that, although most pregnancies in women who have undergone kidney transplantation resulted in live births, there were significant incidences of maternal and fetal adverse events. The most common adverse outcomes were cesarean section, preterm delivery, PIH, and pre-eclampsia. Other significant adverse outcomes included gestational diabetes, neonatal mortality, stillbirth, miscarriage, and induced abortion. Compared with the rates in the US general population, this study reported higher rates of live births, stillbirths, preeclampsia, and cesarean sections but lower rates of ectopic pregnancies, gestational diabetes, mean gestational age, birth weight, and graft rejection.
Our study reported a higher live birth rate compared with that in the US general population. 117 The 2018 Annual Report of the Transplant Pregnancy Registry International reported a 75% live birth rate in renal transplant recipients. 130 However, a single-center study reported a lower live birth rate, of only 33.3%, among 182 renal transplant recipients. 131 The high live birth rate in our study may be attributed to reporting and selection bias and the exclusion of pregnancies with confirmed intrauterine fetal abnormalities and/or transplant recipients managed with teratogenic immunosuppressants, such as mycophenolate and sirolimus. Our study’s live birth rate agrees with the live birth rates of 72.9% and 73.5% reported in previous meta-analyses by Shah et al. and Deshpande et al., respectively.120,132
Although our study reports encouraging live birth rates, preterm delivery-induced abortions and miscarriages are common. The preterm birth rate in our study was approximately three-fold higher than that in the US general population, 117 and similar rates (50%–64%) have been reported by the UK, US, and European transplant registries. 133 The higher preterm delivery rate may be due to greater risk factors in renal transplant recipients, such as premature rupture of membranes, urinary tract infections, and acute graft rejection. 134 However, the literature suggests that iatrogenic preterm deliveries should be reserved for patients with suspected fetal renal compromise and preeclampsia. 135
The higher rates of induced abortion and miscarriages in the US than those in our study may be due to the use of mycophenolate, which is associated with a higher risk of miscarriage and fetal malformation. 136 Thus, it is essential to advise transplant recipients to discontinue mycophenolate for at least 6 weeks before conception. 137 Consequently, the lower rates of abortions and miscarriages in our study may be due to the selection of women who were qualified to continue with their pregnancies. Neonatal mortality and stillbirth rates in our study were comparatively lower than the rates in the US119,126; however, excessive preventive measures in terms of pre-pregnancy counseling and antenatal care are still required. Similar neonatal mortality rates have been described in a retrospective cohort study with data pooled from the Australia and New Zealand Dialysis and Transplant Registry and perinatal datasets, advocating the need for antenatal care and preconception counseling for pregnancies in renal transplant recipients. 138
Our study highlights the significantly increased risk of complications for mothers who have undergone kidney transplantation, with preeclampsia affecting almost a quarter of women and being approximately six times more common than that in the US population. 122 Preeclampsia can lead to several maternal and fetal complications and poses a significant challenge for clinicians in terms of diagnosis and management. 132 Our research outcomes correspond with those reported by Coscia et al., who observed notably elevated incidence rates of preeclampsia (31%) and hypertension (54%) in female transplant recipients. 135 Furthermore, in another study of 15 female transplant recipients, the rate of hypertension was 46.6%. 139 The high rate of hypertension in pregnant transplant recipients could be associated with the use of calcineurin inhibitors and corticosteroids, donor kidney type, and modifiable maternal factors, such as smoking, alcohol consumption, and obesity. 140
The incidence of gestational diabetes in transplant recipients was lower in our study than in the US general population 123 ; however, close monitoring is important because of the potential risks for the mother and newborn. Moreover, factors such as immunosuppressive drugs, like tacrolimus, pre-existing conditions such as obesity, family history of diabetes, and advanced maternal age can increase this risk. 141 Women who have received a transplant require guidance on managing pre-existing conditions before becoming pregnant to optimize their health before conception. 142
Regarding the regional disparities in acute renal allograft rejection rates, observed variations, Asia had the highest rejection rates followed by South America, Oceania, North America, Europe, and Africa. Medical management, including pre-transplant evaluation and preparation, surgical techniques, post-operative care, immunosuppressive therapy protocols, and monitoring strategies, are more accessible in developed countries than in developing countries. Moreover, regions with higher rejection rates face challenges related to access to advanced medical technology, medications, or healthcare professionals specialized in transplant care. In contrast, regions with lower rejection rates, like Europe and North America, have extensive resources in transplant centers. Furthermore, variations in donor characteristics, such as donor age, Human Leukocyte Antigens matching, and organ preservation techniques affect transplant outcomes and rejection rates. Regions with limited access to suitable donors or where donor quality may be compromised could experience higher rejection rates, compared with regions with more favorable donor profiles. 143
The mode of delivery for renal transplant recipients remains controversial. In our study, the rate of cesarean sections in renal transplant recipients was at least twice as high as that in the US general population, 122 and several studies have reported similar findings.144,145 The reasons for this include non-medical factors, such as fear of infection and graft injury, newborn welfare, and low optimism for a trial of labor. However, trials of labor and normal delivery did not increase the risk of renal and cardiovascular complications, allograft injury, or sepsis, as suggested by Yin et al. 146 Therefore, cesarean delivery should only be reserved for obstetric reasons, and hospital and delivery unit policies should be revised to lower the rate of cesarean delivery after organ transplantation. Preconception and prenatal care within a patient’s transplant center may improve interdisciplinary management and communication during vaginal delivery. 146
The optimal time interval between transplantation and pregnancy remains debatable. Previously, it was suggested that pregnancy should be delayed for at least 2 years post-transplantation; however, these guidelines have been replaced by the American Society of Transplantation guidelines, which suggest that a transplant recipient can conceive as early as 1-year post-transplantation. 133 Our study showed fewer adverse outcomes and rates with intervals of <2 years, whereas more outcomes and higher rates were found with a 2–3-year interval between transplantation and pregnancy. These outcomes include induced abortion, neonatal death, cesarean delivery, preeclampsia, PIH, gestational diabetes, and acute graft rejection. The mean gestational age and live birth rates were lowest in the 2–3-year interval and highest in the <2 year interval. This is consistent with a meta-analysis by Shah et al. that reported the lowest rates of fetal and maternal complications within 2 years of transplantation, whereas the outcomes were reported to be the highest during the 2–3-year interval. 120 Another study reported that 97% of transplant recipients had successful pregnancies 1 year after transplantation, with 73% having live births. 71 This finding reinforces the importance of following the current guidelines regarding the optimal time interval between transplantation and pregnancy, as well as including preconception counseling, family planning, and contraception as crucial components of the transplant counseling process. 132
Our study provides valuable information on pregnancy outcomes in renal transplant recipients from a diverse region-specific population over several decades. This information can assist in updating the guidelines and management of pregnancy in transplant recipients that are specific to a particular region. However, this study has limitations, including potential bias in participant selection and data reporting owing to voluntary participation. This study excluded patients treated with mycophenolate and sirolimus, which may have affected the overall favorable results of the meta-analysis. Therefore, future research should further investigate this parameter. In addition, there were inconsistencies in the diagnostic criteria for complications such as PIH, preeclampsia, and gestational diabetes, as well as potential confounding factors, such as baseline variations in medical care and socioeconomic differences between countries and regions. The absence of comprehensive data on post-pregnancy reproductive planning among transplant recipients limits the depth of our analysis. This underscores the need to address this crucial aspect of care, considering the associated risks.
Conclusion
Pregnancy after kidney transplantation poses significant risks to maternal and fetal health, including preeclampsia, hypertension, cesarean delivery, stillbirth, preterm birth, and low birth weight. Our meta-analysis revealed variations in outcomes across geographic regions, with differences in the rates of ectopic pregnancy, live births, induced abortions, miscarriages, and stillbirths. Notably, we observed a decrease in ectopic pregnancies over time. Trials of labor and normal delivery do not escalate maternal or graft-related complications and advocate judicious cesarean delivery. Regarding the interval between transplantation and pregnancy, we found that, although the outcomes in those pregnant 2–3 years post-transplantation were worse, outcomes in those pregnant >3 years post-transplantation were the best when compared with the outcomes in the other groups. Improvements in antenatal care have mitigated risks, such as preeclampsia and maternal mortality, with decreased rates of miscarriage attributed to better immunosuppressive regimens and prenatal care. Despite advancements, the risk of congenital abnormalities remains elevated owing to immunosuppressive medications. Although progress has been made, pregnant kidney transplant recipients still require specialized care. Our findings underscore the importance of ongoing research and technological advancements to further enhance outcomes in this high-risk population.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241277520 – Supplemental material for Pregnancy outcomes in renal transplant recipients: A systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057241277520 for Pregnancy outcomes in renal transplant recipients: A systematic review and meta-analysis by Muhammad Saqlain Mustafa, Amber Noorani, Aniqa Abdul Rasool, Fatema Ali Asgar Tashrifwala, Shubha Jayaram, Sandesh Raja, Fatima Jawed, Muhammad Usama Siddiq, Sowmya Govindanahalli Shivappa, Ishaque Hameed and Sriharsha Dadana in Women’s Health
Footnotes
Acknowledgements
The authors would like to acknowledge the Research Council of Pakistan (RCOP) for their support in all aspects of the study.
Declarations
Author’s Note
Ishaque Hameed is also affiliated to Department of Medicine, Medstar Health, Baltimore, USA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.