
Abstract
Lipomas are common benign adipose tissue tumors but are infrequently found in the labia majora, especially at a large size. We report a case of a giant lipoma of the labia majora in a 37-year-old woman diagnosed by imaging methods and successfully treated by surgery. This case highlights the importance of considering lipoma in the differential diagnosis of labial masses and underscores the role of imaging in diagnosis. They need to be differentiated from liposarcoma or omental herniation into Nuck’s canal. It also demonstrates the effectiveness of surgical management for large lipomas in sensitive areas, with attention to both medical and aesthetic outcomes.
Introduction
Lipomas, which are the most common benign tumors of connective tissue, are commonly found in many different parts of the body. 1 They can occur at any age but are most common in middle age.1,2 Most lipomas are small, the majority are less than 5 cm in size and rarely larger than 10 cm. When they exceed 5 cm, they are considered giant lipomas. 3 When excessively large, they can cause serious health problems by compressing blood vessels, nerves, or surrounding organs, leading to swelling and pain.2,4 They affect the patient’s quality of life, causing difficulty in daily tasks, anxiety, discomfort, aesthetic problems, and frigidity.3,5 Giant lipomas often appear in the subcutaneous tissue of the back, shoulders, neck, and limbs. They are extremely rare in the inguinal–perineal area. The first perineal lipoma was reported by Myers 6 in 1923. Several cases of congenital perineal lipoma in infants were reported subsequently. 7 The cause of these tumors remains unclear; however, trauma is believed to be a precipitating factor.1,4 It is difficult to differentiate a perineal lipoma from an inguinal hernia. Misdiagnosis can negatively affect the choice of treatment strategy, even causing secondary injury to the patient.2,3,8
The importance of this condition lies in its rarity and the challenges it presents in diagnosis and management. Through this case, we aim to contribute to the existing knowledge of giant lipomas in this rare location and provide insights that may assist in the management of similar cases in the future. This case report was prepared following the CARE (Case Report Guidelines).
Case presentation
A 37-year-old female patient came to the hospital for examination because she had a mass in her labia majora that had gradually increased in size for about 2 years. She admitted that the mass was a bit uncomfortable but not painful and did not change size significantly with position. Because she was not in pain and embarrassed, she delayed seeking medical attention. She experienced difficulty sitting, walking, and engaging in sexual activity. Her personal and family medical history was unremarkable. During the clinical examination, a large, soft mass was found in the right inguinal–labia majora area. This mass remained stationary when pressure was applied in the groin area and did not change in size when the patient changed positions or performed the Valsalva maneuver. Ultrasound revealed that the right labia majora area had a heterogeneous echogenic space-occupying mass with large multi-arc borders and quite clear boundaries, no vascular signal, about 8 × 11 × 16 cm in size, and no communication with the abdomen through the inguinal region (see Figure 1). Ultrasound diagnosis suspected a lipoma, while differential diagnosis included liposarcoma or omental hernia. Computed tomography (CT) and magnetic resonance imaging (MRI) showed a signal mass of adipose tissue consisting of multiple fat lobes with thin walls and septa, without involvement of the abdominal omentum (see Figures 2 and 3). Diagnosis based on CT and MRI was a lipoma of the labia majora. The patient underwent surgery in the obstetric position, with an elliptical skin incision through the mass, dissection, and removal of the entire mass. A portion of excess skin was removed along with the tumor, then the skin edges were meticulously sutured to stop bleeding and for aesthetics. The surgical gross specimen showed a yellow multilobular lipoma-like mass with excess skin (see Figure 4). Histopathology showed that the cut edges were free of tumor cells, and the tumor consisted of benign fat cells arranged in clusters separated by collagenous fibrous tissue, confirming the diagnosis of benign lipoma (see Figure 5). The patient was discharged from the hospital 3 days after surgery without complications. She was re-examined after 3 months with good health conditions.

(a) Gray-scale and (b) color Doppler ultrasound images showed a hyperechoic mass (asterisks), with interlobular septa (arrows), attached to the perineal soft tissue (arrowheads).

MR images showed that the lesion (asterisks) had a signal intensity similar to adipose tissue, had thin septa (arrows) and was divided into lobes, attached to the right perineum (arrowheads), without enhancement of contrast agent.

Non-enhanced CT scan images in (a) axial, (b) coronal, (c) sagittal planes; (d) 3D reconstruction showed the mass with fat density (asterisks), with multiple lobed septa (arrows), attached to the right labia majora (arrowheads).

The patient (a) photograph and (b) operative specimen showed that the lesion had a characteristic yellow color of fat and had many lobes (asterisks), and excess skin in the labia majora (yellow arrow) was cosmetically cut along with the mass.
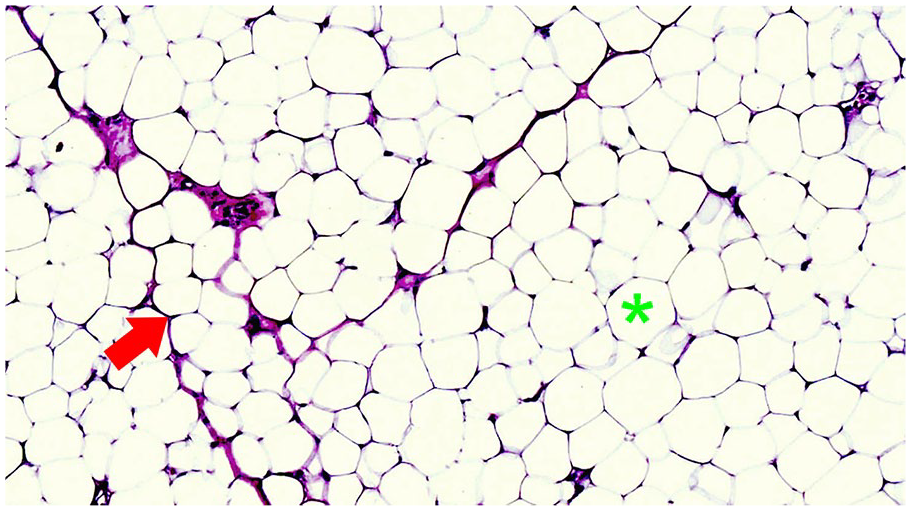
Microscopic image (Hematoxylin & Eosin stain, 400× magnification) showed that the tumor tissue consists of benign fat cells with bright plasma cells, small nuclei shifted toward the periphery, and unclear cell membranes (asterisk). These cells form clusters separated by collagen fiber tissue (arrow).
Discussion
Lesions in the inguinal area can be non-neoplastic or neoplastic. Neoplastic lesions include lipomas, epidermoid cysts, synovial sarcomas, and abnormal lymph nodes. Non-neoplastic lesions include hernias, Kimura disease, inflammation, and hematomas. Their clinical manifestations are very similar. Lipomas rarely occur in the perineal area in adults, and they are very rare in the labia majora.1,2,4
Occurrence of lipoma in the labia majora is relatively rare and little discussed in the medical literature. The origin areas of perineal lipomas cannot be fully detected and reported. Lipomas grow slowly and do not penetrate nearby tissues. Lipomas typically vary in sizes, from very small to giant, and are usually painless.2,3,5
This report presents a rare case of labia majora lipoma, one that is notable due to its unusual size and location. Lipomas in this area, although benign, can cause significant discomfort and psychological distress to the patient, primarily due to their size and their potential to affect daily activities and personal hygiene. Giant lipomas are easily confused clinically and radiologically with inguinal hernias, atypical lipomas, or well-differentiated liposarcomas; accurate diagnosis often relies on postoperative and pathological findings. The basic manifestation of an inguinal lipoma appears as a swollen mass and sometimes pain. The mass usually increases gradually over a period of months or years.4,6,7
Different lesions in the inguinal region have similar clinical symptoms but different treatment strategies. Therefore, it is important to combine clinical tests to accurately assess the diagnosis of the lesion to support precise surgery. Imaging techniques such as ultrasound, computed tomography, and magnetic resonance are important in distinguishing benign lipomas from other conditions. While labial mass is often approached initially with suspicion of a canal of Nuck hernia, a giant lipoma offers a different direction in both diagnostic evaluation and treatment.8,9 Additional differential diagnoses include vulvar cyst, Bartholin cyst or abscess, leiomyoma, leiomyosarcoma, schwannoma, fibroma, hemangioma, aggressive angiomyxoma, and dermatofibrosarcoma.10 –12
In our case, based on the patient’s physical signs and clinical manifestations, the possibility of labia majora lipoma or canal of Nuck hernia was considered for preliminary diagnosis. However, the ultrasound image of an inguinal hernia with omental fat tissue was very similar to the ultrasound image of an inguinal lipoma; it was difficult to differentiate these two entities. Therefore, further CT or MRI examination is necessary. CT and MRI help differentiate diseases such as inguinal hernia, lipoma, liposarcoma, great saphenous vein tumor, inguinal lymph node lesion, and cold abscess.13,14
Furthermore, the unique surgical challenges and considerations for labia majora lipoma excision, addressing both technical aspects and cosmetic concerns are integral to patient satisfaction, especially in young patients like our case. Because of the large size of the lesion and the difficulty in diagnosis and treatment, accurate diagnosis and appropriate treatment are essential.15,16
Surgical excision is the main clinical treatment for giant lipomas. Liposuction was not performed preoperatively to reduce tumor volume, because the patient did not have biopsy results and the mass remained potentially malignant.1,3,7,17 Instead, we chose dissection and made incisions along the tumor surface to open surgery and completely remove the tumor along with attached excess skin tissue. The treatment effect for patients is very good.
Recurrence of completely resected lipomas is rare, except for specific types such as infiltrative lipomas and spindle cell lipomas.3,5,17,18
Conclusion
Giant labia majora lipoma, though rare, should be considered in the differential diagnosis of large labial masses. Imaging plays a critical role in diagnosis, and surgical excision remains the mainstay of treatment. This case contributes to the limited but growing body of literature on giant lipomas in atypical locations and underscores the need for awareness and skill in managing such unique cases. Through this case, we aim to contribute to the existing knowledge about giant lipomas in this rare location and provide insights that may aid in the management of similar future cases.