
Abstract
Background:
Premenstrual syndrome is a relatively prevalent condition that affects a significant number of menstruating women worldwide. It can range from mild to severe and may interfere with daily activities.
Objective:
This study aims to investigate the prevalence of premenstrual syndrome and its associated factors among female university students in Dubai.
Design:
This study was designed as a cross-sectional study.
Methods:
The analysis for this study involved 217 female university students (aged ⩾18 years old) who completed a self-reported online questionnaire. Participants were recruited through simple random sampling, and the study received ethical approval from the Zayed University Ethical Committee.
Results:
All participants reported that they experienced at least one premenstrual syndrome symptom with different levels of severity. The prevalence rate of psychological, physical, and behavioral symptoms was 83.0%, 79.4%, and 76.6%, respectively. The most frequently reported premenstrual psychological symptoms were loss of control (69.6%). Most reported physical premenstrual symptoms included lethargy/fatigue/decreased energy (56.7%); premenstrual syndrome symptoms interfered with participants’ daily routines (45.2%). Normal body mass index, no smoking, milk consumption, cruciferous vegetables, fruits, animal foods, fish oil supplements, and no fast-food consumption were all significant factors associated with decreasing premenstrual syndrome.
Conclusions:
Premenstrual syndrome is a common menstrual disorder among university students that interferes with their daily routines. Dietary habits and other lifestyle factors were highly related to premenstrual syndrome. Therefore, health promotion programs are highly recommended to encourage healthy diets and lifestyles for females as early as adolescence at the school level.
Introduction
Menstruation is a natural biological process crucial to the reproductive cycle in females. Typically, it recurs approximately every 28 days. 1 Premenstrual syndrome (PMS) is a menstrual disorder characterized by a cluster of behavioral, physical, and emotional symptoms. These symptoms typically manifest during the last week of the luteal phase, coinciding with a decrease in progesterone and estrogen levels, usually occurring in the week preceding menstruation. It is important to note that PMS symptoms can occur at any point during the reproductive years and are not exclusive to the early reproductive age. 2 Furthermore, PMS symptoms can significantly disrupt a woman’s daily life for an extended period. About 5%–8% of women suffer from a severe form of PMS, and its common symptoms include irritability, tension, depressed mood, tearfulness, and mood swings, in addition to several pains, including back pain, headache, tender breasts, generalized body aches, and joint pain. Moreover, PMS patients usually experience cravings for sweet, salty, fatty foods3 –5 and appetite changes.1,6,7 In his book “The Palgrave handbook of critical menstruation studies,” King et al. 8 emphasize the emergence of menstruation as both an ethical and an emotional issue, resulting in many females feeling self-conscious and embarrassed due to the ongoing sociocultural stigma surrounding this natural process. Likewise, research conducted in Gana and Pacific Island countries has established a direct association between these perceptions and prevalent cultural and religious beliefs.9,10
PMS is a relatively prevalent condition that affects many menstruating women worldwide. Globally, between 20% and 32% of premenopausal women and 30% and 40% of women of reproductive age reported having PMS during their menstrual cycle. 11 Another recent study showed that the prevalence of PMS increased from 10% to 53% among female adolescents worldwide. 12 In addition, one study in Saudi Arabia found that one-third of secondary school females complain of PMS. 13 Moreover, a woman starts to face it the weeks before her menstrual period, as it can describe the combination of emotional and physical hurtful symptoms. It might be mild or severe enough to conflict with performing daily activities. PMS is more likely to affect adults, especially those with poor physical health, high body mass index (BMI), or who suffer from amenorrhea (the absence of periods), in addition to those with high levels of stress, a family history of depression, and/or postpartum depression. 14 The exact cause of PMS is not clear yet. Generally, estrogen and progesterone hormone levels decline a few days before the period. That is what doctors have suggested as the primary cause that triggers PMS symptoms, in addition to the occurrences of deficiencies in specific vitamins and minerals, eating too many salty foods, drinking alcohol, or using caffeine. 14 Several studies identified the contributing factors to PMS, especially in the Arab regions, including jobs, marital status, BMI, menarche, the average length of the menstruation cycle, the number of bleeding days per cycle, a family history of PMS, physical inactivity, excess consumption of coffee, frequent consumption of fast food, and smoking.4,15 Regular exercise, as found in one study, is associated with a reduction in both pain and physical as well as psychological symptoms of PMS. 16 Smoking might exacerbate PMS symptoms due to nicotine’s impact on neurocircuitry, which heightens vulnerability to environmental stressors. 17 It can also lead to social relationship strains, depression, anxiety, mood disorders, and irritable bowel syndrome, in addition to substance abuse like alcohol, drugs, and smoking. 18
PMS is a widespread condition impacting most females of reproductive age physically and psychologically in the United Arab Emirates (UAE). A cross-sectional study was conducted in 2019 in Sharjah to assess the prevalence of PMS among 300 adult university students aged 18–24 years. It showed that 95% of participants suffered at least one PMS symptom during their menstrual cycle. Regarding the prevalence of PMS, it was 35.3%. In addition, smoking and high-calorie/sugar/fat/salt food intake were strongly associated with PMS in the UAE. 4 However, there is limited knowledge about PMS in the UAE, with only one study conducted in Sharjah in 2019. Many questions regarding the association between PMS and lifestyle factors are still not answered, excluding diet and smoking. In addition, numerous menstruating women in the UAE experience harmful symptoms that hinder their ability to perform their daily tasks when it is present. They often perceive that it is normal and every woman can pass through the same experiences. 10 Therefore, conducting this research will help to explore more causes and highlight the effects of PMS.
This study will help women in their reproductive age as it will contribute to concluding the main contributing factors to PMS. Therefore, it will increase their awareness and knowledge about PMS as it is a serious issue and should be treated. The study can also contribute to the health promotion measures and health policies in the universities dealing with females and raising awareness. This study aims to assess the prevalence and severity of PMS and determine the effect of dietary habits and lifestyle behaviors on PMS among female university students in Dubai.
Method
Study design and settings
A cross-sectional study using a self-reported online questionnaire was used to collect the data from female university students in Dubai. Participants were presented with written informed consent before they accessed the survey questions. They were required to read and understand the terms and conditions of participation, which included information about the purpose of the study, data usage, confidentiality, and their rights as participants. Informed consent has been provided electronically through a checkbox. To keep the confidentiality of the participants, names, identifications, emails, and phone numbers were not collected. Participants were informed that their participation was voluntary and that they could exit the questionnaire if they felt uncomfortable. The article adheres to the STROBE checklist guidelines.
Population and sampling
The estimated sample size of the study was 354 participants 19 out of the whole population, which was estimated to be 4500 female students registered at the University in Dubai campus. The confidence interval (CI) used to determine the study sample size was 95% CI, with a margin error of 5, providing 80% power to test differences at a 5% error and a CI of 95%. The online survey was distributed to the selected sample via email by the first author, who had access to all university students’ emails. Simple random sampling was employed to recruit the participants for this study. In total, 400 students approached to participate in completing the survey. After attaining the desired sample size, additional follow-up stopped. Following data cleaning procedures and removing the participants who failed to fill in the necessary information before analysis, the sample size utilized in this study comprised 217 participants, resulting in a response rate of 86.25%.
Eligibility criteria included adult female students aged ⩾18 years and registered at any college in the Dubai campus who experienced regular menstrual periods for at least the past 3 consecutive months. In addition, eligible participants needed to have the capability to understand either English or Arabic and provide informed consent to participate in the study. Exclusion criteria included females not studying at the same university in Dubai campus, those with irregular menstrual cycles, and/or females experiencing amenorrhea (an abnormal absence of menstruation).
Data collection
A self-reported online questionnaire collected the data from October 13, 2021 to November 5, 2021. The questionnaire consisted of demographic information (age, marital status, college, academic year), lifestyle factors (physical activity (PA), dietary, and smoking), and anthropometric measurements (height and weight). The PA used a valid and reliable open International Physical Activity Questionnaire. 20 This section aimed to assess the intensity level (high, moderate, or low intensity), frequency (number of days per week), and duration (hours and minutes per day) of the PAs undertaken by the participants in the past week. In addition, the questionnaire includes a Food Frequency Questionnaire (FFQ) to gather information about the consumption of the foods and beverages that could potentially influence PMS. The FFQ included starchy foods, caffeinated beverages, milk and dairy products, leafy green vegetables, cruciferous vegetables, non-starchy vegetables, fruit, animal foods, herbal teas, and high-calorie/sugar/fat/salt foods. 4
A pilot study was conducted on 10 students (about 3% of the targeted sample size of 368 female students) to make sure that the questionnaire is valid and reliable and has no issues, especially for students who are not familiar with the topic and who might find the terminology difficult, for instance there was the word “legumes” that they did not know what it exactly means. Thus, a clarification consisting of more popular examples has been added, including beans, peas, and lentils. In addition, “fish oil supplements” was unclear for some, so “omega 3” has been added to simplify it, as “omega 3” is more common when talking about fish oil supplements. The collected data underwent a thorough examination to assess its accuracy and completeness. Subsequently, it was meticulously cleaned and coded in preparation for data analysis. Premenstrual symptoms were assessed using the Arabic Premenstrual Syndrome Scale, where validity and reliability of this scale were studied before by Algahtani and Jahrami 21 to be suitable for Arabic-speaking participants with relatively high Cronbach’s values of 0.910. The scale has a symptoms list associated with PMS divided into three categories (psychological, physical, and behavioral symptoms) and four classifications indicating the severity of the symptoms: none, mild, moderate, and severe. It focuses only on the symptoms that participants experienced 1 week before menstruation and a few days into menstruation in the last 3 months. The online survey was distributed by email and WhatsApp.
Statistical analysis
The data collected via Google Forms were imported into Statistical Package for the Social Sciences software version 27.0 for analysis. Descriptive statistics, including mean, standard deviation, and frequencies, was computed for continuous data.
A multivariable logistic regression analysis examined the association between dietary and lifestyle factors (considered explanatory variables) and PMS (the outcome). Odds ratios (ORs) and their corresponding 95% CIs were calculated to elucidate the association between dietary factors, such as dairy products, fruits, and supplements, and lifestyle behaviors, including PA and smoking, as explanatory variables, and the PMS as the outcome. PMS was converted into a binary variable, with “no” indicating the absence of symptoms and mild symptoms, whereas “yes” signifying moderate and severe cases.
To facilitate the interpretation of the OR, the logistic regression analysis used the less healthy option for dietary and lifestyle behaviors as the reference level.
Results
This study involved 217 female students whose ages ranged between 18 and 28 years old. Table 1 presents demographic characteristics and BMI information for the 217 participants in the study. The mean age was 19.7 years, and the mean height and weight were 159.5 cm and 58.1 kg, respectively. Most participants were single (90.3%), 7.8% were married, and 1.8% were divorced. Regarding weight status, 22.1% were underweight, 50.7% had a healthy weight, 16.1% were overweight, and 10.1% were obese.
Participants’ demographic characteristics and BMI (n = 217).

BMI, body mass index; SD, standard deviation.
Table 2 presents the dietary and lifestyle factors of 217 participants. Most participants were non-smokers (94.0%), while 6% reported that they were currently smokers. The majority (85.3%) were performing low-intensity PA.
Participants’ lifestyle and dietary behaviors (n = 217).
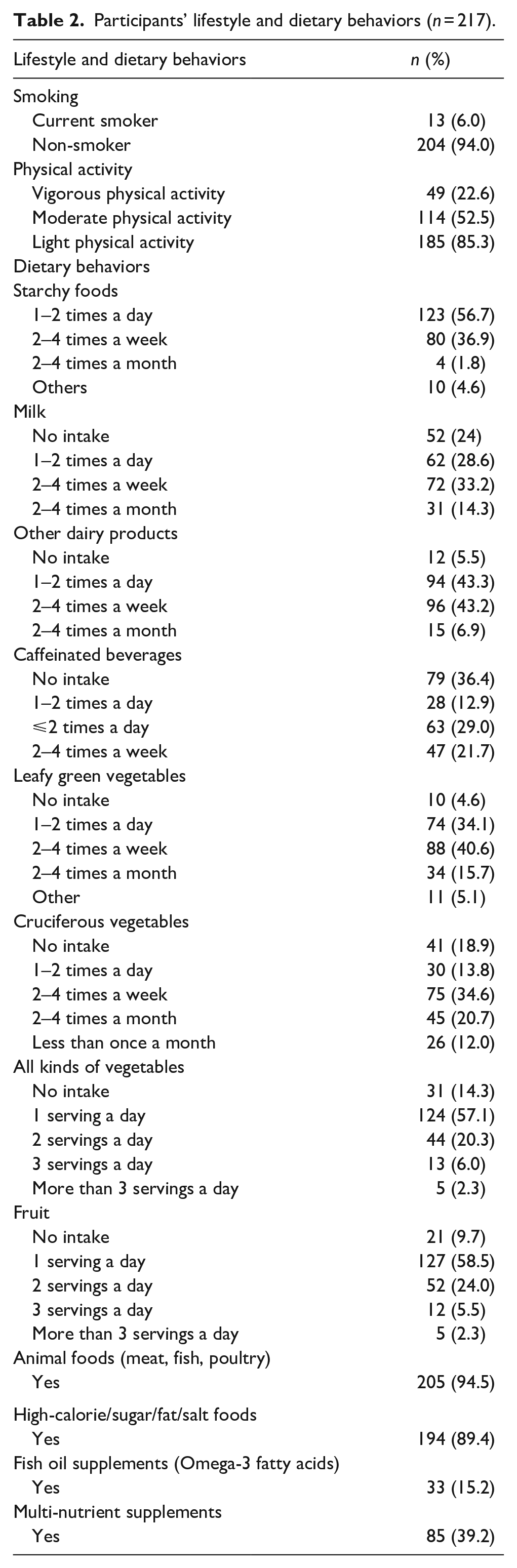
Regarding dietary behaviors before or during PMS, 4.6% do not experience any change in their dietary habits. Daily intake of starchy foods and fruit and vegetables as a minimum of one serving was reported by more than 50% of the participants, with weekly intake of milk, dairy products, leafy green vegetables, and cruciferous vegetables being the most frequently reported choices. More than half (56.7%) of participants consumed starchy foods one to two times a day, while 28.6% consumed milk one to two times a day and 24% did not consume milk, 43.3% consumed dairy products one to two times a day, and 34.1% consumed leafy green vegetables one to two times a day, while cruciferous vegetables were consumed one to two times a day (13.8%). More than half of the participants (58.5%) consumed at least one serving of fruit per day, and the majority (94.5%) reported that they consume animal foods (meat, fish, poultry). Moreover, a large proportion of participants reported consuming high-calorie/fat/sugar/salt foods (89.4%), while a smaller proportion reported taking fish oil supplements (15.2%) or multi-nutrient supplements (39.2%; Table 2).
Table 3 presents the prevalence of PMS symptoms among 217 participants, categorized by levels of severity, ranging from none to severe. The symptoms are grouped into three categories: psychological, physical, and behavioral. Table 3 shows the number and percentage of women who reported none, mild, moderate, or severe symptoms. The psychological symptoms with the highest prevalence were affective lability (68.2%), followed by anxiety/worry (59.9%) and depressed mood (58.1%). The physical symptoms with the highest prevalence were lethargy/fatigue/decreased energy (56.7%), followed by breast tenderness (35.9%) and breast engorgement or weight gain (35.9%). Among the behavioral symptoms, symptoms interfering with relationships (24.4%) and work or school (38.7%) had the highest prevalence.
Prevalence of premenstrual syndrome symptoms by the level of severity (n = 217).

Total for moderate and severe symptoms only.
Generally, mild and moderate premenstrual symptoms were the highest frequently reported, followed by severe symptoms with the least prevalence. Overall, the prevalence rate of psychological symptoms was 83.0%, 79.4% for physical symptoms, and 76.6% for behavioral symptoms. All participants (100%) reported experiencing at least one PMS symptom with different levels of severity. In general, the most frequently reported premenstrual psychological symptoms were loss of control (69.6%), affective lability (68.2%), anger feelings (60.4%), anxiety/worry feeling (59.9%), depressed mood (93.2%), (89.2%), anxiety/worry (88.3%), and increased sensitivity toward others (59%). Most were muscle, abdominal, joint, and back pain (60.4%), craving specific foods (88.6%), and acne (85.0%). Regarding the behavioral symptoms, PMS symptoms interfere with participants’ everyday routine (45.2%), work or school (38.7%), and relationships (24.2%; as shown in Table 3).
Multiple logistic regression
The study findings show a significant positive association between dietary routine and the severity of PMS symptoms (milk product consumption, cruciferous vegetables, animal foods, fast foods, fish oil supplements, BMI of healthy weight). The increase in milk product consumption was significantly related to decreasing the PMS symptoms (OR 0.402, 95% CI (0.192–0.841), P = 0.016). No fast-food consumption was highly significant in decreasing the severity of PMS symptoms (OR 0.101, 95% CI (0.028–0.368), P = 0.001), healthy body weight was significantly associated with less severe symptoms of PMS (OR 0.231, 95% CI (0.070–0.782), P = 0.016), and more consumption of fruits was significantly associated with less severe PMS symptoms (Table 4).
Multiple logistic regression analysis investigating the associations between eating and lifestyle behaviors and the incidence of premenstrual syndrome.

OR, odds ratio; CI, confidence interval; BMI, body mass index; PA, physical activity.
P-value significant at <0.05.
Discussion
This study aimed to assess the prevalence and severity of PMS symptoms within a university student sample and to identify associated dietary and lifestyle factors. According to the available literature, this is the second study that examined the prevalence of PMS among university students in the UAE after the one was done at Sharjah University in 2019. 4 In our study, the participants 100% reported experiencing at least one PMS symptom with different levels of severity. Similarly, Jahrami et al. 15 have found that among the 300 participants in their study, 98.2% reported at least one PMS symptom. In this study, the most prevalent premenstrual symptoms included loss of control, angry feelings, and muscle, abdominal, joint, and back pain. Yeşildere Sağlam and Basar 22 found that the severity of PMS might lead to increased levels of anger as well as anger control level decreases. A study conducted in the United States found that feelings of loss of control and nervousness were experienced by women of reproductive age, with approximately 70% of participants reporting these symptoms. 23 This result is also consistent with the findings of Hashim et al., 4 who reported joint/muscle/back pain and feeling angry are the most common severe symptoms mentioned in their study. Acikgoz et al. 24 have found a significant association between depression and PMS. Likewise, Chumpalova et al. 25 reported irritability, fatigue, changes in appetite, depressed mood, and mood swings were the most common symptoms among the 305 participating females, representing 87.8%, 79.6%, 78.6%, and 76.5%, respectively. Moreover, Al-Qazaz and Al-Dabbagh 26 found that 50% of participants complained of depressed mood out of the other PMS symptoms. In addition, they found that sleep disturbances and difficulty in performing school-related tasks are more common by 90.4% and 82.6%, respectively. PMS is associated with psychological symptoms that range from irritability to depression and could depend on cultural perspectives and dealing with menstruation and social environmental as well as hormonal changes.27 –29 Looking to the fact that stressful university study and the responsibilities that the students go through might increase and intensify the psychological symptoms of other PMS symptoms, which was found in one study in Lebanon among university students. 30 In this study, we found that PMS symptoms were interfering the most with participants’ daily routine work or school and relationships, similar to the findings by Malki among 274 females, aged from 18 to 57 years, having PMS interfering with their home responsibilities, relationships with their families, social life activities, and work productivity. 31
In our study, we observed several factors associated with a reduction in PMS symptoms, including the consumption of milk products, cruciferous vegetables, and animal foods. A randomized controlled study conducted in Turkey examined the impact of milk and dairy product intake on PMS symptoms and women’s quality of life, aiming to determine whether such consumption could alleviate PMS symptoms and enhance the quality of life.32,33 Cruciferous vegetables such as broccoli, cauliflower, and cabbage have been found to exhibit antioxidant properties and aid in the fight against cancer, particularly breast cancer. These vegetables are also rich in vitamins and minerals, help balance estrogen levels, and can alleviate inflammation,34,35 which suggests their effect on reducing PMS. Fruit consumption was another significant diet found to decrease PMS. Fruits such as banana that contains magnesium and potassium were found in one study to effect in reducing PMS, 36 and it was consistent with one study conducted among Spanish university female students in the Halva region, that eating two pieces of fruits would most probably decrease the PMS symptoms. 37 Although possibly owing to the abundance of vitamins and minerals found in fruits, further research is warranted to confirm this. However, this contradicts a recent study conducted in Egypt, which reported no significant association between fruit consumption and the relief of PMS symptoms. 38 Animal products, those containing niacin and B vitamins such as thiamin and riboflavin, are associated with PMS symptom reduction. Research has demonstrated that the consumption of these specific nutrients found in animal products has a positive effect on reducing PMS symptoms. In other words, a diet rich in niacin, thiamin, and riboflavin can potentially alleviate the severity of PMS symptoms. 33
Eating fast food was found in our study to have an adverse effect on the PMS, which was consistent with other studies.33,36,39 Consumption of fatty foods is associated with a decrease in plasma estrogen levels, which in turn is associated with PMS. 39 Studies have shown a significant association between smoking and an increased risk of experiencing PMS symptoms. 40 Moreover, smoking can lead to menstrual irregularity, miscarriage, and other menstrual issues. Smoking for 5 or more years was found to be correlated with a higher prevalence of harmful symptoms of PMS and with many physiological symptoms, including depression and anxiety. The reason for this could be attributed to the impact of cigarette smoking on the regulation of progesterone, estrogen, androgen, and gonadotropin levels. These hormonal imbalances may be considered leading factors in the development of PMS. 4
Our study results indicated no significant associations between PA and PMS symptoms, which is consistent with the findings of Hashim and her colleagues. 4 One systematic review study concludes that there is uncertainty in the relationship between exercises and reducing PMS. 41 However, several studies with different approaches found a significant association between aerobic exercises and reducing PMS symptoms.42 –44 Our findings may not be statistically significant as most female students reported engaging in light PA.
Normal BMI was significantly associated with decreased PMS in our study; a study found that overweight was significantly associated with increasing PMS symptoms possibly due to the lower level of estradiol in women with adiposity. 45 However, this result is inconsistent with what was found by Mizgier and his colleagues, as they reported that women with normal BMI suffered twice as those with overweight (BMI >25 kg/m2). 46 On the other hand, Mesquita and Mahishale found no significant association between BMI and PMS. 47
Limitations
The limitations of our study include a relatively small sample size, as we focused solely on one university in Dubai that might not be representative of female university students in the UAE. Another limitation is that because most of the questions depend on recall, some students may not remember the specific information we are looking for, for instance, the frequency of eating starchy foods, ending up making guesses for the answers. It is difficult to determine the exact risk factors of PMS, such as social stigma and other cultural factors, due to the impact of various important confounding exposures.
Conclusion
In conclusion, the findings of this study emphasize the necessity of considering multiple lifestyle factors to reduce PMS symptoms effectively. While adopting a healthy diet is crucial, the study highlights the significance of other lifestyle factors, such as smoking cessation and maintaining a healthy weight, to alleviate the symptoms. Therefore, early intervention through health promotion programs is essential to increase awareness and encourage the adoption of a healthy lifestyle, including a healthy diet, no smoking, and maintaining a healthy weight among young girls. Moreover, future research should investigate other potential contributing factors, such as socioeconomic status, marital status, and the use of oral contraceptives, on PMS. Furthermore, extending this study beyond universities to encompass the entire UAE may provide a more comprehensive understanding of the prevalence and impact of PMS.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241260026 – Supplemental material for Prevalence of premenstrual syndrome and its associations with dietary and other lifestyle factors among university female students in Dubai: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057241260026 for Prevalence of premenstrual syndrome and its associations with dietary and other lifestyle factors among university female students in Dubai: A cross-sectional study by Haleama Al Sabbah, Noof Al Mutawa and Enas A Assaf in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241260026 – Supplemental material for Prevalence of premenstrual syndrome and its associations with dietary and other lifestyle factors among university female students in Dubai: A cross-sectional study
Supplemental material, sj-docx-2-whe-10.1177_17455057241260026 for Prevalence of premenstrual syndrome and its associations with dietary and other lifestyle factors among university female students in Dubai: A cross-sectional study by Haleama Al Sabbah, Noof Al Mutawa and Enas A Assaf in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.