
Abstract
Round ligament endometriosis is a rare phenomenon reported in approximately 0.3% to 0.6% of endometriosis cases. Presurgical diagnosis is carried out for about 50% of the cases. The association of the right-sided inguinal hernia, nonspecific pain in the organs, and no history of surgery or labor make the diagnosis intricate. We report a case of endometriosis of the round ligament in a 39-year-old woman who complained of intense pain in the right groin during the menstrual period for about 4 years, with no complaints of bulging or change in the size of the mentioned area. The clinical suspicion of inguinal endometriosis, supported by sonography and magnetic resonance imaging, was confirmed by histological examination of the surgical specimen after laparoscopic surgery, which included the mass and the extraperitoneal segment of the round ligament. After surgery, the patient’s pain disappeared completely. The round ligament endometriosis or endometriosis of the inguinal region could be considered an important differential diagnosis in women of reproductive age without a history of surgery who presented with inguinal region pain during menstruation but no clear mass was palpable in the physical exam.
Background
Endometriosis has been reported in approximately 10%–20% of women of reproductive age. It is characterized by the development of ectopic endometrial tissue, which under the stimulus of ovarian hormones takes on the typical proliferative and functional aspects of normal endometrium. 1 It mainly affects pelvic organs, and in 9%–15% of cases, extra pelvic organs are involved. Round ligament endometriosis, which was reported in 1896 for the first time, 2 is a rare finding as it is reported in only 0.3%–0.6% of the cases. 3 Round ligament endometriosis might affect the inguinal canal or the inside part of the ligament. Inguinal endometriosis is often unilateral and occurs on the right side of the body. 4
This study aims to present inguinal endometriosis in a 39-year-old woman with no history of past surgery, complaining of right groin pain with no palpable mass who underwent laparoscopic surgery, with emphasis placed on its radiological and operative features.
Case presentation
The patient was a 39-year-old virgin woman referred to Hazrat Rasoul Hospital of Iran University of Medical Sciences due to severe pain in the inguinal region during menstruation for about 4 years, with no previous diagnosis. Patient had regular menstruation, no history of underlying disease or previous surgery, and a history of dysmenorrhea (Visual analog scale (VAS) 5 of 10) and dyschezia (VAS 8 of 10). She complained of a dull pain in the right groin area during the menstrual cycle, started about 4 years before the visit. The patient mentioned that during the past year, the pain in the groin lasted for 3 days to 2 weeks after the end of the period. However, she did not mention any complaint of feeling a mass or change in the size of the mentioned area. The abdominal and vaginal examinations were normal, and there was no bulging in the right groin; no palpable mass was detected, although the patient experienced mild tenderness on deep palpation of the right inguinal area.
In the sonographic assessments, hypoechoic and hypervascular mass was reported in the right inguinal area with a dimension of 24 × 32 × 21 mm. An abdominal and pelvic magnetic resonance imaging (MRI) was performed, which reported a mass with dimensions of 27 × 16 mm adhesive to the abdominal wall in the right inguinal area. Therefore, based on the clinical history of the patient and the results of paraclinical examinations, abdominal wall endometriosis without involvement of the pelvis and ovaries was proposed as a diagnosis for the patient. This patient was a candidate for surgery after the first visit but she refused to receive any type of treatment.
One year later, the patient returned to our medical center again due to the increased pain in the right groin that continued throughout the day and became continuous. She underwent abdominal and rectal sonographic assessment again. Sonography findings indicated the following: (1) myomas with a maximum size of 50 mm and adhesion from the right ovary to the uterus. (2) An 11 × 20-mm endometriotic nodule adhesive to the anterior serous of the lower rectum in the posterior cervix. MRI indicated a hypoechoic mass of 19 × 50 mm. This mass had a lower intensity than the muscles in T1-weighted images (Figure 1(a)) and T2-weighted images (Figure 1(b)). Based on her history, round ligament endometriosis was proposed. Doppler sonography showed a low level of blood flow in the mass. The mass was close to the inferior epigastric artery origin. Computed tomography (CT) angiography examination of the pelvic arteries, especially the common iliac artery and the external iliac vessels, was normal. Our patient became a candidate for laparoscopic surgery.
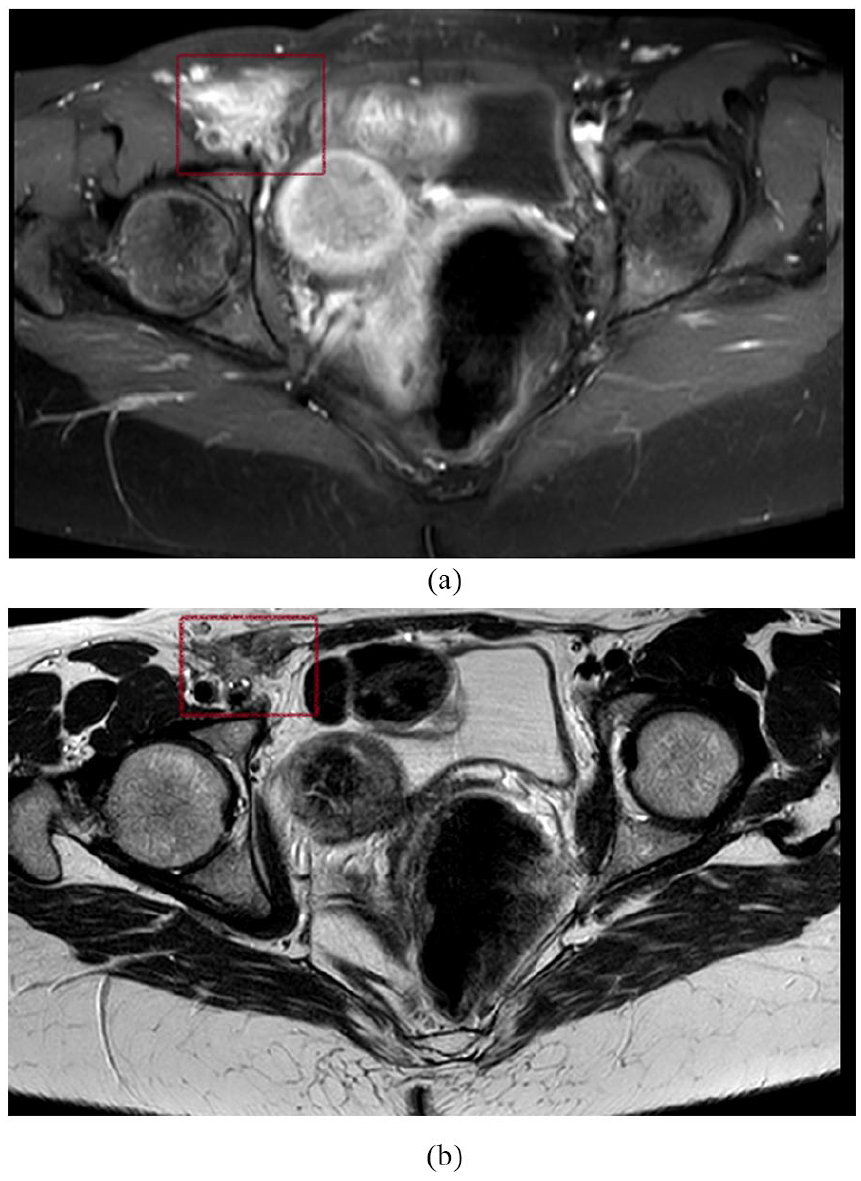
(a) Magnetic resonance imaging T1-weighted image of a hypoechoic solid mass with dimensions of 19 × 50 mm, showing lower intensity than the muscles, and (b) T2-weighted image of the same lesion.
Laparoscopic surgery was performed under sterile conditions and following general anesthesia with the presence of a gynecologist as the surgeon. First, the pelvic cavity and pelvis were explored, and no pathological lesions were observed. The uterus had evidence of myomatosis and contained multiple subserosal and intramural myomas. Both ovaries were normal, and there were no signs of endometrioma. Fallopian tubes were normal. An endometriotic nodule in the uterosacral ligament was present, which was removed. There were no signs of endometriosis in the anterior cul-de-sac or the rectum. The rectovaginal septum was normal. There was an endometriotic solid mass in the right distal round ligament with adhesion to the origin of the inferior epigastric artery. Endometriotic solid tissue surrounding the inferior epigastric artery was removed from the origin to the inguinal ligament site (Figures 2 and 3). Next, microscopic evaluation confirmed the clinical diagnosis of round ligament endometriosis. Microscopically, the tumor consisted of endometrial glands associated with cellular stroma scattered in the fibrous tissue (Figure 4). Right ureteral dissection was also performed.

Endometriotic solid mass in the right distal round ligament with adhesion to the origin of the inferior epigastric artery.

Endometriotic solid tissue removed from the origin to the inguinal ligament site.
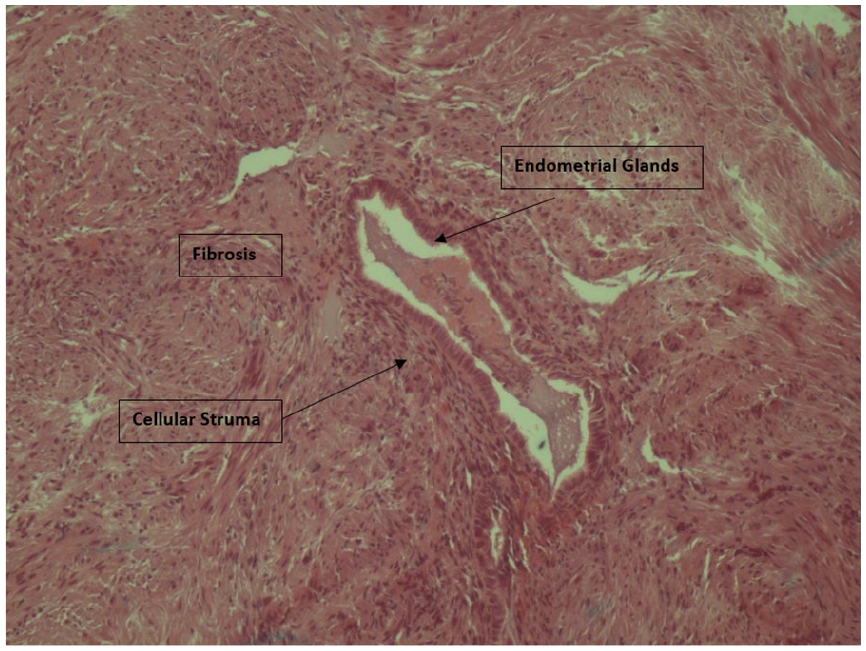
Histopathological evaluation after excision. Verification of endometrial glands associated with cellular stroma scattered in the fibrous tissue.
The postoperative course was regular, and the patient was discharged one day after the operation. To impede relapse, a dienogest tablet was administered every day.
Discussion
Inguinal endometriosis is a rare finding that occurs in less than 1% of endometriosis-affected women. 2 Increasing menstruation pain is the cause of referral to the medical system. The right inguinal region is more commonly involved (90%–94%), and the underlying etiology of this phenomenon has not yet been revealed. 5 Although there are three hypotheses, one is the protective effect of the rectosigmoid colon on the left inguinal canal, and the other is the effect of the clockwise flow of intraperitoneal fluid, which causes endometriosis cells to stay longer on the right.6,7 Third, the vaginalis process closes later in women on the right side and creates a potential space and peritoneal connection to the inguinal canal that causes endometriosis cells to be implanted in the inguinal canal. 8 Endometriosis in the inguinal region was first reported by Cullen in 1896. Candiani et al. 20 reviewed 958 patients who underwent clinical evaluation for endometriosis and reported that the incidence of endometriosis in the inguinal region was 0.6%. The intraperitoneal and extraperitoneal portions of the round ligament, hernia sacs, skin, and scars have been cited as regions of endometrial involvement in the groin. 9 It seems that bilateral endometriosis is rare, although two cases were reported in a 20-year-long survey in Japan. 3
The primary manifestation of inguinal endometriosis is the presence of a palpable mass in the groin, which can fluctuate in size and is often accompanied by severe dull pain with periodic exacerbation, that tends to intensify before or during menstruation. Although some individuals may not report pain, they may still experience catamenial symptoms. Pain associated with round ligament endometriosis can spread to the hip and is commonly associated with tenderness in the lower abdomen. Additional symptoms may include dysmenorrhea, lower abdominal pain, discomfort in the suprapubic region, and infertility.10 –12 In our case, the patient did not mention any development or alteration in the size of the groin, and there was no detectable mass during the physical examination. However, the patient exhibited slight tenderness upon deep palpation and reported experiencing intense, persistent pain in the right inguinal area during menstruation and catamenial symptoms. While the involvement of the intraperitoneal segment of the round ligaments typically does not lead to significant symptoms, the involvement of the extraperitoneal segment can result in similar manifestations, as observed in our case. 13
In 2022, Dalkalitsis et al. 10 conducted a systematic review and numerical analysis of all reported cases and retrospective studies of inguinal endometriosis worldwide. The results of this study showed that, on average, inguinal endometriosis is diagnosed for the first time at the age of 36, the majority of the patients initially present with a unilateral right-sided lump in the inguinal area, and more than half of them complain of periodic pain in this region. 10 A diagnostic hallmark is increasing menstrual pain and an increase in tumor size. Seventy-five percent of cases did not have a history of any gynecological or obstetric surgery, and 40% had a history of at least one operation. In the reported cases that we reviewed, patients were often multiparous. AlSinan et al. 14 reviewed case reports of inguinal endometriosis until 2021 and found only 30 nulliparous cases at the time of diagnosis. Inguinal endometriosis-affected patients are mainly referred to general surgeons and can be misdiagnosed with a wide variety of conditions in the inguinal area, such as inguinal hernia, hemangioma, lymphadenopathy, neuroma, lipoma, hematoma, cancers, and hydrocele of the canal of Nuck.15 –17 It is noteworthy that in 40% of cases, inguinal hernia coincides with endometriosis.18,19 In the present case, there was continuity with the right round ligament but no association with the inguinal hernia. Pelvic endometriosis may be present simultaneously with inguinal endometriosis, although the association has not yet been clarified. Candiani et al. 20 reported coexisting pelvic endometriosis in 91% of inguinal endometriosis patients and found pelvic endometriosis on laparoscopic investigation in all six patients whom they diagnosed with inguinal endometriosis.
Different diagnostic modalities, including abdominal ultrasound, transvaginal sonography, transrectal sonography, MRI, and CT, can be used to diagnose inguinal endometriosis; however, radiologic findings are not diagnostic when used alone. Ultrasound is mostly the first-line imaging method used to evaluate inguinal lesions, but sonographic presentations of endometriosis are quite variable and nonspecific, and the average tumor size ranges from 1 to 6 cm. 17 Despite these limitations, ultrasound is found to be helpful in identifying concomitant hernia sacs. 21 Sonographic findings of round ligament endometriosis show that it can have a solid or cystic structure or a combination of both. 22 The presence of a mass with variable size during the menstruation cycle improves diagnosis. 23 CT scan findings are also useful for excluding other pathological lesions since inguinal endometriosis features are inconclusive and difficult to differentiate from masses that share similar densities. 24 As severe endometriosis can mimic the symptoms of malignant tumors, such as a high level of CA125, and could also show a high uptake level of fluorodeoxyglucose in positron emission tomography scans, endometriosis masses may not be easily separated from soft tumors based on sonographic evaluation or CT scans. 25 MRI is the most specific and sensitive imaging modality to diagnose inguinal endometriosis, as it is able to detect iron in hemosiderin deposits in endometrioma. 12
In a 13-year study of 28 patients with inguinal endometriosis, they were divided into three types: a hernia sac or hydrocele of Nuck’s canal (type I), round ligament (type II), or subcutaneous area (type III), based on their location, and showed that the lack of preoperative diagnosis of type 1 was greater than the others. For this reason, complete resection of the hernia sac or hydrocele in the inguinal canal was recommended. 21 Sonography and roll-out of inguinal hernia is a first-tier diagnosis. In one study, the application of antibodies against estrogen and progesterone increased diagnostic accuracy. 22 MRI is useful as a second-tier diagnosis as well as a pre-surgery procedure. MRI can help in identifying the size and vastness of the tumor. MRI can also aid in complete and successful excision of the tumor, with a diagnostic accuracy of 91%–96%, based on cases. 23 Fine-needle aspiration cytology and pathological assessment are diagnostic for endometriosis and can be a huge help for proper diagnosis in selected cases.26,27
Treatment includes radical surgical excision, either laparotomic or laparoscopic. Hormone therapy after surgery is not necessary if there is no sign of pelvic endometriosis and the excision of the lesion is complete. There is no consensus among studies on the management of the disease. In most reported cases, surgery was performed in an open way (87%). 10 In a 1991 report, laparoscopy was used as a treatment for this disease. 20 In a 20-case evaluation in Japan, 6 of 20 patients underwent surgery as treatment, and in 4 of them, the laparoscopic method was used. 3 Since disease recurrence has been reported in some cases at different time intervals after the surgery, follow-up or at least the patient’s awareness of the symptoms is recommended. 10
Conclusion
Based on available reports obtained during the last 100 years, one can conclude that due to cyclic pain during reproductive age in women, paying attention to inguinal endometriosis is crucial, even without a history of gynecological surgery. It can be quite useful when the pain is on the right side of the body, with no physical sensing of the mass.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241257174 – Supplemental material for Laparoscopic surgery for endometriosis of the round ligament: A case of a patient with right-sided inguinal pain
Supplemental material, sj-docx-1-whe-10.1177_17455057241257174 for Laparoscopic surgery for endometriosis of the round ligament: A case of a patient with right-sided inguinal pain by Samaneh Rokhgireh, Abolfazl MehdizadehKashi, Shima Ghafourian Noroozi, Zahra Aminzade and Roya Derakhshan in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.