
Abstract
Background:
Menstrual health is an important indicator of overall health and has large impacts on quality of life. Despite number and impact, discussion of menstruation remains largely taboo within health care. Patients and physicians are not engaging in regular, meaningful discussions on menstruation. Family physicians, as primary care providers, can facilitate these important conversations.
Objectives:
We sought to understand the profile of menstrual care providing family physicians and assessed physician comfort, knowledge, training, and perceived importance regarding menstrual care.
Design/Methods:
This is a cross-sectional analysis of the 2022 Council of Academic Family Medicine Educational Research Alliance survey. The survey included actively practicing US physicians who are members of the Council of Academic Family Medicine organizations. Descriptive demographic statistics were calculated; chi-square tests were generated for menstrual care-specific items; logistic regression models were fit to determine the association between receiving formal menstrual care training, importance of physician training in menstrual care, and demographic factors.
Results:
Eighty-five percent of respondents report frequently providing menstrual care. Participants of younger age, or who had earned their degree more recently, were significantly more likely to provide frequent menstrual care. Respondents who earned their medical degree at an earlier year were significantly more likely to believe that physician training in menstrual care was of limited importance (OR = 1.02, 95% CI = 1.00, 1.03).
Conclusions:
Our findings show that family physicians are providing menstrual care, despite non-uniform training, and recognize its importance to patients. By understanding physician profile and the care they provide, we can work toward comprehensive physician education in menstrual care and providing appropriate menstrual care to patients.
Introduction
Three hundred million individuals menstruate daily worldwide, with 86 million of those being in the United States. 1 In addition to the sheer number of menstruators—cisgender women and girls, transgender people, and non-binary people—menstrual health is also an important indicator of overall health and impacts quality of life.2 –4 One national study found that 85% of menstruators reported dysmenorrhea, 77% reported psychological complaints, 71% reported tiredness, and 38% reported not being able to perform all their regular daily activities due to menstruation (from self-reported data). 5 Despite the quantity and impact, discussion of menstruation remains largely taboo, with menstruation viewed as “shameful, dirty, and something that shouldn’t be talked about,” subsequently leading to under discussion in health care settings. 6
Current guidelines from the American College of Obstetricians and Gynecologists (ACOG) 7 state that physicians should educate adolescents on what to expect with menstruation and continue to take an ongoing history during annual exam. This guidance should transcend gynecologic specialties, as menstruator’s first medical contact is often their primary provider, such as a family physician. Family physicians play a critical role in initiating discussion on menstruation and providing ongoing menstrual care. 8 However, the American Academy of Family Physicians does not have guidelines regarding menstrual health, despite recognizing that “identification of abnormal menstrual patterns in adolescence may improve early identification of potential health concerns for adulthood,” ultimately demonstrating the need for timely and comprehensive menstrual care. 7
Despite current guidelines and importance to patient health, many physicians do not feel comfortable nor engage in regular discussions with patients about menstrual health.9 –11 Lack of physician comfort can be attributed to universal stigmatization of periods and lack of physician training and knowledge in menstruation care.6,8 –10 This gap in care is nuanced by physician specialty and gender, with female physicians more likely to engage in longer, more emotionally adept communication regarding gynecological health compared to their male counterparts in primary care specialties, while the inverse is true for OB/GYN (obstetrics/gynecology) physicians. 11 Additional research has shown that while physicians may understand the biomedical process and needs of menstruating individuals, they may fall short of understanding the societal and cultural struggles their patients face.10,12
Data from other highly industrialized countries demonstrate many physicians, especially those in primary care, recognize the need to discuss menstrual health with their patients.13,14 This phenomenon has been under explored in the United States. Our primary objective was to understand the profile of menstrual care-providing family physicians. Secondarily, we assessed physician comfort, knowledge, training, and perceived importance regarding menstrual care. By understanding the profile of family physicians who provide menstrual care and the extent to which they do, we can better educate and train physicians and ultimately improve the quality of life for people who menstruate.
Methods
The CERA survey
Data were gathered and analyzed as part of the 2022 Council of Academic Family Medicine’s (CAFM) Educational Research Alliance (CERA) survey of practicing family physicians. CAFM is an initiative of four major academic family medicine organizations, including the Society of Teachers of Family Medicine, North American Primary Care Research Group, Association of Departments of Family Medicine, and Association of Family Medicine Residency Directors. CAFM invited members to propose survey questions for inclusion in the CERA survey. Approved projects were assigned a CERA Research Mentor to help refine questions. The project team worked with research mentors, the survey director, and the CERA steering committee to evaluate questions for consistency with the overall subproject aim, readability, and existing evidence of reliability and validity. Pretesting, conducted with family medicine educators who were not included in the sampling frame, evaluated questions for flow, timing, and readability. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational (cross-sectional) studies were utilized throughout the conceptualization of this study and the writing of this article. The American Academy of Family Physicians Institutional Review Board approved the study in December 2022.
Survey participants were members of one of the CAFM organizations. The pool excluded program directors, clerkship directors, and department chairs as these groups are surveyed separately. The survey contained qualifying questions to ensure that only practicing physicians and educators participated. Survey participants were sent a letter signed by the presidents of the four sponsoring organizations with a link to the survey via SurveyMonkey®. Non-respondents received four requests to complete the survey via SurveyMonkey. The final request was 2 days before survey closing.
The 2022 General Member Survey collected data on demographics, imposter phenomenon and discrimination, menstrual health topics, family medicine after Dobbs rulings, and food insecurity. The survey population included 5161 candidates. Of these, 210 were returned as undeliverable email addresses and 80 were excluded (previously opted out of receiving SurveyMonkey surveys). The survey was delivered to a final sample of 4871 members of CAFM organizations between January 11 and February 12, 2023. The survey was sent to all available qualifying members of the previously discussed CAFM organizations to maximize sample size and response rate. The overall response rate for the survey was 25.0% (n = 1216, 1216/4871). For this study on menstrual health, respondents were excluded if they were not clinically practicing physicians (n = 303), had not earned a Doctor of Medicine (MD) or Doctor of Osteopathic Medicine (DO) degree (n = 257), or had incomplete data for analysis variables (n = 476), yielding a final analytic sample of 739 physicians.
Measures
To better understand the profile of family physicians providing menstrual care, questionnaire items included measures of menstrual care frequency. Five menstrual care-specific items were included in our analysis to better understand the knowledge and clinical practices of menstrual care physicians in family medicine; these items assessed physician comfort and knowledge regarding menstrual frequency and flow; menstrual pain and associated symptoms; and probing questions about how menstruation impacts patient daily life; physician training in menstrual care, and importance of physician training in menstrual care. The full questionnaire is available as Supplemental material in Appendix 1.
Demographics and career characteristic measures also included in analyses were: gender, race, ethnicity, age, highest degree earned, year of highest degree earned, workplace geographic location, workplace community size, institution residency status, self-described professional role, practice setting, physician representation in medicine, workplace underserved status, and medical school affiliation.
Statistical analysis
For this cross-sectional study, STATA version 17.0 was used to complete the quantitative analyses self-reported data of menstrual care-providing family physicians. Descriptive statistics, sample size, and percentages for categorical variables, and mean and standard error for continuous variables were generated. Additional descriptive statistics, sample size, percentages, and chi-square tests were generated for menstrual care-specific items. Logistic regression models were fit to determine the crude association between receiving formal menstrual care training, importance of physician training in menstrual care, and various demographic factors. Measures of association and corresponding confidence intervals are reported for both crude and adjusted logistic regression models.
Results
Participant characteristics
Of the 739 clinically active physicians who responded, 62% self-identified as female, 74% White, with an average age of 47 years old (SE = 0.4). Average year of highest degree conferral was 2003 (SE = 0.4). Roughly, half of the respondents reported their community as urban, 56% work in a medical school setting, and 97% reported having some type of residency education. The most prevalent professional role was medical school or residency faculty (54%).
In total, 85% of respondents reported always or frequently providing menstrual care in clinical practice (n = 631). Participants whose self-assigned professional role was leadership, faculty, or practicing physician significantly more likely to have frequently provided menstrual care compared to those whose role was other. Participants of younger age were significantly more likely to provide frequent menstrual care compared to those who were of older age. Participants who earned their highest degree more recently were significantly more likely to provide frequent menstrual care compared to those who had earned their medical degree in an earlier year (Table 1).
Sample demographic characteristics (N = 739) based on frequency of providing menstrual care.
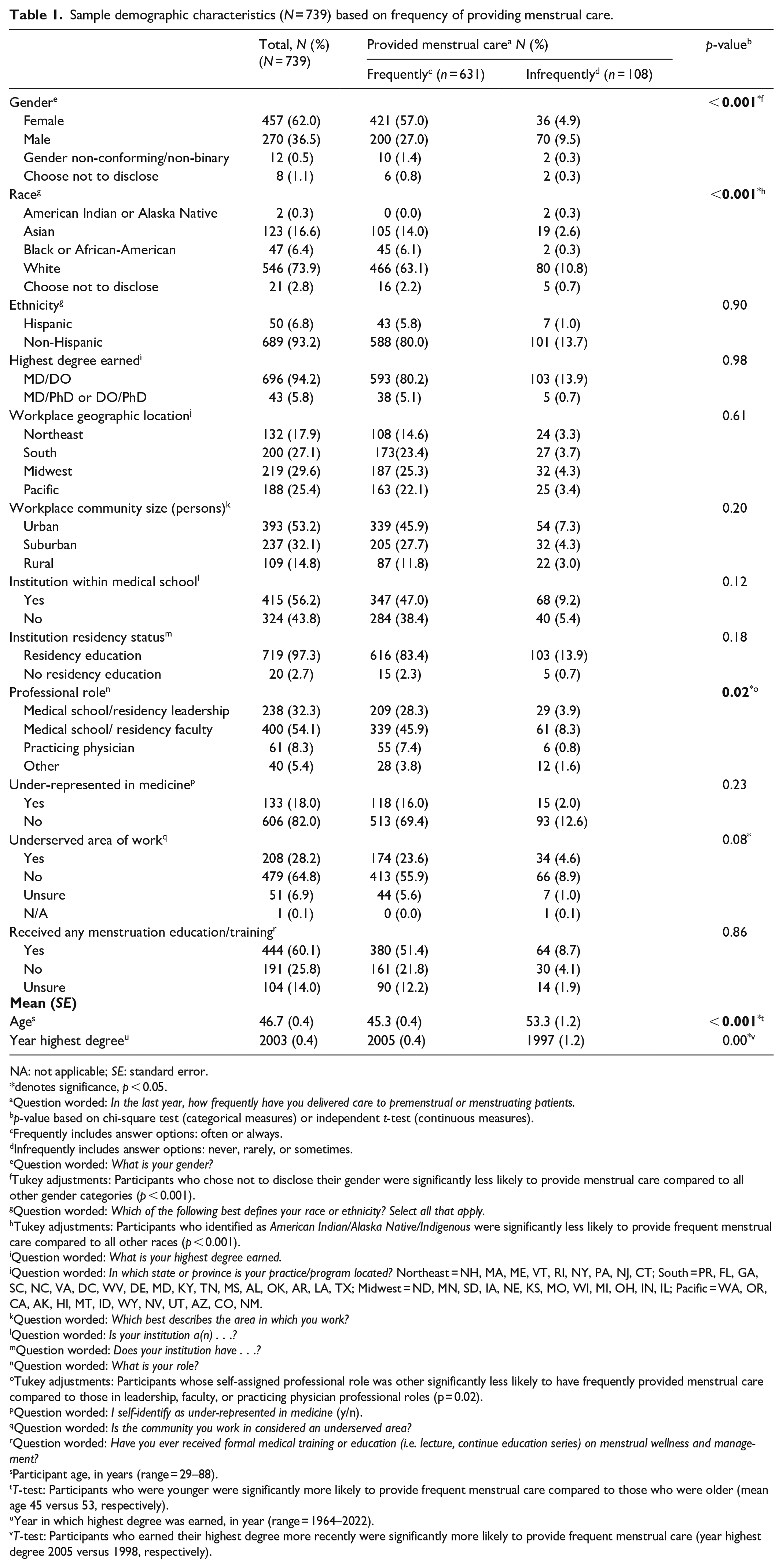
NA: not applicable; SE: standard error.
denotes significance, p < 0.05.
Question worded: In the last year, how frequently have you delivered care to premenstrual or menstruating patients.
p-value based on chi-square test (categorical measures) or independent t-test (continuous measures).
Frequently includes answer options: often or always.
Infrequently includes answer options: never, rarely, or sometimes.
Question worded: What is your gender?
Tukey adjustments: Participants who chose not to disclose their gender were significantly less likely to provide menstrual care compared to all other gender categories (p < 0.001).
Question worded: Which of the following best defines your race or ethnicity? Select all that apply.
Tukey adjustments: Participants who identified as American Indian/Alaska Native/Indigenous were significantly less likely to provide frequent menstrual care compared to all other races (p < 0.001).
Question worded: What is your highest degree earned.
Question worded: In which state or province is your practice/program located? Northeast = NH, MA, ME, VT, RI, NY, PA, NJ, CT; South = PR, FL, GA, SC, NC, VA, DC, WV, DE, MD, KY, TN, MS, AL, OK, AR, LA, TX; Midwest = ND, MN, SD, IA, NE, KS, MO, WI, MI, OH, IN, IL; Pacific = WA, OR, CA, AK, HI, MT, ID, WY, NV, UT, AZ, CO, NM.
Question worded: Which best describes the area in which you work?
Question worded: Is your institution a(n) . . .?
Question worded: Does your institution have . . .?
Question worded: What is your role?
Tukey adjustments: Participants whose self-assigned professional role was other significantly less likely to have frequently provided menstrual care compared to those in leadership, faculty, or practicing physician professional roles (p = 0.02).
Question worded: I self-identify as under-represented in medicine (y/n).
Question worded: Is the community you work in considered an underserved area?
Question worded: Have you ever received formal medical training or education (i.e. lecture, continue education series) on menstrual wellness and management?
Participant age, in years (range = 29–88).
T-test: Participants who were younger were significantly more likely to provide frequent menstrual care compared to those who were older (mean age 45 versus 53, respectively).
Year in which highest degree was earned, in year (range = 1964–2022).
T-test: Participants who earned their highest degree more recently were significantly more likely to provide frequent menstrual care (year highest degree 2005 versus 1998, respectively).
Menstrual care provision and training
Around 90% of respondents felt very comfortable discussing menstrual frequency and flow, menstrual pain and symptoms, and questions on impacts of daily life, regardless of how frequently they provided menstrual care. However, for all aspects of comfort discussing menstruation, respondents who were very comfortable were significantly more likely to frequently provide menstrual care (p < 0.001).
The percentage of respondents who felt very knowledgeable discussing menstrual frequency and flow, menstrual pain and symptoms, and questions on impacts of daily life were 81.6, 80.5, and 75.4%, respectively, regardless of how frequently they provided menstrual care. However, for all aspects of menstrual knowledge, respondents who were very knowledgeable were significantly more likely to frequently provide menstrual care (p < 0.001).
Regardless of frequency of menstrual care provision, 83.1% of respondents thought it was very important to discuss menstruation with patients, while 80% think physician education and training in menstrual care was very important. Respondents who thought patient education and physician training on menstruation was very important were significantly more likely to provide menstrual care (p < 0.001) (Table 2).
Family physician comfort, perceived knowledge, and perceived importance by frequency of menstrual care provision.
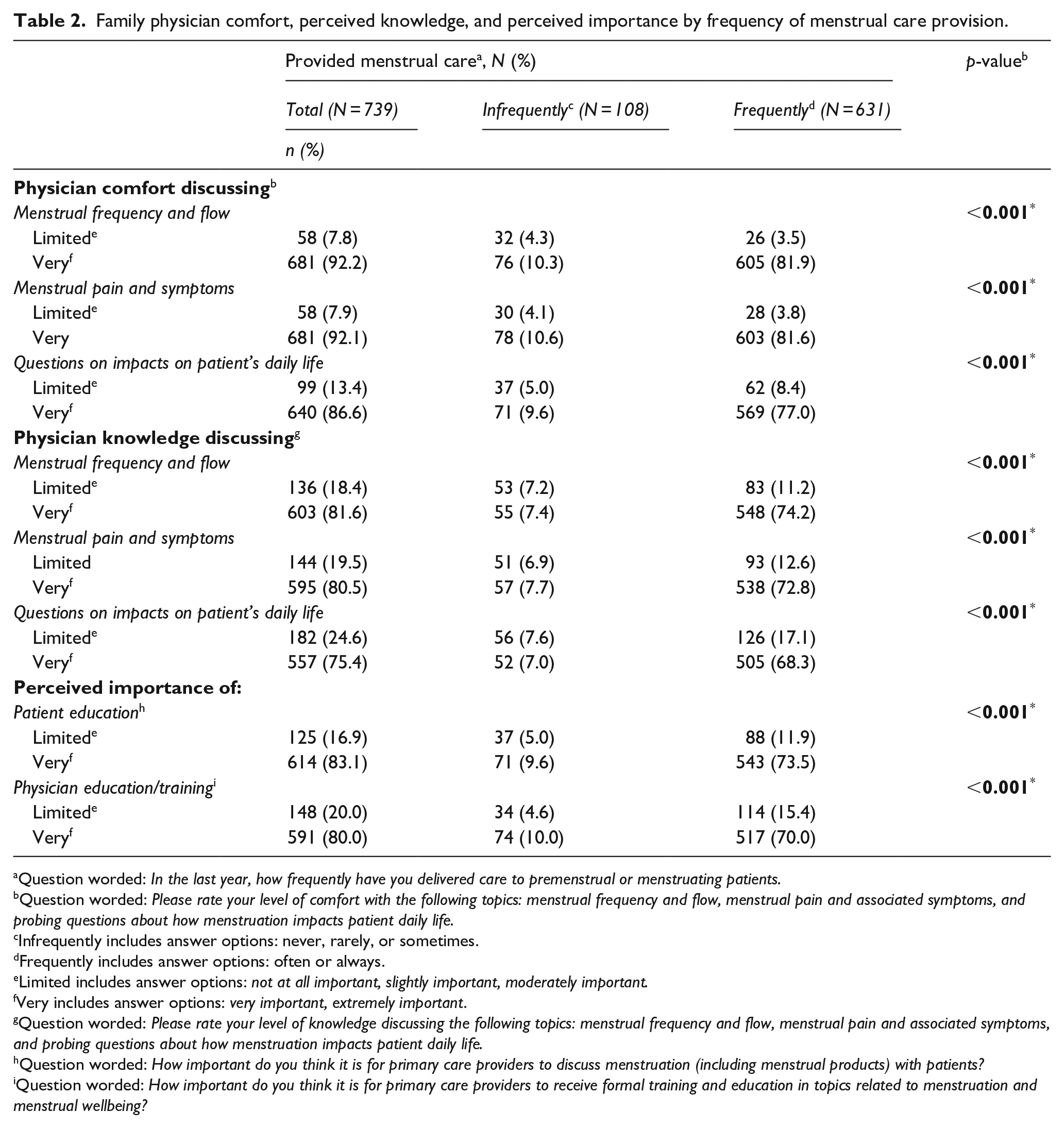
Question worded: In the last year, how frequently have you delivered care to premenstrual or menstruating patients.
Question worded: Please rate your level of comfort with the following topics: menstrual frequency and flow, menstrual pain and associated symptoms, and probing questions about how menstruation impacts patient daily life.
Infrequently includes answer options: never, rarely, or sometimes.
Frequently includes answer options: often or always.
Limited includes answer options: not at all important, slightly important, moderately important.
Very includes answer options: very important, extremely important.
Question worded: Please rate your level of knowledge discussing the following topics: menstrual frequency and flow, menstrual pain and associated symptoms, and probing questions about how menstruation impacts patient daily life.
Question worded: How important do you think it is for primary care providers to discuss menstruation (including menstrual products) with patients?
Question worded: How important do you think it is for primary care providers to receive formal training and education in topics related to menstruation and menstrual wellbeing?
Respondents who earned their medical degree at an earlier year were significantly more likely to believe that physician training in menstrual care was of limited importance (OR = 1.02, 95% CI = 1.00, 1.03) (Table 3).
Association between menstrual care training, importance of menstrual care training and selected demographic characteristics (N = 739).

OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
denotes significance, p < 0.05.
Confidence intervals that do not contain a value of 1 are indicated in bold and with *.
Question worded: Have you ever received formal medical training or education (i.e. lecture, continue education series) on menstrual wellness and management?
Question worded: How important do you think it is for primary care providers to receive formal training and education in topics related to menstruation and menstrual wellbeing?
Model adjusted for respondent gender.
Year in which highest degree was earned.
Question worded: Is your institution a(n) . . .?
Question worded: Does your institution have . . .?
Discussion
With over half the population experiencing menstruation at some point during their lives, menstrual health is an integral part of physical, mental, and emotional health. However, menstruation is still a widely taboo subject and many people, both patients and physicians, still do not discuss it even in a health care setting.6,13 When frequent menstrual care is provided, our findings show it was done so by female physicians practicing in urban Midwestern communities at institutions with residency programs and affiliated with medical schools. The vast majority of respondents, regardless of how frequently they provide menstrual care, were comfortable and knowledgeable about the different facets of menstruation, agreeing that both patients and physician education on menstruation is very important.
Despite the lack of formal guidelines regarding physician training in menstrual care across medical school, residency, or continuing medical education opportunities, our findings show promise that physicians are engaging patients in these conversations and recognize their importance.8,9,15,16 The more physicians deliver this care the more comfortable and knowledgeable they are on menstruation and menstrual issues.6,8 Our study demonstrates physicians are more comfortable than knowledgeable on this topic. This finding highlights the need and opportunity for medical education at all levels. Overall, physicians recognize the importance of engaging patients in menstrual education. Patient education often starts with a knowledgeable, comfortable physician.
Our findings also show that respondents who earned their degrees less recently were less likely to provide menstrual care, or view physician menstrual care education as very important. The field of menstrual care is a relatively recent phenomena, with few physician resources and scholarly investigations.12,13,16 The ongoing research and advocacy within this field encourages destigmatization, and increases physician comfortability and knowledge, fostering open communication on this topic with patients. Primary care physicians have the opportunity to facilitate factual, empathetic conversations that break the ongoing spiral of silence that menstruators have historically suffered under.6,8
This study utilized a well-established national survey of family physician educators across the United States and Canada in diverse practice and community settings. However, the survey was only sent to members of academic family medicine professional organizations, and does not encompass community physicians who do not participate in medical student or resident education. The survey yielded a 25.0% response rate, which is lower than the pre-pandemic average response rate to similar CERA General Membership Physician Surveys, and draws respondents who are largely faculty members. For this study, respondents needed to have earned a medical degree and be clinically active, limiting generalizability to family physicians practicing clinically. One of the most significant limitations of this study was that the survey captured self-reported data, limiting our ability to truly quantify outcomes. We also relied on the knowledge–attitude–behavior model, that is that knowledge influences attitude that drives changes in behavior; in the context of our conclusions, this model supports the idea that we must equip family physicians with appropriate knowledge and training to provide menstrual care to all patients who need it. 17 While appropriate for comfortability of menstrual care delivery and discussion, future work should seek to measure objective knowledge on menstruation and menstrual care, as this article is a preliminary investigation. There was also no set definition of what “providing menstrual care” meant and was up to the interpretation of the respondent. In addition, the survey design limited in-depth exploration of the type of menstrual care family physicians provided and feelings about their own menstrual care training and provision. Future works should seek to understand why certain groups of family physicians do not provide menstrual care or do not view it as important, and, for physicians that do provide frequent menstrual care, what areas of menstrual care training are the weakest. Additional exploration should focus on how to best meet these needs, with an emphasis on standardized curriculum spanning all levels of medical education as well as a renewed support of graduate medical education, with practices like ad hoc lectures, enhanced skills programs, grand rounds, and continuing education courses that adopt a holistic, life-span approach to menstrual health.
Conclusion
Menstrual health is an important part of a patient’s health and significantly impacts quality of life. Primary care physicians, including family physicians, are critical in menstrual care provision as they serve as first line for promoting good menstrual health. Family physicians can identify potential menstrual abnormalities, and serve as a gateway to more specialized care. Our findings show that family physicians are providing menstrual care and recognize its importance to their patients. Our study serves as a foundation for filling current literature gaps on who menstrual care physicians are and their knowledge and training on this topic. By understanding the profile of these physicians and the care they provide we can promote training that focuses on holistic care that recognizes that menstrual care transcends the siloed thinking of reproductive health, sexual health, or women’s health.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241247799 – Supplemental material for Family physicians and menstrual care: An analysis of CERA 2023
Supplemental material, sj-docx-1-whe-10.1177_17455057241247799 for Family physicians and menstrual care: An analysis of CERA 2023 by Allison R Casola, Olivia Rea and Tiffany Ho in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241247799 – Supplemental material for Family physicians and menstrual care: An analysis of CERA 2023
Supplemental material, sj-docx-2-whe-10.1177_17455057241247799 for Family physicians and menstrual care: An analysis of CERA 2023 by Allison R Casola, Olivia Rea and Tiffany Ho in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.