
Abstract
Background:
Given the estimated high rate of unintended pregnancies, it is important to investigate long-term effects on psychological distress in women carrying an unintended pregnancy to term. However, research into associations between unintended pregnancies carried to term and psychological distress postpartum is mixed, and especially, evidence on long-term associations is scarce.
Objective:
To examine whether carrying an unintended pregnancy to term is associated with maternal psychological distress later in life, up to 12 years postpartum.
Design:
This study is based on the population-based birth cohort study ‘Amsterdam Born Children and their Development’ study, which included pregnant people in 2003 (n = 7784) and followed them up until 12 years postpartum.
Methods:
Unintended pregnancy was measured as a multidimensional construct, based on self-reported data around 16 weeks gestation on pregnancy mistiming, unwantedness and unhappiness. Symptoms of maternal psychological distress were assessed around 3 months, 5 years and 12 years postpartum using multiple questionnaires measuring symptoms of depression, anxiety and stress. Multiple structural equation modelling models were analysed, examining the associations between dimensions of unintended pregnancy and maternal psychological distress per time point, while controlling for important co-occurring risks.
Results:
Pregnancy mistiming and unhappiness were significant predictors of more maternal psychological distress around 3 months postpartum. Around 5 years postpartum, only pregnancy mistiming was positively associated with maternal psychological distress. Dimensions of unintended pregnancy were no longer associated with maternal psychological distress around 12 years postpartum. Strikingly, antenatal psychological distress was a much stronger predictor of maternal psychological distress than pregnancy intention dimensions.
Conclusion:
Those who carried a more unintended pregnancy to term reported more symptoms of psychological distress at 3 months and 5 years postpartum. People carrying an unintended pregnancy to term may benefit from extra support, not because of the pregnancy intentions per se, but because they may be related to antenatal psychological distress.
Plain Language Summary
Carrying an unintended pregnancy to term and maternal psychological distress over time
Every unintended pregnancy is different, like every person is different. Nevertheless, carrying an unintended pregnancy to term might be stressful, that might impact mental health (e.g. depression or anxiety) of people carrying an unintended pregnancy to term. Research into long-term effects of carrying an unintended pregnancy to term on maternal mental health is scarce. In this study, we investigated effects of carrying an unintended pregnancy to term on maternal mental health up to 12 years postpartum. We used data from 7784 pregnant people living in Amsterdam, who participated in the Amsterdam Born Children and their Development (ABCD) study in 2003. Participants were followed up to 12 years postpartum. During pregnancy, participants answered questions about pregnancy mistiming (did the pregnancy happen at the right time), unwantedness (did they want to become pregnant) and unhappiness (how did they feel when they found out they were pregnant). We investigated these ‘dimensions’ of unintended pregnancy separately, to grasp to complexity of unintended pregnancy. Furthermore, participants answered multiple questions about experienced symptoms of depressions and anxiety around 3 months, 5 years and 12 years postpartum. People, who reported that their pregnancy was more mistimed, reported more mental health problems up to 5 years postpartum. Furthermore, people who reported more unhappiness with their pregnancy, reported more mental health problems around 3 months postpartum. People with an unintended pregnancy reported no longer more mental health problems around 12 years after birth, compared to people with more intended pregnancy. Strikingly, the mental health of people during pregnancy was more important for their mental health later in life, compared to their unintended pregnancy. Thus, the (emotional) circumstances around the pregnancy might be more influential for mental health later in life, compared to their pregnancy intentions. People carrying an unintended pregnancy to term may benefit from extra support, tailored to their individual needs and circumstances. Nevertheless, our results also showed that people are also resilient to deal with the many events and challenges faced during the periods after birth, since the effect of unintended pregnancy on maternal mental health disappeared over time.
Introduction
When someone finds out she is unexpectedly pregnant, she is not always on a pink cloud. It is estimated that 28% of Dutch pregnancies are unintended, around 53% of those are carried to term. 1 Given the estimated high rate of unintended pregnancies and its potential health impact on both women, their partners and children, it is important to investigate long-term psychological distress in women who carried an unintended pregnancy to term. Throughout this study, we will sometimes use the terms woman and women for practical reasons. This includes all persons with a uterus who do, or do not, identify as female.
Psychological effects of unintended pregnancy have been widely studied in women having abortions,2 –4 but very few studies focused on women who carried an unintended pregnancy to term. Available previous studies investigating short-term effects of unintended pregnancies that were carried to term on maternal mental health found mixed results.5,6 While some studies did find that carrying an unintended pregnancy to term was associated with a risk of maternal mental health problems,5,7 –9 others did not.10 –12 These mixed findings might first be explained by different categorizing approaches of unintended pregnancy in previous studies. Second, the context in which unintended pregnancies are carried to term may be very different in these studies. In some countries, women have fewer options to terminate the pregnancy than in others, which may lead to different results as well. Third, the use of different measures of mental health (depression, anxiety, mood disorders, and so on), different measurement moments and the different comparison groups that were used might also explain differences in results.
Research on the long-term risks for women who carried an unintended pregnancy to term is scarce. 13 Studies on associations between unintended pregnancies carried to term and maternal mental health over time have mostly been done in countries with less available abortion care, such as the United States.5,14,15 Women being denied an abortion reported higher anxiety symptoms and perceived distress compared with women who received an abortion, although the two groups converged over time.14,16 However, the situation might be different for women who have not been denied an abortion, but chose to carry the unintended pregnancy to term. This situation might be more prevalent in countries with fairly liberal abortion laws, such as the Netherlands,17,18 but remains unstudied up to now.
The question remains to what extent the decision of carrying an unintended pregnancy to term is a cause for mental health adversities, or whether there are other underlying mechanisms influencing both. While previous studies indicated that women with unintended pregnancies more often have lower SES, are younger and are unmarried than women with intended pregnancies,19 –21 these socioeconomic and demographic variables have been associated with a higher risk for psychological distress in the general population as well.22,23 Furthermore, women who have been sexually and/or physically abused have a higher risk for mental disorders, but also for having an abortion.24,25 Thus, in this study, we adequately controlled for these co-occurring risk factors in the analyses.
Pregnancy intentions are a complex construct with a lot of factors involved.26,27 Women might experience conflicting attitudes and emotions towards their pregnancy or fail to form explicit pregnancy intentions.28,29 Consequently, dichotomizing unintended pregnancy (being either intended or unintended) might lead to oversimplification. 28 Thus, in this study, we tried to grasp the complexity of unintended pregnancy by taking a multidimensional approach, based on the extent of pregnancy mistiming and unwantedness, and unhappiness with the pregnancy. These are in line with the key factors of pregnancy intentions pointed out by Santelli et al. 26
The aim of this study is to examine associations between unintended pregnancy and maternal psychological distress over a longer time span (up to 12 years postpartum), while taking co-occurring factors into account. This is investigated in a large-scale population-based birth cohort in an abortion liberal context (the Netherlands), while considering the complexity of pregnancy intentions by using a multidimensional approach towards the concept of unintended pregnancies.
Methods
Participants and procedure
This study is part of the ABCD study. 30 The broad aim of the ABCD study was to study the health and development of children, and their families born in Amsterdam, the Netherlands. For this ongoing population-based birth cohort study, 12,373 pregnant women living in Amsterdam between 2003–2004 were invited to participate during their first obstetric care visit. 30 Information about the study was given by an obstetric caregiver. Two weeks later (around 16 weeks gestation), all women subsequently received an informed consent form and the first questionnaire at their home address. 31 Women who wanted to participate signed the informed consent form filled out the questionnaire and send it back to the data collectors. Furthermore, at each subsequent data collection point, signed informed consent was obtained in the same manner.
Of the pregnant women approached, 8266 participated in the study (response rate 67%), with selection bias being reduced to a minimum. 32 Inclusion criteria were being pregnant currently and living in Amsterdam. Questionnaires were available in Dutch, Turkish, Arabic and English. 30 In the current study, women who gave birth to twins (n = 135) and/or children with major congenital diseases (n = 162) were excluded. Furthermore, only participants over 16 were included in the current sample. This resulted in a final sample size of 7784 pregnant women (Figure 1).

Structure of the Amsterdam Born Children and their Development study.
A post hoc statistical power analysis for testing a covariance structure model using RMSEA was conducted, 33 estimating power for a given RMSEA (null RMSEA = .05 and alternative RMSEA = .1), sample size (n = 7784) and an alpha of .05. Results indicated that the sample size was sufficient to answer our research questions considering the amount of parameters in the model (power >.9). 34
Data were anonymously derived from four measurement waves in this study: (1) antepartum (around 16 weeks gestation), (2) 13 weeks postpartum (during infancy), (3) 5–6 years postpartum (start of primary school) and (4) 11–12 years postpartum (past year of primary school) (Figure 1). All measurements consisted of posted, self-reported questionnaires that were filled out at home. In each questionnaire, it was clearly stated that data were processed confidential. Filling out confidential psychological health questions at home minimized social desirability bias. 35 For more detailed information on the study design, see Van Eijsden et al. 30 In this study, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies were followed.
Outcome measures
Due to over-time changes in the ABCD cohort study design, psychological distress was assessed with different instruments measuring symptoms of anxiety and depression. During the first and second measurements, the State-Trait Anxiety Inventory State form (STAI-S)36,37 and the Center for Epidemiological Studies Depression (CES-D)38,39 scale were used to measure anxiety and depression, respectively. During the third and fourth measurements, the Depression Anxiety Stress Scale (DASS-21)40,41 was used to measure depression and anxiety concurrently, because this instrument was less time consuming and its psychometric qualities were comparable. All three instruments have been demonstrated to be good predictors of clinical anxiety and depression, and the STAI and CES-D correlate moderately to strongly with the DASS-21 anxiety or depression subscales.42,43 Hence, it is assumed that the use of different instruments might not have influenced the estimation of symptoms of depression and anxiety in this study.
Maternal psychological distress around 3 months postpartum
Around 3 months postpartum, depressive symptoms were measured with the reliable and validated Dutch version of the CES-D,38,39 measuring the frequency of depressive symptoms experienced over the preceding week. In line with results of previous studies into the robustness and suitability of the CES-D, 44 depressive symptoms were modelled based on a 14-item three-factor structure: (1) negative affect, (2) anhedonia and (3) somatic symptoms. These are congruent with current diagnostic criteria for depression. 45 Items were rated on a 4-point Likert-type scale ranging from 0 (rarely or none of the time) to 3 (most of the time).
Furthermore, symptoms of state anxiety were assessed with the reliable and validated Dutch version of the 20-item STAI-S.36,37 The STAI-S measured experienced temporarily anxiety over the preceding week. Items were rated on a 4-point Likert-type scale ranging from 0 (rarely or none of the time) to 3 (most of the time). A latent factor ‘anxiety’ was modelled based on two second-order latent variables: (1) positive-state anxiety and (2) negative-state anxiety. This latent structure was substantiated by previous studies into the factorial structure of the STAI-S46,47 and further confirmed by the results from the confirmatory factor analysis in this study.
Maternal psychological distress around 5–6 years postpartum
Around 5–6 years postpartum, maternal psychological distress was measured with the reliable and validated Dutch version of the DASS-21. The DASS-21 measured the experience of symptoms of depression, anxiety and stress over the preceding week on a 4-point Likert-type scale ranging from 0 (never or rarely) to 3 (very often). Psychological distress was explained by three first-order latent variables, representing the three subscales of the DASS-21 (depression, anxiety and stress, 7 items per subscale). 41
Maternal psychological distress around 11–12 years postpartum
Around 11–12 years postpartum symptoms of psychological distress in the preceding week were measured using the DASS-21. Again, psychological distress was explained by three first-order latent factors, representing the subscales of the DASS-21 (depression, anxiety and stress, 7 items per subscale). 41
Predictor variables (antepartum, around 16 weeks gestation)
Pregnancy intentions
Pregnancy intentions were measured as a multidimensional construct, based on self-reported data on the extent of pregnancy mistiming, unwantedness and unhappiness. Dimensions of unintended pregnancy were measured with an item each: ‘I did not want to be pregnant (anymore)’ (unwantedness), ‘This pregnancy happened too soon’ (mistiming) and ‘I am happy to be pregnant’ (unhappiness; recoded). Items were rated on a 4-point Likert-type scale ranging from 0 (definitely not true) to 3 (very true), with a higher score indicating more unintendedness.
Co-occurring risks
Different co-occurring risks were taken into account. First, sociodemographic characteristics were obtained. Regarding maternal characteristics, we controlled for maternal age, ethnicity (being born in the Netherlands; yes/no), educational level (measured in years of educational attainment after primary school), having a paid job (yes/no) and being a single parent during pregnancy (yes/no). Furthermore, we controlled for the sex of the child (boy/girl) and the number of children already present in the family. Second, maternal experience with sexual and physical assault was assessed with two questions. Due to low prevalence, it was combined into one variable (experience with sexual and/or physical abuse, yes/no). Third, we controlled for maternal antepartum psychological distress psychological with the validated Dutch versions of the CES-D for depressive symptoms and the STAI-S for state anxiety.36,37 A total score was calculated for depression and anxiety each, with a higher score indicating more symptoms.
Statistical analyses
Sample characteristics were obtained for the co-occurring risk factors. Furthermore, correlations between variables of interest were obtained. To examine whether nonresponse was selective, women with missing data on one or more of the follow-up measurement phases were compared with women who completed all measurement waves.
Statistical analyses were performed in Rstudio. 48 Missing data were handled using Full Information Maximum Likelihood (FIML) estimation in RStudio, providing more reliable results compared with list-wise deletion 49 and similar results to other multiple imputation methods. 50 The p values less than 0.05 were considered statistically significant.
Associations between unintended pregnancy and psychological distress were investigated using Structural Equation Modelling (SEM) with the lavaan package. 51 In a SEM path model, each estimated standardized regression coefficient can be used to interpret the unique variance of each predictor, while controlling for the effects of the other predictors. 52 Models were considered to have a good fit when the Root Mean Square Error of Approximation (RMSEA) was smaller than .05, and adequate fit when the Comparative Fit Index (CFI) was larger than .90.53 –56 To account for the non-normality in the data, maximum likelihood with robust standard errors (MLR) was used. 57
A path model was estimated per timespan ((1) 3 months postpartum, (2) 5–6 years postpartum and (3) 11–12 years postpartum). In the model estimating the effects on psychological distress around 3 months postpartum, a model was estimated for state anxiety and depressive symptoms separately, since they were derived from different inventories and hence items overlapped too much to estimate a single model for both latent constructs. In line with recommendations from previous studies, state anxiety was modelled as a latent construct explained by a positive and negative factor. 47 Furthermore, depression was modelled as a latent construct explained by three factors (anhedonia, negative affect and somatic symptoms). 44 In the models estimating the effects around 5–6 years and 11–12 years postpartum, one model was estimated for psychological distress in total, explained by three factors (depression, anxiety and distress) in line with previous studies. 41 In each model, the dimensions of unintended pregnancy were added as separate exogenous variables: (1) mistiming, (2) unwantedness and (3) unhappiness with the pregnancy. Furthermore, we controlled for maternal antepartum depression and anxiety, experience with abuse and sociodemographic variables by adding them as predictors in each model (Figure 2).
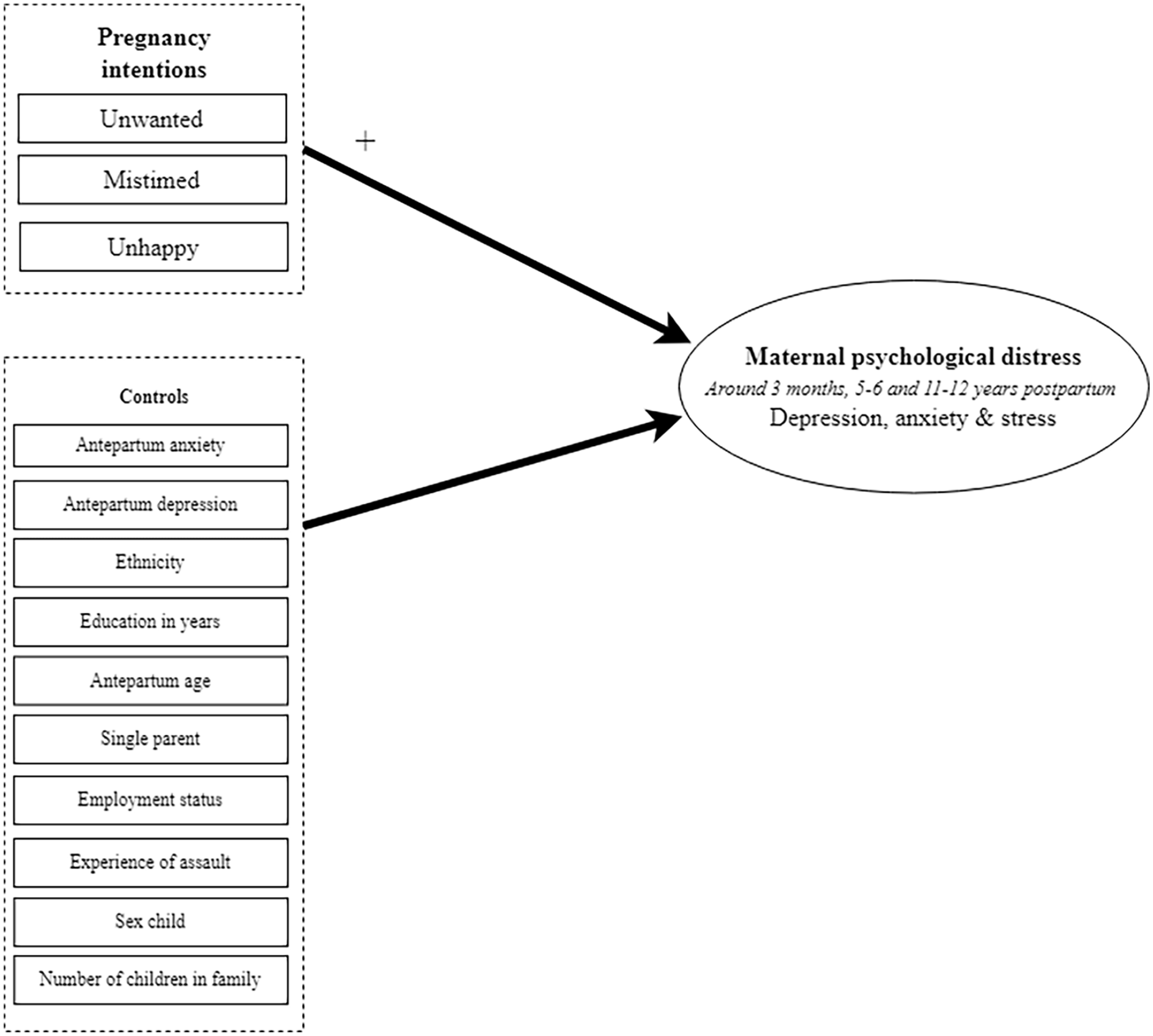
Research model.
Nonresponse analyses
Participants who were lost to follow-up (40.0% dropped out after phase 1, 59.0% after phase 2% and 69.8% after phase 3) were compared with those who responded to each measurement (n = 2035). Compared with responders, dropouts were younger and more likely to be a single parent, and unemployed. Furthermore, they more often had a migrant background and less years of education (Table 1).
Characteristics of responders and nonresponders (antepartum, around 16 weeks gestation).
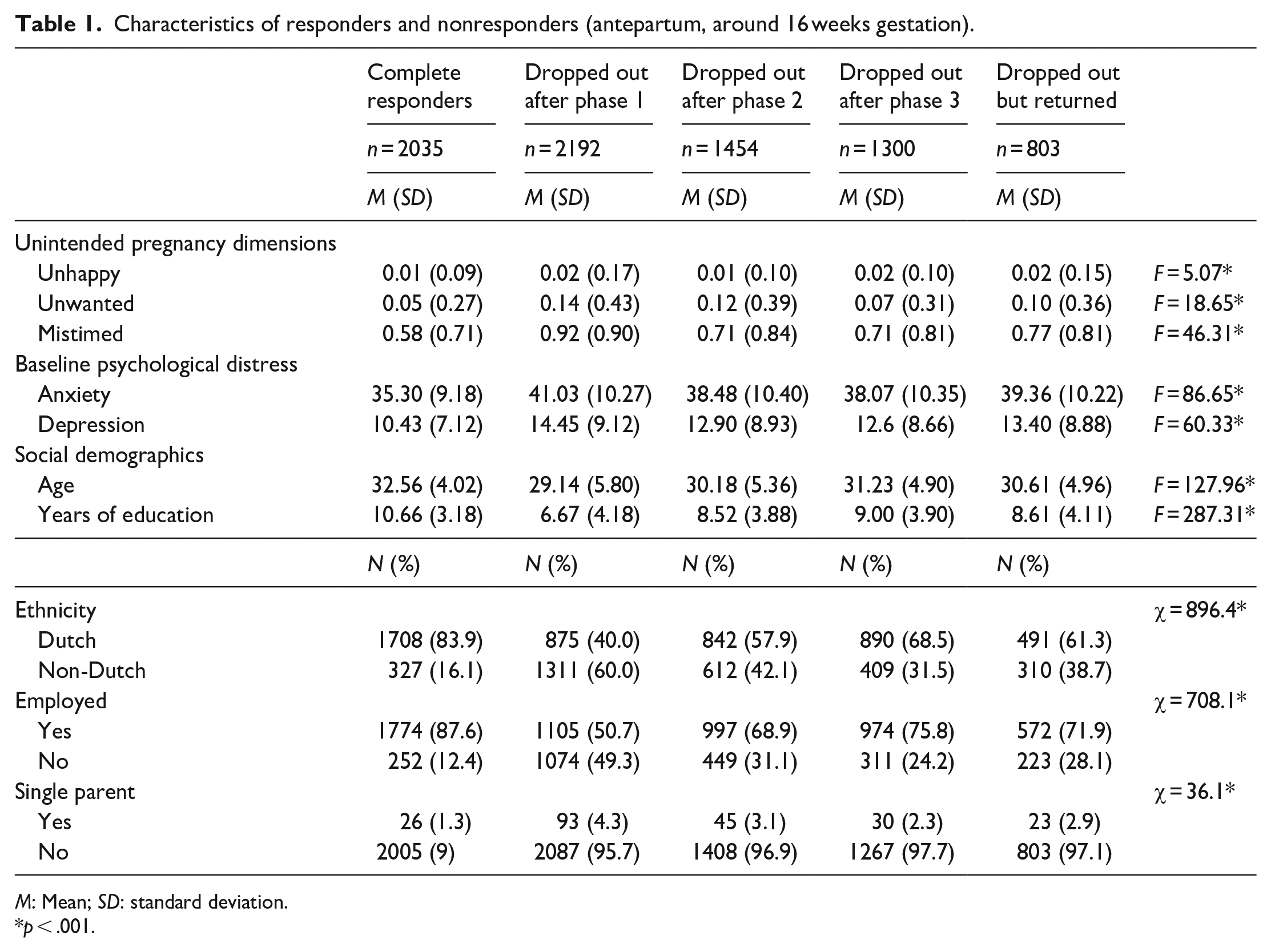
M: Mean; SD: standard deviation.
p < .001.
Results
Descriptive analyses
Participants were between 16–46 years during the first measurement (antepartum). Most participants indicated that their pregnancy was much wanted but a bit mistimed, and that they were very happy with their pregnancy. Other participant characteristics are described in Table 2.
Participant characteristics.

M: mean; SD: standard deviation; STAI: State-Trait Anxiety Inventory; CES-D: Center for Epidemiological Studies Depression.
Assault was assessed as experience with sexual and/or physical assault during pregnancy.
Dimensions of unintended pregnancy were measured on a 4-point Likert scale (0–3), with a higher score indicating more unintendedness.
With regard to correlations between our variables of interest, results indicated that on average, women who received less years of education were younger, not Dutch-born, did not have a job or were a single parent reported more pregnancy mistiming and unwantedness. However, no differences were found in happiness with the pregnancy. Furthermore, maternal psychological distress at baseline (both depression and anxiety) were positively correlated to the dimensions of unintended pregnancy, indicating that women experiencing more psychological distress antepartum also report more unintended pregnancies (Table 3).
Bivariate correlations between variables of interest.

STAI: State-Trait Anxiety Inventory; CES-D: Center for Epidemiological Studies Depression; DASS: Depression Anxiety Stress Scale.
Total scores of the STAI.
Total scores of the CES-D.
Assault was assessed as experience with sexual and/or physical assault during pregnancy.
Total scores of the DASS-21.
p < .01; **p < .001.
Over-time associations between unintended pregnancy and maternal psychological distress
Maternal psychological distress around 3 months postpartum
With regard to results on psychological distress around 3 months postpartum, the hypothesized anxiety path model showed an adequate fit, RMSEA = .043 and CFI = .902. While controlling for antepartum background variables, baseline psychological distress and other dimensions of unintended pregnancy, pregnancy mistiming and unhappiness were significant predictors of maternal anxiety levels around 3 months postpartum (β = .03, p = .050; β = .04, p = .007, respectively). Effect sizes are small 58 due to the large number of predictors in the model. In contrast, pregnancy unwantedness did not significantly predict anxiety levels around 3 months postpartum (Table 4). Furthermore, antepartum symptoms of depression and anxiety were the strongest predictors of symptoms of anxiety around 3 months postpartum (β = .08, p = .013; β = .50, p < .001, respectively), indicating a, respectively, small and large effect size. 58
Structural equation modelling regression results of the associations between predictor variables and maternal psychological distress around 3 months postpartum.

SE: standard error; CI: confidence interval.
Depression was measured with the CES-D.
Anxiety was measured with the STAI-S.
Furthermore, the hypothesized depression path model was well-fitted, RMSEA = .032 and CFI = .928. In line with results from the anxiety model, pregnancy mistiming and unhappiness were significant predictors of maternal depression levels around 3 months postpartum (β = .04, p = .031; β = .05, p = .006, respectively), while controlling for antepartum background variables and other dimensions of unintended pregnancy. Effect sizes are small. 58 Pregnancy unwantedness did not significantly predict depression levels around 3 months postpartum (Table 4). Furthermore, antepartum symptoms of depression and anxiety were the strongest predictors of symptoms of depression around 3 months postpartum (β = .37, p < .001; β = .19, p < .001, respectively), indicating a, respectively, medium and small effect size. 58
Maternal psychological distress around 5–6 years postpartum
The hypothesized path model estimating associations between pregnancy intentions and psychological distress levels around 5–6 years postpartum showed a good fit, RMSEA = .026 and CFI = .921. While controlling for all other variables in the model, pregnancy mistiming was a significant predictor of maternal psychological distress levels around 5–6 years postpartum (β = .05, p = .040). However, pregnancy unwantedness and unhappiness did not significantly predict psychological distress levels around 5–6 years postpartum (Table 5). Furthermore, antepartum symptoms of depression and anxiety were the strongest predictors of symptoms of psychological distress around 5–6 years postpartum (β = .26, p < .001; β = .14, p = .001, respectively), although these effect sizes are small. 58
Structural equation modelling regression results of the associations between predictor variables and psychological distress around 5–6 years postpartum.

SE: standard error; CI: confidence interval.
Depression was measured with the CES-D.
Anxiety was measured with the STAI-S.
Maternal psychological distress around 11–12 years postpartum
The hypothesized path model estimating associations between pregnancy intentions and psychological distress levels around 11–12 years postpartum showed a good fit, RMSEA = .019 and CFI = .933. Results indicated that while controlling for all other variables in the model, the three dimensions of unintended pregnancy were no significant predictors of maternal psychological distress levels around 11–12 years postpartum (Table 6). Again, antepartum symptoms of depression and anxiety were the strongest predictors of psychological distress around 11–12 years postpartum (β = .28, p < .001; β = .15, p = .003, respectively), indicating small effect sizes. 58
Structural equation modelling regression results of the associations between predictor variables and psychological distress around 11–12 years postpartum.

SE: standard error; CI: confidence interval.
Depression was measured with the CES-D.
Anxiety was measured with the STAI-S.
Discussion
Results of this study show that women carrying a more unintended pregnancy to term experience more symptoms of maternal psychological distress (depression, anxiety and stress) at 3 months and 5 years postpartum. However, unintended pregnancy was no longer associated with symptoms of maternal psychological distress around 12 years postpartum. Strikingly, antenatal psychological distress was a much stronger predictor of maternal psychological distress over time compared to unintended pregnancy.
This study investigated unintended pregnancy as a multidimensional construct (based on self-reported extents of pregnancy mistiming, unwantedness and unhappiness), taking its complexity into account. These dimensions are in line with the work by Santelli et al. 26 Results of this study indicated that pregnancy mistiming was among the other dimensions of unintended pregnancy the strongest predictor of maternal psychological distress over time.
Consistent with results of previous studies,12,59 –61 current results show that women who carried a more mistimed pregnancy to term reported more symptoms of psychological distress around 3 months and 5 years postpartum, but no longer 12 years postpartum. Although previous research into long-term effects of carrying a mistimed pregnancy to term is scarce, some studies also found that women reported diminishing levels of depression and anxiety in the first years postpartum. 62 Moreover, previous studies into women who had access to and underwent abortions, versus women who were denied abortions, found differences in perceived distress levels soon after being denied abortions; however, those differences were no longer present on the longer term. 16 This might explain the absence of an association between carrying a more mistimed pregnancy to term and maternal psychological distress around 12 years postpartum in this study as well. In this way, results of our study show that although women’s experiences of carrying a more mistimed pregnancy to term can have influence on maternal psychological distress over time, those women are also resilient to deal with the many events and challenges faced during these periods.
In contrast to what was found in previous studies,5,14 pregnancy unwantedness was not associated with maternal psychological distress at any point measured later in life. Several reasons might explain this contradiction in research findings. First, previous studies into long-term effects of carrying a (highly) unwanted pregnancy to term were mostly done in populations in which women were not legally allowed to have an abortion, or were denied one. However, in this study’s context women who carried a strongly unwanted pregnancy may have chosen to terminate the pregnancy due to the more liberal abortion context, 63 and, therefore, not be part of the sample. Second, since participants reported on their pregnancy intentions while they were already pregnant, deliberately choosing to carry an unwanted pregnancy to term might positively influence the perception of the degree of unwantedness (i.e. reporting a pregnancy as more wanted compared with before the pregnancy). 64 Third, social desirability might have also lead to an underestimation of pregnancy unwantedness.64 –66 Fourth, finding an effect of pregnancy mistiming but not of unwantedness might be explained by the statistical approach of this study, since different dimensions of pregnancy intentions were added to the same statistical models. Thus, although pregnancy mistiming is the strongest predictor of symptoms of postpartum psychological distress, this might also reflect part of the effect of carrying a more unwanted pregnancy to term, since pregnancy mistiming and unwantedness were also highly correlated.
In line with results of previous studies, 60 results of this study indicated that women who were more unhappy with their pregnancy experienced more symptoms of anxiety and depression around 3 months postpartum. Previous studies concluded that women reporting more pregnancy unhappiness felt that the costs of another baby did not weigh against other competing personal commitments or aspirations, 29 or felt they were not prepared for maternity. 67 This might explain the association between pregnancy unhappiness and short-term maternal psychological distress. Results of this study further indicate that this association disappears over time, since pregnancy unhappiness was no longer associated with maternal psychological distress from around 5 years postpartum. Emotions regarding a pregnancy might be less stable over time (for instance, due to other life circumstances that come along), explaining the disappearance of the effect around 5 years postpartum.
Another important result of this study is that the strongest and most consistent predictors of maternal psychological distress over time were antepartum symptoms of psychological distress. This suggests that mental health during pregnancy is an important influence on maternal health later in life, which is in line with previous studies. 68 Hence, in line with recent recommendations from other researchers in the field, 69 current results imply that the circumstances around the pregnancy might be more important than the actual amount of pregnancy intendedness to explain maternal psychological distress later in life.
We acknowledge several limitations of this study. First, we cannot eliminate the risk that selection bias in participants who dropped out our cohort data affected our results. Cohort studies are prone to selective dropout and hence are likely to underestimate prevalence of mental health problems. 70 In this study, dropouts were younger and more likely to be a single parent and unemployed, compared with responders. Furthermore, they more often had a migration background and fewer years of education. Since these are all risk factors for psychological distress as well,22,23 it was assumed that dropouts could have possibly reported higher levels of psychological distress. Moreover, dropouts reported more unintended pregnancies and more antepartum psychological distress compared with responders. Consequently, the dropout rate might have led to an underestimation of the associations between unintended pregnancy and maternal psychological distress, 71 and possibly the disappearance of the association between aspects of unintended pregnancy and psychological distress around 12 years postpartum. Second, we were not able to control for a history of psychological distress, which has repeatedly been found to be an important predictor of psychological distress among women who have had an abortion2 –4 and parental (postpartum) depression. 72 However, in this study, we controlled for psychological distress at baseline (antepartum), which might be a good proxy for mental health history due to a high consistency in reports of psychological distress over time. 73 Third, although pregnancy intentions were measured as a multidimensional construct in line with the work by Santelli et al. 26 some information was missing in the current cohort data. Contraceptive use might be an important dimension of pregnancy intentions, since people who (consistently) use contraceptives have higher intentions to avoid a pregnancy. 74 Furthermore, the intentions of the partner involved in the pregnancy might be another important dimension of pregnancy intentions 28 that also might have an influence on maternal psychological distress over time.75,76 Thus, future studies are advised to incorporate both the partner’s pregnancy intentions and contraceptive use when considering pregnancy intentions.
Despite these limitations, this study was the first to investigate long-term associations between dimensions of unintended pregnancy carried to term and symptoms of maternal psychological distress in an abortion liberal context. Our findings were derived from a large-scale and multi-ethnic prospective birth cohort, providing results that might be translatable to the Dutch population, and other countries with a similar abortion climate. Furthermore, in line with recommendations from previous studies, 6 the design of this study made it possible to consider the complexity of pregnancy intentions, by taking into account different dimensions of unintended pregnancy and providing meaningful insights in different associations on maternal psychological distress. Moreover, associations were investigated while taking into account other important co-occurring risks, like socioeconomic factors (maternal age, education, relationship status, having a job and ethnicity), antepartum psychological distress and experiences with assault. Thus, reported associations are present despite other important influencers of symptoms of maternal psychological distress over time.
Conclusion
Our study showed that pregnancy intentions and psychological distress were associated. The more unintended a pregnancy was, the higher the levels of psychological distress around 3 months and 5 years postpartum, but no longer at 12 years follow-up. Strikingly, results also showed the importance of antepartum psychological distress when explaining levels of maternal psychological distress later in life. These results implicate that women with more symptoms of antenatal psychological distress may benefit from extra support. Unintended pregnancy is a complex personal experience with a lot of other factors involved. This study, but also other studies 6 show the importance of considering co-occurring risks when looking at psychological distress in relation to unintended pregnancy. Psychological distress may contribute to the unintendedness of a pregnancy, rather than the other way around. Future studies should explore ways to (better) support these women tailored to their individual needs, focusing on protective factors decreasing the risk on psychological distress.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231213737 – Supplemental material for Carrying an unintended pregnancy to term and long-term maternal psychological distress: Findings from the Dutch prospective Amsterdam Born Children and their Development study
Supplemental material, sj-docx-1-whe-10.1177_17455057231213737 for Carrying an unintended pregnancy to term and long-term maternal psychological distress: Findings from the Dutch prospective Amsterdam Born Children and their Development study by Wieke Y Beumer, Tessa J Roseboom, Marjette H Koot, Tanja Vrijkotte and Jenneke van Ditzhuijzen in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231213737 – Supplemental material for Carrying an unintended pregnancy to term and long-term maternal psychological distress: Findings from the Dutch prospective Amsterdam Born Children and their Development study
Supplemental material, sj-docx-2-whe-10.1177_17455057231213737 for Carrying an unintended pregnancy to term and long-term maternal psychological distress: Findings from the Dutch prospective Amsterdam Born Children and their Development study by Wieke Y Beumer, Tessa J Roseboom, Marjette H Koot, Tanja Vrijkotte and Jenneke van Ditzhuijzen in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.