
Abstract
Maternal mortality is disproportionately higher in low- and middle-income countries compared to other parts of the world. International research efforts are reflective of the urgency to improve global maternal outcomes. The existing literature of maternal health interventions in low- and middle-income countries targets a variety of populations and intervention types. However, there is a notable lack of systemic reviews that examine the wider contextual and mechanistic factors that have contributed to the outcomes produced by interventions. This article aims to use realist synthesis design to identify and examine the relationships between the contexts, mechanisms and outcomes of maternal health interventions conducted in low- and middle-income countries. This will inform evidence-based practice for future maternal health interventions. In May 2022, we searched four electronic databases for systematic reviews of maternal health interventions in low- and middle-income countries published in the last 5 years. We used open and axial coding of contexts, mechanisms and outcomes to develop an explanatory framework for intervention effectiveness. After eligibility screening and full-text analysis, 44 papers were included. The majority of effective interventions reported good healthcare system contexts, especially the importance of infrastructural capacity to implement and sustain the intervention. Most intervention designs used increasing knowledge and awareness at an individual and healthcare-provider level to produce intended outcomes. The majority of outcomes reported related to uptake of healthcare services by women. All mechanism themes had a relationship with this outcome. Health system infrastructure must be considered in interventions to ensure effective implementation and sustainability. Healthcare-seeking behaviours are embedded within social and cultural norms, environmental conditions, family influences and provider attitudes. Therefore, effective engagement with communities and families is important to create new norms surrounding pregnancy and delivery. Future research should explore community mobilization and involvement to enable tailored interventions with optimal contextual fit.
Keywords
Introduction
The burden of maternal mortality is disproportionately represented in the world’s low- and middle-income countries (LMICs). 1 Sub-Saharan Africa and South Asia accounted for 86% of the global 130,000 maternal deaths that occurred in 2017. 1 The World Health Organization (WHO) reported that maternal mortality rate (MMR) in LMICs in 2017 was 415 per 100,000 live births; 40 times higher than the MMR in Europe. 1
The Sustainable Development Goals (SDGs) proposed by the United Nations aim to reduce global MMR to less than 70 per 100,000 live births. 2 However, at our current pace of progress, this goal will not be reached by 2030, at the detriment of 1 million lives of pregnant women and mothers. 1 The majority of maternal deaths in LMICs are caused by haemorrhage, infection, unsafe abortion, hypertensive disorders or obstructed labour. 3 Insufficient service provision, higher prevalence of infectious diseases and higher total fertility rate increase the risk of complications for pregnant women in LMICs. 3
Provision of maternal healthcare can be measured through the coverage of interventions for women during and after pregnancy. WHO recommends that women should receive at least eight antenatal care (ANC) contacts to reduce the risk of perinatal mortality and improve the pregnancy experience. 4 However, in 2017, only half of women worldwide received the recommended antenatal and postnatal visits. 5 Lack of access to services is exacerbated by various factors including poverty, poor access to resources, gender inequality and illiteracy. 3 These factors not only influence variations in MMR across countries but also across socioeconomic groups. 5 Therefore, policy and programme makers aiming to increase coverage and improve maternal health must consider these socioeconomic and health system factors in their intervention design and implementation. 3
There are numerous systematic reviews and observational studies that determine the effectiveness of specific interventions. For example, Nyamtema et al.’s 6 systematic review explored the barriers to intervention implementation. These barriers were categorized into leadership and management, (lack of) resources and end-user-related factors. 6 Another systematic review and network meta-analysis of maternal care reported effectiveness in intervention domains of nutrition and hygiene. 7 Specific types of interventions have also been extensively researched, such as maternal mobile health (mHealth) applications, psychosocial interventions and perinatal home visits.8 –10 Global maternal research efforts are reflective of the urgency of improving maternal care in LMIC.
Kabongo et al. 11 used realist approach to explain the impact of mHealth interventions in LMICs. Their research showed that psychosocial mechanisms improved uptake of maternal care, and positive mechanisms were influenced by sociocultural, economic and network infrastructure contexts. Mwije and Holvoet 12 used realist synthesis to examine interventions to improve male involvement in maternal care. However, their research, while insightful of the mechanisms that motivated fathers to participate in maternal care, was limited to studies only in Uganda. While realist synthesis of maternal health interventions is available within the existing literature, it is limited to specific intervention types and regions. There is a distinct lack of realist synthesis of literature that examines the overarching themes of contexts, mechanisms and outcomes (CMOs) of a variety of maternal health interventions in LMICs.
This review aims to address this evidence gap using realist synthesis in an overview of reviews (also known as a ‘systematic review of reviews’) to identify and examine the relationship between CMOs of maternal health interventions that have been conducted in LMICs. We focused on existing systematic reviews given the breadth of the interventions of interest and because this is an extensively reviewed field. Realist synthesis is rooted in realist theory where interventions are recognized as theories that have been implemented on a particular hypothesis of cause and effect. The realist approach uses contexts and mechanisms to better understand the theoretical and practical conditions in which an intervention was or was not successful.13,14 Contexts are defined as any set of factors that are capable of influencing the delivery of an intervention or the mechanisms by which an intervention produces an outcome. 15 Contextual factors vary in scope and can include factors relevant to attitudes and actions of key stakeholders or broader socioeconomic, cultural and political factors. 16 The realist concept of mechanism is the particular processes or structures that operate in specific contexts that generate outcomes. 14 The outcomes included in realist synthesis not only include the desired outcomes reported by the intervention authors but also reported outcomes that were unintended but occurred due to the contexts and mechanism of the intervention. 14
Realist review methods aim to steer away from inferences of successionist models of causation and instead explain what causal mechanisms occurred in what contexts and how they produced the specified outcomes. 17 Therefore, creating an evidence base for policy and programme makers on why and how future interventions may work under different contexts, and what further resources may be required to generate the right mechanisms to produce the desired health outcomes.13,14
Methods
We conducted and reported this study using the Realist and Meta-narrative Evidence Synthesis: Evolving Standards (RAMESES) guidelines. 14
Search, selection and appraisal
We included (a) systematic reviews (defined as evidence synthesis drawing on systematic search and selection of a specific body of evidence) (b) of maternal health interventions in LMICs (c) that included assessment of outcomes for pregnant women or mothers and (d) that were published in the English language. The Organization for Economic Cooperation and Development (OECD) list of LMICs was used to identify the appropriate reviews. 18 Because systematic reviews can go out of date, we restricted inclusion to reviews published since 2017. We excluded reviews of interventions conducted in high-income countries, or that did not reflect a robust search for the evidence.
We undertook an electronic search based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines on 2 May 2022. Search terms are reported in Supplementary file 1. The electronic databases searched included Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica Database (Embase), WHO (Maternal, Newborn, Child and Adolescent Health and Ageing Portal) and Latin American and Caribbean Health Sciences Literature (LILACS).
After deduplication of search results, we screened records for relevance and then retrieved full texts to produce a final set of included papers. This was undertaken by one reviewer with audit and checked by a second reviewer.
We critically appraised included studies using the Critical Appraisal Skills Programme (CASP) checklist for systematic reviews, see Supplementary file 2. 19
Coding of CMOs
After identification of relevant studies, we undertook a realist synthesis. A grounded theory approach underpinned the process of CMO configuration. 20
The first step, open coding, involved inductive classification of the interventions reported within the included papers into discrete categories. Initially, the Effective Practice and Organization of Care (EPOC) taxonomy of health system interventions was used to classify the domains of interventions. 21 However, this was found to be too broad for contextual analysis. Consequently, we inductively derived intervention categories that better reflected similarities and differences between interventions. Within each category, we analysed relevant reviews to retroduct the appropriate CMOs. Some reviews overlapped in categories of interventions, in which case reviews were ‘double-counted’. Primary studies included within reviews were also occasionally examined when reviews lacked discussion of contexts and mechanisms. Pawson et al.’s 22 definition of the four contextual layers (individual, interpersonal relations, institution and infrastructure) influenced the levels into which retrieved contexts and mechanisms were organized. Mechanisms were categorized into levels at which they occurred: intervention, individual, healthcare provider and social. Finally, we used axial coding and dimensionalization to draw connections between review-level open codes and to create higher-order, analytically generalizable CMOs.
Results
Results of the search
The search initially yielded 2287 records. After deduplication and eligibility screening, 44 papers were included for the study (see Figure 1) which included 947 relevant primary studies.23 –66 Details and characteristics of all the included studies are described in Supplementary file 2 (Table 1). Reviews included a wide range of interventions targeted to improve maternal care and health across LMICs. The complexity of maternal care interventions was reflected in the characteristics of included studies as many reviewed interventions covered multiple EPOC domains. The most prevalent domain reviewed was delivery arrangements (n = 29), followed by implementation strategies (n = 10), financial arrangements (n = 7) and finally governance arrangements (n = 1).

Flowchart of search results.
Critical appraisal
An item-level critical appraisal of included studies is reported in Supplementary file 2 (Table 2). Most reviews detailed thorough search strategies which demonstrated a strong likelihood of capture of all relevant studies. Clear research aims were present in all reviews and most studies also conducted quality assessment of included studies.
The generalizability of review findings was often complicated by heterogeneity in intervention type, components and measured outcomes. As a result, authors of reviews were generally unable to conduct meta-analyses, instead summarizing statistical tests of effectiveness or distinguishing between the effectivity of particular components of an intervention.
Lack of statistical study of quantitative data was compounded by the small number of studies eligible in the majority of reviews. Some reviews included only studies conducted in specific regions, such as Sub-Saharan Africa. This further limited the generalizability of findings within and between the included reviews.
CMO configurations
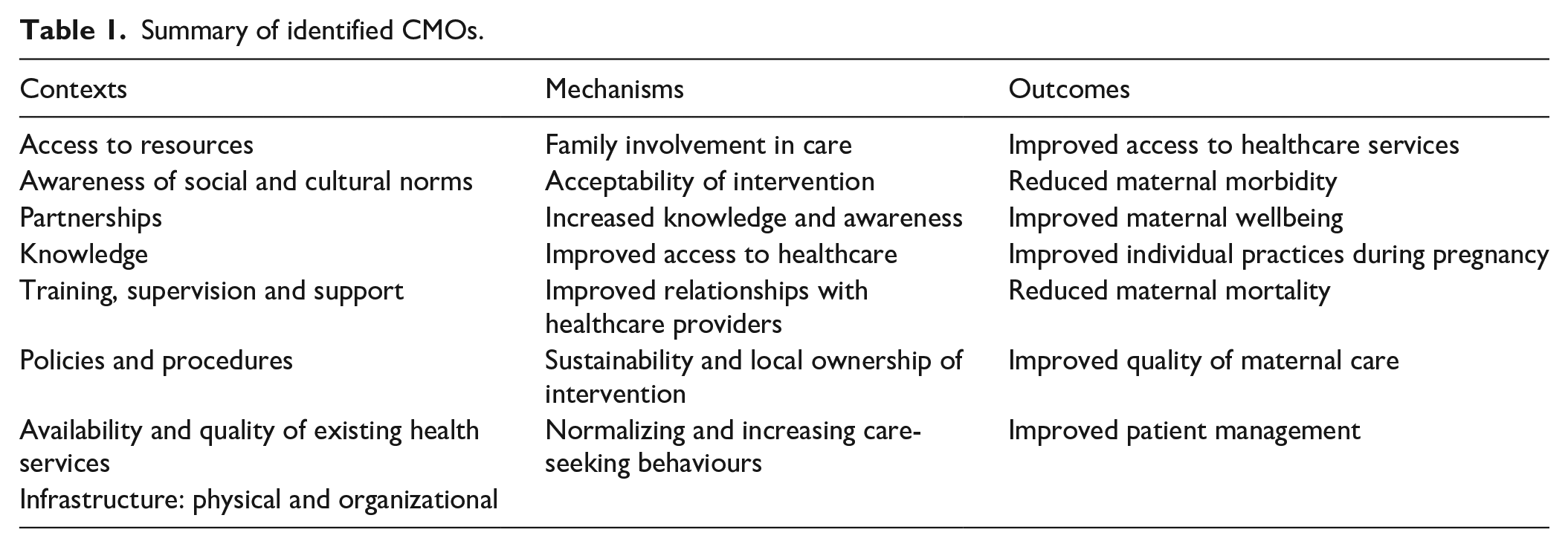
Key CMOs are listed in Table 1. The relationship between CMOs is illustrated in Figure 2.
Summary of identified CMOs.

Relationships between CMOs.
Contexts
Infrastructural capacity
Healthcare system contextual factors were the most frequently reported for effective intervention implementation. The majority of factors within this level were related to the infrastructural capacity of a country’s health system. This comprises both the system’s human resources and organizational capacity to implement and maintain the intervention programme. Physical space, water and electricity supply was identified as essential for intervention contexts where facilities were required for staff to receive training and for women and partners attending health facilities to receive care and education.25,28,31 Papers also reported sufficient healthcare and organizational staff as necessary for the effective organization, implementation and monitoring of interventions.23,36,67
Training, supervision and support
Reviews emphasized the importance of providing sufficient training and supervision to healthcare professionals (HCPs) to both safely and effectively carry out the proposed intervention and to ensure that staff felt confident and supported in their tasks.23,24,27,36,40,48,67
Availability and quality of existing health services
The availability and quality of pre-existing healthcare services is another contextual factor at the healthcare system level. For example, Rahman et al.’s 55 review of mHealth interventions reported that strategies designed to increase service coverage could only perform effectively if structural factors such as established ANC services and resources were available for women to use.
Access to resources
This contextual factor spans almost all contextual levels but was especially important for the individual and HCP. This is clearly demonstrated in mHealth interventions where both the pregnant women/mothers who receive the message and the HCPs delivering the messages require access to mobile phones and a reliable mobile network.68,69 HCPs also require resources, such as transportation, medical equipment and access to medication, to implement proposed interventions and provide standard care. 67
The definition of a resource not only covers physical resources required for the logistical operation of the intervention but also includes socio-political factors that enable access to resources required for an intervention. For example, political instability, road closures or poor road conditions, and disruption and displacement of populations can reduce women’s access to transport, adequate nutrition or medication.23,24,29
Awareness of cultural and social norms
The norms of a community can function as enablers and barriers for intervention implementation and sustainability. For example, in patriarchal societies, men can be the main decision-makers of their households and in charge of their partner’s healthcare.55,59 Barriers for pregnant women and new mothers due to societal gender or cultural norms prevent women from participating in community groups or from attending ANC or postnatal care (PNC) visits.48,67
Partnerships
The importance of cooperation and partnership of health systems with their community, local or national authorities and external agencies was a recurrent theme required for success and sustainability of an intervention. For instance, Munodawafa et al.’s 48 review of task-sharing interventions to improve perinatal depression outcomes showed that interventions in rural contexts faced challenges due to difficulties in building rapport with marginalized individuals. Intervention organizers who worked with established and trusted community groups or local partners deemed this as important contextual factors for training outreach volunteers, raising awareness and changing norms within the community.26,70
Knowledge
The level of knowledge of pregnant women/mothers and HCPs is an enabling or disabling contextual factor. For example, an individual’s lack of knowledge about abortion laws or locations that provide abortion services can restrict the effect of interventions to access to services for women. 36 HCPs knowledge of their required skills and ability to explain care to their patients is an enabler of interventions that aim to increase women’s use and trust of maternal care services. 40
Policies and procedures
This contextual factor includes the existence and adherence of HCPs to health policies and procedures and existence of laws that protect the rights of women and mothers. This factor was common for interventions at the political, economic and geographical and healthcare system level. Hunter’s and Murray’s 71 review of conditional cash transfers (CCT) reported that the establishment and enforcing of procedures for correctly identifying and allocating financial incentives to women was necessary for the implementation of the intervention. In a review of interventions to improve outcomes for pregnant women experiencing domestic abuse, the existence and enforcement of laws that protect abused women was a significant contextual factor and effect moderator for women engaging with the intervention. 28
Mechanisms
Individual-level mechanisms were the most common level of effect of intervention, followed by healthcare provider mechanisms. The most common mechanisms reported were increased knowledge and awareness, followed closely by increased access to healthcare mechanism factors.
Family involvement
Involvement of male partners and wider members of a pregnant or mothering women’s family was a common component of reviewed interventions.28,53,55,60,61 This mechanism often overlapped with the mechanism of increased knowledge and awareness and normalizing care-seeking behaviours. For example, better informed relatives and male partners were reported to facilitate and implement positive health behaviours, such as encouraging women to attend ANC or PNC.55,61
Acceptability of intervention
Women’s trust and acceptability of interventions and of existing health services moderates intervention effect. Educational interventions aiming to increase access to care worked by increasing women’s trust and acceptability of the care services available and the information that they were being taught.55,63 Zuñiga et al.’s 66 review of interventions to increase the use of skilled birth attendants reported that community health workers (CHWs) effectively promoted confidence and trust of healthcare services and professionals. Involving the community was effective by challenging and changing norms surrounding pregnancy and PNC to create a safer and more supportive environment for pregnant women and new mothers.26,53
Acceptability of HCPs was also reported as interventions that integrated with their daily work created an acceptable working environment and motivated staff to provide and improve maternal care.25,48
Increased knowledge and awareness
This mechanism was prevalent at both the individual and HCP level. Improving women’s knowledge and awareness of signs of poor health and ANC and PNC empowered women to increase their use of care services and therefore improve their health outcomes. 32 At the HCP level, improved knowledge of delivering care increased women’s trust and acceptability of care services, and improving the quality of care provided and improving health outcomes.25,44
Improved access
Increasing women’s physical and socio-political access to healthcare services was a mechanism of improving health outcomes. For example, interventions that provided emergency transportation to health facilities improved access and lead to increased coverage and utilization of maternal care services. 47 Interventions that also provided educational community outreach helped women living in rural areas to receive maternal care education that they could not otherwise access.24,41
Sustainability and local ownership
An intervention’s capacity to generate local ownership contributes to the effectivity and sustainability of the intervention. Lazzerini et al.’s 44 review reported that successful interventions consulted frontline healthcare staff before hospital management in proposed actions to improve care. This improved quality of maternal care by encouraging ownership and accountability for the successful implementation and maintenance of the programme.
Normalizing and increasing care-seeking behaviours
This mechanism was reported in reviews of financial incentive, community involvement interventions and in interventions to inform and empower women of their health rights.26,35,46 A vital component of normalizing care-seeking was challenging traditional norms surrounding pregnancy while still acknowledging and respecting these norms.26,48,53 This was demonstrated in Dada et al.’s 26 review which reported that successful interventions incorporated consideration pregnancy norms through stakeholder engagement in the planning stage but also challenged these through education and awareness during the intervention implementation.
Outcomes
Various outcome themes were reported within included reviews. These were categorized into broad themes.
Uptake of healthcare services
This was the most prevalent outcome theme. This included ANC and PNC coverage, use of skilled birth attendants, attendance at maternity waiting homes and engagement with CHWs.26,32,35,72 All mechanism themes were reported to have a relationship with this outcome.
Maternal mortality and morbidity
These outcomes were the second and third most common outcome theme reported within included reviews. These outcomes were associated with intervention mechanisms associated with acceptability of intervention, increased knowledge and awareness and improved access to healthcare.23,27,36,40
Quality of maternal care
Improved quality of maternal care was reported in the majority of CMO relationships. Dimensions of quality of care across reviews included efficiency of processes of care, such as waiting times, improved efficacy of structure of care, such as essential equipment and supplies, and quality of facilities, such as maternity waiting homes, as judged by the service users.37,44,47
Individual practices
Individual practices referred to the theme of women’s improved behaviours during pregnancy such as improved nutrition, improved use of nutrient supplementation and increase in safety behaviours in the context of domestic abuse.28,56,70 This outcome was seen in only two contexts: access to resources and awareness of social and cultural norms.
Maternal wellbeing
This outcome was only reported within the contextual theme of awareness of social and cultural norms. This was commonly in association with interventions providing psychosocial counselling/education.28,48
Patient management
Patient management was a common outcome theme and includes the clinical and organizational management of a patient’s care. This outcome theme was common within interventions targeting healthcare system contextual factors related to the health system’s physical and organizational infrastructure of a health system, policies and procedures and partnerships.
Discussion
This realist synthesis examined and identified contexts and mechanism that shape the effectiveness of maternal health interventions. We summarize our findings and relate these to implications for policy and practice.
Contexts
Our review showed that the majority of contextual factors associated with effective intervention implementation were regarding infrastructural capacity of a health system. This is the personnel, organizational, logistical and physical capabilities of the system to conduct, organize and allocate resources. Poor development of infrastructure in LMICs, such as Sub-Saharan Africa, especially in rural areas, contributes to the poor progress made in maternal and child health. 73 This is especially relevant in contexts of displacement or civil unrest where access to water, electricity and safe transport networks are scarce. 24
A consequence of weak and under-resourced health systems is the challenges in recruiting and retaining HCPs. Poor working conditions, lack of supervision, equipment and infrastructure contribute to HCPs leaving remote and rural areas for more urbanized areas.74,75 Therefore, increasing the burden of care on existing rural HCPs and health infrastructure. Lack of health infrastructure can also be a restricting factor for staff to implement and use their newly gained knowledge during clinical practice. 76
In contrast to this, a cross-sectional analysis of the association between infrastructure and observed care across eight LMICs found that inputs to care, such as amenities, equipment and medications available in health services, was not correlated with quality of evidence-based care. 77 For instance, HCPs working in well-equipped facilities were shown to often provide poor care and vice versa. This study suggests that while infrastructure is an important component of how well a health system or intervention performs, it may not be the most accurate measure or important enabler of the quality of care provided by HCPs.
Partnerships formed an interesting contextual factor that arose in many included reviews.24,26,30,35,37,48 This factor encompassed relationships between HCPs and the community and broader relationships between health systems, local authorities and external agencies. HCP–patient relationships in maternal care significantly contribute to the quality and quantity of care that women receive and have implications for maternal morbidity and mortality in LMICs.78,79 Socioeconomic differences can exacerbate existing power differentials within the healthcare setting where HCPs can demonstrate dominance through their differences in knowledge, skill set and roles in professional workplaces. 80 Blanchard et al.’s review of contextual factors influencing CHWs emphasized the influence of social hierarchies on maternal care uptake. CHWs, who resided and existed in the same social networks of the women and families that they worked with, reported improved skilled birth attendance and home-based care practices. 24 This is supported by a survey of community members and health workers in Ghana which found that women from low socioeconomic status (SES) were at higher risk of difficult experiences in formal health settings due to feeling ashamed or disrespected by HCPs. 80 The discrimination that women faced due to socioeconomic differences from HCPs contributed to the power imbalance and subsequently affected the quality of care women received and consequently, their care-seeking behaviours. 80
This evidence also demonstrates that effective partnerships in health interventions require an understanding and awareness of cultural and social norms. Therefore, interventions that do not acknowledge these contextual factors may prove to be ineffective if not designed to be culturally acceptable by the community. 23 This is further reflected in the finding that CHW-led outreach was a common component in interventions to promote women’s trust and confidence in healthcare services.24,41 CHWs are often the first point of contact for healthcare for pregnant women in LMICs, especially in hard-to-reach areas, and can significantly contribute to achieving equitable maternal health outcomes.24,81
Partnerships formed between health systems and local or external agencies were another important contextual factor in interventions, especially those related to demand or supply-side financing and mHealth.30,32,35,37 Barnett et al. 82 highlighted two main purposes of interorganizational partnership: material and symbolic. Material partnerships provide the organization with the resources it requires for implementation and diffusion of new programmes. Whereas symbolic partnerships are important to gain local consensus and legitimize the new programme. This was demonstrated in the review findings that partnerships with local community groups not only provided a source of physical space, resources and volunteers for the implementation but also enabled rapport and support to be gained from key community stakeholders that was necessary for intervention acceptability and engagement.26,48,53 Including the community and local stakeholders in the design and process of an intervention implementation was an important component of maintaining local ownership and sustainability of the intervention and implementing behaviour change.44,48,53,70,83
Mechanisms
Turning attention to identified mechanisms, we found that the majority of reviews identified targeted mechanisms of interventions at an individual level of the pregnant woman or the healthcare provider. This mechanism was achieved through most contexts. Educational intervention strategies for pregnant women, family members and HCPs to improve their clinical skills were a common intervention component.32,44 –46,53,54
Lack of knowledge of the importance of seeking medical care during pregnancy and labour hinders women’s health behaviours and the decision-making process. 84 However, an international survey of maternal health researchers suggests that the major challenge for improving maternal care is access to healthcare rather than women’s knowledge of the importance for healthcare. The authors suggest that maternal research efforts should prioritize strategies to strengthen and improve the quality of health systems and to increase women’s access to healthcare. 85 For example, involving family members and male partners in intervention strategies was an important mechanism in contexts and cultures where patriarchal gender norms dominate. 86 Women are often not the sole decision-makers of their healthcare, and male partners and other family members can hold the majority of decision-making and financial power. 86 Involving male partners in interventions enabled men to facilitate and implement positive health behaviours in their pregnant partners.55,60,61 This also enables men to support their partners both financially and emotionally to access healthcare.55,60,61 Programme and policymakers must acknowledge that mechanisms must go further than providing education and must understand the interplaying factors that exist in different contexts and influence women’s access to and utilization of maternal care.
Outcomes
Health system-level factors were a common theme in contextual and mechanism factors. However, this theme was less frequently found within outcomes of reviews of maternal care interventions. Measured and reported outcomes were often related to actions and uptake of maternal care, maternal behaviours and clinical outcomes. This suggests that the worldwide focus on improving maternal outcomes is judged by the numerical and direct indicators of maternal care, such as MMR and uptake of ANC/PNC services. However, our evidence suggests that contexts of healthcare systems and mechanisms, such as community and effective partnerships, are necessary for provoking these improved outcomes. Therefore, an appreciation and focus on the outcomes of improved healthcare systems and community functioning, education and changing of norms can directly improve maternal health outcomes.
Limitations
The limitations of the review include the potential risk for language and publication bias as only published papers in English were included for review. While not strictly a limitation, realist synthesis is a fundamentally inductive method. On this basis, a different review group may have generated different CMOs. Logistical and time constraints also limited the extent of the databases used to capture reviews which could have been widened to include more reviews.
Conclusion
The relationships between CMOs were complex and often overlapped, suggesting that contexts are not independent in their influence and rely on the presence of other contexts to produce mechanism and outcomes. This suggests that a single intervention cannot by itself improve maternal health and interventions must work in multiple contexts and mechanisms to show effect.
Various relationships within and between contexts and mechanisms exist in maternal health interventions which provide an evidence base for future interventions. First, healthcare system factors being the most prevalent contextual factor suggest that programme and policymakers must ensure interventions designed to increase coverage are conducted in contexts of functioning health systems and infrastructure. This ensures that systems can withstand the pressure of additional resources required and the potential increased service utilization.
Second, intervention strategies must recognize that health-seeking behaviours are intricately intertwined and embedded within cultural and social practices, SES, environmental conditions and family influences and providers’ attitudes. Therefore, interventions that focus solely on increasing women’s knowledge or awareness of accepting healthcare are limited in effectivity. Interventions that recognize the other moderators of positive health behaviours, such as family and community support, HCP–patient provider relationships and broader socio-political factors are more likely to be effective.
Third, programme makers must involve key community stakeholders, local health management and governance, and local families in the design and process of the health intervention. This ensures local ownership and sustainability, and ensuring maternal health is considered and supported as a community issue rather than an individual one.
Future research should focus on the contexts and mechanisms of community engagement and mobilization to change social norms and improve maternal health. This would offer recommendations to programme makers about building health intervention programmes that are tailored to the needs of a specific community and appropriate to the community’s contexts.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231205687 – Supplemental material for A realist review of interventions targeting maternal health in low- and middle-income countries
Supplemental material, sj-docx-1-whe-10.1177_17455057231205687 for A realist review of interventions targeting maternal health in low- and middle-income countries by Julie Mariam Abraham and GJ Melendez-Torres in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231205687 – Supplemental material for A realist review of interventions targeting maternal health in low- and middle-income countries
Supplemental material, sj-docx-2-whe-10.1177_17455057231205687 for A realist review of interventions targeting maternal health in low- and middle-income countries by Julie Mariam Abraham and GJ Melendez-Torres in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231205687 – Supplemental material for A realist review of interventions targeting maternal health in low- and middle-income countries
Supplemental material, sj-docx-3-whe-10.1177_17455057231205687 for A realist review of interventions targeting maternal health in low- and middle-income countries by Julie Mariam Abraham and GJ Melendez-Torres in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.