
Abstract
Background:
Black women and their infants face heightened health risks during pregnancy, labor, and delivery that, for many, cost them their lives. Such health risks during this critical period are linked to increased rates of anxiety among Black pregnant and postpartum women. Black women also endure racism when seeking support from mental health and healthcare providers, which further contributes to pregnancy and postpartum-related anxiety. Evidence on sister circles has demonstrated that this indigenous form of healing may provide Black pregnant and postpartum women with the support and skills needed to cope with stressors associated with mental and physical health concerns and racism.
Objective:
Our study aimed to evaluate the feasibility and acceptability of the Birthing Beautiful Babies Sisters Offering Support, a sister circle cognitive behavioral therapy-based stress and anxiety intervention for Black pregnant and postpartum women.
Design:
Our study employed a mixed-methods framework.
Methods:
Descriptive analyses, paired samples t-test, and open and selective coding were conducted. We utilized the following measures: Penn State Worry Questionnaire–Abbreviated, Kessler Psychological Distress Scale, Pregnancy-Related Anxiety Scale, focus booklet, and focus group discussion.
Results:
Participants reported experiencing moderate levels of worry and distress and low levels of pregnancy-related anxiety prior to the start of the Birthing Beautiful Babies Sisters Offering Support intervention. Eighty women participated in Birthing Beautiful Babies Sisters Offering Support. Eleven focus groups were conducted to assess their experience. Participants reported a perceived increase in their knowledge about panic attacks and stress and ability to manage stressors effectively. They found that all completed activities contributed to their development and application of skills. They reported they enjoyed Birthing Beautiful Babies Sisters Offering Support because of the supportive environment, openness, and emphasis on sisterhood. Participants provided helpful feedback about the structure and flow of the intervention.
Conclusion:
Limitations of the present study and future directions are discussed.
Introduction
Black women and their infants face heightened health risks during pregnancy, labor, and delivery that cost many their lives. 1 For example, in the USA, Black pregnant women are five times more likely to die from pregnancy-related complications than White women. 2 Similarly, Black infants are twice as likely to die before their first birthday than their White, Asian, and Hispanic counterparts. 3 Furthermore, the awareness of these racial health disparities is a painstaking reality for Black women, which likely contributes to the growing rates of pregnancy-related anxiety in this population.
Black women have a high risk of experiencing perinatal and postnatal mood and anxiety disorders (PMADs), such as anxiety, depression, obsessive-compulsive disorder, and post-traumatic stress disorder. 4 In recent decades, Black pregnant women and mothers, including celebrities such as Serena Williams and Taraji P. Henson, have become vocal about the importance of mental health support for this community.5,6 Despite their wants for mental health care, Black women continually experience difficulty gaining access to quality providers that are both culturally responsive and aware of their own implicit biases.7 –9 Multiple studies have shown that mental health care providers may be uncomfortable talking about race-based topics or hold negative attitudes and beliefs about Black Americans, which affects how they interact with their patients and which treatments they provide.10,11 Regarding receiving mental health care during pregnancy and birth, Black women report greater provider mistreatment and discrimination, based on insurance and race, than White women.12 –14 These stressful racialized experiences likely also contribute to the growing rates of anxiety among Black women.4,15 –19
Sister circle interventions
One anxiety intervention that may be effective and address the unique needs of Black women is sister circles. Sister circles can be defined as “support groups that build upon existing friendships, fictive kin networks, and the sense of community among [Black] females” (p. 1). 20 Importantly, sister circles are unstructured, and they promote relationship-building. 20 A Black woman may be exposed to various forms of sister circles throughout her life that naturally develop within her community and organizations. 21 She may also be exposed to more organized and structured sister circles in her school or workplace. For example, sister circles have been used to increase cultural values and beliefs, improve academic performance, and reduce disruptive behaviors in school among Black adolescent girls.22 –24 Within collegiate and professional spaces, multiple sister circles were created to not only provide support but also to serve as a form of resistance to the oppression that Black women face daily.25 –30
While these forms of sister circles were successful in targeting their various goals, few studies have evaluated the effectiveness of the sister circle format as a manualized, culturally relevant group intervention for Black women. One example is the Prime-Time Sister Circles (PTSC) intervention. 31 The PTSC used a cognitive behavioral modality integrated with the values and beliefs salient to midlife Black women to reduce their health-risk behaviors. Findings from both the original and replication studies revealed increases in physical activity and reductions in stress.31,32 Another example of a manualized sister circle is the Sisters Offering Support (SOS) intervention developed by Neal-Barnett et al. 20 SOS was developed as an early intervention for anxious professional Black women. It is unique because it utilizes cognitive behavioral techniques infused with cultural aspects to educate Black women about anxiety, cognitive restructuring, and progressive muscle relaxation.
Birthing Beautiful Babies Sisters Offering Support theoretical framework
Considering the various uses of the sister circles for Black women across the lifespan to address mental and physical health risks and concerns, we believe that this format would be beneficial for Black pregnant and postpartum women experiencing stress and anxiety. To the best of our knowledge, sister circles have not been utilized with Black perinatal samples.
Thus, we developed the Birthing Beautiful Babies Sisters Offering Support (BBB SOS) intervention to address specific pregnancy and cultural concerns of this population to reduce pregnancy-related anxiety. It is grounded in cognitive behavioral therapy (CBT) because it is one of the most effective treatments for anxiety-related disorders. 33 CBT emphasizes the importance of changing thinking and behavioral patterns and improving physical symptoms of anxiety through skill use. 34 Within the context of BBB SOS, the overarching goals of the sister circle were to educate pregnant women about anxiety, stress, and panic attacks and help them challenge maladaptive thoughts, learn how to manage their emotions, and engage in positive behavioral changes. In order to maximize the potential effectiveness of the CBT framework with the present study’s sample of Black women, we followed recommendations from studies35,36 that encouraged the use of “gender-race-specific modifications and infusion” (p. 269). 20
Since sister circles are peer-supported interventions, we felt it was best to have women from the community serve as facilitators. Specifically, we utilized Black perinatal support persons (i.e. doulas) who were well-trained on all aspects of the prenatal and postpartum periods and shared the general experience of being a Black woman. Furthermore, while the participants were learning common CBT strategies (e.g. visualization, goal setting, and progressive muscle relaxation), there were also discussions about culturally relevant stressors, including racial discrimination, stereotypical images of Black women in the media, health, nutrition, hair care, and hair health.
Research indicates that stereotypical images of Black women as strong, angry, and promiscuous are associated with increased anxiety.37 –39 Further, in addition to anxiety, Black women report high rates of obesity. 40 BBB SOS provides prenatal yoga and nutrition, which helps Black women combat their many health outcomes and risks,41,42 including obesity, preeclampsia, and hypertension, which are heavily influenced by poor diet and limited exercise.43,44 Black women also experience specific hair care needs and restrictions during pregnancy. 45 BBB SOS provides solutions for Black women with natural or relaxed hair that remedy hair-related stress and anxiety. 46 Research underscores that for Black women, hair is culturally important and significant47,48 and a potential source of anxiety as textured hair is associated with discrimination. 49
Present study
The primary objective of this study is to evaluate the feasibility and acceptability of BBB SOS, a manualized culturally relevant stress and anxiety intervention for Black pregnant and postpartum women using a mixed-methods framework. Our research question is: will Black pregnant and postpartum women perceive the BBB SOS sister circle anxiety intervention to be helpful? We opted to use a mixed-methods design as we believe the complementary quantitative and qualitative data would (1) answer our primary research question and (2) provide substantial and specific feedback to improve our intervention. In addition, we hypothesized that (1) participants would report a perceived increase in knowledge about anxiety and panic attacks and (2) participants would rate all session activities and skills as helpful in reducing anxiety.
Method
Participants
Our convenience sample consisted of 80 Black pregnant and postpartum women from an urban city in the Midwest. The average participant was 26.72 (SD = 6.51) years old. Participants were recruited from our community partners. Our partners are a perinatal support program that was developed to aid communities at risk for maternal and infant mortality. Women enrolled in the perinatal support program were invited by their doulas face to face and via a call to participate in the in-person BBB SOS sister circle. Our study and recruitment occurred pre-pandemic, between 2017 and 2019. During this time, approximately 203 women received perinatal support services from our community partner and were offered participation in the study. One hundred and twenty-three (60.59%) did not enroll in our study. Reasons for declining participation were not recorded. Table 1 displays the complete demographic information of this sample.
Participant demographic information (N = 80).

Note percentages may not equal 100% due to rounded decimals.
Measures
Demographic survey
Demographic questionnaires were used to collect information on participants’ self-identified race, age, pregnancy status, number of children, and type of insurance to describe the sample.
The following three measures of worry, stress, and pregnancy-related anxiety were utilized only to confirm that our sample was our target population and that we could appropriately ask about their perceptions of the feasibility and acceptability of our sister circle anxiety intervention.
Penn State Worry Questionnaire–Abbreviated
The Penn State Worry Questionnaire–Abbreviated (PSWQ-A) 50 is an 8-item scale designed to measure worry severity. Given that the present study’s sample is composed of Black women, an additional item was added to assess participants’ level of worry about racism. Each item was scored on a scale from 0 (not at all typical of me) to 5 (very typical of me), which yielded composite scores ranging from 0 to 45. DeLapp et al. 51 found the PSWQ-A to be a psychometrically sound brief measure of worry in Black Americans.
Kessler Psychological Distress Scale
The Kessler Psychological Distress Scale (K10) 52 is a 10-item measure of global distress experienced within a 4-week period. Specific items include questions about symptoms of anxiety and depression. The items were rated on a scale from 1 (none of the time) to 5 (all of the time). Composite scores can range from 10 to 50 and are derived from summing item responses. Krieger et al. 53 found the K10 to be a reliable and valid measure of distress in Black American men and women.
Pregnancy-Related Anxiety Scale
The Pregnancy-Related Anxiety Scale 54 is a 10-item measure for expectant mothers that determines the severity of their worries about the various aspects of pregnancy, labor, and delivery, and then caring for a child. Items were scored on a scale from 1 (not at all) to 4 (very much). Composite scores were calculated by summing and then dividing the items’ responses by 10, yielding a possible range from 1 to 4. This questionnaire demonstrated high reliability and validity in a sample of Black pregnant women. 54
Focus group booklet
A focus group booklet was created and piloted for this study. It contained questions assessing participants’ understanding of panic attacks and stress before and after the intervention on a scale from 0 (nothing at all) to 10 (a great deal). Items that measured participants’ perceived effectiveness of exercises and strategies covered in each session were also included. Participants were asked to rate their overall experience participating in the sister circle on a scale from 0 (very negative) to 10 (very positive) and comfortability with sharing with others within the sister circle on a scale from 0 (not so much) to 10 (very much so). The final question asked participants if they would participate in a BBB SOS sister circle in the future.
Focus group discussion
An academic and community research team formulated 10 focus group discussion questions. Questions centered on participants’ initial thoughts when asked to participate in BBB SOS, experiences and thoughts about exercises and activities utilized in the group, the timing of sessions, comfortability with doulas, identification in personal development, their experiences versus expectations, any ideas for improvement, and initial thoughts when asked to participate in BBB SOS.
Procedure
All study procedures were approved by the Kent State University Institutional Review Board. As noted above, recruitment procedures were completed by our community partner, a perinatal support program.
BBB SOS sister circle
Intervention training
Two Black female perinatal doulas received in-person training from a licensed clinical psychologist to facilitate the BBB SOS intervention. They were provided with a manual that contained all intervention materials and instructions to use as a training guide. The training covered intervention goals and objectives, data measures, and data collection procedures. The BBB SOS curriculum was presented in detail. The clinical psychologist taught the intervention session by session, thoroughly covering session-specific content and materials, including psychoeducational and activity components. Prior to study implementation and independent of our study specifications, our BBB SOS doula facilitators possessed mental health certifications (e.g. Qualified Mental Health Professional and Community Health Worker) and were up-to-date with their continuing education courses as a part of their professional development. Therefore, we determined an extensive CBT training was not needed. Instead, the training included a brief CBT review and emphasized administering CBT-based activities to our target population. Finally, our BBB SOS doulas practiced administration with the staff multiple times before study implementation. Training took place over 3 months.
Intervention overview
BBB SOS was initially administered as an 11-week intervention. Staff and participants gathered weekly for 2-h sessions in a local community center. After two iterations, participant feedback led us to condense the 11-week intervention to 7 weeks. Review exercises and casual group discussions were shortened. However, no exercises were removed in their entirety. The remaining manuscript will focus mainly on our procedures and data on the 7-week intervention. Descriptive data from the 11-week intervention will be briefly discussed.
In the first session, doulas explained the general goals of the research project. Then, written consent and participants’ demographic information (e.g. age, pregnancy status, and household income) were obtained during sign-in by a Black female undergraduate or graduate research assistant. Participants received a binder with the BBB SOS group mission statement that read:
This is a place to speak your truth, to be heard, embraced, and received in a loving, relatable way that supports, encourages, and empowers Black women.
and a covenant we adapted from the Women of Color Foundation with permission, that read:
I see your beauty I sense your power I celebrate your potential I support your prerogative to sing your own song.
Participants were also given a copy of Soothe Your Nerves: The Black Woman’s Guide to Understanding and Overcoming Anxiety, Panic, and Fear 55 as a complementary text to multiple intervention components. This text uses anecdotes to discuss Black women’s experiences with stress, anxiety, and panic attacks. These firsthand accounts include Black women who are childless, pregnant, postpartum, and mothers, highlighting that the stressors of Black women magnify during pregnancy and motherhood. It also promotes a sense of “sisterhood” by normalizing familiar and novel experiences. This is particularly helpful for BBB SOS groups with few or shy participants. Second, this text discusses and dispels harmful myths and stereotypes, such as the “Strong Black Woman” trope. Next, it breaks down the stigma of therapy within the Black community and introduces the basic tenets of CBT. Finally, CBT components and related strategies are explained and recommended to promote healthy emotional functioning.
Doulas encouraged participants to read specific chapters of Soothe Your Nerves for assigned homework related to specific BBB SOS sessions. Doulas also provide verbal summaries of the text at the beginning of sessions so that participants who did not have time to read or do not enjoy reading can follow group discussions.
After participants were settled, the doulas checked in with participants, completed introductions, and then introduced the BBB SOS guiding principles and group mission statements. Later, they instructed participants to develop their personal mission statement that allowed them to establish their goals for participating in the sister circle. Doulas ended session one by leading the group in reciting the BBB SOS covenant, reinforcing the sisterhood dynamic of the sister circle.
Sessions 2 through 5 began similarly: check-in and review of Soothe Your Nerve text and review of group guidelines and mission statement. During these check-ins, doulas would discuss previous exercises, homework completion, and participation in BBB SOS strategies outside of the intervention. Afterward, participants were provided with detailed psychoeducation about the emotional, cognitive, and biological consequences of stress, anxiety, and panic attacks. Some education on postpartum depression was also discussed with participants, given its prevalence in this population. 56
During these sessions, doulas led discussions about the psychological impact of images and stereotypes of Black women in the media. They encouraged the participants to share their experiences with anxiety, racism, and racial stress. In addition, doulas introduced and led evidence-based strategies to reduce anxiety, including goal setting, progressive muscle relaxation, and visualization. Participants also learned how to engage in cognitive restructuring through a Build Your Own Theme Song (BYOTS) activity that helped them use music to replace negative thoughts with positive thoughts. Participants also received hair consultations, information about hair care needs during pregnancy, and a hair scarf wrapping demonstration.
In the latter half of sessions five and six, participants participated in pregnancy yoga led by a certified instructor. Session six was also devoted to educating participants about nutrition using the U.S. Department of Agriculture’s recommendations. 57
Focus group
During the final session, participants celebrated their completion of the BBB SOS with a graduation party. A focus group discussion also occurred and lasted approximately 2 h. It was led and audio recorded by either a trained Black female graduate student (MA) or a project coordinator (MA). Both women have previous work experience related to mental health concerns in Black communities in the sampled area. These women did not participate in any of the other BBB SOS sessions and are not authors on this article. Their focus group training was conducted by a licensed clinical psychologist (PhD). The focus group interviewer took observational notes.
In addition to the focus group discussion, participants also answered questions in paper focus group booklets. All data were collected at the local community center, where the BBB SOS sessions occurred. No other individuals were present besides doula facilitators, undergraduate or graduate students, and project coordinator, all of whom were Black females.
Participants received a certificate, a US$50 Walmart gift card, a yoga mat, and food storage containers for their participation in the study. We also provided transportation and onsite childcare to participants in need for all our sessions to reduce additional attendance barriers for pregnant mothers. See the Online Appendix for a flowchart of the BBB SOS Curriculum (Figure 1).
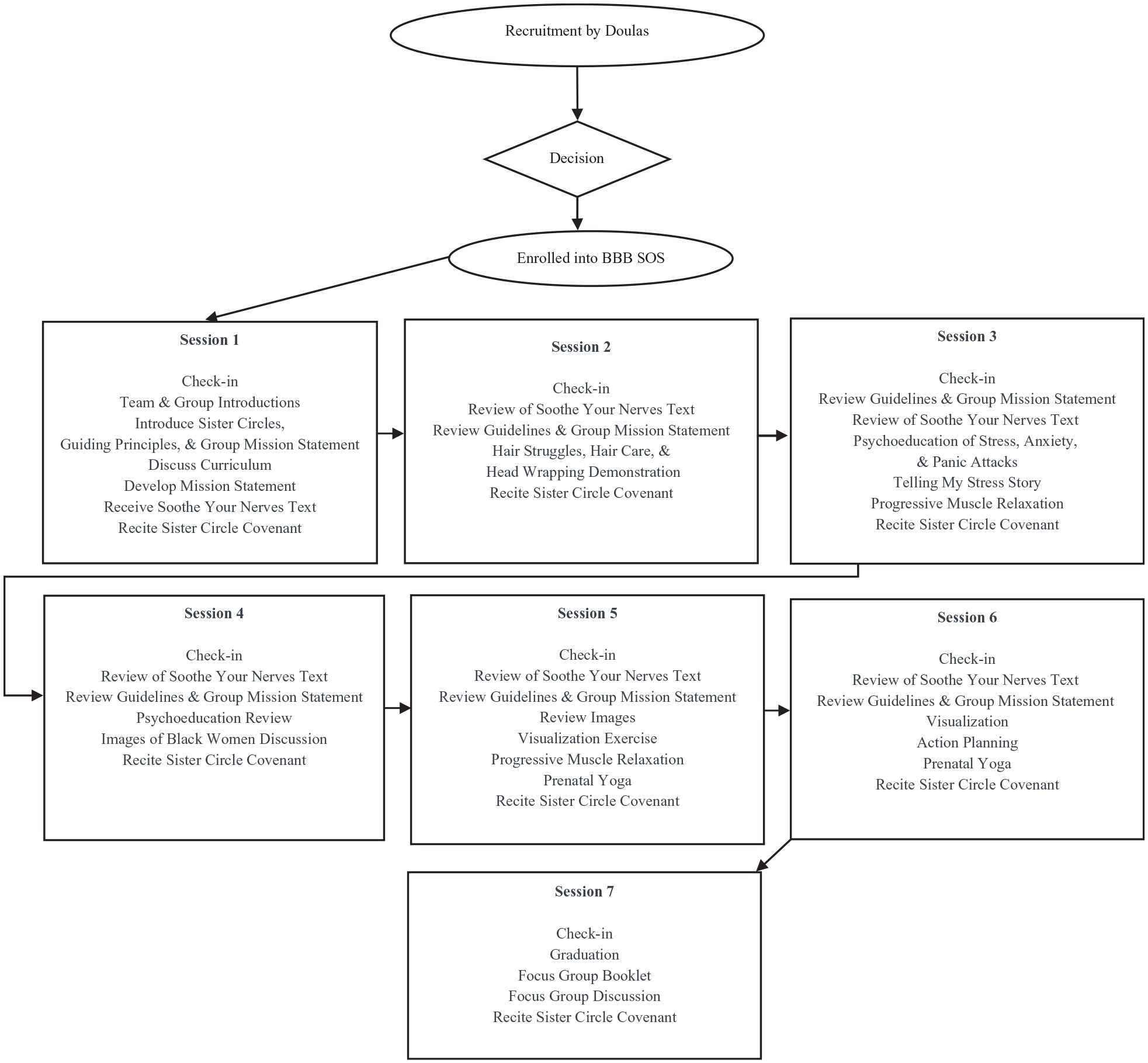
BBB SOS intervention flowchart.
Supervision
We conducted fidelity checks weekly to assess the doula-led intervention implementation. Checks were completed live during the sessions by a Black female undergraduate or graduate research assistant. A standard CBT checklist was modified to assess group intervention-specific components such as guiding principles, facilitators’ knowledge, and group participation questions. Doulas were provided a completed fidelity checklist and weekly observational report. See Online Appendix for our fidelity checklist. A licensed clinical psychologist also provided weekly group supervision, which BBB SOS doula facilitators, doulas on separate projects, research assistants, and project coordinators attended.
Statistical analysis
We conducted power analyses to determine an appropriate sample size for our study.
According to G*Power, approximately 34 study participants were required to detect an effect for our study-specific hypotheses. 58 Specifically, we evaluated a priori power analyses for our paired t-tests, with an alpha of 0.05, a power of 0.80, and a medium effect size.
Quantitative
Quantitative data analyses were conducted using SPSS 25.0. Skewness and kurtosis data were reviewed to assess normality according to Kline’s 59 recommendation. Descriptive data analyses of participant baseline worry, distress, and pregnancy-related anxiety were analyzed. Participants’ baseline and post-knowledge about panic attacks and stress were collected via the focus group booklets and evaluated using paired samples t-tests.
Qualitative
Qualitative data analysis procedures were rooted in Grounded Theory60,61 and were led by the first author on this manuscript, a Black female doctoral student. Audio transcripts of the BBB SOS focus groups were reviewed by all authors on the paper. Then, they conducted an organizational meeting to discuss and create coding guidelines.
The data was open-coded by four undergraduate research assistants (two Black females, one Black male, and one White female) for general themes. Coders were instructed to read the transcripts and identify any general themes they felt represented many participants’ responses. In addition, coders were asked to highlight and note any specific examples on the transcript indicative of such themes on a coding form. They were not given any specific themes to identify in the transcripts.
Once coders completed and submitted their initial open coding, they met with the lead author, who provided them with selective coding procedures. Coders were asked to re-read the transcripts and identify quotes that represented or related to learning and feasibility. These themes were selected by authors on this article during the organizational meeting as they related to our research question: will Black pregnant and postpartum women perceive the BBB SOS sister circle anxiety intervention to be helpful? More specifically, the theme “Learning/Valuable” was defined as experiences that represented, but were not limited to, successful or useful skills, beneficial takeaways, or additive value. Coders were given the following examples to guide their selective coding further: “Because of SOS, I take deep breaths when I am stressed,” “Gained friendships,” and “I enjoyed talking about my issues.” The theme “Feasibility” was defined as comments that represented sister circles being practical, achievable, reasonable, or workable (e.g. “the sessions occurred regularly,” “doulas handed out materials,” “the members worked together as a team”). Coders were also asked to identify noteworthy themes. They were instructed to note such themes as “Other” and provide a descriptor that appropriately categorized the statement and/or theme.
Coders documented their selective codings on a separate coding form and submitted it to the lead author. She combined all coding forms into a single composite summarizing all coders’ responses on an Excel spreadsheet. Afterward, a consensus meeting was held with the coders and the first author to discuss the composite. The first author shared identified discrepancies among the coders in open and selective codings. Then, she led the coders to discuss among themselves to reach resolutions. At the beginning of the meeting, the coders were in 86% agreement. At the end of the meeting, the coders were in 100% agreement. The first author prepared a summary of the coders’ themes, which was shared with the four coders for final confirmation. Our results in this manuscript will include both the open and selective coding findings. Some open coding findings were also identified during the selective coding process. These findings will be summarized once in our “Results” section under the subsection selective coding for brevity. Finally, we believe that saturation was achieved in our study. After multiple focus group discussions were coded, the codes derived in later focus group sessions were redundant with earlier sessions. No new themes appeared to emerge from coders in the last five focus groups. Therefore, after coding eleven focus groups, the authors on this article and coders collectively decided that (1) we received sufficient data to address our research questions and (2) further data collection would likely not yield additional insights.
Descriptive analyses
Demographic
Data were normally distributed. Participants reported having an average of 1.83 (SD = 1.31) children. The average household size was 3.31 (SD = 1.86) and the majority of participants (52%) had a household income of below US$10,000 annually. Seven (8.75%) of participants reported being privately insured; 63 (78.75%) were publicly insured; 1 (1.25%) was not insured; and 9 (11.25%) data were unavailable. Table 1 displays the number of children, household size, income levels, and health insurance data.
Additional demographic data on the sample was obtained via city records. Data highlight that the neighborhoods from which the sample was drawn are racially homogeneous. Ninety-five percent of residents in these neighborhoods identify as Black and 11% identify as Hispanic or Latino. 62 Twenty-five percent of residents are college-educated. 63 The sampled neighborhoods are also considered high-crime areas by national standards, as one out of 14 neighborhood resident reports being a victim of a crime annually. 64
Results
Anxiety symptomology
Data indicate that participants were experiencing moderate levels of worry (M = 25.32, SD = 11.38) and distress (M = 21.86, SD = 7.14) and low levels of pregnancy-related anxiety (M = 1.90, SD = .60) prior to the start of the BBB SOS intervention (Table 2). Participants also reported experiencing race-related worries, ranging from low (0) to high frequencies (5). Eleven participants (13.75%) indicated that it was “very typical of [them],” a 5, to worry they may be treated or viewed unfairly to because of their race; 8(10%) reported a 4 rating; 12 (15%) reported 3, 9 (11.25%) reported 2, 11(13.75%) reported 1; 26 (32.50) reported it was “not at all typical of [them]” 0. Data of 3 participants were unavailable.
Summary of descriptive analyses.

PSWQ-A, Penn State Worry Questionnaire–Abbreviated; K-10, Kessler Psychological Distress Scale.
BBB SOS intervention completion
Eleven cohorts (N = 80) of BBB SOS were conducted between 2017 and 2019. Of the 80 participants in this study, 24 participated in the 11-week intervention, and 56 participated in the 7-week intervention. On average, participants attended four sessions. Thirty-six participants completed the focus group session. Forty participants (50%) were considered treatment completers, as they attended 50% or more BBB SOS sessions, which was pre-determined by our grant project objectives. Table 3 displays a summary of participants that completed approximately 25%, 50%, and 75% of the BBB SOS Intervention.
Summary of participant BBB SOS intervention completion.

BBB SOS Intervention Completion Cuttoffs by Group. Participants who were in the 7-week BBB SOS group: <25%–49% completion is approximately one to two sessions completed; 50%–74% completion is approximately three to four sessions completed; ⩾75% completion is approximately at least five sessions completed. Participants who were in the 11-week BBB SOS group: 25%–49% completion is approximately two to four sessions completed; 50%–74% completion is approximately five to seven sessions completed; ⩾75% completion is approximately at least eight sessions completed.
Focus group booklet responses
A paired sample t-test revealed an increase in knowledge about panic attacks (t(34) = 9.09, p < .001, d = 1.54) and stress (t(1, 34) = 6.12, p < .001, d = 1.03) after completing the sister circle (Table 4). In addition, participants’ responses suggested that they found all activities completed and skills learned in the sessions to be quite effective. Specifically, they reported high ratings for the development of a personal mission statement (M = 8.24, SD = 2.57), visualization exercise (M = 8.80, SD = 1.53), progressive muscle relaxation (M = 9.12, SD = 1.24), pregnancy yoga (M = 9.03, SD = 2.04), nutrition instruction (M = 8.70, SD = 2.14), cognitive restructuring (M = 8.19, SD = 1.81), and action planning (M = 9.12, SD = 1.41).
Comparisons of pre- and post-knowledge about panic attacks and stress.

The mean rating for participants’ overall experience was 9.60 (SD = 1.09), and the mean rating for comfortability with sharing was 9.69 (SD = .80). Finally, most participants (94.30%) indicated that they would be interested in participating in a sister circle in the future.
Open coding themes
Supportive environment
Open coding analysis of focus group responses indicated that the BBB SOS provided a supportive and non-judgmental environment. For example, one participant stated, “I can speak freely now. You know what I mean. Without fear of being judged.” Another woman expressed similar sentiments, “It brought a lot out of me . . . So it’s like I was comfortable in this setting to speak how I feel without being judged to get what I needed to get out.” Many participants attributed their comfortability in the group setting to the efforts of the facilitators. For example, participants commented, “I think the doulas made it very comfortable . . . to come and talk” and “In there, you’re not being judged. Like they don’t want nothing from you. Like they trying help you as much as you can and your situation that you’re about to go through.”
Openness
Another woman compared this group to ones that she participated in the past stating, “They went over and beyonder [sic] . . . this group made us feel, or made me feel more comfortable.” Others highlighted how the openness of the facilitators impacted their experience and encouraged them to be vulnerable and transparent. For example, one woman discussed a facilitator’s approach,
In this field they want to hear your story, but they’ll never tell you theirs and that’s where a connection is lost. But the minute she started talking, she shared her whole life story and that instantly got a connection.
Another woman shared a similar viewpoint and added that the facilitators normalized her experience: “I’m not the only one who goes through A, B, and C. Hearing different ways that they handle these situations . . . it gives me a whole new insight on things.”
Building a sisterhood
Focus group participants viewed the BBB SOS as a sisterhood. They reported, “We got our little bond together” and “You gain additional family . . . you create a definite bond with them. Everybody here that works here really been helpful and understanding.” Some expressed their appreciation for the support and their lack of that in prior experiences. For example, “It’s nice. It’s kind of building that community . . . I have a lot of strong Black women friends, but all of us live very far apart now, so I don’t have that.” Others discussed their admiration for being connected to women with similar experiences and challenges: “I’m the only one of my friends who has a child or who’s pregnant, so it was nice to be able to talk to other people who are pregnant like on a regular basis” and “I don’t have a whole bunch of moms. So I be in here trying to soak it up okay.”
Sharing experiences with others
Many focus group participants reported that they enjoyed their experience and would recommend BBB SOS to others in need. For example, “I would tell people about the sister circles and stuff because it’s like a support . . . we come here, and we know that we gonna be able to express ourselves . . . Gonna get to learn something. We gonna be getting some feedback.”
Other participants agreed and added, “Whether you’re a single mother or not, I mean everybody can get something from it,” and “Yeah, same here. I just be like ‘Girl you better get over there. Get those problems out. Girl they talk to you. You just get in the class, get with the program honey like. Just let them know.’” In addition to discussing the benefits of the group with close friends and family, one woman recommended it to her young pregnant clientele: “I think that they could use the information and use the support since they are so young. If they could get the skills now or at least get introduced to different components.” Additional findings related to positive experiences not only appeared in the open coding analysis but also reappeared in the selective coding analysis. These results will be outlined in the section below for brevity.
Selective coding
Learning/valuable
Psychoeducational
Sixty-six statements were related to identified benefits and valuable takeaways. Specifically, focus group participants reported enhanced knowledge about various psychoeducational topics after their participation in the BBB SOS. For example, they reported, “I could identify a panic attack from a mile away” and “I think I learned a lot more about stress and anxiety.” Another expressed that she valued the information she received about nutrition during pregnancy and postpartum: “When you’re pregnant, a lot of things change and what you can and cannot eat is one of them. So getting that professional opinion on what is good for us.”
Applying coping skills
In addition, focus group participants reported that BBB SOS sessions facilitated their identification of emotions and triggers and implementation of adaptive coping skills. For example,
I was able to let go in the beginning when we talked about stress, family, and things like that. I was able to let go of some of the stresses and let go of a couple more stresses so now I feel like I’m carefree and I have a lot more freedom.
Similarly, one woman explained that she was able to manage her emotions in an effective manner and “stop [the anger] before it gets too bad.” In regard to identifying triggers, one woman stated, “It was an eye opener because it’s one thing to feel stressed. It’s another thing to be able to express why you feel stressed . . . When you’re able to kind of pinpoint what’s triggering your stress, you’re able to then find coping skills to match your stressors.” Finally, another woman stated that visualization exercises “recentered” her and assisted her ability to manage parental stress.
Instructional materials and activities
Text
Many focus group participants commented on specific activities and the related impact on their learning or skill development. One woman explained that the Soothe Your Nerves text aided in her understanding of stress and offered normalization. She stated, “It defines [stress] in a way that is unique, and it doesn’t make it seem to be like this outcasted feeling.”
Build Your Own Theme Song
The focus group participants also reported favorable opinions about the BYOTS activity improving their ability to reframe their negative beliefs. Specifically, some participants alluded that their theme song helped them remain hopeful during times of adversity. For example, “I think everyone having an individual theme song . . . is very helpful because it gives you assurance and it gives you that boost of self-confidence that everybody needs.” Another woman added, “The theme song, I personally had one gospel song . . . I think it is very helpful.”
Yoga
Multiple participants reported that the pregnancy yoga activity alleviated stress. One woman stated, “I think that yoga is a really good stress reliever for me personally. I like to stretch, and I’ve always found it to kind of be really relaxing.”
Action planning
Focus group participants found the action plan activity to be a simple and effective tool for setting goals and increasing adaptive and decreasing maladaptive behaviors. One woman explained that the activity helped her “break things down” to the point that it made tasks “seem less severe.” Another woman added, “[Action planning] would help somebody who never set a goal before . . . so they could just go back and make a plan.” Some focus group participants attributed the action plan to increasing their motivation and commitment to goal directed behavior. For example, “It gave me a vision. It helped me see something to look forward to ‘cause I didn’t. It gave me another goal to see that.” Others commented in agreement:
That’s like my biggest thing is, like I could set a goal, but I’ll never stick to it so being in this class kinda taught me how to stick to my goals and make a game plan and plan of management.
Improved mood
Findings showcased that the focus group participants reported participation in BBB SOS increased behavioral activation, mood, and functioning and facilitated personal growth and self-empowerment. For example, one woman stated, “Having a sister circle that you like dedicated to every week, it make you feel better leaving the house every week, especially being a stay-at-home mom and everything.” In addition, one woman verbalized her increased ability to effectively process her anger: “Just like knowing what triggers is and how to refrain from just cussing people out . . . I think that’s just pretty much where I came from.” Another woman stated that she can now manage her internalizing symptoms: “I’m in a better place . . . becoming a better person,” and “Us talking about depression and things we’ve been through. It definitely helped out in those areas.”
Empowerment
The focus group participants underscored that their participation helped change their perspectives on their circumstances, others, and the environment. For example, one woman stated,
I have more knowledge of my situation and I have more information as far as what I’m going through that can take me in my day-to-day life with my child. I’m fully aware of things that I wasn’t. I have a little bit more confidence . . . this situation helped me a lot me ‘cause I stay by myself. It helped a lot with that and to better open up myself up a little bit more so I wouldn’t be so closed minded to things that I was before.
Another woman shared a similar realization about how the sister circle influenced interactions with her mother. For example,
[My mom] has panic attacks and anxiety so . . . I told her about the book. It helped with our relationship and our bonding because . . . this is what we needed our whole life. It made a difference in my life because it was something I didn’t see that needed more focus.
In addition to changing perspectives, some participants specifically noted an increase in positive thinking:
I just really like the feeling. It was just really nice, and it gave us a different view of ourselves and everything. How to make ourselves more positive and not think of the negative in every situation. It made us more confident.
Family and community impact
One woman concluded that her participation in BBB SOS helped her and others in her family: “I actually helped a lot of people now. Like my sisters and them. They know how to open up and how to talk about things.” Another woman shared her beliefs about the impact BBB SOS could have on the Black community and family unit:
I think that they could use the information and use the support since they are so young. If they could get the skills now, or at least get introduced to different components, read the book, come to class, or see an environment where black women aren’t just fighting each other . . . they would set a good tone for their family that they’re making.
Feasibility
Forty-two statements were related to feasibility aspects, specifically the structure and flow intervention and format of sessions. Participants varied in their opinions about the length and timing of the sessions. Many reported enjoying the incorporation of various materials and activities to increase their skill building and understanding of anxiety or panic. Some participants wanted a wider range of discussion topics:
We always talked about how we done broke up, and that we may be mad at each other. So how are we going to coparent? See I came in and I was like, ‘That’s not my life. That’s not my reality.
In addition, some commented on the varying levels of participation from participants: “I guess the participation kinda dwindled as we progressed in the program,” and “See some people kind of get bored. And them younger girls, y’all have to try to find a way to draw those younger girls in and keep them here.”
Discussion
The present study utilized a mixed-methods framework to evaluate the feasibility and acceptability of BBB SOS, a manualized culturally relevant stress and anxiety intervention, for pregnant and postpartum Black women. To the best of our knowledge, we are the first to utilize a sister-circle intervention with a Black perinatal sample. Quantitative and qualitative study findings supported our hypotheses. Data showcased that participants reported increased perceived knowledge about stress, anxiety, panic attacks, and emotional triggers and their ability to identify such feelings and events and manage them effectively using CBT coping strategies.
Focus group participants described their overall BBB SOS experience as positive, empowering, and enriching. They found the environment and group dynamic supportive and enjoyed connecting with individuals experiencing similar milestones and adversities. This finding is consistent with other studies that employed sister circle frameworks.20,26 –28,65
Focus groups reported that session activities increased their motivation for behavior change, encouraged planning and goal setting, and increased support and behavioral activation, ultimately contributing to their reported improved mood. This aligns closely with well-documented evidence of the effectiveness of CBT approaches in treating anxiety and depression.33,66 Participants also reported mixed feelings about session length and group-member participation, which have been common critiques made by individuals participating in group-based interventions. 67
The present study revealed several noteworthy findings. First, our study had a 39.4% enrollment rate. Evidence shows that community participatory-based research studies that utilize samples of low-income individuals, racial minorities, or perinatal women traditionally face significant recruitment and enrollment barriers.68,69 There were limited data on the enrollment rates of low-income Black perinatal samples. However, multiple marginalized sample-specific factors would likely contribute to lower enrollment rates.
We attribute our enrollment success to participants’ established relationships with doulas prior to study enrollment. Participants were familiar with receiving resources from their doulas and valued their referrals and recommendations. In addition, cumulatively, our doula facilitators have over 35 years of experience working with this population. This likely was beneficial to our study as they were the first point of contact for participants and could communicate project objectives in a culturally-receptive manner. Also, we believe our study compensation was viewed favorably by prospective participants. Our study compensations included Walmart gift cards, yoga mats, and food storage containers. These were not miscellaneous incentives but were linked to population-specific needs and/or topics and activities discussed in BBB SOS. They showcased that our team cares about participants’ experiences during pregnancy and motherhood and wants to aid in reducing their financial and health burdens.
Second, multiple participants reported that they held the research team and facilitators in high regard, which is uncommon among Black research participants. Despite previous study findings of cultural mistrust of healthcare workers and researchers due to historical injustices 70 even when staff included racial minorities or Black women, 71 our focus groups commented that the BBB SOS facilitators’ transparency and authenticity created a safe space and atmosphere of trust. This development may be due to our facilitators’ willingness to use self-disclosure. Some clinicians strongly discourage the use of self-discourse of personal details in attempts to uphold concrete professional boundaries between the therapist and the client.72,73 However, this can have an adverse effect. By continually prompting clients to be vulnerable, without sharing on the therapist’s part, clients may become disconnected and frustrated by the overt power differential. We believe our facilitators’ use of self-disclosure followed by modeling techniques of identifying and labeling emotions, quickly set the therapeutic framework for our participants. Our data suggest that self-disclosure may be particularly helpful when working with Black women, as they report feeling alienated, dismissed, and ignored in their health encounters.
In addition, Black women are aware of their marginalized and often powerless disposition, which is only amplified in a therapeutic setting. Self-disclosure may help create authentic conversations, resulting in careful attentiveness from staff and active participation from Black women. In addition, we believe our facilitator-led discussions that utilized storytelling to self-disclose, a common cultural practice among Black individuals,74,75 promoted group connectedness and shaped a sister-like dynamic. Collectively, these factors helped increase participants’ confidence in the facilitators and their instruction.
Third, the group dynamic of Black female facilitators and peer support sharply contrasts with participants’ frequent experiences of marginalization and rejection linked to racism and sexism in modern-day society. 76 BBB SOS likely fosters feelings of belonging, security, and safety, as all staff members and group participants identify as Black and female. These racial and social components embedded in the structure of BBB SOS potentially decrease participant anxiety and stress intuitively. Research indicates that Black individuals in predominately White spaces experience increased stress and anxiety.77,78 Some of these responses may be linked to anticipating and experiencing frequent microaggressions in these spaces. 79 However, others may be related to the fear of being a victim of a hate crime, such as physical or sexual violence that could be potentially life-threatening or fatal.80 –82 Experiences of stress and anxiety are also likely to present among groups of other races or ethnicities, given the pervasiveness of anti-Black racism. 83 Similarly, studies of Black women report within racial group conflict and tensions due to gender-based stereotypes, suggesting that all-female support groups may be preferred.84,85
Fourth, participants perceived the culturally-tailored and traditional CBT-based activities to be effective in managing stress and anxiety. Multiple participants reported enjoying the BYOTS Song musical cognitive restructuring activity. Some explained that they chose familiar gospel songs with uplifting and encouraging lyrics, prompting them to decrease their overall negative thinking. Prior research supports this finding, as music and spirituality often promote resiliency and serve as protective factors for Black individuals against poor mental health outcomes.20,75,86,87 Participants also expressed appreciation for a traditional CBT action plan worksheet activity that utilized a step-by-step outline approach. They noted that it reduced their hopelessness and helped them identify a path to change. Previous studies highlight mixed findings regarding individuals’ receptiveness to using worksheet-based activities in therapy.88,89
Finally, participants reported that they believed the assigned psychoeducational text, Soothe Your Nerves, enhanced their understanding of topics and the development of CBT skills. In contrast to our findings, previous studies revealed that participants often do not complete their assigned homework or complain about having additional work outside of the group.90,91 An explanation for our finding is that the utilized text readings were recommended, not mandatory. In discussion, facilitators asked people if they read the text, provided chapter summaries, and led discussions related to skill development and application. It’s possible that BBB SOS participants enjoyed group discussions and completed assigned readings to contribute actively and have enriching group discussions.
Limitations
The present study is not without limitations. We could not collect data from participants who stopped attending BBB SOS sessions, which may have highlighted additional treatment barriers and provided valuable recommendations for future interventions. A second limitation is that our BBB SOS doula facilitators served dual roles for participants. As part of their job with our community partners, they provided perinatal support. Methodologically, this limits the generalizability of our data to situations where this dual role is not present. Clinically, however, this decision likely increased participant trust and the development of positive rapport. This dual role likely has a similar clinical strength as when individual therapists encourage their clients to participate in group therapies that the therapist facilitates.92,93
Implications
Despite these limitations, the clinical implications of this study’s findings are promising. For example, the BBB SOS culturally relevant framework may aid Black women in understanding and mastering CBT concepts and skills. Previous research outlines that Black individuals are likely to struggle to apply CBT skills despite being the leading modality in mental health treatment. 94 Studies suggest that most intervention approaches fail to teach in a culturally sensitive manner. 95 However, the BBB SOS intervention created a sense of sisterhood akin to those already present in the Black community, which likely made learning new CBT approaches and techniques less daunting for group members, given participants’ perceived helpfulness. Moreover, research shows that individuals are more likely to try new behaviors and take risks with family or friends in a supportive and nurturing environment. 96
Future directions
Future studies should document various maternal mental health outcomes of Black women before, during, and after the sister circle to thoroughly and comprehensively investigate the mental health impact of BBB SOS or other CBT interventions that utilize sister circles. Studies incorporating sister circles may also want facilitators to cover specific session topics that complicate pregnancy and postpartum, including domestic violence, custody issues, grief, and COVID-19-related stressors.97 –99 Role-playing activities could help increase interpersonal effectiveness among participants, friends, and family and navigate racial mistreatment at doctor offices and hospital settings.100 –102 Finally, incorporating journaling activities may help quieter and shyer participants engage in group activities and be motivated to share their experiences. 103
Sustainability plan
As we continue to implement BBB SOS, we regularly invest in efforts that promote sustainability and meet the multitude of needs of our target population. Our project staff reviews data from each focus group discussion, paying particular attention to concrete critiques or suggestions noted by participants. We also request feedback from our facilitators. Then, we actively incorporate their feedback in our following BBB SOS groups as applicable. We polled participants for our most recent group to identify a convenient meeting time before finalizing a schedule. In addition, we prompted our independent reviewers to assess our facilitators’ efforts to be lively and maintain the group’s interest. This component was recently added to enhance our fidelity checks.
We implement weekly group supervision throughout the intervention and provide training reviews upon request from doula facilitators or if our clinical psychologist identifies a need. We also conduct biannual meetings to review the cohesiveness and practicability of the BBB SOS curriculum, intervention materials, and staff resources.
Finally, we regularly disseminate our BBB SOS development, experience, and findings. Our team presents at community events and regional, national, and international conferences featuring our community-based participatory research, which includes Black female lay individuals (e.g. perinatal doulas, cosmetologists) and researchers and clinicians (e.g. doctoral students and licensed clinical psychologists). These efforts allow us to (1) educate audiences about the mental health and physical health risks and needs of Black pregnant women, (2) present our innovative efforts to address our population-specific needs using cultural-infused strategies and components, (3) showcase our participants’ experiences, and (4) exchange information from other researchers. We have effectively utilized these exchanges to foster new collaborations and partnerships and obtain additional funding for our work.
Conclusion
Too often, Black women and their children suffer due to systemic racism, and their needs are not prioritized in mental health care settings. The present study aimed to address these problems by developing a culturally relevant stress and anxiety intervention for Black pregnant and postpartum women, prioritizing their needs and perceptions in our study design and objectives. Our findings highlight that doula-led peer-supported interventions are practical, feasible, and acceptable to Black perinatal women. We believe our existing community partnerships, use of lay Black female doula facilitators and peer supports, and interactive curriculum with comprehensive psychoeducation and concrete strategies to address general pregnancy-related anxieties and race-related worries contributed significantly to our enrollment success and overwhelmingly positive feedback from BBB SOS participants. We hope to see others invest in similar cultural considerations when developing public policy, designing research, and treating clients. More specifically, we challenge others to employ an iterative process of asking and listening to Black women. This validates their experience, gives them a voice and power, and creates a safe space to receive helpful mental health information and resources. Collectively, these actions work to combat the mental and physical health effects and realities of systemic racism for Black women.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231185405 – Supplemental material for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women
Supplemental material, sj-docx-1-whe-10.1177_17455057231185405 for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women by Keaton Somerville, Tiffany Rowell, Robert Stadulis, Debra Bell and Angela Neal-Barnett in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231185405 – Supplemental material for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women
Supplemental material, sj-docx-2-whe-10.1177_17455057231185405 for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women by Keaton Somerville, Tiffany Rowell, Robert Stadulis, Debra Bell and Angela Neal-Barnett in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231185405 – Supplemental material for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women
Supplemental material, sj-docx-3-whe-10.1177_17455057231185405 for An evaluation of the feasibility and acceptability of sister circles as an anxiety intervention for pregnant Black women by Keaton Somerville, Tiffany Rowell, Robert Stadulis, Debra Bell and Angela Neal-Barnett in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.