
Abstract
Pelvic actinomycosis with an intrauterine device accounts for approximately 3% of all actinomycoses. It is a chronic infectious disease characterized by infiltrative, suppurative, or granulomatous inflammation, sinus fistula formation, and extensive fibrosis, and caused by filamentous, gram-positive, anaerobic bacteria called Actinomyces israelii. The slow and silent progression favors pseudo tumor pelvic extension and exposes the patient to acute life-threatening complications, namely colonic occlusion with hydronephrosis. Preoperative diagnosis is often difficult due to the absence of specific symptomatology and pathognomonic radiological signs simulating pelvic cancer. We discuss the case of a 67-year-old woman who complained of pelvic pain, constipation, and weight loss for 4 months, and who presented to the emergency department with a picture of colonic obstruction and a biological inflammatory syndrome. The computed tomography scan revealed a suspicious heterogeneous pelvic mass infiltrating the uterus with an intrauterine device, the sigmoid with extensive upstream colonic distension, and right hydronephrosis. The patient underwent emergency surgery with segmental colonic resection and temporary colostomy, followed by antibiotic therapy. The favorable clinical and radiological evolution under prolonged antibiotic therapy with the almost total disappearance of the pelvic pseudo tumor infiltration confirms the diagnosis of pelvic actinomycosis and thus makes it possible to avoid an extensive and mutilating surgery with important morbidity.
Introduction
Actinomycosis is a rare, chronic, infectious disease characterized by infiltrative, suppurative, or granulomatous inflammation, sinus fistula formation, and extensive fibrosis and caused by filamentous, gram-positive and anaerobic bacteria called the A israelii, described for the first time by Israel in 1978.1,2 Actinomycosis occurs most commonly in the cervicofacial region (50%–65%), followed by the thoracic (15%–30%) and abdominopelvic (20%) regions but rarely involves the central nervous system. 3 Pelvic actinomycosis accompanied by intrauterine device (IUD) accounts for about 3% of all actinomycosis. 4 Although uncommon, a long duration of IUD appears to confer the greatest risk. 1 The rarity of this pathology, the absence of specific symptoms as well as the pseudotumoral clinical and radiological presentation makes preoperative diagnosis raise a challenge.
Case presentation
A 67-year-old woman, gravida 3 para 3 with no preceding chronic disease or constant medication complained of increasing pelvic pain and constipation associated with weight loss and fatigue for 4 months. The patient’s medical history included the insertion of a copper IUD 30 years ago. The patient was referred to emergency for the worseness of abdominal pain and distension with a frank cessation of intestinal transit and vomiting suggesting a neoplasic intestinal occlusion.
At admission, the vital signs were stable, and the patient was apyretic. Physical examination revealed a mild tenderness at the lower quadrants with abdominal distension without a palpable mass. No signs of inflammation in the cervical or vaginal mucosa were found on gynecological examination. Laboratory investigations demonstrated anemia (hemoglobin: 9 g/dL), raised C-reactive protein (CRP) at 140 mg/L, and high white blood cell (WBC) count (12.3 × 103/μL). Serum levels of carcino-embryonic antigen (ACE) and CA19-9 and CA 125 were also within the normal range.
The abdominopelvic computed tomography (CT) revealed a 75 × 61 mm heterogeneous pelvic mass with poorly defined margins comprising cystic areas and involving the uterus with an IUD, adnexa, and rectosigmoid colon, which caused right hydronephrosis by compression on the ureter and important colonic distension (Figure 1).

Pretreatment CT scan with an injection of contrast product: (a) coronal section: poorly limited heterogeneous pelvic mass comprising fluid compartments encompassing the uterus with an intrauterine device (yellow star) and compression of the right ureter (red arrow) responsible for significant dilation of the urinary cavities. (b) Oblique coronal slice and (c) axial slice: heterogeneous pelvic mass sheathing the sigmoid (red arrow) with significant colonic distension.
Initial treatment consists of fluid resuscitation of the patient, correcting the electrolyte abnormalities, and gastrointestinal decompression with a nasogastric tube placed to suction, as well as close monitoring of urine production. Due to the deterioration of her symptoms, the inflammatory syndrome, the debutant renal failure, and hydroelectrolytic disorders she required an emergency surgical procedure.
We performed exploratory laparotomy for debulking. The intraoperative findings were no ascites and no obvious abnormalities in the peritoneum or the surface of the intestine of the middle abdomen. There was a pelvic mass conglomerated with the uterus, adnexa, and distal colon with tight adhesion between the mass and pelvic organs including the small and large bowels and the bladder which could not be dissected out. It involves the right ureter, the rectosigmoid, and caused ureteral dilatation and significant colonic distension with signs of early ischemia. Dissection into the pelvis was impossible due to inflammatory phenomena giving an appearance of pelvic shielding and surgery was considered to be debilitating and morbid in this emergency setting. Based on these findings, a locally advanced ovarian process has been suggested; we performed decompression of the bowel with proximal loop colostomy.
After 2 weeks of metronidazole 4 × 500 mg intravenous (IV) and ceftriaxone 1 × 2 g IV treatment, her WBC was 7500 mm3/mL and CRP was 10 mg/dL. She was then switched to oral amoxicillin 500 mg three times daily. A repeat CT scan, after 4 weeks of antibiotic therapy, showed a resolution of the right hydronephrosis and a reduction in the volume of the pelvic mass with the persistence of a latero-uterine fibrous residue (Figure 2). Post-operative endoscopy did not reveal any suspicious intramucosal lesions. The initial clinical and radiological presentation, as well as the favorable evolution under antibiotic therapy, were considered to support the diagnosis of pelvic actinomycosis and justified the continuation of oral antibiotic therapy for 6 months. She had neither gynecologic nor bowel complaints during the follow-up period until the reversal of the colostomy.
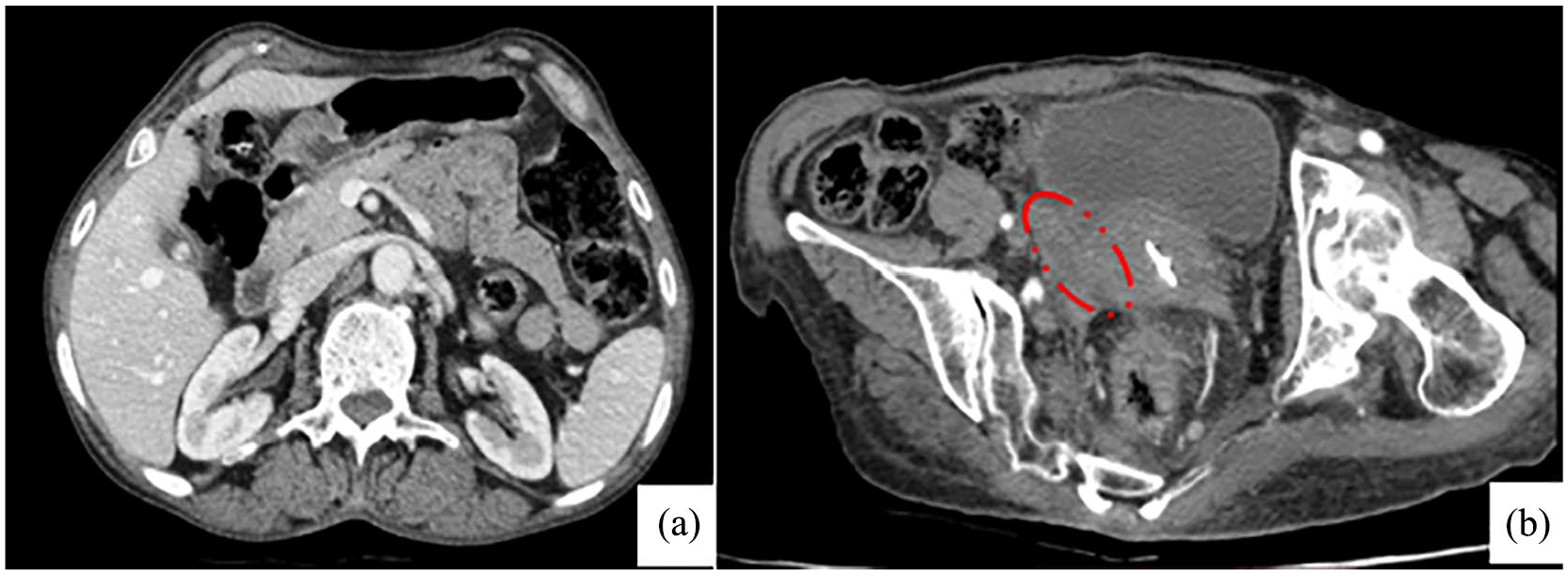
CT scan with an injection of contrast product after antibiotic treatment. Axial section (a) shows the regression of the dilation of the right renal cavities and (b) of the size of the pseudo pelvic mass with the persistence of a right latero-uterine fibrous residue (red dashed circle).
Discussion
Pelvic actinomycosis is considered to be a rare disease, although the use of IUDs can promote its appearance and was identified as a predisposing risk factor. The colonization rate increases with the duration of its maintenance.2,5 Vasilesco et al. 6 reviewed the medical records of 28 patients with abdominopelvic actinomycosis (9 men and 19 women) and the cause of actinomycosis in the studied group was an IUD device in 17 cases from which, 6 patients were admitted because they mimicked a complicated abdominopelvic malignant ovarian advanced ovarian cancer. To reduce the occurrence of this affection, it is recommended that IUDs be changed periodically, every 3–5 years. Nevertheless, some patients may be affected even after the removal of an IUD because of various degrees of endometrial damage caused by stimulation from the IUD and flora disorders. 7
The clinical presentation is variable depending on the primary site and the duration of the infection and represents a challenge to clinicians in distinguishing pelvic actinomycosis from intraabdominal or pelvic malignancies. However, common symptoms include abdominal pain with or without palpable mass, body weight loss, fever, constipation or diarrhea, vaginal discharge, and symptoms related to bowel obstruction or obstructive uropathy.8 –11 In our cases, abdominopelvic pain associated with weight loss constituted the prominent chronic symptoms preceding bowel occlusion.
Laboratory parameters commonly revealed anemia, leukocytosis, high values of CRP, and elevated erythrocyte sedimentation rate which was the case with our patient.12,13 Moreover, some authors reported that tumor marker values like CA125 and alpha-fetoprotein are usually within the reference ranges or slightly elevated. 11
The positive diagnosis is bacteriological and/or pathological. 14 However, bacteriological diagnosis is difficult due to the sensitivity of Actinomyces to oxygen, the difficulty of its culture, and its frequent association with other anaerobic bacteria; in fact, its identification is only made in 50% of cases.14,15 It has been reported that the rate of preoperative diagnosis is less than 10% and most were diagnosed posteriorly on the anatomopathological examination surgical specimen obtained after the performance of a laparotomy or a laparoscopy to evaluate the suspicious pelvic mass.7,16
Despite the lack of diagnostic specificity, the role of the CT scan remains essential to evoke the diagnosis of pelvic actinomycosis, to specify its extent and its impact on the neighboring organs, and to evaluate the effectiveness of the treatment. CT scan results of an infiltrating abdominopelvic mass without border limits and increased heterogeneous contrast may suggest actinomycosis, especially in patients with fever, leukocytosis, or predisposing factors. 6 Triantopoulou described the different aspects of abdominopelvic actinomycosis of 18 patients on cross-sectional imaging and indicated discriminative findings from other inflammatory or neoplastic diseases. In this study, 11 female patients had a history of using IUDs and CT findings confirmed the infiltrative nature of the disease, which tended to invade across tissue planes and boundaries. In 11 patients, an inflammatory mass involving the uterus and ovaries was revealed. 10 In 17 cases, peritoneal or pelvic mass involving the bowl appeared to be predominantly cystic and heterogeneously enhanced which was the same radiological presentation of our patient. The authors suggested that this radiological aspect reflects the histologic features of actinomycosis: central suppurative necrosis surrounded by granulation tissue and intense fibrosis. Moreover, many authors reported that hydronephrosis with ureteral obstruction is related to the presence of an IUD in most cases and can be relieved by antibiotic medication and transient insertion of a ureteral stent.9,11,17 –19 Lee et al. 20 assessed the radiological feature of 18 of gastrointestinal actinomycosis and reported perirectal, pericolic, or pericentric infiltration in 17 patients (94%). Moreover, the urinary tract was involved in 9 patients (50%), with hydronephrosis and hydro-ureter in 6 and hydro-ureter in 3; in all of these patients, ureteral obstruction was caused by the extension of the peritoneal or pelvic mass or inflammatory infiltration. These findings confirm the aggressive behavior of this disease simulating a malignant process. Such a pattern may be attributed to the proteolytic enzyme produced by A israelii. 2 Moreover, some investigators suggested that patients with elevated CRP, decreased hemoglobin, increased erythrocyte sedimentation rate, and slightly increased CA125 can have renal pelvis dilation or hydronephrosis. 7 Our patient presented anemia and elevated CRP with normal tumor marker and the CT scan had objectified the local urinary and digestive impact of actinomycosis resulting in hydronephrosis and colonic occlusion. Another interesting radiological finding in our patient was the absence of lymphadenopathy contrasting with the initial appearance evoking locally advanced ovarian cancer which supported the diagnosis of actinomycosis. Regional lymphadenopathy is uncommon or develops late as the organism of actinomycosis usually does not spread via the lymphatic system because of the size of the bacterium.10,20,21
The usual treatment of actinomycosis is based on high and prolonged doses of penicillin G (20 million units per day) or amoxicillin for 4–6 weeks, followed by penicillin V (4 g per day) orally for 6 to 12 months. 13 In case of penicillin allergy, macrolides, cyclins, or rifampicin can be used. In addition, it has been observed that actinomycosis is also sensitive to third-generation cephalosporins, ciprofloxacin, and trimethoprim-sulfamethoxazole.5,8,22 Surgical treatment is usually proposed due to the difficulty in diagnosis and also in case of persistent disease and the occurrence of complications such as bowel obstruction and fistula.13,22 This combination of surgery and antibiotics results in healing in the majority of cases (Table 1) which was the case of our patient as the colostomy was indicated to remove the occlusion, and the antibiotic therapy had made it possible to treat inflammatory and infectious phenomena and to free the urinary tract.
Case report studies on pelvic actinomycosis.

IUD: intrauterine disposif; CT: computed tomography; MRI: magnetic resonance imaging; US: ultrasound; IV: intravenous.
Through our case, we raise the interest of adequate radiological explorations allowing evoking the diagnosis of actinomycosis in face of an infiltrating pelvic mass mimicking a locally advanced tumoral carcinogenic process, especially in the context of the inflammatory syndrome and long-disposed IUD. Our diagnostic and therapeutic approach made it possible to avoid an extirpative and extensive surgery.
Conclusion
Pelvic actinomycosis is a rare pathology that should be considered in any woman with an IUD for several years and who presents with deterioration in general condition, an inflammatory syndrome, and a pelvic tumor syndrome. Ignorance of this entity can lead to a diagnostic delay with the risk of the occurrence of serious complications requiring surgical management. The diagnosis is often histological and could be evoked with adequate radiological exploration. The treatment is essentially medical and based on long-term antibiotic therapy and surgery should be indicated for complicated cases, such as bowel obstruction or unusual radiological presentation of cancer.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231181009 – Supplemental material for Pseudo tumor pelvic actinomycosis revealed by colonic obstruction with hydronephrosis: Can extensive surgery be avoided? A case report
Supplemental material, sj-docx-1-whe-10.1177_17455057231181009 for Pseudo tumor pelvic actinomycosis revealed by colonic obstruction with hydronephrosis: Can extensive surgery be avoided? A case report by Houyem Mansouri, Ines Zemni, Malek souissi, Houda Henchiri, Sabrine Boukhris, Mohamed Ali Ayadi and Leila Achouri in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.