
Abstract
Background:
As the awareness towards gender-specific therapies continues to increase among all fields of medicine, so does the need for gender-sensitive evaluations of established surgical techniques. With a higher likelihood of anterior cruciate ligament injury in women, a critical assessment of the functional outcome of anterior cruciate ligament reconstruction regarding patient sex is indispensable. Almost all pre-existing literature on this subject is based on anterior cruciate ligament reconstructions carried out before 2008, when ‘all-inside’ techniques did not exist. This implicates the need to investigate this technique towards its differences in outcome between male and female patients.
Objectives:
The purpose of this study was to determine whether there is a difference concerning the functional outcome of an ‘all-inside’ technique for anterior cruciate ligament reconstruction in female patients when compared to a cohort of male patients matched for body mass index and age.
Design:
Retrospective analysis.
Methods:
All female patients who underwent anterior cruciate ligament reconstruction using an all-inside technique between 2011 and 2012 were examined for inclusion. Functional outcome parameters investigated included the Lysholm Knee Score, International Knee Documentation Committee score, Visual Analogue Scale score and the Tegner Activity Scale. All parameters were documented before surgery and at 3-, 6-, 12- and >24 months follow-up. At 24-month follow-up, anterior–posterior knee laxity was tested using the KT-2000 arthrometer device. For comparison, an equivalent group of male patients who underwent the same procedure was matched.
Results:
27 female patients were matched with 27 male patients. The average age was 29 years, and a mean follow-up of 90 months could be achieved with 27 of patients reaching a follow-up of > 10 years. The evaluated scores showed no significant difference between female and male patients. Women presented with poorer functional outcome at 3- as well as 6-month follow-ups compared to men, without reaching statistical significance. After 12 months, no further differences could be found.
Conclusion:
This study proved that an all-inside technique for anterior cruciate ligament reconstruction is able to produce the same functional outcome in female as in male patients at long-term follow-up. The results on short-term outcome indicate the need for further research towards gender-specific differences after anterior cruciate ligament reconstruction, their potential causes and potential of improvement.
Level of evidence:
Level III, retrospective comparative study.
Background
Anterior cruciate ligament (ACL) reconstruction is among the most common procedures performed in orthopaedics, with more than 250,000 ACL-reconstructions (ACL-Rs) performed annually in the United States alone.1,2 Female athletes have been shown to present with a two- to nine-fold higher risk of ACL rupture compared to male athletes.3–5 Multiple factors have been proposed to account for this variation in ACL rupture rates, including differences in anatomy (e.g. increased posterior tibial slope and decreased notch width in women), hormonal factors, and an increased prevalence of deficits in dynamic neuromuscular control of the knee in females.1,4,6
Although techniques for ACL-R have evolved tremendously over the past decade,7–9 mainly to better restore the native ACL anatomy and knee joint kinematics, the influence of patient sex on the outcome after ACL-R remains unclear, with some authors reporting poorer outcomes in female patients 10 and others noting no difference. 11 A recent systematic review of Tan et al. 1 revealed poorer results in terms of subjective and functional outcome scores for female patients compared to male subjects. These findings are in contrast to the systematic review of Ryan et al. 12 in which the authors demonstrated similar results after ACL-R for both groups.
However, all systematic reviews comparing sex-related outcomes after ACL-R1,12,13 mainly consist of studies published prior or around the year 2008, at a time where the conventional trans-tibial technique for the creation of the femoral tunnel was widely used. Biomechanical studies have shown that the trans-tibial technique can result in non-anatomically femoral bone tunnels, which may not restore native knee joint kinematics.14,15 Furthermore, Van Eck et al. 16 showed that a majority of studies on ACL-R do not describe in detail how and where exactly the femoral tunnel was placed. As a result, an assumption on whether the femoral tunnel was placed within the native ACL insertion site or not is not possible. The new all-inside technique used with patients of this study enables the surgeon to place the femoral tunnel closer to the native ACL insertion site, therefore, promising a more anatomical restoration of knee kinematics. Furthermore, promising results for the all-inside technique have been reported, especially in younger patients and regardless of graft choice.17,18 As young females are showing a significantly elevated risk for ACL injury 5 this sub-group might be particularly suited for the all-inside technique.
The objective of this retrospective study was to determine whether this new technique of ACL-R is able to produce the same results concerning functional outcome at mid-term follow-up in female patients when compared with male patients.
It was hypothesised that, following an ‘all-inside’ ACL-R, female and male patients exhibit no differences in objective and patient-reported outcome scores.
Methods
A retrospective analysis of data of 27 female and 27 male patients who underwent primary, anatomic single-bundle ACL-R using the all-inside technique between January 2011 and December 2014 was performed. All surgical procedures were performed by one experienced, sports-medicine fellowship trained orthopaedic trauma surgeon or under his guidance.
Subsequently, patients were matched for age at the time of surgery and body mass index (BMI) into two groups (group A: males and group B: females). The inclusion criteria were as follows: 1 primary ACL-R using the all-inside technique and Wilson et al. 19 minimum of 2 years of clinical follow-up. Patients who were younger than 18 years of age, those undergoing a multi-ligamentous knee reconstruction or ACL revision surgery, patients with a history of ACL injury or rupture of the contralateral ‘healthy’ knee and those who presented with chondral lesions greater than grade 2 according to the Outerbridge classification 20 and additional injuries to the collateral ligaments greater than grade 2, diagnosed on either magnetic resonance imaging (MRI) findings or during arthroscopy, were excluded from the analysis.
Surgical technique
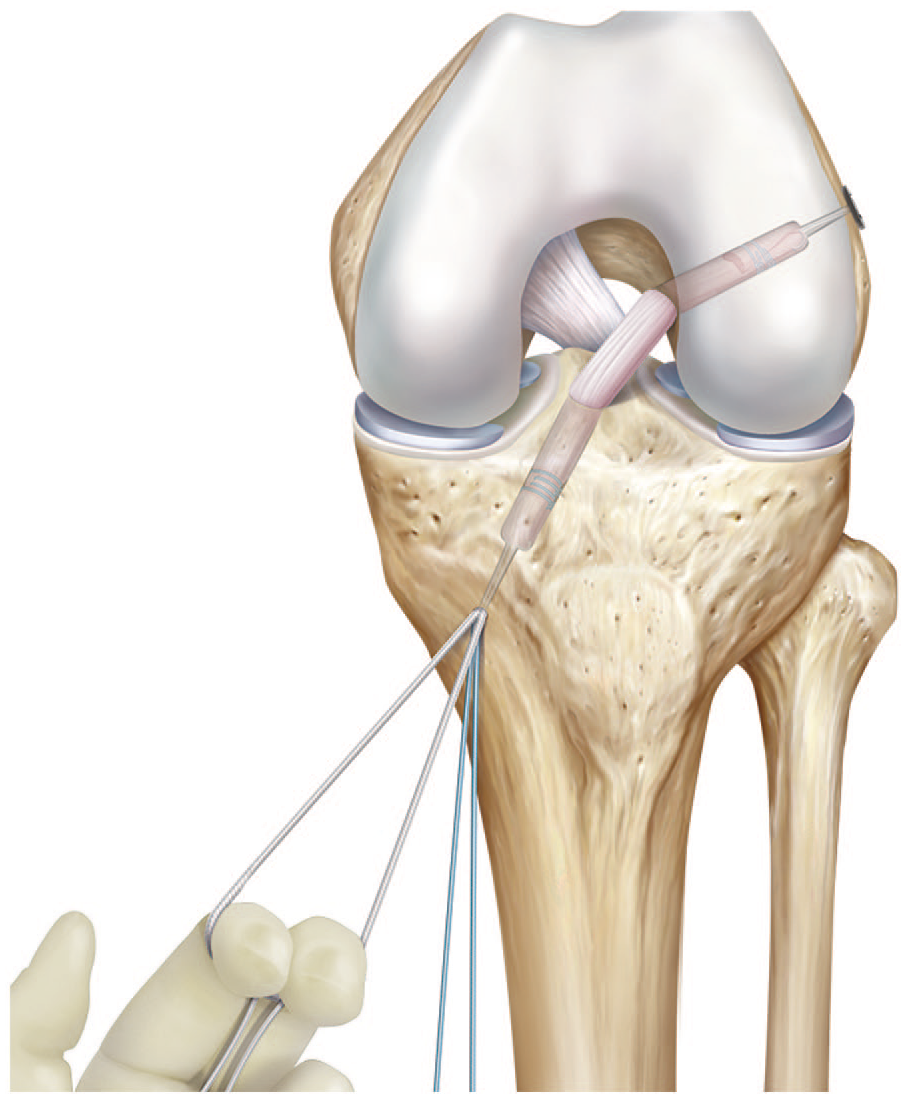
All patients underwent anatomic ACL-R using the all-inside technique as described previously by Wilson et al. 19 Following standard arthroscopy to confirm a complete tear of the ACL and treatment of associated meniscal and cartilage lesions, the semitendinosus tendon (ST) was harvested through a small incision over the pes anserinus. The tendon was then loaded onto two adjustable suspensory devices (ACL TightRope RT®; Arthrex, Naples, FL) and quadrupled to make a GraftLink® (Arthrex, Naples, FL). 21 The femoral socket was created by a FlipCutter® (Arthrex, Naples, FL) to create a ‘socket’ by outside-in drilling (Figure 1) at the centre of the native ACL footprint, at the midpoint between the anteromedial (AM) and posterolateral (PL) 19 bundle. The socket was routinely drilled to a depth of at least 20 mm. The tibial socket was created using the same technique, with the tibial aiming device placed in the middle between the AM and PL positions, resulting in an incomplete bony socket in average 35 mm long (Figure 2). The socket size was based on the measured diameter of the soft-tissue graft. Through the AM portal, the femoral TightRope RT® was pulled through to fully seat the graft within the femoral socket (Figure 3). The tibial TightRope RT® was then passed through the tibial socket and the GraftLink® was pulled into the tibial socket (Figure 4). Final cortical suspensory fixation and tensioning of the GraftLink® was performed at a 20° of knee flexion angle (Figure 5).
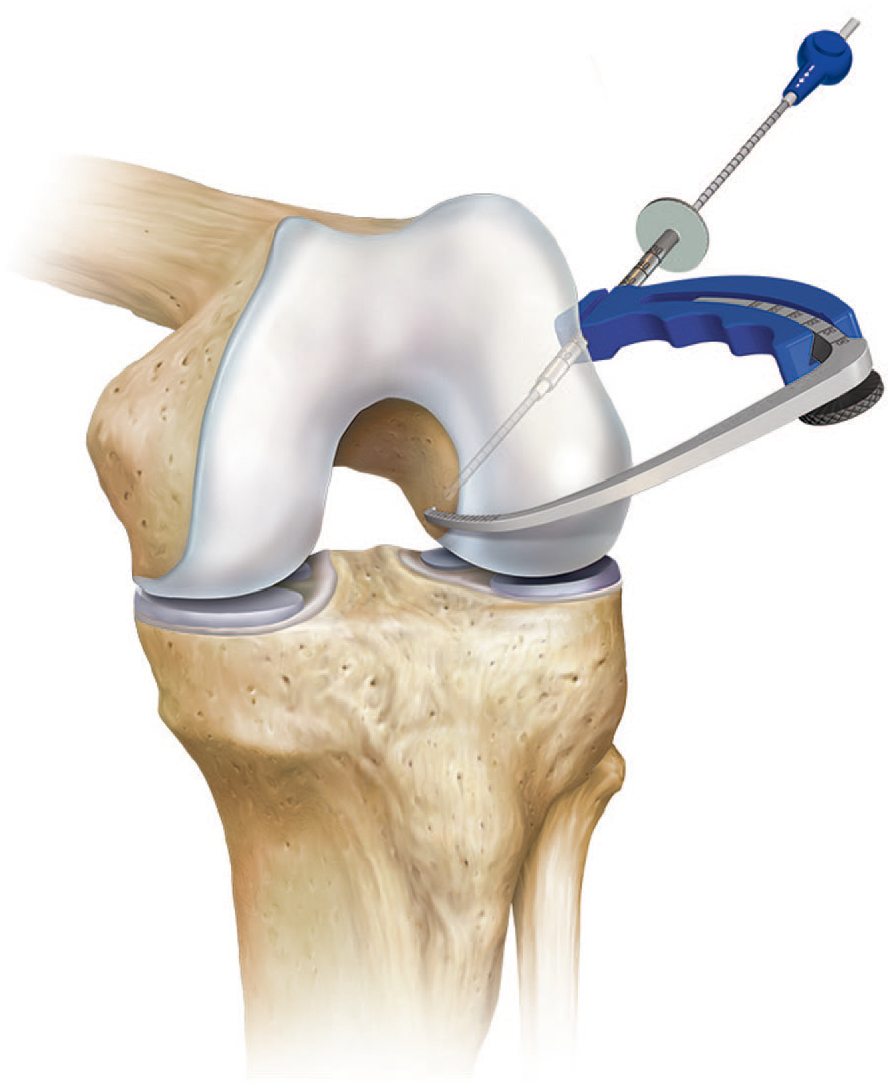
Femoral socket creation.
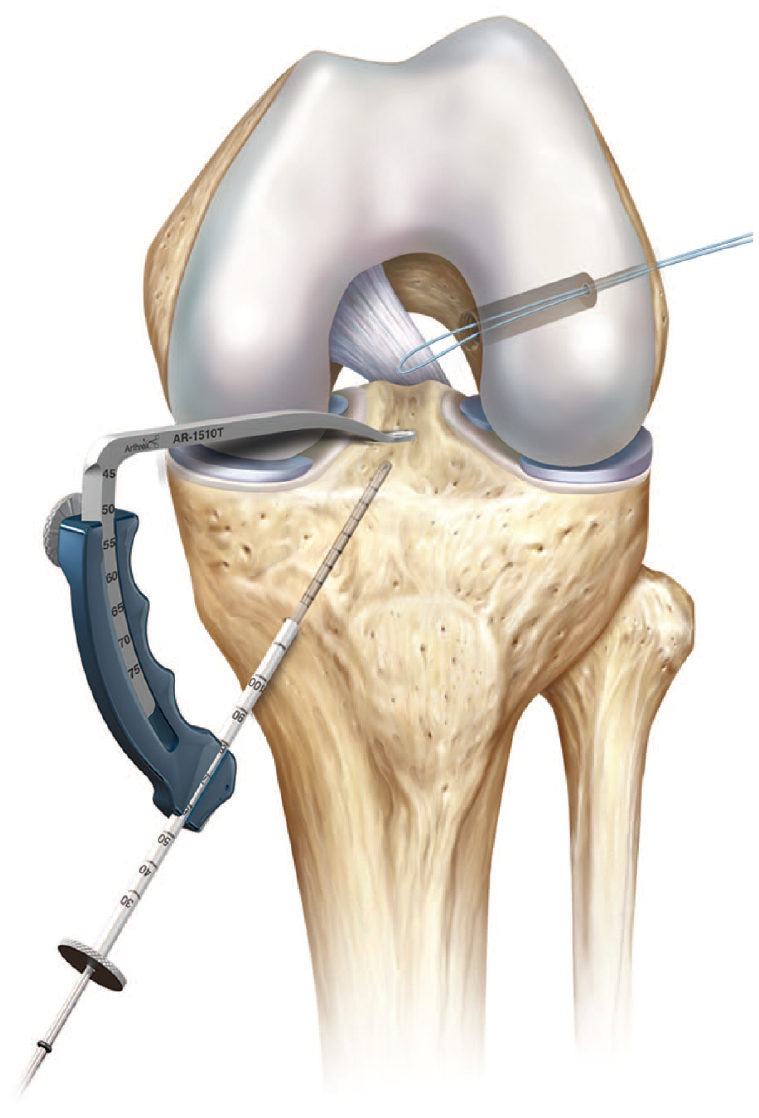
Tibial socket creation.

Femoral seating of graft.

Preparation of tibial graft passage.
Graft tightening.
All patients were treated according to a standardised ACL rehabilitation protocol, with focus on achieving immediate full knee extension equal to the preoperative measurement, return to running at 3 months and return to cutting and pivoting sports at 6 months.
Outcome assessment
Outcome was assessed in all patients by evaluating the Lysholm score, 22 International Knee Documentation Committee (IKDC) score (AOSSM IKDC Committee in 1987), Visual Analogue Scale 23 (VAS) score, 24 Tegner Activity Scale 22 prior to surgery and at 3-, 6-, 12- and > 24-month follow-up. At 24 months, clinical assessment was performed by evaluation of side-to-side difference testing using a knee laxity-testing device (KT-2000; MEDmetric, San Diego, CA) by an experienced and independent examiner. Extension weight-bearing antero-posterior (AP) and lateral radiography were performed at final clinical follow-up to grade the osteoarthritic status of knee according to the Kellgren–Lawrence grade 25 and to prove the correct position of the TightRope button at the lateral cortex of the femur. Follow-up radiographs were analysed by an independent senior orthopaedic trauma surgeon who was not involved in the surgical treatment of these patients.
Statistical analysis
Descriptive data (mean, range and proportions) were reported for the entire patient cohort. Statistical analysis focussed on clinical and functional outcome over time period. Therapeutic variables (surgery, adjuvant therapy and function) and demographic variables (sex, age and follow-up) were examined. Differences between the two groups were reported. Means and proportions were tested with the chi-square test for categorical variables and the unpaired t-test for continuous variables. Alpha was set at p < 0.05 to declare significance, all analyses were performed via SPSS (Version 22.0, SPSS Inc., Chicago, IL). Given the recent evidence for the potentially misleading nature no post hoc power analysis was carried out.26–28
Results
Between January 2011 and December 2014, 92 patients underwent primary all-inside ACL-R at this department. 54 patients were found to match equally according to age, BMI and follow-up and, therefore, enrolled in this study. There were 27 female and 27 male patients with a mean age of 29 years (range: 18–54 years) and a mean follow-up of 90 months (range: 24–144 months) were included. Patient demographic data are shown in Table 1.
Patient demographics.

BMI: body mass index; ACL: anterior cruciate ligament; ROM: range of motion.
In the female group, the mean age was 29.9 years (range: 18–53 years) with a mean follow-up of 95.6 months (24–143 months) and a mean BMI of 23.3 (range: 22–37.4). The mean duration between injury and surgery was 2.7 months (range: 0.1–21 months). Two patients (7.4%) presented with an additional grade 2 lesion of the medial collateral ligament and 15 patients (55.6%) with additional meniscal tears. In 17 patients (63%), ACL injury occurred during sports, and in 10 patients (27%), a low-energy trauma caused an ACL rupture. Mean graft size diameter was tibial 7.95 mm (range: 7.0–9.0 mm) and femoral 7.75 mm (range: 6.0–9.5 mm).
In the male group, the mean age was 29.8 years (range: 18.7–54 years) with a mean follow-up of 85.8 months (24–144 months) and a mean BMI of 24.7 (range: 21–34.3). The mean duration between injury and surgery was 8.9 months (range: 0.2–73 months). One patient (3.7%) presented with an additional grade 2 lesion of the medial collateral ligament and 11 patients (40.7%) with additional meniscal tears (Table 1). In 18 patients (67%), ACL injury occurred during sports, and in nine patients (32%), a low-energy trauma led to an ACL rupture. Mean graft size diameter was tibial 8.5 mm (range: 6.0–12.0 mm) and femoral 8.11 mm (range: 6.0–11.5 mm).
In each group, one patient sustained a deep surgical side infection of the ACL-reconstructed knee requiring a combination of intravenous antibiotics (clindamycin, levofloxacin and fosfomycin) and two times lavage of the knee. A follow-up MRI evaluation revealed an intact ACL graft in each case with good functional knee stability at final follow-up. In both groups, four patients (14%) reported skin numbness around the graft harvesting area at 24-month follow-up.
A significant improvement of symptoms, pain, daily function and sports activity level between baseline and 2-year clinical follow-up was found in both groups (Table 3). Female patients revealed lower IKDC and Lysholm scores preoperatively and at 3- and 6-month follow-up compared to the male patients, however, the findings were not statistically significant (Table 2).
Clinical outcome over time according to sex.
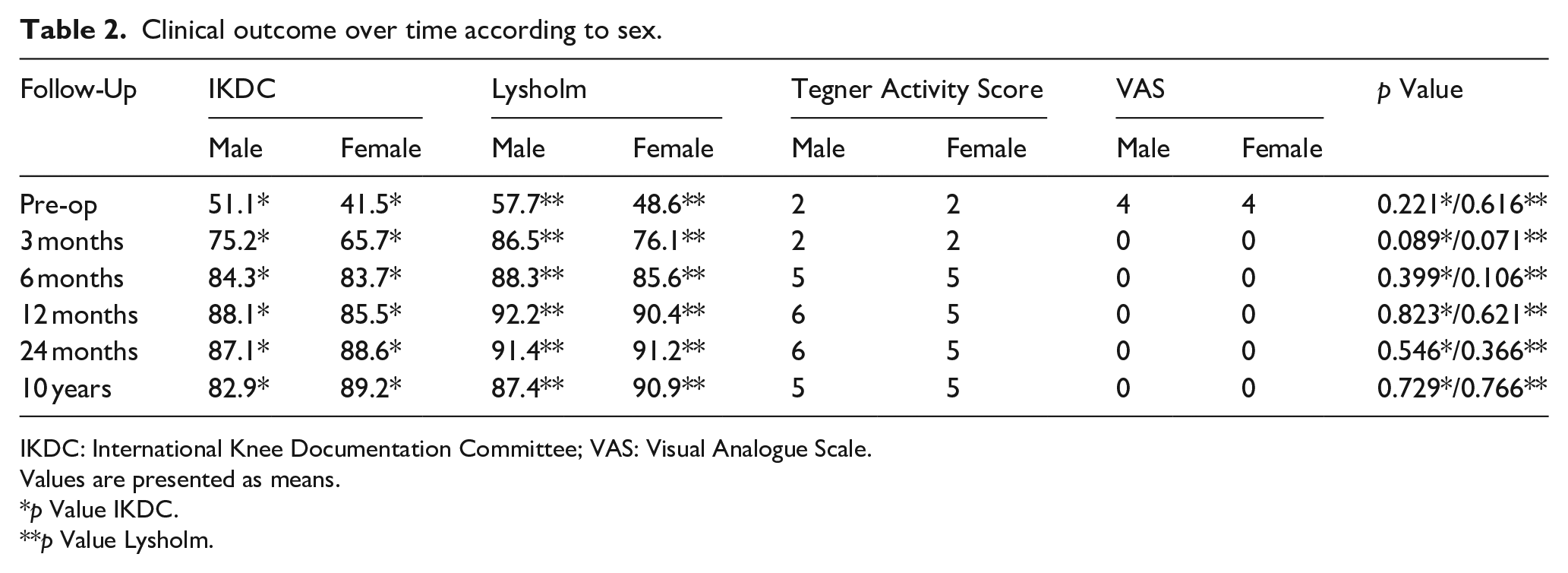
IKDC: International Knee Documentation Committee; VAS: Visual Analogue Scale.
Values are presented as means.
p Value IKDC.
p Value Lysholm.
At 12- and 24-month follow-ups, the scores showed nearly equal means in both groups. At 24 months, KT-2000 measurements showed no significant side-to-side difference with a mean of 1.79 mm (range: 0–5 mm) in female and 1.52 mm (range: 0–6 mm) in male patients (Table 3). One male patient revealed a side-to-side difference of ⩾ 5 mm, however, the patient did not complain of any functional knee instability.
Changes in clinical outcome over time according to sex.

IKDC: International Knee Documentation Committee.
Values are presented as means.
p Value pre-op to 24 months.
p Value pre-op to 10 years.
Radiographic evaluation at 24-month follow-up proved a correct TightRope® button position in all patients with no signs for the onset of early osteoarthritic changes compared to preoperative images according to the Kellgren–Lawrence Scale. 25
Long-term follow-up of over 10 years was reached by 27 of 54 patients. Outcome scores at > 10 years still showed no significant differences between female and male patients. However, the average scores were lower at 10 year than at 24-month follow-up (see Table 2).
A total of six patients (five males and one female) suffered from re-ruptures and two male patients sustained meniscal lesions between 24 months and > 10-year follow-up. All re-ruptures and meniscal lesions were associated with adequate re-trauma to the knee.
Discussion
The results of this study support our hypothesis that, following anatomic ACL-R using the all-inside technique, male and female patients exhibit no differences in objective and patient-reported outcome scores. Improvement of symptoms, pain, daily function and sports activity level between baseline and 2-year clinical follow-up was found in both male and female patients. The improvement towards baseline prevailed in patients who reached long-term follow-up of > 10 years. The lower average in IKDC and Lysholm at > 10 years can be linked to five patients who suffered a re-rupture and two patients who sustained meniscal lesions in the course of long-term follow-up, all of which happened through adequate re-trauma to the knee.
Our results also show that female patients reported lower IKDC, Lysholm and Tegner activity scale scores at 3 and 6 months postoperatively compared to male patients with equal scores at 12- and 24-month follow-ups. These findings are in line with data from the Scandinavian knee ligaments registers. 29 The differences found might be the reason for the phenomenon of female athletes taking longer to return to sports than male athletes following ACL injury thus influencing the subjective outcome scores. This was shown by Ardern et al. who reported that women were significantly less likely to have returned to sports at 12 months when compared to men. 30 An explanation to this might be found in previous studies which showed that male sex is positively associated with return to sports. 31 Digging deeper the difference in general pain perception between male and female patients could bear an answer. Etherton et al. 32 studied gender differences in physiological and subjective reaction to pain. Their work showed that while male probands had a stronger physiological reaction in terms of higher blood pressure reactivity their subjective pain ratings during pain induction were lower than those of female probands. Possible reasons put up by the authors for this phenomenon are different coping strategies like distraction or a reluctance to report actual levels of discomfort in men. Apart from a higher failure rate in female patients treated with a ST/G grafts and an Endobutton® fixation Noojin et al. 10 also reported women to be at a higher risk of pain after ACL-R compared to men. In the present study, no significant difference in the evaluated VAS in pre-, 3-, 6-, 12- and > 24-month follow-ups between men and women was found. These controversial results clearly indicate the need for further research towards the relationship between pain, subjective and objective outcome and its differences between male and female patients.
No significant differences were found for patient-reported outcome scores between male and female patients. These findings are in line with those of a systematic review carried out by Ryan et al. 12 and in contrast to the results reported by Senorski et al. 29 who showed poorer subjective outcomes to be present in female patients compared to males. However, all available systematic reviews comparing the subjective and objective outcome after ACL-R between male and female patients include studies that were published prior or around the year 2008, at a time where the trans-tibial technique for creation of the femoral tunnel was widely used and the all-inside technique was not yet used. To our knowledge, apart from this, study no further literature exists on outcome differences of the all-inside technique according to sex.
Another strength of this study was that patient groups were matched according to BMI and age in order to reduce bias. Nevertheless, this study has some limitations. This is a retrospective study and therefore subject to the usual limitations inherent in this type of study design. The inclusion of patients with additional knee pathologies might be a bias, however, a necessary one, as single ACL lesions in the absence of any additional pathology remain rare. There was only one surgical method evaluated in this study with no comparative group and there were no preoperative KT-2000 measurements or information on patients’ level of physical activity available. Therefore, it was not possible to determine or compare the degree of improvement between the preoperative and final follow-up measurements. No post hoc power analysis was carried out due to the potentially misleading nature of it.26–28
Due to the low number of cases, significance could not be shown; however, a trend for lower scores in women pre-surgery as well as 3 and 6 months after surgery could be observed. A recent review in ‘The Lancet’ investigated sex and gender as modifiers of health, disease and medicine and concluded the following: ‘When warranted on the basis of initial findings of sex differences or gender differences, or both, trials should be designed and powered to address sex-specific endpoints and pharmacology’. 33 This and the general progress of our society towards gender equity clearly indicate the need for biomedical research to keep up with this welcome development.
Conclusion
In conclusion, the findings of the present study reveal that equal objective and subjective success can be obtained following primary ACL-R using the all-inside technique in both women and men at long-term follow-up. The differences seen at 3 and 6 months with lower scores in women at early follow-up implicate the need for further, sex-sensitive investigation of this most crucial phase of rehabilitation after ACL-R.