
Abstract
Background:
Physical activity has known benefits during pregnancy; however, the optimum volume of physical activity through the different stages of pregnancy is not well known.
Objectives:
The aims of this study were to investigate the associations of physical activity volume in pregnant women in each trimester of pregnancy with maternal and infant outcomes.
Design:
The study involved 1657 pregnant women from the Australian Longitudinal Study on Women’s Health, who completed surveys from 2006 to 2012 (aged 28–39 years).
Methods:
Women reported being in either the first, second or third trimester of pregnancy. Women were grouped into four groups according to their self-reported physical activity during pregnancy: (1) Nil (0–<33.3 MET.min/week), (2) Low (33.3–<500 MET.min/week), (3) Moderate (500–<1000 MET.min/week) and (4) High (⩾1000 MET.min/week). Women who reported their physical activity during pregnancy completed a survey within three years after the birth, relating to outcomes associated with pregnancy and childbirth (gestational diabetes, hypertension, and antenatal depression and anxiety) and infant outcomes (birthweight and prematurity).
Results:
There was no association of physical activity in any trimester with infant birthweight, prematurity, gestational diabetes, hypertension or antenatal depression. Antenatal anxiety was less prevalent in women who reported low (1.7%) or moderate (1.1%) physical activity than in those who reported no activity (4.7%; p = 0.01).
Conclusion:
Different amounts of physical activity during pregnancy were not associated with the measured adverse health outcomes. However, low and moderate amounts of physical activity were associated with reduced incidence of antenatal anxiety.
Keywords
Introduction
Physical activity prior to, during and after pregnancy has known benefits to both mother and infant. 1 For the mother, benefits of physical activity include reduced risk of excess weight gain during pregnancy, preserving cardiovascular fitness, management of mental health, a reduction in duration of labour and decreased risk of complications (e.g. gestational diabetes and pre-eclampsia).2,3 For the infant, vigorous physical activity during pregnancy is associated with longer gestation. 4 However, there is limited evidence on the influence of physical activity in each of the trimesters of pregnancy on maternal and infant outcomes. Indeed, the optimum volume of physical activity throughout different stages of pregnancy and its influence on birth outcomes is not well known.
Recommendations for physical activity during pregnancy from the Australian Department of Health (2021) recognize that, in the absence of medical or obstetric complications, pregnant women should accumulate 150–300 min per week of moderate-intensity physical activity, or 75–150 min per week of vigorous intensity physical activity. The 2020 World Health Organization guidelines on physical activity and sedentary behaviour during pregnancy also recommend at least 150 min of moderate-intensity physical activity per week for substantial health benefits. 5 These guidelines do not discriminate between trimesters of pregnancy. A recent meta-analysis indicated the safety of 25–60 min of vigorous intensity exercise, 3–5 times per week, in the third trimester for health indicators such as prematurity and infant birthweight. However, whether this extends to high volume of physical activity (⩾1000 MET.min/week) is not known. Volume is a measure of the total amount of physical activity defined as intensity (METs) multiplied by duration (minutes) and frequency.
Vast physiological changes occur throughout pregnancy, with associated morphological changes in placental tissue as foetal demands increase with gestation. The enhanced ability for nutrient and gas exchange from placenta to foetus, as a likely result of regular physical activity, is advantageous to placental function. 6 As such, the benefits derived from physical activity during pregnancy may differ in each trimester. Currently, the associations of different amounts of physical activity with birth outcomes in each trimester are unclear.
The aims of this study were to investigate the association of physical activity in pregnancy with maternal and infant outcomes.
Methods
Study population
This study used data from the Australian Longitudinal Study on Women’s Health. This is a longitudinal study of women living in all regions of Australia who were randomly selected from women in the Medicare database. All participants gave written informed consent and ethical clearance was approved by both the University of Queensland and the University of Newcastle Human Research Ethics Committees (2004000224 and H-076-0795, respectively). Further details of the recruitment method and response rates have been described elsewhere. 7
In this study, we used data from women in the 1973–1978 cohort (18–23 years in 1996) who reported being pregnant in Survey 4 (2006–2009), Survey 5 (2009–2012) and Survey 6 (2012–2015). These women also provided birth details at the following survey (surveys 5, 6 and 7). We were then able to match information on pregnancy status by trimester, pregnancy physical activity data and resultant birth outcomes (Figure 1). The women reported being in either their first (n = 312), second (n = 715) or third trimester (n = 630) of pregnancy at surveys 4, 5 or 6. Women were excluded if they had a multiple birth (i.e. twins/triplets). If the women reported more than one pregnancy in the 3-year period between surveys, only the birth that occurred within 9.5 months of the previous survey was included (so as to match with pregnancy physical activity levels).
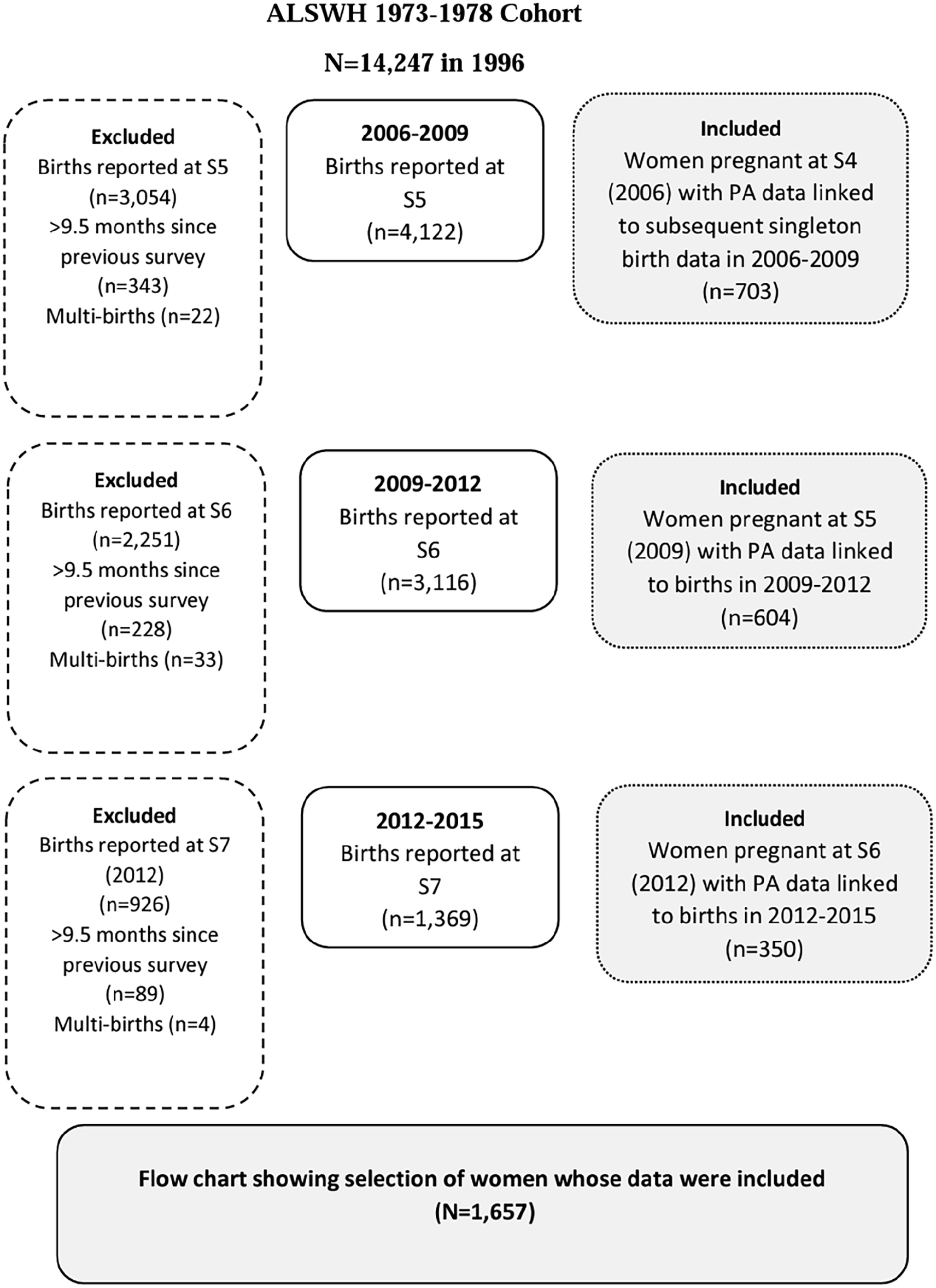
Consort diagram to show selection of women whose data were included in the analyses.
In each survey, physical activity was assessed with an adapted version of the Active Australia questionnaire. Women were asked to report weekly time spent walking briskly, and in moderate and vigorous activities during leisure and transportation. Time spent in each category was multiplied by a MET score (3.33 for walking and moderate-intensity activities; 6.66 for vigorous intensity activities). Total physical activity was estimated as the sum of overall MET.min. Women were categorised as inactive (0–<33.3 MET.min/week), low-volume physical activity (33.3–<500 MET.min/week), moderate-volume physical activity (500–<1000 MET.min/week) or high-volume physical activity (⩾1000 MET.min/week). Meeting the Australian Physical Activity guidelines was defined as ⩾500 MET.min/week). 8
Body mass index (BMI) was categorized into the four National Health and Medical Research Council (NHMRC) 9 categories of (1) Underweight (<20 kg/m2), (2) Healthy weight (20–25 kg/m2), (3) Overweight (>25–30 kg/m2) or (4) Obese (>30 kg/m2), as per the criteria at the time of the survey. Risk of harm associated with alcohol consumption was classified into five categories using NHMRC guidelines: (1) Low risk – up to 14 drinks per week (up to two drinks per day), (2) Non-drinker, (3) Rarely drinks, (4) Risky – 15–28 drinks per week (3–4 drinks per day), (5) High risk – More than 28 drinks per week (five or more drinks per day). Women were asked about their ‘usual’ alcohol intake, which we assumed indicated their alcohol intake pre-pregnancy. The Socio-Economic Index for Area (SEIFA) indicated the socioeconomic disadvantage of participants.
Maternal and infant outcomes
At surveys 5, 6 and 7, women were asked the following questions about their prenatal diagnoses: ‘Where you diagnosed with or treated for 1) hypertension during pregnancy, 2) gestational diabetes, 3) antenatal depression, and 4) antenatal anxiety’. Women were also asked ‘Did you experience: 1) a low birthweight baby (weighing less than 2.5 kg), 2) a high birthweight baby (weighing more than 4 kg), or 3) a premature birth (born before 36 weeks gestation)’. Women were also asked to report baby weight at delivery. The ALSWH researchers have previously assessed the reliability of these self-reported reproductive outcomes against more objective medical records, showing very high agreement (⩾92%) between the two data sets. 10 The questions are available on the Australian Longitudinal Study of Women’s Health website (http://alswh.org.au).
Statistical analyses
Means and standard deviations (SDs) are presented for continuous variables (age and index of relative disadvantage) and proportions are presented for categorical variables (number of previous children, smoking and alcohol intake status, physical activity volumes and BMI). The association between volume of physical activity and birthweight was assessed using linear regression. The analysis was undertaken separately for women who were in each trimester. The association of volume of physical activity and categorical variables (hypertension, gestational diabetes, antenatal depression, antenatal anxiety, low birthweight, high birthweight and prematurity) was assessed using logistic regression. Due to the low incidence of negative birth outcomes in this cohort, volume of physical activity in any trimester was used in the analysis (to retain adequate sample size) rather than being separated into trimesters. Potential confounders included maternal age, current smoking status, usual alcohol intake, index of relative disadvantage, number of children, and pre-pregnancy BMI. Risks are presented as unadjusted and adjusted odds ratios with 95% confidence intervals. Analyses were performed using the statistical software package Stata IC, version 16.
Results
Characteristics of the 1657 women included in this study are shown in Table 1. Their mean (SD) age was 32.8 ± 2.6 years, and most reported having a ‘healthy’ pre-pregnancy BMI (57.6%), with 37.5% being considered overweight or obese. According to the NHMRC alcohol category, most participants reported being low risk drinkers (45.8%) and never smokers (64.5%). The SEIFA socioeconomic disadvantage score indicated lower levels of disadvantage than the general population. 11 The characteristics of the sample of women who were pregnant were similar to those of the entire 1973–1978 ALSWH cohort during the same period (2006–2012). 12
Characteristics of the participants (N = 1657).

SEIFA: Socio-Economic Index for Area.
Fewer than half the women met physical activity guidelines (⩾500 MET/mins.week) in the first trimester of pregnancy (39.1%). Women in their second and third trimesters were even less likely to meet physical activity guidelines than women in their first trimester (35.9% and 29.4%, respectively). By the third trimester, only 10.6% of women were in the high physical activity category and 20.8% reported no physical activity.
Birthweight was slightly higher in women who reported low (3.53 ± 0.55 kg) and moderate (3.49 ± 0.57 kg) volumes of activity in the first trimester, than in those who were reporting no physical activity (3.31 ± 0.59 kg) in the first trimester (Table 2). There were no associations between birthweight and physical activity in women who were in their second or third trimesters. Birthweight was slightly lower in women meeting guidelines (3.45 ± 0.50 kg) than women not meeting guidelines (3.56 ± 0.50 kg) in the third trimester. However, these differences in birthweight are not clinically significant, given the average weight of infants in each group were within the healthy weight range (2.5–4 kg).
Associations of physical activity volume and meeting physical activity guidelines in each trimester on birthweight (kg).

SD: standard deviation; CI: confidence interval.
Not meeting guidelines = none + low (< 500 MET/mins.week); Meeting guidelines = moderate + high (⩾ 500 MET/mins.week). Model adjusted for: maternal age, current smoking status, usual alcohol intake, index of relative disadvantage, number of children, and pre-pregnancy BMI.
The associations between physical activity volume in any trimester of pregnancy and maternal and infant outcomes are presented in Table 3. There were no associations between physical activity volume and low birthweight, high birthweight or prematurity. Likewise, there were no associations between physical activity volume and incidence of gestational diabetes, gestational hypertension or antenatal depression. Rates of antenatal anxiety were lower in women who reported low (1.7%) or moderate (1.1%) physical activity, than in those who reported no activity. There was no difference in antenatal anxiety rates between those who reported high physical activity (2.7%) and those who were inactive.
Associations between physical activity volume in any stage of pregnancy and maternal and infant outcomes.

OR: odds ratio; CI: confidence interval.
Not meeting guidelines = none + low (<500 MET/mins.week); Meeting guidelines = moderate + high (⩾500 MET/mins.week). Model adjusted for maternal age, current smoking status, usual alcohol intake, index of relative disadvantage, number of children and pre-pregnancy BMI.
Discussion
Main findings
The majority of women did not meet the current Australian physical activity guidelines for any trimester in pregnancy. Moreover, reported physical activity levels were lower in women who were in their third trimester than in women who were in their first trimester. The findings from this study indicate that different volumes of physical activity reported in each trimester of pregnancy were not associated with outcomes for mother or infant. However, a low and moderate volume of exercise during pregnancy was associated with slightly reduced incidence of antenatal anxiety.
The findings from this study indicate that only 10.6% of women reported high levels of physical activity in their third trimester, and one in five women abstained from physical activity altogether in the third trimester. These physical activity patterns are consistent with those reported in the literature, which show that fewer than 50% of women report meeting guidelines during pregnancy, with levels declining throughout pregnancy. 13 These low levels of activity may persist for up to four years postpartum. 14 A recent qualitative assessment of women’s experiences and decision-making about physical activity during pregnancy highlighted that many women felt a sense of disapproval from others in regard to the safety of physical activity during pregnancy. 15 Participants perceived symptoms such as fatigue, nausea and pain, which can be symptoms of physical exertion, as perceived threats or risks. These externally and internally derived perceptions may explain, at least in part, the low physical activity reported in the current study.
There were no associations between physical activity in any trimester with clinically low or high birthweight in this study. The influence of physical activity and exercise on infant birthweight and other anthropometric data has been evaluated previously.16,17 Previous findings have suggested an inverted U-shaped relationship between physical activity and infant birthweight, that is, moderate volume of exercise was associated with the highest infant birthweight, with both low and high physical activity associated with lower infant birthweight. 17 However, the study did not examine whether this association was trimester specific. The study by Bell et al. 18 did show that increasing the frequency of vigorous intensity exercise from 3 to 5–7 sessions was associated with 0.63 kg lower infant birthweight. However, the study by Zeanah and Schlosser 19 showed no influence of higher volume of exercise in pregnancy on infant birthweight. Furthermore, the study by Kuhrt et al. 20 indicated that increasing the weekly distance run did not influence birthweight percentile, even when the increased distance was continued into the third trimester. These conflicting findings demonstrate the need for future studies to investigate the specific dose–response relationship of exercise volume in various stages of pregnancy with infant outcomes. Importantly, this study showed maternal physical activity volume in any trimester was not associated with clinical outcomes such as large or small for gestational age infants. The findings from this study indicated that higher amounts of physical activity in any of the three trimesters, was not associated with infant birthweight.
There was no association between physical activity volume in any trimester and maternal outcomes of gestational diabetes, hypertension or antenatal depression. The mechanisms behind how high physical activity in any trimester may influence foetal development and outcomes is not well studied. There is some evidence to suggest that the redirection of blood flow in acute high intensity exercise does not negatively influence foetal heart rate, due to compensatory mechanisms in the foetal autonomic nervous system.21–23 However, it is still not clear whether foetal compensatory mechanisms for redirected blood flow occur with increased frequency of higher intensity exercise (resulting in a high volume of exercise). The findings from the current study show no association with higher physical activity on foetal outcomes such as prematurity. This indicates that any foetal compensatory mechanism which is potentially active during acute higher intensity exercise may be maintained during increased frequency or duration of exercise as well. This interpretation is speculative at best but does provide grounding for future studies of the dose–response relationships between exercise volume and maternal and foetal outcomes.
Low and moderate volumes of physical activity appear to be protective of antenatal anxiety. Previous research has shown that accumulating 150 min of moderate-intensity exercise (e.g. brisk walking, water aerobics, stationary cycling and resistance training) reduces the severity of antenatal depressive symptoms in pregnant women. 24 However, our study did not indicate any association between physical activity and antenatal depression. Interestingly, there was no statistically significant difference in antenatal anxiety prevalence between those who reported high volumes of physical activity and those who were inactive. More studies of the associations between physical activity and anxiety during pregnancy are required to elucidate any differences between highly active and inactive women. This is important, because it is possible that the trend of a ‘Belly Only Pregnancy’ and its relationship with body image dissatisfaction, may be driving an ‘over-exercise’ disorder in some women. 25 If this is the case, then a sub-set of pregnant women may require more mental health support.
Limitations
Some limitations to the study should be noted. First, it was not possible to track physical activity throughout pregnancy. Rather, we were only able to establish physical activity volume at a single time point during pregnancy and it was not possible to examine individual changes in physical activity throughout the trimesters. Second, the small sample size for some outcomes may have been insufficient to detect associations if they exist. Indeed, the low occurrence of negative birth outcomes in this cohort meant we had to use volume of physical activity from any time point in pregnancy, rather than in specific trimesters, in the logistic regressions. Third, the use of self-reported measures of physical activity is a limitation, and future research should confirm these findings with objective measures of physical activity. Finally, this cohort may not be representative of the entire pregnant population, as the SEIFA socioeconomic disadvantage scores indicate lower levels of disadvantage (i.e. greater affluence) in our sample than the general population. Also, as this longitudinal data set was collected from 1996 to 2015, the findings may not apply to the current pregnant population.
Conclusion
Most pregnant women do not meet the guidelines for moderate-vigorous physical activity during pregnancy, and the proportion who meet this guideline is lower in the second and third trimesters than in the first. The current findings indicate that different volumes of physical activity through any trimester of pregnancy are not associated with maternal or fetal outcomes. However, low-moderate volumes of physical activity in pregnancy may reduce the prevalence of antenatal anxiety. The results provide a platform for future research to investigate the relationships between exercise volume in each trimester of pregnancy and birth outcomes. In particular, the dose–response of moderate-high volumes of exercise in the different stages of pregnancy warrants further investigation.