
Abstract
Women who are fertile experience a significant burden from thyroid cancer. In reality, delaying childbirth is the current trend in maternity. Women who have thyroid cancer may later want to get pregnant after it has been treated, which presents a multidisciplinary issue for their doctors. A variety of specialists are frequently involved in the treatment of thyroid cancer. This review aims to address the key elements of the strategy and places special emphasis on the significance of fertility in women with thyroid cancer diagnosis and remission. We will cover topics including the role of thyroid hormones in pregnancy and fertility.
Introduction
The incidence of thyroid cancer in women is increasing at an alarming rate, with the highest risk in the reproductive years. According to statistics from the World Cancer Observatory, in the population of women between 25 and 45 years of age, thyroid cancer is the third most common cancer found, after breast and cervical cancer. Epidemiological studies have shown that the female prevalence in thyroid cancer is greater during reproductive age, 1 considering that between 1978 and 2019, the median age of women who gave birth in developed countries increased from 26.8 to 33.2 years, 2 and that the tendency to postpone motherhood even more continues. 3 We are going to have more cases of thyroid cancer in women with the desire for pregnancy after its cure. This represents a new challenge for the clinical team. 4
A cancer diagnosis is a life crisis for anyone. Younger people face additional potential loss of reproductive function and the opportunity to have children. Thyroid hormones play an essential role in maintaining pregnancy and promoting optimal fetal development. 1 According to its histological characteristics, thyroid cancer can be classified in follicular-derived thyroid cancers and neuroendocrine C-cell-derived thyroid cancer.5,6 Among the follicular-derived thyroid cancers, we find the differentiated thyroid cancer that originates from thyroid follicular epithelial cells. 5 Under the differentiated thyroid cancer category, we find the well-differentiated thyroid cancers: papillary thyroid cancer, follicular thyroid cancer, and Hurthle cell thyroid cancer, as well as anaplastic thyroid cancer (ATC). 6 In the neuroendocrine C-cell-derived thyroid cancer, we have the medullary thyroid cancer (MTC) which originates in the parafollicular neuroendocrine cells of the thyroid.5,6
During thyroid cancer treatments, thyroid hormone changes are expected, and fertility can be compromised. 4 Despite this, and the physician’s duty to preserve the reproductive capacities of young women with cancer, 7 there is little information on the approach to patients with thyroid cancer who wish to become pregnant or that are diagnosed during pregnancy. In our daily practice, fertility issues are widely discussed with patients of reproductive age diagnosed with breast, cervical, and ovarian cancer; however, in our opinion, this is not done with the same frequency and thoroughness for thyroid cancer cases in many centers. 8
This article is the result of the meeting of a group of specialists from different areas involved in the treatment of thyroid cancer in women of reproductive age. We present a review of the literature addressing main key aspects that, in our opinion, can help doctors to better approach the problem and may raise concern about the importance of fertility in women with thyroid cancer. This review addresses: the physiology of thyroid hormones in women during reproductive age, pregnancy, oncofertility, and thyroid cancer, as well as the assisted reproduction techniques (ART) available for the preservation of fertility in cancer survivors and some important aspects to consider for the treatment and follow-up of thyroid cancer in women of reproductive age.
Thyroid hormones and women’s reproductive health: mechanistic links
The regulation of thyroid hormones is a key factor for the process of fertility, conception, and pregnancy; thyroid hormone dysfunction leads to menstrual disturbances, subfertility, and maternal and fetal complications during pregnancy, including miscarriage, stillbirth, and premature delivery. 9 It is worth mentioning that fetal thyroid function depends on maternal thyroid function during the first trimester. 9 There are several molecular mechanisms that could explain the link between the regulation of the thyroid axis and the reproductive health of women; some of them are as follows:
There are receptors for thyroid hormone on ovarian surface epithelium, granulosa cells, and in oocytes of primordial, primary, and secondary follicles. 10 Also, receptor TSHR, TRa1, TRa2, and TRb1 have been founded to be present in endometrium, and their expression varies during the menstrual cycle. 11 Then, there is a direct impact of thyroid hormone concentration in both ovary and endometrium function. In addition, mature human granulosa cells and placenta expressed transcripts for 5’ deiodinase types 2 and 3, indicating the possibility of conversion of peripheral thyroid hormone thyroxin (T4) to its metabolic active form.10,12
Thyroid dysfunction disrupts the hypothalamic–pituitary–ovarian axis by altering the secretion of gonadotropin-releasing hormone (GnRH) and impairing folliculogenesis, fundamental process in human reproduction. 12 Thyroid hormones stimulate follicle-stimulating hormone (FSH) induced granulosa cell survival with direct impact on folliculogenesis, steroidogenesis, and synthesis of follicular fluid. 13 Thyroid hormone synergizes with FSH to increase luteinizing hormone (LH) receptors and progesterone secretion affecting the reproductive cycle. 14 In hyperthyroidism, LH and FSH secretion can be increased, but with an abnormal pulse in LH affecting ovulation. 12 It has also been described the presence of hyperprolactinemia induced by an increased stimulation of the thyrotropin-releasing hormone (TRH). 15
Angiogenesis is considered as a crucial event for successful implantation, decidualization, and placentation. 14 Thyroid hormones may influence in angiogenesis and immune function during conception and embryogenesis. 16 The placenta also expressed transcripts for 5’ deiodinase types 2 and 3, implying the possibility of conversion of peripheral thyroid hormone thyroxin (T4) to its metabolically active form.10,12
Thyroid hormones interfere with estrogen activity. Hypothyroidism reduces the uterine cell’s estrogenic response, resulting in development of reduced endometrial thickness and causes a reduced in the serum levels of sex hormone-binding globulin decreasing the level of total estradiol (increased level of free estradiol), 14 while in hyperthyroidism the opposite situation is observed. 14 In addition, the metabolic clearance rate of estradiol is reduced in both conditions.
Thyroid dysfunction and autoimmunity are associated with female and idiopathic subfertility. 9 Thyroid supplementation is recommended in this scenery and even in patients getting ART. 9 There is some evidence that suggests thyroid autoantibodies could induce cytotoxic reaction and alteration in the follicle fluid. 9 Women with a positive thyroid autoantibody going through pregnancy loss should take thyroid supplementation. 9
Diagnosing thyroid cancer
The diagnosis of thyroid cancer in the female population, including pregnant women, should include a careful history and physical examination. 17 The physical examination includes a thorough inspection and palpation of the neck, searching for nodules, either the increasing volume of existing ones or the appearance of new ones. 18 The appearance of a firm lesion, a sensation of pressure on structures adjacent, symptoms of obstruction, dysphagia, vocal cord paralysis, hoarseness, and appearance of enlarged cervical lymph nodes are some warning symptoms to consider diagnosis. 17 Given this, it is important to perform an assessment of the thyroid gland and palpation, as well as an active search for supraclavicular and submandibular adenopathy. 18
The initial evaluation of thyroid nodules discovered during pregnancy or postpartum is the same as in the non-pregnant, nonlactating population and includes measuring serum thyroid function and performing an ultrasound. 19 Afterward, fine-needle aspiration (FNA) should be performed, if applicable, based on the sonographic pattern (Bethesda Classification) and patient preference according to a risk stratification algorithm. 18 Several studies to date have shown that FNA is a safe procedure and may be performed in any trimester of pregnancy. 17
Serum TSH should be measured; however, this may present unique challenges during pregnancy as serum TSH physiologically decreases during early gestation. 17
Treatment modalities of thyroid cancer
Treatment of patients with thyroid cancer is often multidisciplinary and involves surgeons, endocrinologists, medical oncologists, radiation oncologists, and nuclear medicine physicians. Thyroid cancer has several treatment modalities, such as surgery, partial or total, radioactive iodine therapy (RAI), drugs such as tyrosine kinase inhibitors, immunotherapy, mTOR, BRAF, and MEK inhibitors and external beam radiation therapy (EBRT). 20 The indication of any of these treatments will depend mainly on the risk assessment, which is defined according to the stage, the histological characteristics, and the molecular markers of the tumor.
In most cases, surgery is the standard treatment. There are various surgical options such as lobectomy, lobectomy and isthmectomy, subtotal thyroidectomy or total thyroidectomy, and the choice of one of these procedures will depend mainly on the risk classification. Thyroid lobectomy involves removing all the thyroid tissue on one side of the trachea or removing half of the thyroid gland. It is known as a lobectomy and thyroidectomy when the thyroid lobectomy is extended to the midline. Extension to the contralateral lobe, but with preservation of a portion of the contralateral thyroid lobe, is defined as subtotal thyroidectomy. Finally, total thyroidectomy refers to the removal of both lobes of the thyroid. 21 In addition to these surgical management options, most patients are taken to central compartment dissection (Level VI) as therapeutic or prophylactic management, considering that this is the main site of lymph node metastatic disease.22,23 Less commonly, a lateral neck dissection is performed (Levels II–V), and Levels I and VII, in case there is evidence of lymph node disease in these areas documented by ultrasound, fine-needle aspiration cytology or thyroglobulin washout measurement.22,23 RAI is the treatment based on the administration of the radioisotope I-131, which is trapped by the sodium iodide symporter (NIS) are expressed by differentiated thyroid cells. 24 Once the NIS catches I-131, the cell is destroyed. Considering that NIS is expressed in well-differentiated thyroid cells, this treatment will be effective in well-differentiated tumors such as papillary and follicular tumors.
Finally, EBRT consists of the administration of a dose of ionizing radiation with the intention of eradicating a tumor. This is not a commonly used treatment for the management of thyroid cancer. However, its use may be considered in non-iodine-avid tumors, such as ATC, tumors with large extrathyroidal extension, or in patients with residual disease who cannot be treated with RAI or surgery. 21 The exposure of the thyroid gland to ionizing radiation causes damage to it, which leads to secondary hypothyroidism, which, according to the systematic review by Boomsma et al., 25 occurs in patients with tumors of the head and neck receiving radiotherapy in 48% at 5 years and 67% at 8 years after being irradiated.
In pregnant women, cytologically benign nodules should be managed as those found in general population. 17 Cytologically indeterminate thyroid nodules (atypia of undetermined significance/follicular lesion of undetermined significance, suspicious for follicular neoplasm, or suspicious for malignancy) during pregnancy may be followed conservatively, and it is advisable to delay surgery until postpartum. 17 Levothyroxine suppression therapy targeted at keeping TSH levels within the lower normal range (0.1–1.5 mU/L) is advised for these patients. 26
There are specific scenarios where thyroidectomy should be done in the second trimester: in more aggressive thyroid cancer types: MTC and ATC, 18 metastatic cervical lymph nodes (diagnosed by cytology), severe compressive symptom, and the significant growth of a malignant nodule (>50% in volume or >20% in diameter in two dimensions) before Week 24 of pregnancy. 26 Pregnancy is a contraindication for nuclear imaging and RAI. 19
Regarding patients with a history of thyroid cancer who received RAI treatment and have pregnancy desires, pregnancy should be avoided 6–12 months after the administration of radioiodine doses. 26 In addition in these patients, there is no reported information about infertility, disturbances in pregnancy such as miscarriage, stillbirth, premature delivery, low birthweight, congenital malformations, neonatal mortality, or tumor growth or risk of recurrence. 26
Fertility preservation
Fertility treatment has three clear indications: cancer, benign diseases (i.e. endometriosis), and for personal reasons. 27 Reproductive age counseling is a fundamental pillar in women who develop some type of cancer and is periodically being attended only by gynecologists or fertility experts.28–30
Fertility is currently a sensitive and very important issue for women and doctors. The role of the oncologist and other fertility specialists is established and should always be addressed. 27 The ovarian reserve decreases physiologically with age; for this reason, fertility is also a time-sensitive issue. 27 That said, early and prompt advice in fertility care makes all the difference.
Cancer survivors may seek to fulfill their reproductive desire after achieving cancer remission as mentioned above. It is clearly established that thyroid function plays an active role in human reproduction. 12 At the preconception visit, thyroid function should always be established and treated if pathologic findings are found. 18 Even in prenatal checkups, thyroid-stimulating hormone (TSH) and FT4 levels should be routinely monitored by obstetricians. 18 Recent clinical data have demonstrated that no significant disease recurrence or worsening of structural disease during pregnancy. 19
Cancer patients and survivors must be informed about the different options to preserve fertility, since their reproductive rights must be respected after cure or remission. 27 Thyroid cancer may be complicated by infertility. 31 Nowadays, ART is an important consideration in women of childbearing age. 32 As one might argue that some of these techniques can stimulate tumor growth, there is evidence about ovarian hyperstimulation and GnRH agonist that can cause high estradiol levels; this may have a negative effect on estrogen-sensitive tumors.33,34 Nevertheless, thyroid cancer is not an estrogen-sensitive tumor, and information about ovarian hyperstimulation in thyroid cancer is scarce.
Recent studies have revealed thyroid cancer history did not affect the pregnancy outcomes or increase the risk of adverse obstetric outcomes after the first ART (in vitro fertilization/intracytoplasmic sperm injection), but it may decrease the number of retrieved oocytes and high-grade embryos. 32 In advanced thyroid cancer patients or even women with thyroid cancer in situ complicated by infertility who had pregnancy desires, ART becomes a feasible option. 35 Table 1 summarizes the different fertility preservation techniques available to date, their considerations, and limitations as an accessible tool for the approach of all specialists.7,36,37
Fertility preservation techniques available to date, considerations, and limitations.
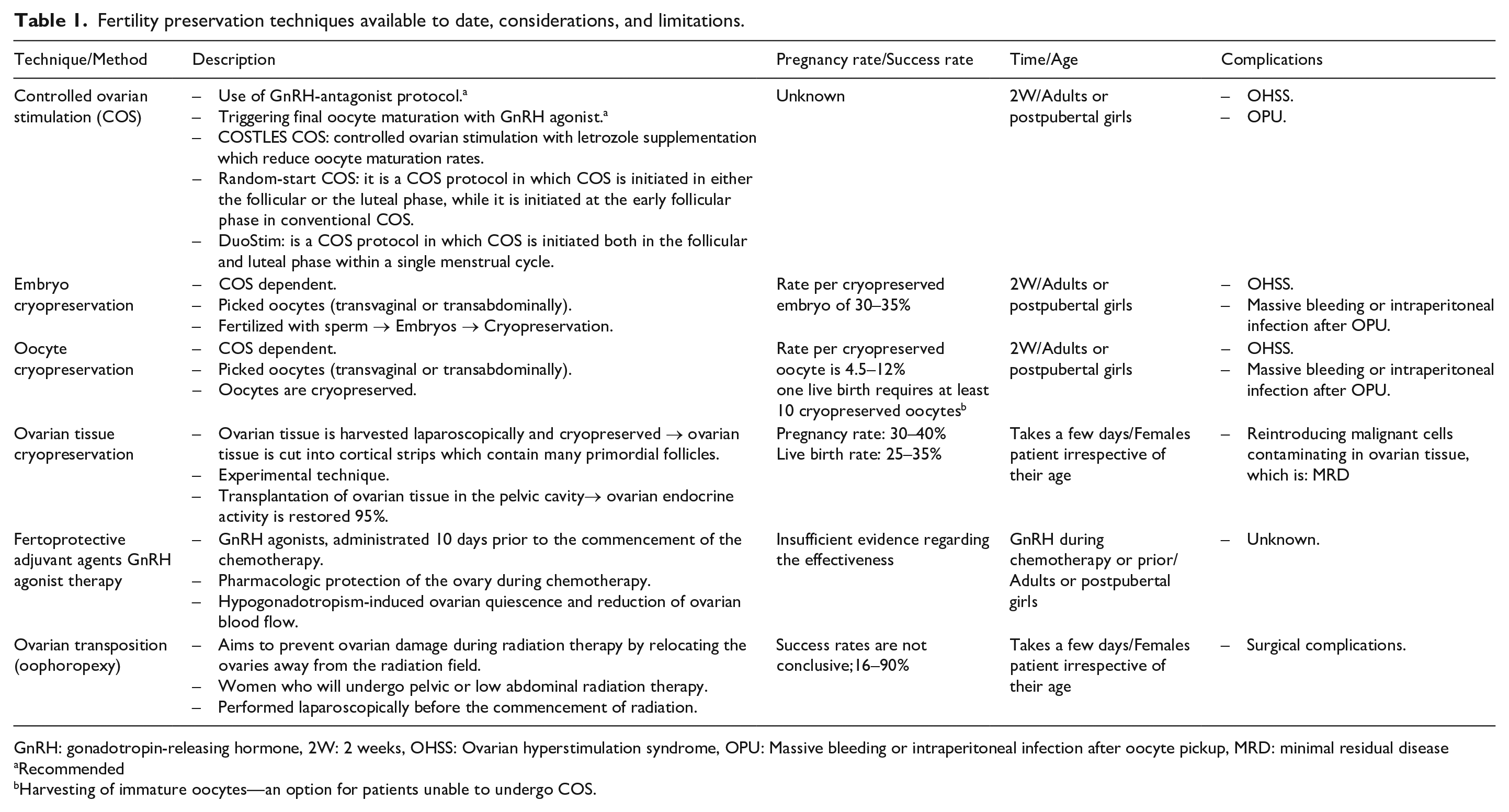
GnRH: gonadotropin-releasing hormone, 2W: 2 weeks, OHSS: Ovarian hyperstimulation syndrome, OPU: Massive bleeding or intraperitoneal infection after oocyte pickup, MRD: minimal residual disease
Recommended
Harvesting of immature oocytes—an option for patients unable to undergo COS.
Even though the main mechanism of accelerated and premature depletion of germ cells in the gonads is caused by direct toxic insults from chemotherapy regimens; 38 and chemotherapy regimens are not part of the regular treatment in thyroid cancer fertility preservation options should be known by the multidisciplinary team and discussed. 38 Time and age are two modifiable factors, thanks to advanced fertility preservation technology, and patients must know all their possibilities, even experimental ones.
Follow-up
Although most patients with thyroid cancer are considered as low-risk patients and will remain without evidence of recurrent disease, follow-up is still very important. Serum TSH should be maintained below 0.1 mU/L indefinitely in patients with incomplete structural response to treatment and for patients with incomplete biochemical response; TSH should be maintained between 0.1 and 0.5 mU/L. 22 Serum thyroglobulin (Tg) and neck ultrasound are the main tools for follow-up; however, Tg levels are not capable of differentiating between normal and tumor cells. Negative serum Tg levels have high negative predictive values, but serum Tg antibody level testing is necessary to avoid errors, as these antibodies can alter Tg results. Neck ultrasound is the recommended study to detect residual disease in the neck; combined with the results of fine-needle cytology and serum Tg, they have a very high accuracy of almost 100%. 39
An emerging challenge for clinicians is the increase of thyroid cancer in women in the reproductive age, recommendations about levothyroxine and pregnancy should be discussed during follow-up with patients who wants to be pregnant. Between 50% and 85% of women with hypothyroidism require adjustment of levothyroxine dose in pregnancy, especially those patients without functional thyroid tissue, as is the case of patients with thyroid carcinoma who underwent surgery. 18
Levothyroxine adjustment should be done as soon as possible after pregnancy is confirmed. The ATA 2015 guidelines recommend increasing the dose by two additional tablets weekly (nine tablets per week instead of seven tablets per week, giving a 29% increase) so it can effectively mimic gestational physiology and thus prevent maternal hypothyroidism during the first trimester. 18 Another option is to increase the dosage of daily levothyroxine by approximately 25%–30%. Pregnant women with thyroid cancer should be managed at the same TSH goal as determined preconception. 18 TSH should be monitored approximately every 4 weeks until 16–20 weeks of gestation, and at least once between 26 and 32 weeks of gestation, 18 ultrasound examination and thyroglobulin tests should be performed every 3 months. 26
Prognosis
The overall survival rate for thyroid cancer depends on histopathological classification. 40 Differentiated thyroid cancer usually has an excellent prognosis with 10-year survival rates exceeding 95%. 40 This percentage diminished as the carcinoma spread to lymph nodes or tissue in the neck, 76% for metastatic papillary thyroid cancer, 64% for metastatic follicular thyroid cancer, and about 28% in stage IV MTC. 40 In contrast, ATC is almost uniformly lethal, with a 1-year survival rate about 20%. 40
Discussion
Available data on reproductive intentions show that women in their 30s and 40s report that they plan to have another child, while women under 30 have delayed their plans to have a child or reduced the number of children they hope to have. 41 Recent research revealed that women put off parenting until their careers are on track, to find a partner, earn money, and get a “family-friendly” job. 3 The World Health Organization (WHO) report suggests that the annual fertility rate may be declining. Births have been declining for 6 consecutive years and have fallen sharply during the pandemic, but the proportion of women having children at the end of their reproductive years has been on the rise. 2 The pandemic acknowledges as COVID-19 pandemic in 2020; a global outbreak of a new virus SARS-CoV-2.
Considering that the multidisciplinary approach of cancer treatment involves a series of different specialist, fertility issues should be address and discussed as soon as the diagnostic is made because of the high burden of this disease in women of reproductive age.27,37 In thyroid cancer, considering thyroid physiology plays an important role in conception, reproduction, and pregnancy, 9 several topics should be discussed related to counseling in reproductive issues. Fertility options use to be limited and possibilities for women beyond the traditional method where off the table. Nevertheless, medicine advancement and development have made fertility a vanguard issue with the possibility of offering diverse options, ART, to fulfill and accomplish women fertility desires (cryopreservation, ovarian tissue preservation, etc.).27,37
As surgery is considered the standard treatment in women with thyroid cancer, post-surgery recovery time should be contemplated regarding preconception planning and counseling. 40 It is known that after surgery women will require thyroid hormone replacement therapy, to accomplish normal thyroid function, this could be a limitation for a prompt pregnancy, making necessary a strict follow-up with biochemical parameters.18,19 If RAI is the selected therapeutic option in the first-place pregnancy should be ruled out and after its administration, patients should be advice to deferred pregnancy for a minimum of 6 months. 17 In advanced thyroid cancer stages or worse prognosis, the ART become a suitable option to discuss with due to the need to postpone pregnancy and minimizing age factor on ovarian reserve.32,35
Warranting women reproductive and sexual rights27,37 is among our task after thyroid cancer is diagnosed since there is a clear and direct relation among thyroid hormones, pregnancy, and fetal physiology. We need to raise the awareness and offer the various preserving fertility options as well as transmitting the importance of a normal thyroid function and antibodies profile in order to obtain and maintain pregnancy.
Conclusion
Thyroid function is highly related to fertility. Before starting treatment, patients of reproductive age diagnosed with thyroid cancer should be asked about their desire to conceive, be informed about possible side effects of treatment on the reproductive organs and informed them about available assisted reproductive technologies for conservation of fertility. During pregnancy, levothyroxine dose and follow-up should be adjusted, and the TSH target for pregnant women is the same as for non-pregnant women.