
Abstract
Objectives:
To evaluate the structural and construct validity, and internal consistency of the Quality of Life Scale among Canadian women with histories of intimate partner violence.
Methods:
Consistent with COSMIN Guidelines, a secondary analysis was conducted using data from a community sample of 250 adult (over 18 years) Canadian women with histories of partner violence and who participated in Wave 5 of the longitudinal Women’s Health Effects Study. Data were collected 4 years after baseline using structured interviews that included the Quality of Life Scale and two mental symptom scales (Center for Epidemiological Depression Scale and Davidson Trauma Scale) used to assess construct validity of the Quality of Life Scale.
Results:
Confirmatory factor analysis in MPLUS 8 with maximum likelihood estimation supported the hypothesized unidimensional structure of the 9-item Quality of Life Scale based on acceptable fit indices. Internal consistency, estimated using Cronbach’s alpha and composite reliability, were .91 and .92, respectively, with item-total correlations ranging from .46 to .84. Inter-item correlation coefficients (range = .30–.79), suggesting that all items contribute to the total score. As hypothesized, the quality of life total score was negatively related to the total scores on both the Center for Epidemiologic Studies-Depression (r = –.739) and Davidson Trauma Scale (r = –.537), providing evidence of construct validity of the Quality of Life Scale.
Conclusion:
The Quality of Life Scale is a brief, reliable, valid, unidimensional self-report measure appropriate for use with women who have experienced partner violence. By addressing an important measurement gap, results of this study have potential to advance research on women’s quality of life in the context of partner violence, including improving the evaluation of a growing body of advocacy and health interventions designed to support women’s healing and well-being.
Introduction
As a concept, quality of life (QOL) first emerged after World War II in response to the reality that technological evolutions were prolonging the lives of individuals, but not necessarily “curing” them. 1 Since that time, attention to the burden of chronic health conditions has prompted increased interest in QOL across the health disciplines, yet research has been mired with conceptual and measurement challenges. 2 In 1998, the introduction of the World Health Organization’s definition of QOL provided a common framework for addressing existing tensions. Accordingly, QOL is defined as a broad concept that reflects an “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and social relations” and that is shaped by the individual’s health status, social relationships, and their environment. 3 Thus, QOL is now understood to be a largely subjective indicator of life satisfaction and general well-being 4 that crosses multiple life domains. While researchers at times conflate QOL and health status, they are different concepts. 5 Researchers and theorists continue to debate the underlying domains of QOL and the structural and construct validity of self-report QOL measures; lack of fit between the definition of QOL and the selection of self-report measures used is also a common problem.2,6,7
Attention to these issues is an important aspect of developing reliable and valid QOL measures capable of advancing knowledge about QOL, including in the context of violence and traumatic stress where specific domains may be important. Interpersonal traumas are common and often enduring experiences that have global implications for QOL. 8 Intimate partner violence (IPV), specifically, affects 1 in 3 women globally 9 and results in significant and often enduring health and social risks for women 10 that may undermine their QOL. 11 While there has been growth in research examining QOL among women who have experienced IPV, this body of research is in the early stages of development. Of note, the effectiveness of health and social interventions in improving women’s QOL in the context of IPV has been tested in a few studies.12,13 Given that IPV is a chronic stressor for many women, with impacts that persist over time, QOL is often an appropriate outcome in these and other types of studies, yet existing QOL measures are often lengthy or too generic to be useful. A brief, psychometrically sound QOL measure that captures salient domains of women’s lives in the context of IPV could result in more appropriate assessment of QOL for women with histories of IPV as well as in general populations, and advance knowledge in this important area relevant to women’s health and well-being.
Using data from a community sample of women with histories of IPV, we evaluated the psychometric properties of a brief, theoretically grounded, self-report measure of QOL specifically developed for women who have experienced IPV. 14 While the QOL Scale has shown promise based on limited psychometric testing, evaluation of the scale’s construct validity (including its structural validity) and its utility with women living in different contexts is needed before broader adoption of this measure in research.
QOL among women who have experienced IPV
Given the considerable evidence that IPV is associated with a wide range of negative health, social, and economic consequences for women,10,15,16 when broadly conceptualized, women’s QOL can be considered an indicator of the both the toll of IPV on women’s lives and of their healing from the effects of abuse. Thus, QOL is an important women’s health issue. Findings from qualitative studies17–19 provide consistent evidence that IPV is a distinct stressor with strong negative effects on aspects on various domains of women’s lives, including their level of independence, control, sense of self, relationships, family responsibilities, and safety, and that women’s vulnerability to abuse and poor QOL often continue after separation from an abusive partner.
Some evidence from cross-sectional quantitative research supports an association between severity of IPV and women’s QOL.11,20,21 Although QOL is a broad indicator of general well-being with many domains, such as role function, enjoyment, pleasure, sense of control, emotional and mental health, social integration, physical and financial security, or esteem, these studies have tended to examine only one or two domains. In addition, some of the research22,23 conducted with women who have experience IPV has focussed on a related concept, health-related quality of life (HRQOL), defined as a person’s subjective perception of their ability to engage in activities that are important to them. 24 Poorer overall QOL and HRQOL have been documented among women with histories of IPV (compared to those who have not experienced IPV), including women from the general population.14,22,23 For example, in a study of 3496 European men and women with histories of IPV, negative relationships were found between the physical and mental components of the Short-Form Health Survey (SF-36), a measure of HRQOL, and the severity of IPV they experienced. 23 As this example illustrates, consistent with the broader QOL literature 25 studies conducted with women who have experienced IPV often use the terms QOL and HRQOL interchangeably, and employ QOL measures that are a mismatch with the conceptualization used. Failure to differentiate between these two concepts makes it difficult to reliably interpret results across studies. In the context of IPV, a narrow focus on HRQOL may result in overlooking QOL domains, such as safety or social connections, that are important to women who have experienced violence, but may be less important in other contexts.
Importantly, there is some evidence that women’s QOL in the context of IPV can change over time, either based on longitudinal cohort studies 15 or studies testing the effectiveness of complex advocacy or health interventions. For example, in a now classic randomized controlled trial of women in the United States, a post-shelter advocacy intervention was found to be effective in improving women’s QOL and social support and decreasing IPV.14,26 More recently, in two Canadian studies27,28 testing a health promotion intervention for women who had separated from an abusive partner, including one study with Indigenous women, significant pre–post intervention changes in women’s QOL, mental health, and other outcomes were found, with these changes maintained 6 months after the intervention ended. Bybee and Sullivan’s 26 process analysis also suggested that short-term improvements in QOL in response to their advocacy intervention reduced future re-victimization, suggesting that QOL might be both an outcome and a mediator of intervention effects. These types of analyses, while seldom published, can yield important insights about the complex mechanisms that explain the relationships among IPV, women’s resources, their health, QOL, and the social conditions of their lives. This is a critical gap in need of exploration.
Measurement of QOL in the context of IPV
Researchers who have examined QOL among women with histories of IPV have employed different QOL measures, including the SF-36 and SF-12 Health Survey, World Health Organization QOL scales (WHOQOL), and the 9-item QOL Scale developed by Sullivan and Bybee. 14 Developed in the 1990s by the Rand Corporation, 29 the Medical Outcomes Short-Form 36 (SF-36) is a self-report tool organized around eight QOL domains (i.e. physical functioning, social functioning, role limitations due to physical problems, mental health, energy, bodily pain, and general health perceptions). The Short-Form 12 (SF-12, SF-12v2) and Short-Form Six-Dimension (SF-6D) are abbreviated measures derived from the original SF-36. However, these scales focus on HRQOL, rather than capturing QOL across a broad range of domains. As previously noted, research on QOL has been critiqued for poor fit between the conceptualization and measurement of QOL25,30 and, in the context of IPV, for failing to capture QOL domains, such as safety, relationships, and control, that are most salient to this population. 31
The WHO QOL group created a series of self-report QOL measures including the WHOQOL-100 32 the WHOQOL-BREF-26 3 and EUROHIS-8. 33 To date, these measures have been widely used 7 including among women with histories of IPV.34–37 The WHOQOL-100 and WHOQOL-BREF-26 are lengthy, multidimensional measures (containing 100 and 26 items, respectively) and designed to measure physical and psychological health, level of independence, social relationships, physical environment, and spirituality/personal beliefs. To address participant burden, two shorter measures (WHOQOL-BREF and EUROHIS-8 Index) have been developed, although these scales exclude questions about safety and emotional well-being that are important dimensions of QOL in the context of IPV.
To respond to gaps in measurement, Sullivan and Bybee 14 developed the QOL Scale drawing, in part, on the social indicators of well-being identified by Andrews and Withey. 38 This conceptual model of QOL focuses on individual perceptions of life as a whole and their affective responses to two interrelated life domains, role-related life situations, and evaluative criteria. For example, satisfaction with family responsibilities (a role-related situation) might depend on how much family members help them achieve success or promote a certain standard of living (if these are important values for them). To develop a brief QOL measure suitable for women who have experienced IPV, Sullivan and colleagues identified nine items, one from each domain captured by Andrews and Withey’s 38 123-item Life Satisfaction Scale, although limited information has been published about the process used to select, adapt, or test the item pool.
The QOL Scale has been used in studies of women who had left an abusive relationship, including participants in a trial evaluating the effectiveness of post-shelter advocacy in the United States14,26,39–41 and in feasibility studies testing a community-based health promotion intervention (iHEAL/Reclaiming Our Spirits) in Canada.27,28 Outside an intervention research context, the QOL Scale has also been used in longitudinal studies examining changes in women’s experience of violence, health and QOL in Canada 15 and women’s help seeking in the United States, 40 although a slightly different version of the scale was used in the latter study. Collectively, these studies support adequate internal consistency reliability of the QOL Scale in diverse community samples in two countries, where Cronbach’s alpha was >.75. However, the construct validity of the QOL Scale, including its structural validity, has not been reported.
In this study, we assessed the psychometric properties of the QOL Scale in a community sample of Canadian women with histories of IPV with a focus on structural validity (factor structure), construct validity (based on testing relationships with theoretically related concepts), and internal consistency. We tested four hypotheses to address the study aims. First, to evaluate structural validity of the QOL Scale, we hypothesized that the nine items would have simple, unidimensional structure. This expectation was based on theoretical grounds, including that which informed the development of the QOL Scale, 38 in which QOL is defined as a broad overarching concept, comprised of multiple domains, but reflecting general well-being and satisfaction with life as a whole.3,38 With respect to construct validity, we hypothesized that the total QOL score would be moderately and negatively associated with total scores on established self-report measures of depression (the Center for Epidemiologic Studies-Depression (CESD) 42 and post-traumatic stress (Davidson Trauma Scale (DTS)) 43 because both of these mental health outcomes have been negatively associated with QOL.15,44 Finally, consistent with previous studies, we hypothesized that the nine items comprising the QOL Scale would demonstrate internal consistency (>.75).
Methods
This study followed the COSMIN Guidelines for patient-reported outcome measures. 45 A quantitative secondary analysis was conducted using data from 250 women who participated in Wave 5 of the Women’s Health Effects Study (WHES), a longitudinal, Canadian study examining changes in women’s health, experiences of IPV, and access to resources over a 4-year period after leaving an abusive partner. 46 Data from Wave 5 were used in this analysis because the QOL Scale was only administered at this time point in the primary study. Secondary analysis is a convenient and cost-efficient approach for extending the use of data beyond the initial purposes for which they were collected. Although secondary analyses are bounded by the type of data that were previously collected, the WHES included the measures we required to conduct psychometric testing of the QOL Scale, including established measures of mental health, important for examining its construct validity. The sample size for planned analyses was also adequate based on COSMIN Guidelines, 45 which classifies samples with 100 or more cases as excellent for studies testing the structural validity of scale with one dimension.
The initial community sample in the WHES included 309 adult (over 18 years) English-speaking women who had left an abusive partner at some point in the 3 years prior to enrollment and were no longer living with an abusive partner. Women were recruited from three provinces (Ontario, British Columbia, and New Brunswick) using advertisements placed in community settings and service agencies that directed women to contact the research team for information or to express interest in participating. A research assistant (RA) used a modified version of the abuse assessment screen (AAS) 47 —including items related to physical abuse, fear of partner, forced sex, and controlling behavior—to confirm exposure to IPV as part of eligibility screening. Eligible women received a verbal description of the study from a RA and were invited to take part in five structured interviews at baseline and 12, 24, 36, and 48 months later. Interviews were conducted in a private location selected by the women or, after the baseline interview, over the phone (if access was limited). Data were collected between 2004 and 2009. 46
The study was approved by Research Ethics Boards at the University of Western Ontario (Protocol # 10128E) and each study site based on the Tri-council Ethics guidelines. 46 Written informed consent was obtained from participants at enrollment and reconfirmed at each data collection session. A detailed safety protocol was used to guide all interactions between women and the research team. 48
Sample
Demographic characteristics of the 250 women who completed Wave 5 are summarized in Table 1. The mean age of participants was 44 years (SD = 9.75, range = 23–68). Women’s educational background varied from 7 to 30 years of formal education, with a mean of 14 years education (SD = 3.270). Most (57.6%) were employed. Women’s annual income ranged from $0 to $80,000CDN/year, with a mean of $28,891.90CDN and median of $20,803CDN (SD = 24,033.79). About half (52%) were parenting children below the age of 18. Some additional diversity was apparent in the sample: 13.6% identified as members of a racialized group, 5.2% identified as Indigenous, and 5.6% reported being born in another country and immigrating to Canada.
Demographic profile of the Wave 5 sample (n = 250).
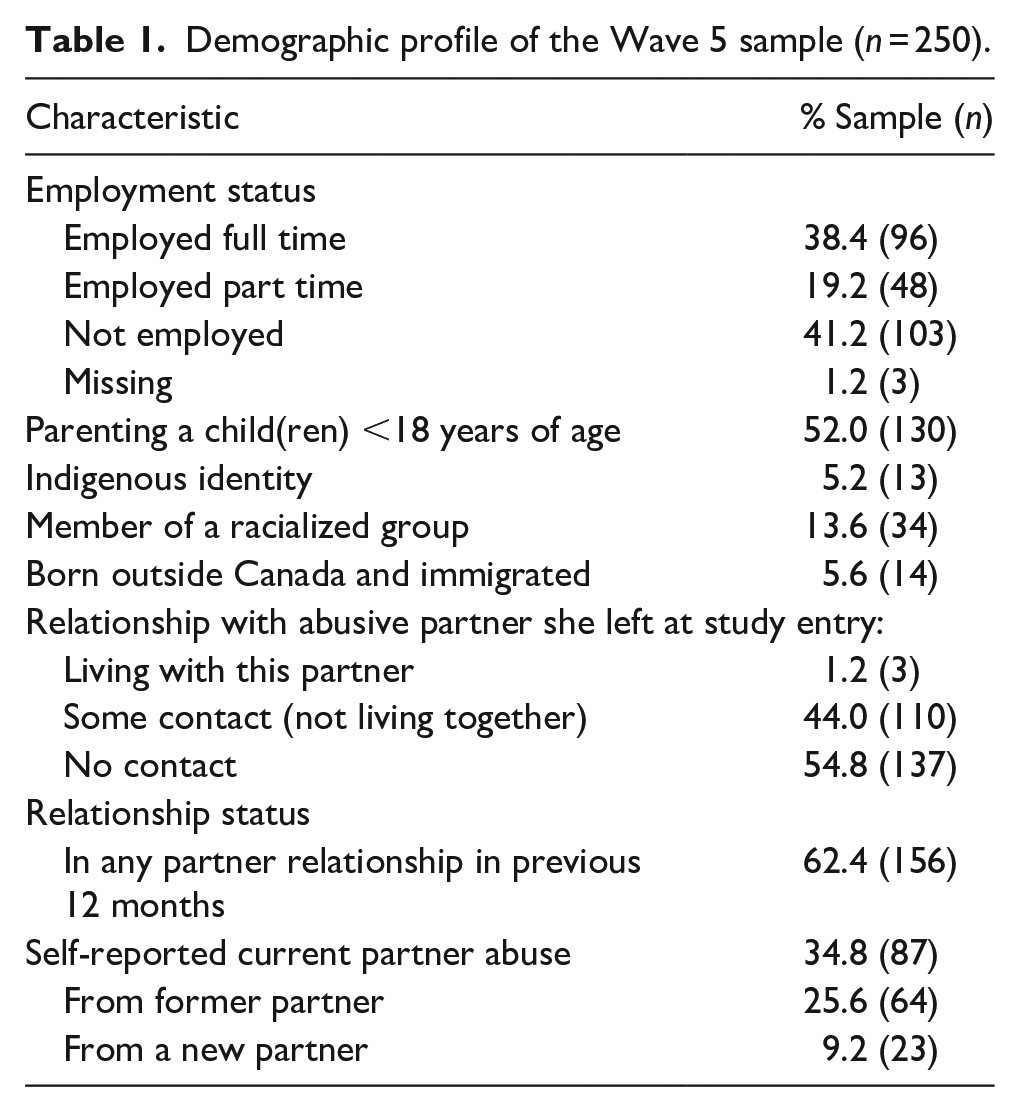
By Wave 5, the majority (62.4%, n = 156) of women reported that they had been in a partner relationship at some point in the previous year. At the time of interview, almost half (45.2%) had contact with the abusive partner they left when the study began 4 years earlier, but only three of these women were living with that partner. However, 34.8% of women (n = 87) reported that they were experiencing current IPV from their former partner (25.6%, n = 64) or a new partner (9.2%, n = 23).
Measurement
This analysis used women’s responses on the QOL Scale along with self-report measures of symptoms of depression and post-traumatic stress disorder (PTSD) to assess construct validity. Women’s responses to questions on a demographic questionnaire were used to describe the sample.
The QOL Scale 14 is a 9-item self-report measure of women’s satisfaction with nine areas of their lives proposed to be important to women who have histories of violence. The first question captures how women feel about their lives as a whole, while the remaining eight questions capture women’s satisfaction with specific aspects of their lives: personal safety, fun and enjoyment, themselves, family responsibilities, accomplishments, independence and freedom, and use of spare time. For each question, women are asked to report their satisfaction using a 7-point Likert-type scale ranging from extremely pleased (1) to terrible (7). All items are reverse-coded and summed to produce total scores ranging from 9 to 63, with higher scores reflecting higher QOL. In the original work by Sullivan and Bybee, 14 internal consistency reliability (Cronbach’s alpha) was .88 with corrected item-total correlations ranging from .56 to .79, suggesting moderate relationships between items in the scale. Internal consistency reliability of the QOL Scale in other studies of women in the United States and Canada has ranged from .84 to .92.15,26,27,41,49 Information about the QOL Scale’s construct validity has not been reported.
The 20-item CESD Scale42,50 was used to measure depressive symptoms. On the CESD, women are asked to report the frequency of symptoms consistent with depression in the previous week using a 4-point Likert-type scale, with responses ranging from none of the time or rarely (0) to most of the time (3). Responses are summed to produce total scores ranging from 0 to 60. Scores ⩾22 are consistent with significant clinical depression, while lower scores (⩾16 and <22) are consistent with mild-to-moderate symptoms. The CESD is a widely used self-report measure that has evidence of reliability and validity in various populations, including women with histories of IPV27,51,52 Internal consistency (Cronbach’s alpha) of the CESD was .78 in our sample.
The 17-item DTS 43 was used to measure post-traumatic stress symptoms. On this summated rating scale, women are first asked to identify the trauma that is most disturbing to them and then, for each of 17 items, to rate the symptom frequency in the past week on a scale ranging from never (0) to daily (4), as well as level of distress (severity) on a scale ranging from not at all distressing (0) to extremely distressing (4). Separate frequency and severity scores are created for each subscale and for all items by summing applicable responses (0 to 68). Total scores are then computed by summing the frequency and severity scores for all items (0–136) and for each symptom cluster. Scores of ⩾40, along with the presence of a minimum number of symptoms in each of three clusters, can be used to reliably classify participants as having symptoms consistent with a DSM-IV diagnosis of PTSD. 53 The DTS has demonstrated acceptable reliability and validity across varied populations.53–55 The internal consistency of the total DTS in this study was .92.
Data analysis
Preliminary analysis revealed that missing data occurred at a low frequency (0%–.8%). Little’s 56 test was used in SPSS version 24 to assess patterns of missing data. Descriptive statistics were computed to inspect the distribution of each variable and the pattern of missing values. Structural equation modeling (SEM) assumes that missing data are missing at random (MAR) or missing completely at random (MCAR). 57 Since the p value for Little’s test was significant, the assumption of MCAR was not confirmed. An item analysis was also run using SPSS to assess reliability (internal consistency) and the extent to which each item was associated with the total score.
The structural validity of the QOL scale was tested using confirmatory factor analyses in MPLUS 8. 58 Missing data were handled in the analysis using the full-information maximum likelihood (FIML) estimator since it has been shown to produce unbiased parameter estimates and standard errors under MAR. The extent to which the model fit the data was assessed using the following indices: comparative fit index (CFI), root-mean-squared error of approximation (RMSEA), chi-square, and standardized root mean square residual (SRMR). These indices were chosen because they are the most insensitive to sample size, parameter estimates, and model misspecification. 59 The CFI is “an incremental fit index (IFI) that is also a goodness-of-fit statistic”; 57 its value ranges from 0 to 1, where 1 reflects “best fit,” with a CFI value of greater than or equal to .95 being recognized as a “good fit.” 60 RMSEA is an absolute fit, where a value of 0 indicates best or exact fit; but because perfect fit is rare, values were interpreted as follows: <.05 is considered close fit; between .05 and .08 is considered fair fit; between .08 and .10 is mediocre fit; and values >.10 is poor fit. 61 Values for the SRMR range from 0 to 1.0, with a well-fitting model having a value of <.05 and values as high as .08 considered acceptable fit. 60 Consistent with SEM analysis, fit indices and modification indices were inspected to determine whether the model could be modified to improve fit. Theoretically reasonable modification indices >4.0 were considered.
Next, the construct validity of the QOL Scale was evaluated by computing bivariate correlations between continuous total QOL scores and total scores for the CESD and DTS. Differences in QOL scores for women who met and did not meet the clinical threshold for depression and post-traumatic stress (using cut scores on the CESD and DTS) were also examined using t tests.
Finally, the internal consistency of the QOL Scale was assessed by computing Cronbach’s alpha and composite reliability coefficients based on omega. Composite reliability, represented by coefficient omega, is a measure based on factor loadings. It can be calculated in two ways: using the variance–covariance matrix or correlation matrix. 62 It is considered a superior choice for reliability in SEM because it draws on the standardized regression weights and measurement errors for each item. 63
Results
Descriptive statistics for each item on the QOL Scale and for the total score are shown in Table 2. The mean of each item was relatively high (ranged from 4.56 to 5.63 on a 7-point scale), with the highest and lowest means observed for personal safety and fun and enjoyment, respectively. Based on recommendations proposed by Kline, 64 the absolute values for skewness index (SI) and kurtosis index (KI) were inspected and showed that the data were normally distributed given that SI <3 and KI < 10 for all items.
Item-level descriptive statistics, item-total correlations, and internal consistency of items on the QOL Scale (n = 249).

QOL: quality of life and SD: standard deviation.
The descriptive statistics for the total score were as follows: M = 43.74, SD = 11.34, and range = .46–.90. Skewness was –.54 and kurtosis was –.34, reflecting a normal distribution. The mean total QOL score in this study was higher (more positive) than that reported in two Canadian studies conducted with women who had separated from an abusive partner in the previous 3 years (M = 39.2) 27 and Indigenous women with histories of IPV and who were living with significant structural and social inequities (M = 38.6). 28 However, the majority of the women in our sample had separated from an abusive partner up to 7 years prior had no contact with them. The mean score in our sample is equivalent to a score of 4.86 on the 7-point scale used in the response options. Using this conversion, mean scores in this study are only slightly higher (more positive) than baseline scores reported by Sullivan and Bybee 14 (M = 4.47 for intervention group and 4.30 for control group) in a sample of women from the United States who were leaving a domestic violence shelter.
Structural validity of the QOL scale
A confirmatory factor analysis of the nine items on the QOL Scale was conducted in MPLUS 8 and model fit assessed using several goodness-of-fit indices. The chi-square test was statistically significant (chi-square = 88.951, p < .0001) but the one-factor model was not rejected because the chi-square statistic is sample sensitive 65 and the remaining fit indices suggested a good fit between the model and data (CFI = .958, TLI = .944, RMSEA = .096, and SRMR = .034). Factor loading for the items ranged from .49 to .90, indicating that the 9-item solution was acceptable (Table 3), supporting our hypothesis.
Factor loadings for QOL items: one-factor solution.

Construct validity of the QOL scale
As hypothesized, the QOL total score was moderately and negatively related to the total score on the DTS (r = –.537) and showed a moderate to strong association with the total score on the CESD (r = –.739). Furthermore, mean QOL Scale scores were significantly lower for women whose scores for depression fell above the threshold (⩾22) for clinical significance on the CESD (M = 37.9 and SD = 11.28) compared to those with scores below this threshold (M = 50.6 and SD = 6.64), t(244) = 10.49, p < .001. Similarly, women with PTSD scores that met the threshold for clinical significance on the DTS (⩾40) had significantly lower QOL scores (M = 34.6 and SD = 11.08) than women who did not meet the threshold for PTSD (M = 47.3 and SD = 9.28), t(244) = 9.10, p < .001. These results provide initial support for the construct validity of the QOL Scale based on hypothesis testing.
Internal consistency
The internal consistency of the QOL estimated using Cronbach’s alpha and composite reliability (.91 and .92, respectively) was acceptable for all nine items, with item-total correlations ranging from .46 to .84. Inter-item correlation coefficients ranged from .30 to .79 (M = .56) for the full scale (Table 4), suggesting that all items contributed to the total score and no items were redundant.
Polychoric correlations among items on the QOL Scale.

Discussion
This research assessed the psychometric properties of the QOL Scale, a brief self-report measure developed specifically for women with histories of IPV. To our knowledge, this is the first published analysis to investigate the structural validity of this scale using confirmatory factor analysis. As hypothesized, the results suggest that the QOL Scale has a simple structure comprised of nine items. Furthermore, evidence of construct validity was supported through the moderate-to-high correlations found between the QOL Scale and established symptom-based measures of depression (CESD) and PTSD (DTS), and by observed differences in QOL for women who did and did not meet the threshold for clinically significant mental health concerns. Internal consistency reliability for the full scale was acceptable based on both alpha and omega, results that are consistent with previous studies conducted with samples of women who had separated from an abusive partner, recruited from shelters in the United States41,49 or from the community in Canada.27,28 Thus, this study provides evidence of structural and construct validity and internal consistency of the QOL Scale among Canadian women with histories of IPV, with implications for measurement beyond this context.
New evidence of sound psychometric properties of the QOL Scale increases its potential to advance research on QOL among women with histories of IPV. Studies that explain the mechanisms by which IPV affects women’s QOL are needed to inform policies, programs, and practices aimed at improving women’s QOL. In the context of separating from an abusive partner, QOL is a “proxy” for women’s well-being and life satisfaction, important aspects of creating a new life. 65 The QOL Scale is particularly promising as an outcome measure in a growing body of research testing the effectiveness of advocacy and health interventions and programs for women with histories of IPV, 10 particularly where the intended effects are broad and extend beyond a focus on women’s safety. Bybee and Sullivan’s26,41 trial of post-shelter advocacy as well as feasibility studies of the efficacy of the Intervention for Health Enhancement and Living (iHEAL)27,28 have already demonstrated that the QOL Scale is responsive to change resulting from interventions delivered by trained advocates 14 or registered nurses.27,28 This is important given that improvements in women’s QOL have been associated with a reduction in IPV re-victimization 66 and increased capacities after separation. 27 Understanding whether changes in women’s QOL also lead to improvements in other health, social and economic outcomes that have been negatively affected by IPV, is a priority area for future study.
While there is value in understanding HRQOL, this narrower concept is different from the broader conceptualization of QOL which informs the QOL Scale, with important implications for measurement of QOL. Researchers who study HRQOL tend to focus on physical and mental functioning and appropriately use self-report measures such as the SF-36, SF-12, and SF-86,23,31,67 to do so. In the context of IPV, the QOL Scale offers several advantages, including its brevity and inclusion of a range of specific aspects of QOL, such as safety, accomplishment, and autonomy, which are important to women with histories of IPV but not captured by HRQOL measures. The consequences of IPV include more than visible physical injuries, but often extend to long-term effects on women’s mental and physical health, relationships, living conditions, finances, and safety for themselves and for their families.19,68–70 The ability to measure different aspects of women’s life quality has the potential to yield more comprehensive and appropriate assessment, while enhancing understanding about the differential impacts of IPV on the many different facets of women’s lives.
Both Sullivan’s QOL Scale and the WHOQOL measures tap a broad number of domains; as previously noted, each scale has evidence supporting its reliability and validity and has been used in studies of women experiencing IPV. The domains captured by each scale should be considered in making decisions about which scale to use in a particular study. The WHOQOL measures a range of general dimensions that are not necessarily specific to women who have experienced IPV, while the QOL Scale includes domains that are particularly important for women who have experienced IPV. When these specific domains, such as safety and sense of control, are important to a study, the QOL Scale may be a more appropriate option.
Strengths and limitations
This analysis provides evidence supporting the reliability and validity of the QOL Scale in a relatively diverse community sample of Canadian women with histories of IPV. It extends psychometric testing of this measure beyond previous studies, with a particular focus on structural and construct validity, using data that were adequate for the analysis. Some limitations should be considered. The data used in the analysis were originally collected to examine women’s mental and physical health after separation from an abusive partner and not to conduct a psychometric analysis of the QOL Scale; thus, the availability of measures to assess construct validity of the QOL scale was limited. In future studies, the WHOQOL index, a gold standard general QOL measure, should be used to examine criterion-related validity of the QOL Scale. Items on the QOL Scale tap different aspects of QOL that should be appropriate to women from different populations. However, it is possible that some items may be less relevant in some contexts. For example, “freedom to live as you want” or “how you spend your personal time” may not be as relevant in contexts where social norms favor the common good over individual freedom or welfare and/or where there is no expectation of having time for personal needs. Additional testing the QOL Scale across different cultural contexts is warranted; this would require a larger sample of women from varied backgrounds.
Finally, while the QOL Scale is a broad measure, it may not include all salient domains. This analysis did not attempt to test new items alongside the existing nine items. Future research should assess the need to further refine this scale by adding items that tap some additional domains (e.g. finances, housing, and health) that reflect long-standing issues for women who have experienced IPV,16,69–71 followed by re-evaluation of the psychometric properties of the revised scale.
Conclusion
The QOL Scale is a brief, reliable, valid, unidimensional self-report measure appropriate for use with women who have experienced IPV. Results of this study extend evidence about the psychometric properties of this scale and provide the first evidence supporting its structural and construct validity using data from a community sample of Canadian women with histories of IPV. While additional testing is needed in different contexts, the QOL Scale offers a promising approach for advancing research on women’s QOL in the context of IPV, including evaluating the impacts of a growing body of advocacy and health interventions and programs for these women and examining the complex mechanisms by which such intervention exert positive effects.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221125574 – Supplemental material for Structural and construct validity of the Quality of Life Scale among Canadian women with histories of intimate partner violence
Supplemental material, sj-docx-1-whe-10.1177_17455057221125574 for Structural and construct validity of the Quality of Life Scale among Canadian women with histories of intimate partner violence by Diana Jaradat, Marilyn Ford-Gilboe, Helene Berman and Carol Wong in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.