
Abstract
Introduction:
Although vitamin D is widely known as an essential micronutrient during pregnancy, the exact supplementation dose to prevent maternal–fetal outcomes remains a question. This study aims to provide a systematic review and a meta-analysis of data from randomized controlled trial on > 2000 IU/day vitamin D supplementation compared to ⩽ 2000 IU/day; and ⩽ 2000 IU/day compared to placebo, on their effects on the incidence of preeclampsia, gestational diabetes mellitus, preterm birth, and differences on birth weight.
Methods:
A systematic literature search on PubMed, EBSCO-MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials databases was carried out to evaluate randomized controlled trial studies on the effects of oral vitamin D > 2000 IU/day versus ⩽ 2000 IU/day; and ⩽ 2000 IU/day versus placebo, on preeclampsia, gestational diabetes mellitus, preterm birth and birth weight. Risk ratio, mean difference, and 95% confidence interval were calculated.
Results:
There were a total of 27 randomized controlled trials selected. Maternal vitamin D supplementation > 2000 IU/day had a positive effect only on gestational diabetes mellitus (seven randomized controlled trials; risk ratio = 0.70, 95% confidence interval: 0.51–0.95, I2 = 0). Vitamin D supplementation ⩽ 2000 IU/day has reduced the risk of preeclampsia (three randomized controlled trials; risk ratio = 0.29, 95% confidence interval: 0.09–0.95, I2 = 0), with no significant difference when compared to > 2000 IU/day (eight randomized controlled trials; risk ratio = 0.80, 95% confidence interval: 0.51–1.24, I2 = 31). No difference in preterm birth risk and birth weight after vitamin D supplementation. The quality of evidence varies from moderate to very low certainty. The risk of preeclampsia and gestational diabetes mellitus after high-dose versus low-dose vitamin D supplementation was the ones with moderate certainty.
Conclusion:
Vitamin D supplementation > 2000 IU/day might be important to reduce the risk of gestational diabetes mellitus. Lower dose vitamin D supplementation (⩽ 2000 IU/day) seemed adequate to reduce the risk of preeclampsia, with no significant difference compared to the higher dose.
Introduction
Vitamin D deficiency during pregnancy is prevalent globally. Its prevalence ranges from 9% to 94%, depending on country, race, ethnicity, skin color, clothing customs, and dietary intake.1,2 A recent study from seven countries found a prevalence range from 39.4% to 76.5%. Another study that included 17 trials suggested that low vitamin D status prevalence was especially high in developing countries.1,3 Contrary to the epidemiological association, studies investigating the effectiveness of vitamin D supplementation in preventing pregnancy complications have shown inconsistent results. 4 Vitamin D deficiency is associated with pregnancy complications, such as preeclampsia (PE), gestational diabetes, and low birth weight. 5 Some studies have proposed that vitamin D deficiency interferes with maternal immune tolerance toward embryo implantation. 6
This has unfortunately led to differing intake and supplementation dosing recommendations among organizations. For example, World Health Organization7,8 recommends a daily nutrient intake of vitamin D at 200 IU/day, with no supplements recommended as part of the antenatal routine. The Royal College of Obstetricians and Gynaecologists (RCOG) recommended 400 IU/day for all pregnant women, 800 IU/day for women at risk of PE, and 1000 IU/day for other high-risk women. 9 The daily intake recommendation of vitamin D dosage by the Institutes of Medicine (IOM) was 400–600 IU/day, with upper safety limit was up to 4000 IU/day. 10 The endocrine society has suggested that the minimum daily supplementation for pregnancy was 1400 IU, with the upper limit 10,000 IU/day. 10 These recommendations were based on optimal circulating 25-hydroxyvitamin (OH) D concentration and adverse effects prevention, such as hypercalciuria. However, other experts recommend that higher vitamin D level maintenance could be achieved through high-dose vitamin D supplementation. 11 And thus, the exact dose on the effect to prevent maternal–fetal outcome is still a question.
In 2019, two Cochrane reviews on vitamin D supplementation in pregnancy were published. In review, the dose of vitamin D was not taken into account, whereas the other one used cut-offs of 600 IU/day, which was the recommended dose, and 4000 IU/day, which was the upper limit dose.5,12 However, based on the American College of Obstetricians and Gynecologists (ACOG), in vitamin D in pregnancy, most experts agree that 1000–2000 IU/day is safe.
Therefore, our study aims to provide a systematic review and a meta-analysis of data from randomized controlled trial (RCT) on > 2000 IU/day vitamin D supplementation compared to ⩽ 2000 IU/day; and ⩽ 2000 IU/day when compared to placebo, on their effects toward the incidence of PE, gestational diabetes mellitus (GDM), preterm birth (PTB), and differences on birth weight.
Materials and methods
Literature search
Two authors independently performed a systematic literature search in PubMed, EBSCO-MEDLINE, Cochrane Central Register of Controlled Trials, and EMBASE databases (R.H. and A.W.L.).
The search used the following MeSH terms, and Boolean operators are shown in supplemental files. All studies published from inception until April 2022 were included in the search without language restrictions. Ethical approval was not necessarily required for this study because the study was based exclusively on published literature with no personal information collected. 13
Inclusion and exclusion criteria
The inclusion criteria used in this systematic search were as follows: (1) RCT; (2) pregnant women of any gestational age; (3) vitamin D alone which is tested as the intervention, or except when other micronutrients are similarly used in both intervention and control groups; (4) the control in the study is either lower dose vitamin D, or placebo/no supplement, or other micronutrients which are equivalently used by the intervention groups; and (5) the outcomes assessed included but were not limited to PE, gestational diabetes, PTB, and birth weight.
However, the exclusion criteria included were as follows: (1) multiple pregnancy; (2) the subjects were pregnant women who were already diagnosed with pregnancy complications prior to enrollment; (3) other micronutrients were used on the intervention group in combination with vitamin D, but not equally given to the control group; and (4) values of the targeted outcome were unavailable. For studies with more than two intervention groups, the disaggregated data were combined to create a single pair-wise group. 14
Study selection and data extraction
Two independent authors (R.H. and A.W.L.) selected the studies from the databases and extracted the necessary information from the eligible studies, which included first author’s last name, year of publication, country where the study was performed, number of participants, age and gestational age, baseline of 25(OH)D serum, information about vitamin D intervention (i.e. formulation, regimen, method of administration, and treatment duration), the incidences of PE, gestational diabetes, PTB, and birth weight. The studies were selected and categorized based on their regimens; 2001 IU/day or more versus 2000 IU/day or less, and 2000 IU/day or less versus placebo or no supplement. The extracted data were entered into Review Manager software (RevMan, version 5.4, Copenhagen, Denmark) by R.H. and cross-checked for accuracy by A.W.L. Any disagreements during study selection and data extraction between R.H. and A.W.L. were resolved by discussion and consensus with another author (R.I.).
Risk of bias and quality assessment
The risk of bias from each eligible and selected study was evaluated using the Cochrane Collaboration’s tool RoB 2.0 (a revised Cochrane risk-of-bias tool for randomized trials), 15 which included the following criteria: random sequence generation (selection bias); concealment of the allocation sequence (selection bias); blinding of participants and personnel (performance bias); blinding of outcome assessment (detection bias); incomplete outcome data (attrition bias); selective outcome reporting (reporting bias); and other biases. The quality assessment of each study was performed based on the framework of Grading of Recommendations Assessment, Development and Evaluation (GRADE), 16 which considered risk of bias, inconsistency, indirectness, imprecision, and publication bias. The risk of bias and quality assessments were performed by two independent authors R.H. and A.W.L. with any disagreements resolved by consensus and discussion with another author (R.I.).
Statistical analysis
The dichotomous data of PE, gestational diabetes, and PTB were presented as risk ratio (RR) with 95% confidence intervals (CI), whereas the continuous birth weight data were presented as weighted mean difference (MD) with 95% CI, both were presented as forest plots. The significance of pooled effect size was determined using the Z-test where p-value less than 0.05 was considered significant. The heterogeneity across studies was assessed using the Q-test based on the χ2 statistic, where p-value less than 0.1 was considered statistically significant. To quantify the level of heterogeneity, the I2 value was calculated, where an I2 value of 0% indicates “no heterogeneity,” whereas 25% is “low,” 50% is “moderate,” and 75% is “high” heterogeneity, and statistically significant heterogeneity is when I2 value is more than 30%. The random-effects model (Der Simonian–Laird method) was used based on the decision flow chart for selecting a statistical model related to clinical and methodological heterogeneity of studies and the number of included studies. 17
Sensitivity analysis was then performed using a leave-one-out approach to assess whether a particular omission could affect effect sizes and heterogeneity. Finally, if studies for selected outcomes were more than 10, the presence of publication bias would be assessed visually using funnel plot asymmetry and statistically by Begg’s test and Egger’s regression asymmetry test.
Results
Study selection
The study selection steps followed the PRISMA flow diagram (2020) as shown in Figure 1. There were 2.701 abstracts retrieved from the databases, with 2.105 excluded during the titles/abstract screening. In total, 103 articles were subjected for a full-text review. From these, 76 studies were excluded due to inappropriate regiments, wrong outcome, wrong population, and not RCT study. There were a total of 27 studies included in this review, with details shown in Tables 1 and 2. There were 19 studies18–36 comparing higher and lower dose of vitamin D (Table 1), 11 studies24,30,35,37–44 comparing lower dose and placebo/no supplement (Table 2), and 3 studies having both of the comparison.

PRISMA flow diagram of study selection.
2001 IU/day or more versus 2000 IU/day or less.

Ca: calcium; PE: preeclampsia; GDM: gestational diabetes mellitus; PTB: preterm birth.
2000 IU/day or less versus placebo or no supplement.

Ca: calcium; PE: preeclampsia; GDM: gestational diabetes mellitus; PTB: preterm birth.
Systematic review
In total, there were 27 studies included with which 14 from Asian countries, 6 from USA, 5 from European countries, and 2 from Australia and New Zealand. There were more than 8000 pregnant women reported in this study, including 3436 pregnant women from PE studies, 1905 pregnant women from GDM studies, and 5166 pregnant women from PTB studies. The duration of supplementation of vitamin D was ranged from 8 to 26 weeks of gestational age to delivery. The birth weight was reported from newborns, with 1336 newborns from mothers supplemented with > 2000 IU/day, 2346 newborns from mother supplemented with ⩽ 2000 IU/day, and 1217 newborns from mothers received placebo or no supplementation. Almost all studies used vitamin D3 (cholecalciferol) as the type of supplementation, with only three studies using vitamin D230,35,38 and two studies did not specify the type of vitamin D supplementation they used.39,42
In total, 19 studies compared > 2000 IU/day and ⩽ 2000 IU/day.18–29 Among those, there were four studies where other micronutrients were given as a combination for both the dosages of vitamin D supplementation,19,21,24,34 while other studies investigated vitamin D supplementation only. In studies with intervention given > 2000 IU/day, there were eight studies where the intervention was given every day, with the least amount given was 3800 IU/day and the highest was 6000 IU/day. Moreover, there were two studies where the intervention was given weekly with the least amount was 16,800 IU/week in weekly schedule, 24 the highest was 50,000 IU/week, 19 and one study with single dose 70,000 IU followed by 35,000 IU/week. 23 Following this, two studies used vitamin D supplementation 50,000 IU/2 weeks in biweekly schedule.21,29 One study also gave a single dose of vitamin D 300,000 IU per trimester. 31
In comparing vitamin D supplementation ⩽ 2000 IU/day and placebo or no treatment, 11 studies included.24,30,35,37–44 Among those, one study used calcium as a combination of treatment in both groups, 39 and two studies combined other supplementations in both groups.24,42 Almost all the interventions were given daily, with the least amount was 400 IU/day and the highest was 2000 IU/day. Only the study by Roth 2018 used a weekly intervention of 4200 IU/week. 24
Meta-analysis
Preeclampsia
Three RCTs found the effect of vitamin D supplementation ⩽ 2000 IU/day on PE risk. Vitamin D ⩽ 2000 IU/day significantly reduced (p < 0.05) the occurrence of PE with RR = 0.29, 95% CI = 0.09–0.95. These studies have no heterogeneity, shown by Q-test and I2 value (p = 1.00, I2 = 0%).
However, the comparison of > 2000 and ⩽ 2000 IU/day vitamin D supplementation on PE was found in eight studies. With moderate heterogeneity, (I2 = 31%), supplementation of > 2000 IU/day was considered protective with RR = 0.80. However, the CI crossed the line of no difference at the value of 1 (95% CI = 0.51–1.24), and is hence not statistically significant. The forest plots are shown in Figure 2.

Forest plot of different vitamin D dosage on the occurrence of PE. (a) ⩽ 2000 IU/day versus placebo. (b) ⩾ 2001 versus ⩽ 2000 IU/day.
Gestational diabetes mellitus
The effect of vitamin D supplementation ⩽ 2000 IU/day on GDM was assessed in only two RCTs. From these studies, we found that vitamin D ⩽ 2000 IU/day has no significantly different effect compared to placebo on GDM (p = 0.69, RR = 0.92, 95% CI = 0.59–1.42). No heterogeneity was also found in this analysis with Q-test and I2 value (p = 0.52, I2 = 0%).
Furthermore, the comparison between > 2000 and ⩽ 2000 IU/day vitamin D in seven studies showed that the incidence of GDM was significantly reduced in the > 2000 IU/day group (p = 0.02, RR = 0.70, 95% CI = 0.51–0.95). There was also no heterogeneity found in this meta-analysis with I2 = 0%. The forest plots are shown in Figure 3.
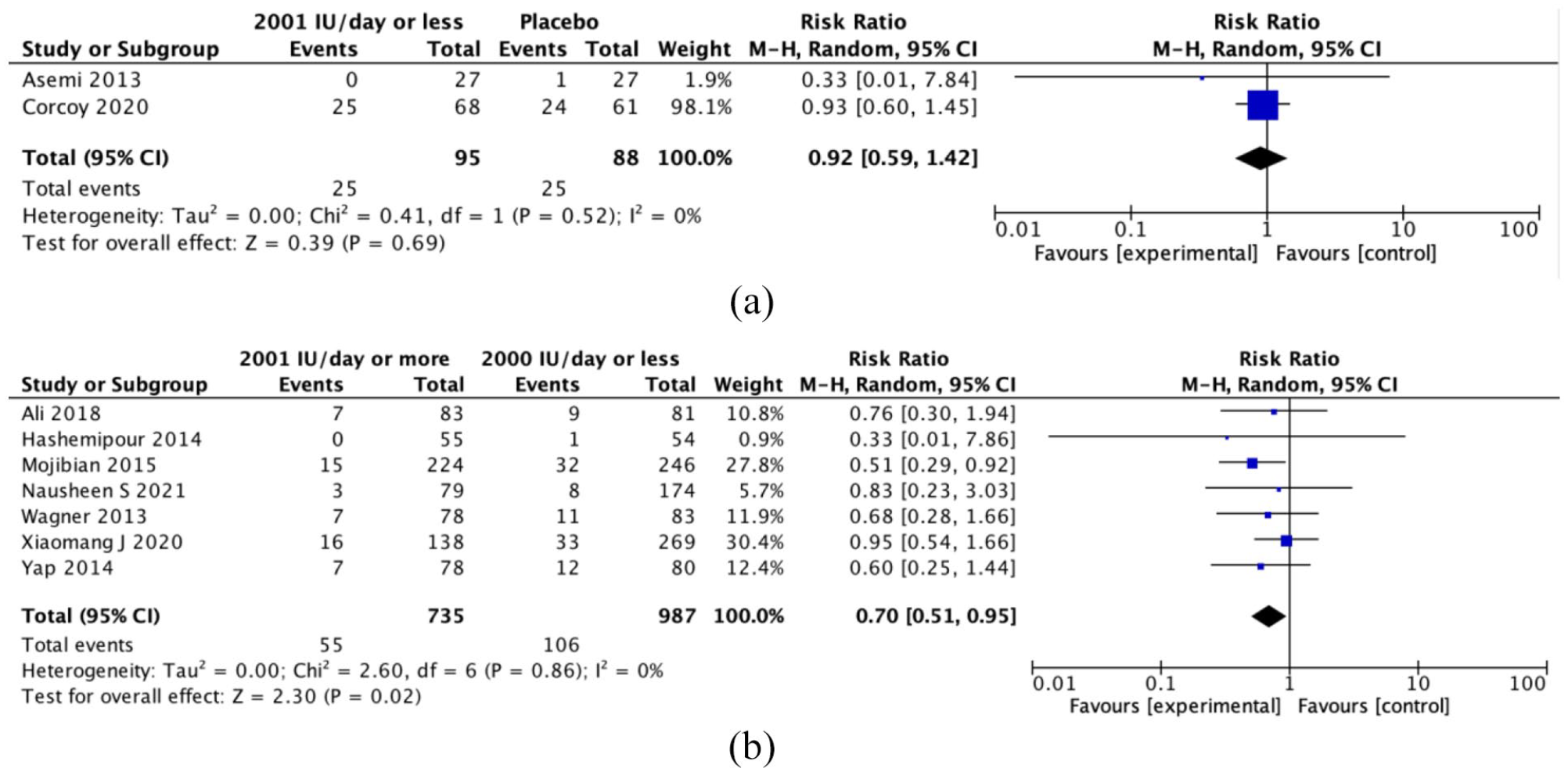
Forest plot of different vitamin D dosage on the occurrence of gestational diabetes mellitus: (a) ⩾ 2001 IU/day versus placebo. (b) > 2000 versus ⩾ 2001 IU/day.
Preterm birth
The effect of vitamin D supplementation ⩽ 2000 IU/day on PTB was assessed in six RCTs. From these studies, we found that vitamin D ⩽ 2000 IU/day has no different effect compared to placebo on PTB (p = 0.57, RR = 0.84, 95% CI = 0.46–1.53). However, the heterogeneity was also considered high with Q-test and I2 value (p = 0.1, I2 = 42%). Therefore, we did a leave-one-out sensitivity analysis to identify single source of heterogeneity across studies. As the study from Naghshineh 2016 omitted, the heterogeneity decreased with p = 0.77, I2 = 0%. The result was still not significant with RR = 1.07, 95% CI = 0.71–1.63.
Moreover, there were 10 RCTs with regard to the > 2000 and ⩽ 2000 IU/day vitamin D comparison. The result was similar as ⩾ 2001 IU/day vitamin D versus placebo, where no significant difference across studies (p = 0.90, RR = 1.01, 95% CI = 0.82–1.26) was found. We also did not find heterogeneity across the studies (I2 = 0%). The forest plots are shown in Figure 4.
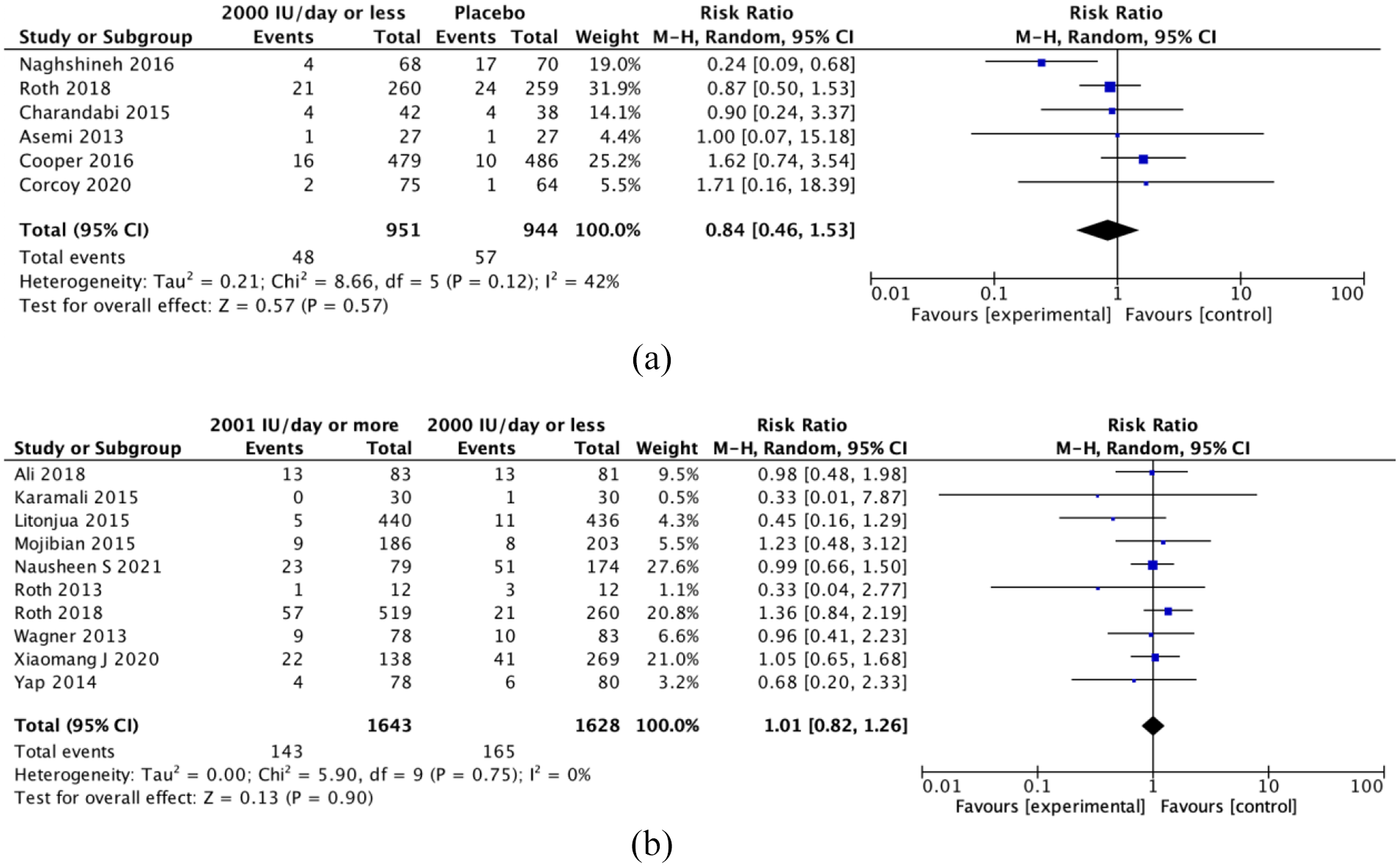
Forest plot of different vitamin D dosage on the occurrence of PTB. (a) ⩾ 2001 IU/day versus placebo. (b) > 2000 versus ⩽ 2000 IU/day.
Birth weight
The effect of vitamin D supplementation ⩽ 2000 IU/day on birth weight was assessed in 10 RCTs. From those studies, we found that vitamin D ⩽ 2000 IU/day has no significant difference compared to placebo on birth weight (p = 0.84, MD = 8.46, 95% CI = 71.38–88.30). The heterogeneity was also considered very high with Q-test and I2 value (p < 0.001, I2 = 91%).
In addition, there were 14 RCTs in comparing vitamin D supplementation > 2000 and ⩽ 2000 IU/day. The result was also considered not significant as p = 0.75, with MD = 10.23 (95% CI = 74.05–53.59 g). The heterogeneity was also too high, as it reached the value of Q-test < 0.001 and I2 = 70%. There were also no significant changes of the heterogeneity after sensitivity analysis for both outcomes. The forest plots are shown in Figure 5.

Forest plot of different vitamin D dosage on birth weight. (a) ⩾ 2001 IU/day versus placebo. (b) ⩾ 2001 versus ⩽ 2000 IU/day.
Risk of bias and quality assessed
The result of Cochrane Risk of bias assessment is shown in Figure 6. Overall, most studies had low risk of bias, despite some studies having a high risk of bias in almost each type of bias, though less than 25%. The reporting bias was the only type of bias with no high risk of bias reported, but the unclear risk was reported in a quarter of the studies. For the three meta-analyses with at least 10 studies, we detected some asymmetry in the funnel plots which can be attributed to high heterogeneity between studies (funnel plots were shown in the supplemental files).

Risk of bias assessment 2.0 of randomized controlled trials included in the meta-analysis: (a) risk of bias summary and (b) graph.
Nevertheless, the quality of evidence varies. Preeclampsia and GDM studies of high-dose versus low-dose vitamin D showed moderate certainty, while studies of low-dose vitamin D versus placebo showed low certainty. In contrast to PTB studies, low-dose vitamin D versus placebo showed moderate certainty, while high-dose versus low-dose showed low certainty. Birth weight studies were shown to have very low certainties as both showed a high level of heterogeneity, asymmetry funnel plots, with studies which were considered to have a high risk of bias. No meta-analysis was considered to have a high quality of evidence.
Discussion
To interpret the results on different doses of vitamin D on maternal–fetal outcomes, the type of intervention and study design of the included studies must be carefully analyzed. To minimalize the heterogeneity effect, we only included RCTs study in pregnant women without pregnancy complications. Here, we compared vitamin D supplementation only, without combinations with other micronutrients, to ensure its specific effect for a specific dose range.
A systematic review suggested that either vitamin D alone, or in combination with calcium, is effective in preventing preeclampsia. 45 The pathogenesis of preeclampsia, which includes pro-inflammatory cytokine secretion, can be reduced by vitamin D supplementation by inhibiting TLR4 monocyte expression. 46 Our findings show that vitamin D supplementation ⩽ 2000 IU/day has a significant effect (p = 0.04) in preventing preeclampsia compared to placebo (OR = 0.29, 95% CI = 0.09–0.95). This finding is also supported by a previous meta-analysis which suggested that vitamin D supplementation was associated with a reduced risk of preeclampsia (OR = 0.37, 95% CI = 0.26–0.52). 47 This showed us that vitamin D supplementation is required for pregnancy, consistent with other studies with a wide range of vitamin D dosages. 5 Regarding the higher dose effect, we found no significant difference between > 2000 and ⩽ 2000 IU/day in the risk of preeclampsia (OR = 0.80, 95% CI = 0.51–1.24). Another study by Cochrane also showed a different dose of vitamin D supplementation; ⩽ 4000 versus ⩾ 3999 IU/day and ⩽ 601 versus ⩾ 600 IU/day. Although both results showed protective relative risk, they were not statistically significant, with a wide range of confidence interval (RR = 0.87, 95% CI = 0.62–1.22 and RR = 0.96, 95% CI = 0.65–1.42). 12 Together with our results, these data suggest that antenatal vitamin D supplementation is essential to reduce the risk of preeclampsia, but the effective dose is between 601 and 2000 IU/day. Dosage of supplementation of more than 2001 IU/day has no different effect from the lower dose.
Studies have shown that most pregnant women with GDM have vitamin D deficiency.48,49 Recent study in GDM prevention suggested that vitamin D supplementation compared to placebo reduced the risk of GDM with RR = 0.51, 95% CI = 0.27–0.97. 50 In our study, a meta-analysis from seven studies suggested that there was a significant difference of higher dose vitamin D supplementation (> 2000 IU/day) compared to the lower dose (⩽ 2000 IU/day with p < 0.05, RR = 0.70, 95% CI = 0.51–0.95), along with no significant difference in the lower dose compared to placebo. Another systematic review showed no difference in ⩽ 4000 versus ⩾ 3999 IU/day and ⩽ 601 versus ⩾ 600 IU/day dosage. 12 This is in agreement with a previous study which also showed that vitamin D 2000 IU/day was more effective in increasing the 25(OH)D serum concentration than a dose lower than that (400 IU/day). 51 Thus, it may be suggested that the optimum dose for vitamin D supplementation to prevent GDM should range from 2001 to 4000 IU/day.
Moreover, a study found that 25(OH)D serum level was related to preterm birth incidence, as the preterm birth rate decreases in serum level 90 nmol/L. 52 A gene expression study also showed dysregulation of immune response in insufficient vitamin D levels during early pregnancy, contributing to preterm birth. 53 However, our study did not find any significant effect of different vitamin D supplementation dosage in preterm birth. This result is supported by other previously published systematic reviews and meta-analyses, which also found that there was no significant effect of vitamin D supplementation on preterm birth compared to placebo nor when a dosage of 600 IU/day was compared to 4000 IU/day.5,12
Furthermore, our study found no significant effect of vitamin D supplementation on birth weight. This contrasts with a previous systematic review of 43 trials suggesting that vitamin D increased birth weight and prevented small for gestational age. 54 Nonetheless, a mendelian randomization study using genetic instruments on maternal 25(OH)D levels found a positive effect on offspring birth weight, yet the effect was considered small thus unlikely to be clinically important. 55 Therefore, with these contrasting results, it seems that more studies are required for us to draw a conclusion on the effect of vitamin D supplementation on birth weight, although our study reports non-significance.
Our study found several similarities and differences compared to the previous meta-analysis findings. In general, our results are in agreement with another meta-analysis which did not consider the dose of the supplementation, which found that supplementation of vitamin D alone probably reduces the risk of preeclampsia (RR = 0.48, 95% CI = 0.30–0.79) and gestational diabetes (RR = 0.51, 95% CI = 0.27–0.97), but makes little or no difference in the risk of having a preterm birth compared to no intervention or placebo (RR = 0.66, 95% CI = 0.34–1.30). 5 However, our results differ from another meta-analysis which took into account the dose of the vitamin D supplementation, suggesting that supplementation of vitamin D of more than 600 IU/day makes little or no difference to the risk of preeclampsia (RR = 0.96, 95% CI = 0.65–1.42), but probably reduces the risk of gestational diabetes (RR = 0.54, 95% CI = 0.34–0.86). 12 The differences between our results are probably caused by the different search terms and included studies based on our more strict criteria, where we did not allow studies where other nutrients are given together with the vitamin D.
Nevertheless, certain limitations need to be considered in interpreting our study. First, a few studies were excluded due to full-text non available and abstract conference. Also, we restrict to only English language studies. Thus, it prevented us from analyzing more data. However, since we only focused on RCT, with a large sample size and numbers of outcome, this study might become a basis for further study related to vitamin D supplementation dosage in pregnancy. Furthermore, in some of the studies we included, the baseline maternal vitamin D was not taken into account. However, we did not exclude those studies because vitamin D supplementation is meant for all pregnant women regardless of their baseline vitamin D level. Also, no study protocol was previously registered and published beforehand as we immediately began with the search due to internal time constraints in performing our study.
Moreover, it is also important to note that our present study did not set any inclusion or exclusion criteria in terms of the duration of supplementation. This results in different studies beginning the vitamin D supplementation in earlier pregnancy than others, with the earliest at 10 weeks and the latest at 30 weeks of gestation. This limits our interpretation of results into vitamin D supplementation before 30 weeks of gestation. Considering that obstetrical complications, such as preeclampsia and GDM, stem from placental pathologies occurring in early placentation, further studies should focus on not only the dosage but also the ideal time to begin the supplementation.
Conclusion
Our study found that vitamin D supplementation > 2000 IU/day is important to reduce the risk of GDM. Lower dose vitamin D supplementation ( ⩽ 2000 IU/day) is adequate to reduce the risk of preeclampsia, with no significant difference when compared to the higher dose (> 2000 IU/day). Furthermore, we found no effect on the incidence of preterm birth and changes in birth weight on different doses of vitamin D supplementation. However, since the quality of evidence was considered moderate to low, more studies are required to soundly conclude on the optimal dose for vitamin D supplementation to prevent maternal–fetal pregnancy complications.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221111066 – Supplemental material for Vitamin D supplementation higher than 2000 IU/day compared to lower dose on maternal–fetal outcome: Systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057221111066 for Vitamin D supplementation higher than 2000 IU/day compared to lower dose on maternal–fetal outcome: Systematic review and meta-analysis by Rima Irwinda, Rabbania Hiksas, Angga Wiratama Lokeswara and Noroyono Wibowo in Women’s Health
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.